

Impact of Vitamin D Deficiency on Mental Health in University Students: A Cross-Sectional Study

 ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Sampling
2.3. Study Questionnaire
2.4. Data Collection
2.5. Statistical Analysis
3. Results
3.1. Demographic Characteristics
3.2. General Characteristics of the Participants
3.3. Vitamin D Status and Academic Performance
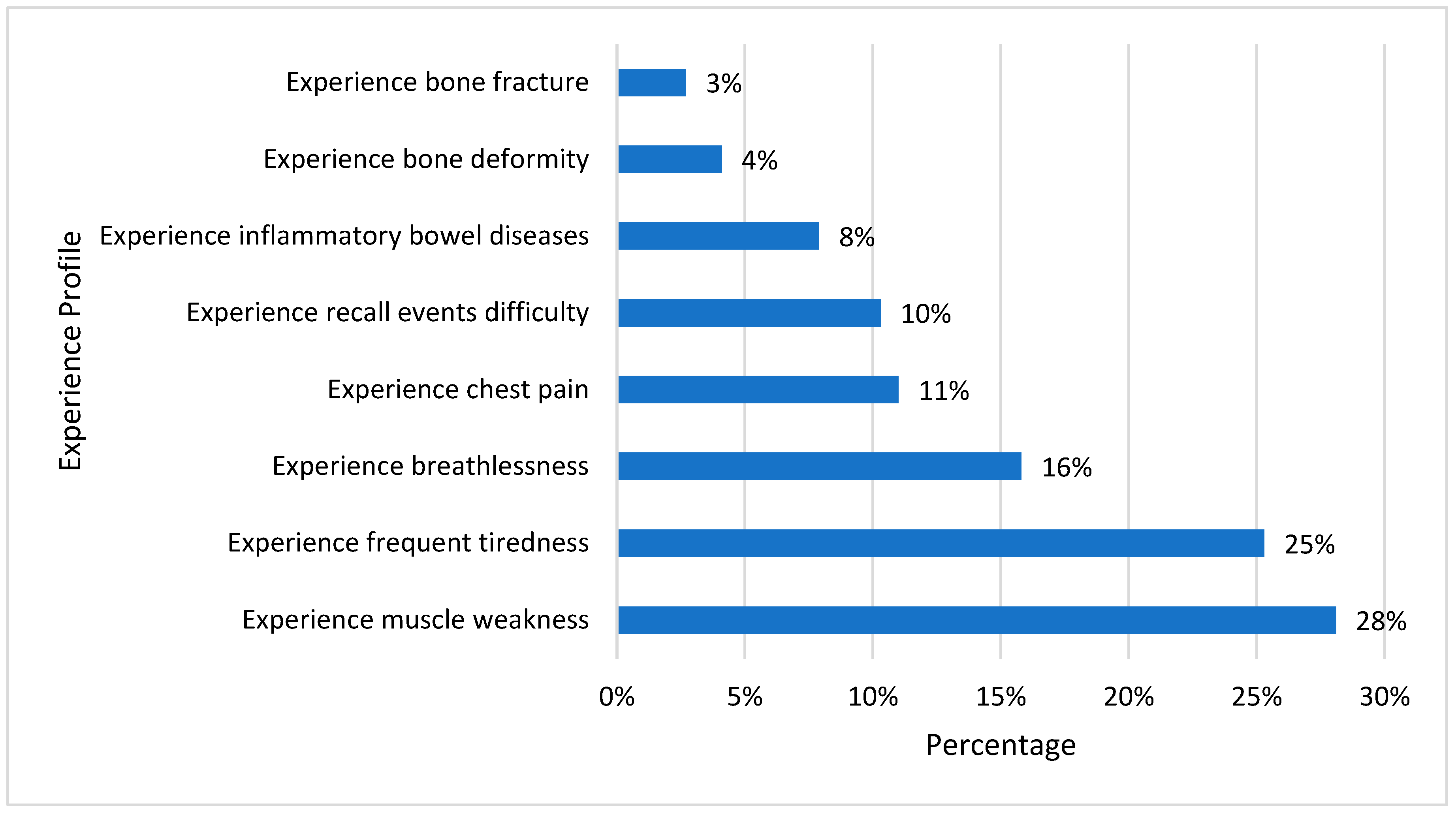
3.4. Symptoms of Vitamin D Deficiency
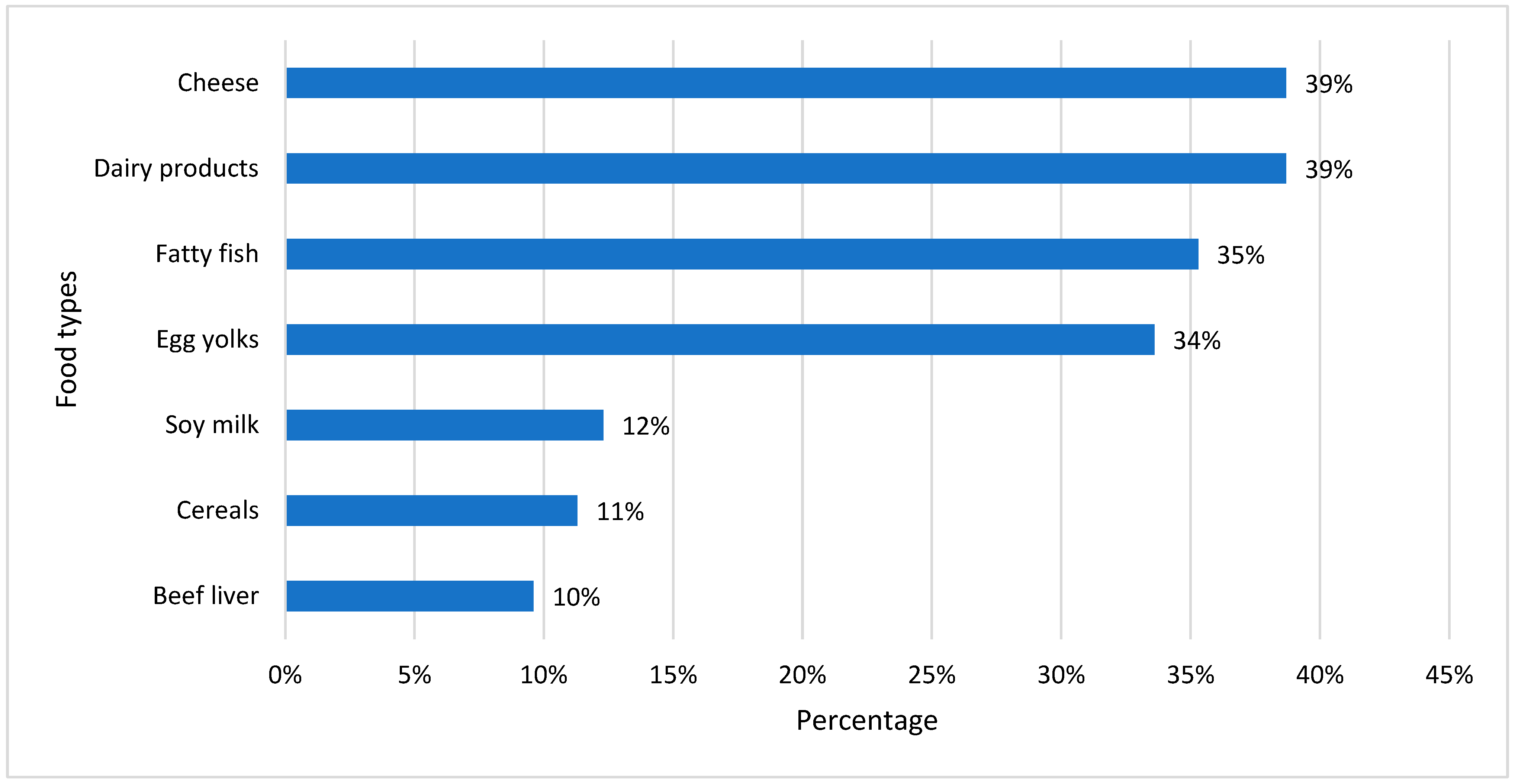
3.5. Dietary Status of Participants
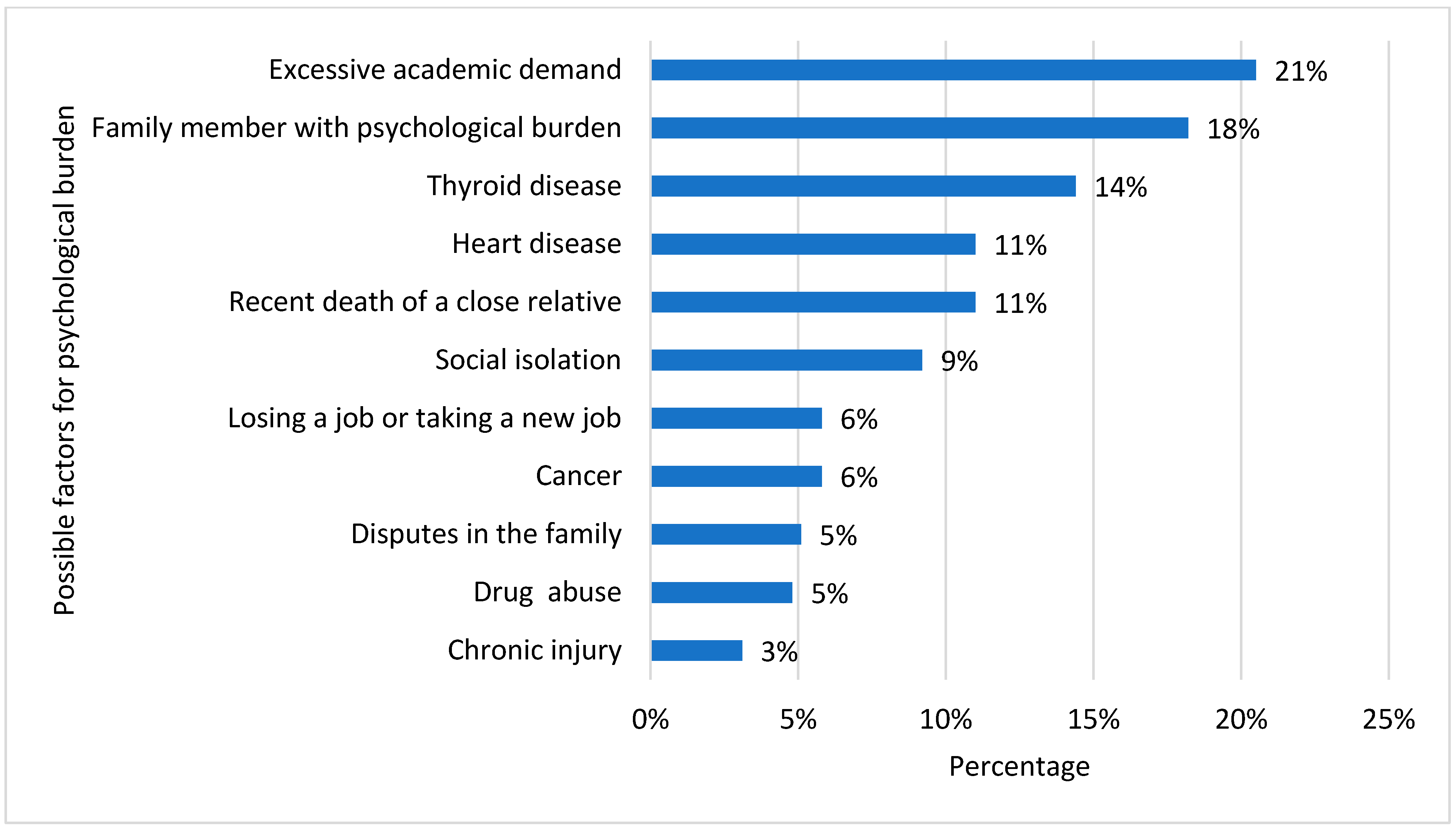
3.6. Risk Factors for Depression
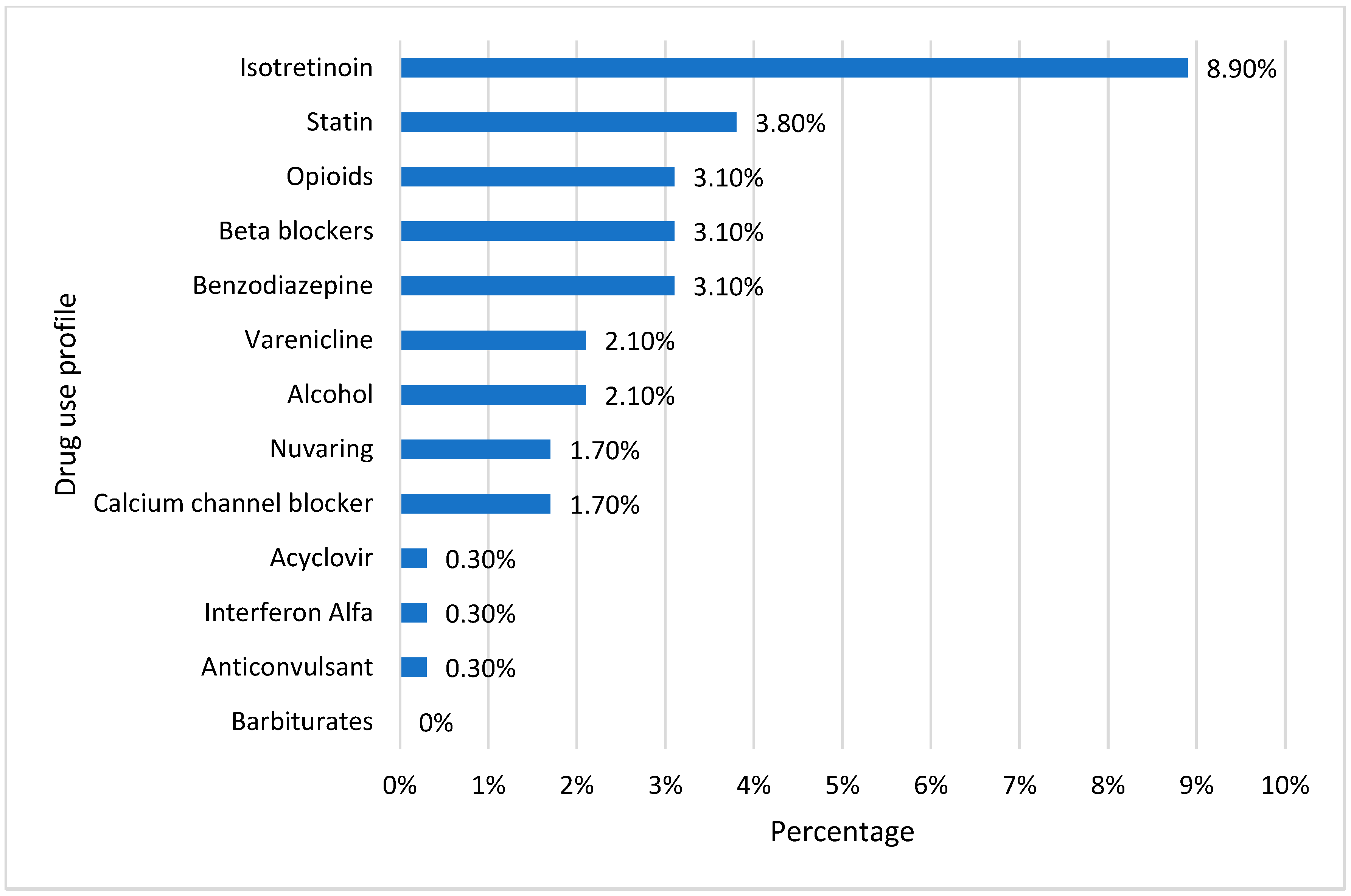
3.7. Drug Use Profile That May Cause Vitamin D Deficiency
3.8. Analysis of Psychological Burden Using DASS-21
3.9. Level of Severity of Psychological Burden among Participants
3.10. Regression Analysis for Depression
3.11. Regression Analysis for Anxiety
3.12. Regression Analysis for Stress
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ramly, M.; Moy, F.M.; Pendek, R.; Suboh, S.; Boon, A.T.T. Study protocol: The effect of vitamin D supplements on cardiometabolic risk factors among urban premenopausal women in a tropical country—A randomized controlled trial. BMC Public Health 2013, 13, 416. [Google Scholar] [CrossRef] [PubMed]
- Jacobsen, R.; Abrahamsen, B.; Bauerek, M.; Holst, C.; Jensen, C.B.; Knop, J.; Raymond, K.; Rasmussen, L.B.; Stougaard, M.; Sørensen, T.I.; et al. The influence of early exposure to vitamin D for development of diseases later in life. BMC Public Health 2013, 13, 515–518. [Google Scholar] [CrossRef] [PubMed]
- Veloudi, P.; Jones, G.; Sharman, J.E. Effectiveness of Vitamin D Supplementation for Cardiovascular Health Outcomes. Pulse 2016, 4, 193–207. [Google Scholar] [CrossRef]
- Holick, M.F. Vitamin D deficiency. N. Engl. J. Med. 2007, 357, 266–281. [Google Scholar] [CrossRef]
- Grober, U.; Spitz, J.; Reichrath, J.; Kisters, K.; Holick, M.F. Vitamin D: Update 2013: From rickets prophylaxis to general preventive healthcare. Derm.-Endocrinol. 2013, 5, 331–474. [Google Scholar] [CrossRef]
- Straube, S.; Moore, A.R.; Derry, S.; McQuay, H.J. Vitamin D and chronic pain. Pain 2009, 141, 10–13. [Google Scholar] [CrossRef]
- Adams, J.S.; Hewison, M. Update in vitamin D. J. Clin. Endocrinol. Metab. 2010, 95, 471–478. [Google Scholar] [CrossRef] [PubMed]
- Jhee, J.H.; Kim, H.; Park, S.; Yun, H.-R.; Jung, S.-Y.; Kee, Y.K.; Yoon, C.-Y.; Park, J.T.; Han, S.H.; Kang, S.-W.; et al. Vitamin D deficiency is significantly associated with depression in patients with chronic kidney disease. PLoS ONE 2017, 12, e0171009. [Google Scholar] [CrossRef] [PubMed]
- Schlögl, M.; Holick, M.F. Vitamin D and neurocognitive function. Clin. Interv. Aging 2014, 9, 559–568. [Google Scholar]
- Nimmrich, V.; Eckert, A. Calcium channel blockers and dementia. Br. J. Pharmacol. 2013, 169, 1203–1210. [Google Scholar] [CrossRef]
- Nair, R.; Maseeh, A. Vitamin D: The “sunshine” vitamin. J. Pharmacol. Pharmacother. 2012, 3, 118. [Google Scholar] [PubMed]
- Bassil, D.; Rahme, M.; Hoteit, M.; Fuleihan, G.E.-H. Hypovitaminosis D in the Middle East and North Africa: Prevalence, risk factors and impact on outcomes. Derm.-Endocrinol. 2013, 5, 274–298. [Google Scholar] [CrossRef] [PubMed]
- Mithal, A.; Wahl, D.A.; Bonjour, J.P.; Burckhardt, P.; Dawson-Hughes, B.; Eisman, J.A.; Fuleihan, G.E.; Josse, R.G.; Lips, P.T.; Morales-Torres, J. IOF Committee of Scientific Advisors (CSA) Nutrition Working Group. Global vitamin D status and determinants of hypo-vitaminosis D. Osteoporos. Int. 2009, 20, 1807–1820. [Google Scholar] [CrossRef] [PubMed]
- E Elshafie, D.; I Al-Khashan, H.; Mishriky, A.M. Comparison of vitamin D deficiency in Saudi married couples. Eur. J. Clin. Nutr. 2012, 66, 742–745. [Google Scholar] [CrossRef] [PubMed]
- Hasanato, R. High Prevalence of Vitamin D Deficiency in Healthy Female Medical Students in Central Saudi Arabia: Impact of Nutritional and Environmental Factors. Acta Endocrinol. 2015, 11, 257–261. [Google Scholar] [CrossRef]
- Naeem, Z.; AlMohaimeed, A.; Sharaf, F.K.; Ismail, H.; Shaukat, F.; Inam, S.N.B. Vitamin D status among population of Qassim region, Saudi Arabia. Int. J. Health Sci. 2011, 5, 116–124. [Google Scholar]
- Kessler, R.C.; Berglund, P.; Demler, O.; Jin, R.; Koretz, D.; Merikangas, K.R.; Rush, A.J.; Walters, E.E.; Wang, P.S. The epidemiology of major depressive disorder: Results from the National Comorbidity Survey Replication (NCS-R). JAMA 2003, 289, 3095–3105. [Google Scholar] [CrossRef]
- Vieth, R.; Bischoff-Ferrari, H.; Boucher, B.J.; Dawson-Hughes, B.; Garland, C.F.; Heaney, R.P.; Holick, M.F.; Hollis, B.W.; Lamberg-Allardt, C.; McGrath, J.J.; et al. The urgent need to recommend an intake of vitamin D that is effective. Am. J. Clin. Nutr. 2007, 85, 649–650. [Google Scholar] [CrossRef]
- Eyles, D.W.; Smith, S.; Kinobe, R.; Hewison, M.; McGrath, J.J. Distribution of the Vitamin D receptor and 1α-hydroxylase in human brain. J. Chem. Neuroanat. 2005, 29, 21–30. [Google Scholar] [CrossRef]
- Krishnan, V.; Nestler, E.J. Linking molecules to mood: New insight into the biology of depression. Am. J. Psychiatry 2010, 167, 1305–1320. [Google Scholar] [CrossRef]
- Anglin, R.E.; Samaan, Z.; Walter, S.D.; McDonald, S.D. Vitamin D deficiency and depression in adults: Systematic review and meta-analysis. Br. J. Psychiatry 2013, 202, 100–107. [Google Scholar] [CrossRef]
- de Abreu, D.F.; Eyles, D.; Feron, F. Vitamin D, a neuro-immunomodulator: Implications for neurodegenerative and autoimmune diseases. Psychoneuroendocrinology 2009, 34 (Suppl. S1), S265–S277. [Google Scholar] [CrossRef]
- Kjærgaard, M.; Waterloo, K.; Wang, C.E.; Almås, B.; Figenschau, Y.; Hutchinson, M.S.; Svartberg, J.; Jorde, R. Effect of vitamin D sup-plement on depression scores in people with low levels of serum 25-hydroxyvitamin D: Nested case-control study and randomised clinical trial. Br. J. Psychiatry 2012, 201, 360–368. [Google Scholar] [CrossRef] [PubMed]
- Wilkins, C.H.; Sheline, Y.I.; Roe, C.M.; Birge, S.J.; Morris, J.C. Vitamin D Deficiency Is Associated With Low Mood and Worse Cognitive Performance in Older Adults. Am. J. Geriatr. Psychiatry 2006, 14, 1032–1040. [Google Scholar] [CrossRef] [PubMed]
- May, H.T.; Bair, T.L.; Lappe, D.L.; Anderson, J.L.; Horne, B.D.; Carlquist, J.F.; Muhlestein, J.B. Association of vitamin D levels with incident de-pression among a general cardiovascular population. Am. Heart J. 2010, 159, 1037–1043. [Google Scholar] [CrossRef] [PubMed]
- Chan, R.; Chan, D.; Woo, J.; Ohlsson, C.; Mellström, D.; Kwok, T.; Leung, P. Association between serum 25-hydroxyvitamin D and psy-chological health in older Chinese men in a cohort study. J. Affect. Disord. 2011, 130, 251–259. [Google Scholar] [CrossRef]
- Pan, A.; Lu, L.; Franco, O.H.; Yu, Z.; Li, H.; Lin, X. Association between depressive symptoms and 25-hydroxyvitamin D in mid-dle-aged and elderly Chinese. J. Affect. Disord. 2009, 118, 240–243. [Google Scholar] [CrossRef]
- Przybelski, R.J.; Binkley, N.C. Is vitamin D important for preserving cognition? A positive correlation of serum 25-hydroxyvitamin D concentration with cognitive function. Arch. Biochem. Biophys. 2007, 460, 202–205. [Google Scholar] [CrossRef]
- Florence, M.D.; Asbridge, M.; Veugelers, P.J. Diet Quality and Academic Performance. J. Sch. Health 2008, 78, 209–215. [Google Scholar] [CrossRef]
- Lacapria, K. Vitamin D Deficiency Likely Not too Relevant to Academic Succeed, Study Says, Inquisitr. 2012. Available online: https://www.inquisitr.com/219131/vitamin-d-deficiency-likely-not-too-relevant-to-academic-success/ (accessed on 3 July 2023).
- Henry, J.D.; Crawford, J.R. The short-form version of the Depression Anxiety Stress Scales (DASS-21): Construct validity and normative data in a large non-clinical sample. Br. J. Clin. Psychol. 2005, 44, 227–239. [Google Scholar] [CrossRef]
- Lovibond, S.H.; Lovibond, P.F. Manual for the Depression Anxiety Stress Scales, 2nd ed.; Psychological Foundation: Sydney, Australia, 1995. [Google Scholar]
- Asdaq, S.M.B.; Yasmin, F. Risk of psychological burden in polycystic ovary syndrome: A case control study in Riyadh, Saudi Arabia. J. Affect. Disord. 2020, 274, 205–209. [Google Scholar] [CrossRef]
- Moussa, M.T.; Lovibond, P.; Laube, R.; Megahead, H.A. Psychometric Properties of an Arabic Version of the Depression Anxiety Stress Scales (DASS). Res. Soc. Work. Prac. 2016, 27, 375–386. [Google Scholar] [CrossRef]
- AlZahrani, W.I.; Oommen, A. Role of vitamin D in the academic performance of health sciences students in Saudi Arabia. Arab. Gulf J. Sci. Res. 2023, 41, 4–47. [Google Scholar] [CrossRef]
- Ardawi, M.-S.M.; Qari, M.H.; Rouzi, A.A.; Maimani, A.A.; Raddadi, R.M. Vitamin D status in relation to obesity, bone mineral density, bone turnover markers and vitamin D receptor genotypes in healthy Saudi pre- and postmenopausal women. Osteoporos. Int. 2010, 22, 463–475. [Google Scholar] [CrossRef]
- Feskanich, D.; Willett, W.C.; A Colditz, G. Calcium, vitamin D, milk consumption, and hip fractures: A prospective study among postmenopausal women. Am. J. Clin. Nutr. 2003, 77, 504–511. [Google Scholar] [CrossRef] [PubMed]
- Bolland, M.J.; Leung, W.; Tai, V.; Bastin, S.; Gamble, G.D.; Grey, A.; Reid, I.R. Calcium intake and risk of fracture: Systematic review. BMJ 2015, 351, h4580. [Google Scholar] [CrossRef]
- Bicikova, M.; Duskova, M.; Vitku, J.; Kalvachová, B.; Ripova, D.; Mohr, P.; Starka, L. Vitamin D in Anxiety and Affective Disorders. Physiol. Res. 2015, 64, S101–S103. [Google Scholar] [CrossRef]
- Ganji, V.; Milone, C.; Cody, M.M.; McCarty, F.; Wang, Y.T. Serum vitamin D concentrations are related to depression in young adult US population: The Third National Health and Nutrition Examination Survey. Int. Arch. Med. 2010, 3, 29. [Google Scholar] [CrossRef]
- Skobowiat, C.; Dowdy, J.C.; Sayre, R.M.; Tuckey, R.C.; Slominski, A. Cutaneous hypothalamic-pituitary-adrenal axis homolog: Regulation by ultraviolet radiation. Am. J. Physiol. Metab. 2011, 301, E484–E493. [Google Scholar] [CrossRef]
- Skobowiat, C.; Postlethwaite, A.E.; Slominski, A.T. Skin exposure to ultraviolet B rapidly activates systemic neu-roendocrine and immunosuppressive responses. Photochem. Photobiol. 2017, 93, 1008–1015. [Google Scholar] [CrossRef]
- Patrick, R.P.; Ames, B.N. Vitamin D hormone regulates serotonin synthesis. Part 1: Relevance for autism. FASEB J. 2014, 28, 2398–2413. [Google Scholar] [CrossRef]
- Sabir, M.S.; Haussler, M.R.; Mallick, S.; Kaneko, I.; Lucas, D.A.; Haussler, C.A.; Whitfield, G.K.; Jurutka, P.W. Optimal vitamin D spurs serotonin: 1,25-dihydroxyvitamin D represses serotonin reuptake transport (SERT) and degradation (MAO-A) gene expression in cultured rat serotonergic neuronal cell lines. Genes Nutr. 2018, 13, 19. [Google Scholar] [CrossRef]
- Asdaq, S.M.B.; Alajlan, S.A.; Mohzari, Y.; Asad, M.; Alamer, A.; Alrashed, A.A.; Nayeem, N.; Nagaraja, S. COVID-19 and Psychological Health of Female Saudi Arabian Population: A Cross-Sectional Study. Healthcare 2020, 8, 542. [Google Scholar] [CrossRef] [PubMed]
- Afifi, M. Depression in adolescents: Gender differences in Oman and Egypt. East. Mediterr. Health J. 2006, 12, 61–71. [Google Scholar] [PubMed]
- Becker, S.; Al Zaid, K.; Al Faris, E. Screening for Somatization and Depression in Saudi Arabia: A Validation Study of the Phq in Primary Care. Int. J. Psychiatry Med. 2002, 32, 271–283. [Google Scholar] [CrossRef]
- Muhairi, S.J.; E Mehairi, A.; A Khouri, A.; Naqbi, M.M.; A Maskari, F.; Al Kaabi, J.; Al Dhaheri, A.S.; Nagelkerke, N.; Shah, S.M. Vitamin D deficiency among healthy adolescents in Al Ain, United Arab Emirates. BMC Public Health 2013, 13, 33. [Google Scholar] [CrossRef] [PubMed]
- Allali, F.; El Aichaoui, S.; Khazani, H.; Benyahia, B.; Saoud, B.; El Kabbaj, S.; Bahiri, R.; Abouqal, R.; Hajjaj-Hassouni, N. High Prevalence of Hypovitaminosis D in Morocco: Relationship to Lifestyle, Physical Performance, Bone Markers, and Bone Mineral Density. Semin. Arthritis Rheum. 2008, 38, 444–451. [Google Scholar] [CrossRef] [PubMed]
- O’Neil, A.; Sanna, L.; Redlich, C.; Sanderson, K.; Jacka, F.; Williams, L.J.; A Pasco, J.; Berk, M. The impact of statins on psychological wellbeing: A systematic review and meta-analysis. BMC Med. 2012, 10, 154. [Google Scholar] [CrossRef]
- Maes, M.; Fišar, Z.; Medina, M.; Scapagnini, G.; Nowak, G.; Berk, M. New drug targets in depression: Inflammatory, cell-mediated immune, oxidative and nitrosative stress, mitochondrial, antioxidant, and neuroprogressive pathways. And new drug candidates—Nrf2 activators and GSK-3 inhibitors. Inflammopharmacology 2012, 20, 127–150. [Google Scholar] [CrossRef]
- Edinoff, A.N.; Nix, C.A.; Hollier, J.; Sagrera, C.E.; Delacroix, B.M.; Abubakar, T.; Cornett, E.M.; Kaye, A.M.; Kaye, A.D. Benzodiazepines: Uses, Dangers, and Clinical Considerations. Neurol. Int. 2021, 13, 594–607. [Google Scholar] [CrossRef]
- Viola, M.; Ouyang, D.; Xu, J.; Maciejewski, P.K.; Prigerson, H.G.; Derry, H.M. Associations between beta-blocker use and psychological distress in bereaved adults with cardiovascular conditions. Stress Health 2021, 38, 147–153. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Variables | Frequency (n = 480) | Percentage | p Value |
|---|---|---|---|---|
| Age | 20–22 years | 245 | 51.04% | 0.032 |
| 23–25 years | 134 | 27.91% | ||
| >25 years | 101 | 21.04% | ||
| Gender | Male | 221 | 46.04% | 0.654 |
| Female | 259 | 53.95% | ||
| College | College of Medicine | 135 | 28.12% | 0.078 |
| College of Pharmacy | 182 | 37.91% | ||
| College of Applied Science | 163 | 33.95% | ||
| Study level | 1–4 | 122 | 25.41% | 0.754 |
| 5–7 | 189 | 39.37% | ||
| ≥8 | 169 | 35.20% | ||
| GPA (in a scale of 4) | 0–1.5 | 137 | 28.54% | 0.048 |
| 1.51–3 | 215 | 44.79% | ||
| 3.1–4 | 128 | 26.66% | ||
| Nationality | Saudi | 391 | 81.45% | 0.001 |
| Non-Saudi | 89 | 18.54% |
| Characteristics | Variables | Frequency | Percentage | p Value |
|---|---|---|---|---|
| Did you gain or lose body weight during the last three months? | Weight loss | 154 | 32.08% | 0.432 |
| Maintaining | 189 | 39.37% | ||
| Weight gain | 137 | 28.54% | ||
| Your perceived body shape | Lean (slim) | 87 | 18.13% | 0.094 |
| Normal | 231 | 48.13% | ||
| Obese | 162 | 33.75% | ||
| Do you practice physical exercise? | Yes | 231 | 48.13% | 0.765 |
| No | 249 | 51.88% | ||
| How many times do you do physical exercise per week? | 1–2 days per week | 112 | 23.33% | 0.065 |
| 3–4 days per week | 76 | 15.83% | ||
| More than 4 days per week | 43 | 8.96% | ||
| Not applicable | 249 | 51.88% | ||
| What is your duration of physical exercise per week? | Intense physical activity for at least 20 min | 132 | 27.50% | 0.076 |
| Moderate physical activity for at least 30 min | 69 | 14.38% | ||
| Walking at least 30 min | 30 | 6.25% | ||
| Not applicable | 249 | 51.88% | ||
| Including exercise, how many hours do you spend outside during daylight hours? | Less than 01 h/day | 231 | 48.13% | 0.034 |
| 1–2 h/day | 122 | 25.42% | ||
| 2–4 h/day | 81 | 16.88% | ||
| 4–6 h/day | 38 | 7.92% | ||
| More than 6 h | 8 | 1.67% | ||
| Do you have vitamin D deficiency? | Yes | 287 | 59.79% | 0.021 |
| No | 98 | 20.42% | ||
| I do not know | 95 | 19.79% | ||
| Do you take vitamin D supplement or a multivitamin that includes vitamin D? | Yes | 182 | 37.92% | 0.038 |
| No | 298 | 62.08% | ||
| Have you used sunscreen/sun protective cream in the last 12 months? | Yes | 176 | 36.67% | 0.041 |
| No | 304 | 63.33% | ||
| Did you ever try tanning beds/tanning booths? | Yes | 162 | 33.75% | 0.042 |
| No | 318 | 66.25% | ||
| Do you currently take an antidepressant medication? | Yes | 89 | 18.54% | 0.001 |
| No | 391 | 81.46% |
| Questions | Variables | GPA, n (Percentage) | p Value | ||
|---|---|---|---|---|---|
| Low | Moderate | High | |||
| Do you have vitamin D deficiency? | Yes | 102 (74.45) | 115 (53.48) | 70 (54.68) | 0.048 |
| No, or not sure | 35 (25.54) | 100 (46.51) | 58 (45.31) | ||
| Do you take vitamin D supplement or multivitamin that includes vitamin D? | Yes | 98 (71.53) | 45 (20.93) | 39 (30.46) | 0.017 |
| No | 39 (28.46) | 170 (79.06) | 89 (69.53) | ||
| Have you used sunscreen/sun protective cream in the last 12 months? | Yes | 75 (54.74) | 52 (24.18) | 49 (38.28) | 0.082 |
| No | 62 (45.25) | 163 (75.81) | 79 (61.71) | ||
| Did you ever try a tanning bed/tanning booth? | Yes | 65 (47.44) | 58 (26.97) | 39 (30.46) | 0.076 |
| No | 72 (52.55) | 157 (73.02) | 89 (69.53) | ||
| Categories | Vitamin D Deficient (N = 285) | Control (N = 193) | Total (N = 480) | p Value * |
|---|---|---|---|---|
| Depression (n) | 172 | 92 | 264 | 0.042 |
| Prevalence (%) | 60.35% | 47.66% | 55% | |
| Anxiety (n) | 189 | 103 | 292 | 0.031 |
| Prevalence (%) | 66.31% | 53.36% | 60.83% | |
| Stress (n) | 214 | 112 | 326 | 0.001 |
| Prevalence (%) | 75.08% | 58.03% | 67.91% |
| Categories | Vitamin D Deficient | Control | Total | p Value * |
|---|---|---|---|---|
| Depression, n (%) | 172 (65.15) | 92 (34.84) | 264 (100) | 0.032 |
| Mild | 51 (29.65) | 42 (45.65) | 93 (35.22) | |
| Moderate | 87 (50.58) | 43 (46.73) | 130 (49.24) | |
| Severe | 34 (19.76) | 7 (7.60) | 41 (15.53) | |
| Anxiety, n (%) | 189 (64.72) | 103 (35.27) | 292 (100) | 0.021 |
| Mild | 82 (43.38) | 42 (40.77) | 124 (42.46) | |
| Moderate | 81 (42.85) | 55 (53.39) | 136 (46.57) | |
| Severe | 26 (13.75) | 6 (5.82) | 32 (10.95) | |
| Stress, n (%) | 214 (65.64) | 112 (34.35) | 326 (100) | 0.011 |
| Mild | 64 (29.90) | 54 (48.21) | 118 (36.19) | |
| Moderate | 116 (54.20) | 44 (39.28) | 160 (49.07) | |
| Severe | 34 (15.88) | 14 (12.5) | 48 (14.72) |
| Categories | Odds Ratio | Confidence Interval (95%) | p Value | |
|---|---|---|---|---|
| Lower | Upper | |||
| Vitamin D deficient | 4.96 | 2.22 | 6.78 | 0.001 |
| Female | 3.45 | 1.99 | 4.14 | 0.011 |
| Experience muscle pain | 3.21 | 2.490 | 5.01 | 0.021 |
| Frequent tiredness | 2.98 | 1.311 | 4.61 | 0.011 |
| Excessive academic demand | 2.87 | 1.76 | 3.98 | 0.001 |
| Family history of psychological burden | 2.76 | 1.98 | 4.02 | 0.025 |
| Obesity | 2.67 | 1.87 | 4.32 | 0.034 |
| Use of isotretinoin | 2.34 | 1.88 | 4.56 | 0.022 |
| Age between 20 and 22 years | 1.67 | 1.23 | 2.87 | 0.039 |
| Study level (1–4) | 1.32 | 1.01 | 2.43 | 0.028 |
| Use of statins | 0.342 | 0.121 | 0.98 | 0.013 |
| Categories | Odds Ratio | Confidence Interval (95%) | p Value | |
|---|---|---|---|---|
| Lower | Upper | |||
| Family history of psychological burden | 4.55 | 2.25 | 8.65 | 0.001 |
| Frequent tiredness | 4.21 | 2.56 | 7.98 | 0.001 |
| Use of isotretinoin | 4.01 | 2.87 | 7.76 | 0.001 |
| Vitamin D deficient | 3.87 | 2.55 | 6.59 | 0.001 |
| Excessive academic demand | 3.56 | 2.11 | 7.65 | 0.001 |
| Experience muscle pain | 3.22 | 2.05 | 6.85 | 0.001 |
| Female | 3.21 | 2.15 | 6.87 | 0.001 |
| Obesity | 3.11 | 2.11 | 5.96 | 0.001 |
| Age between 20 and 22 years | 2.13 | 1.85 | 4.21 | 0.032 |
| Study level (1–4) | 1.32 | 1.04 | 2.76 | 0.022 |
| Use of statins | 0.54 | 0.23 | 0.98 | 0.019 |
| Use of benzodiazepine | 0.44 | 0.18 | 0.76 | 0.019 |
| Use of beta-blockers | 0.32 | 0.10 | 0.65 | 0.010 |
| Categories | Odds Ratio | Confidence Interval (95%) | p Value | |
|---|---|---|---|---|
| Lower | Upper | |||
| Family history of psychological burden | 5.67 | 2.071 | 9.32 | 0.001 |
| Use of isotretinoin | 4.87 | 2.98 | 8.64 | 0.001 |
| Vitamin D deficient | 4.77 | 3.21 | 9.33 | 0.001 |
| Obesity | 4.21 | 2.52 | 8.48 | 0.001 |
| Frequent tiredness | 3.44 | 2.11 | 9.21 | 0.001 |
| Excessive academic demand | 3.21 | 1.98 | 8.61 | 0.001 |
| Experience muscle pain | 2.45 | 1.21 | 6.54 | 0.001 |
| Female | 2.33 | 1.76 | 5.43 | 0.001 |
| Study level (1–4) | 2.31 | 1.73 | 6.21 | 0.001 |
| Age between 20 and 22 years | 1.32 | 0.98 | 3.22 | 0.032 |
| Use of statins | 0.89 | 0.32 | 1.34 | 0.021 |
| Use of benzodiazepine | 0.87 | 0.43 | 1.81 | 0.011 |
| Use of beta-blockers | 0.56 | 0.23 | 1.01 | 0.034 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Almuqbil, M.; Almadani, M.E.; Albraiki, S.A.; Alamri, A.M.; Alshehri, A.; Alghamdi, A.; Alshehri, S.; Asdaq, S.M.B. Impact of Vitamin D Deficiency on Mental Health in University Students: A Cross-Sectional Study. Healthcare 2023, 11, 2097. https://doi.org/10.3390/healthcare11142097
Almuqbil M, Almadani ME, Albraiki SA, Alamri AM, Alshehri A, Alghamdi A, Alshehri S, Asdaq SMB. Impact of Vitamin D Deficiency on Mental Health in University Students: A Cross-Sectional Study. Healthcare. 2023; 11(14):2097. https://doi.org/10.3390/healthcare11142097
Chicago/Turabian StyleAlmuqbil, Mansour, Moneer E. Almadani, Salem Ahmad Albraiki, Ali Musharraf Alamri, Ahmed Alshehri, Adel Alghamdi, Sultan Alshehri, and Syed Mohammed Basheeruddin Asdaq. 2023. "Impact of Vitamin D Deficiency on Mental Health in University Students: A Cross-Sectional Study" Healthcare 11, no. 14: 2097. https://doi.org/10.3390/healthcare11142097
APA StyleAlmuqbil, M., Almadani, M. E., Albraiki, S. A., Alamri, A. M., Alshehri, A., Alghamdi, A., Alshehri, S., & Asdaq, S. M. B. (2023). Impact of Vitamin D Deficiency on Mental Health in University Students: A Cross-Sectional Study. Healthcare, 11(14), 2097. https://doi.org/10.3390/healthcare11142097