

Effectiveness of Physiotherapy in Managing Symptomatology in Gambling Disorder Patients: A Systematic Review

 ,
,  and
and
Abstract
1. Introduction
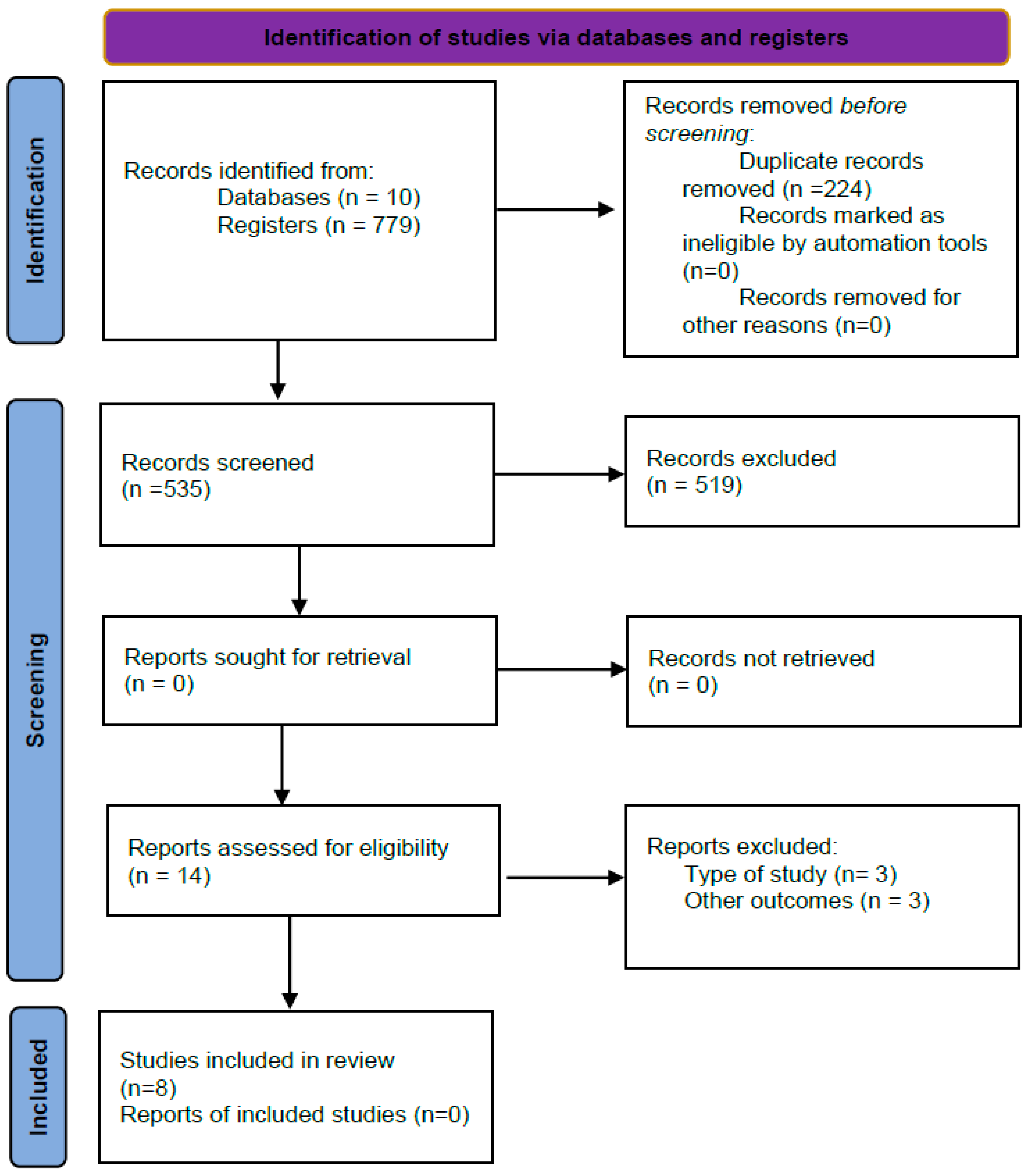
2. Materials and Methods
- Participants: people diagnosed with GD;
- Intervention: procedures typical of physiotherapy in addictions;
- Comparison groups: other treatments, placebo, or control group;
- Outcomes: craving, symptoms of anxiety, depression, impulsivity, stress, quality of life, severity of gambling symptoms, and related physiological measures;
- Study design: clinical trials.
3. Results
3.1. Type of Study and Participants
3.2. Assessment of the Main Variables
3.3. Interventions or Techniques Applied
3.3.1. Aerobic Physical Exercise
3.3.2. Non-Invasive Brain Stimulation (NIBS)
3.3.3. Relaxation Exercises
3.4. Effectiveness of the Interventions in the Experimental Group Compared to the Control
3.4.1. Effects of Aerobic Physical Exercise
3.4.2. Effects of Non-Invasive Brain Stimulation
3.4.3. Effects of Relaxation Techniques
3.5. Methodological Quality of the Studies
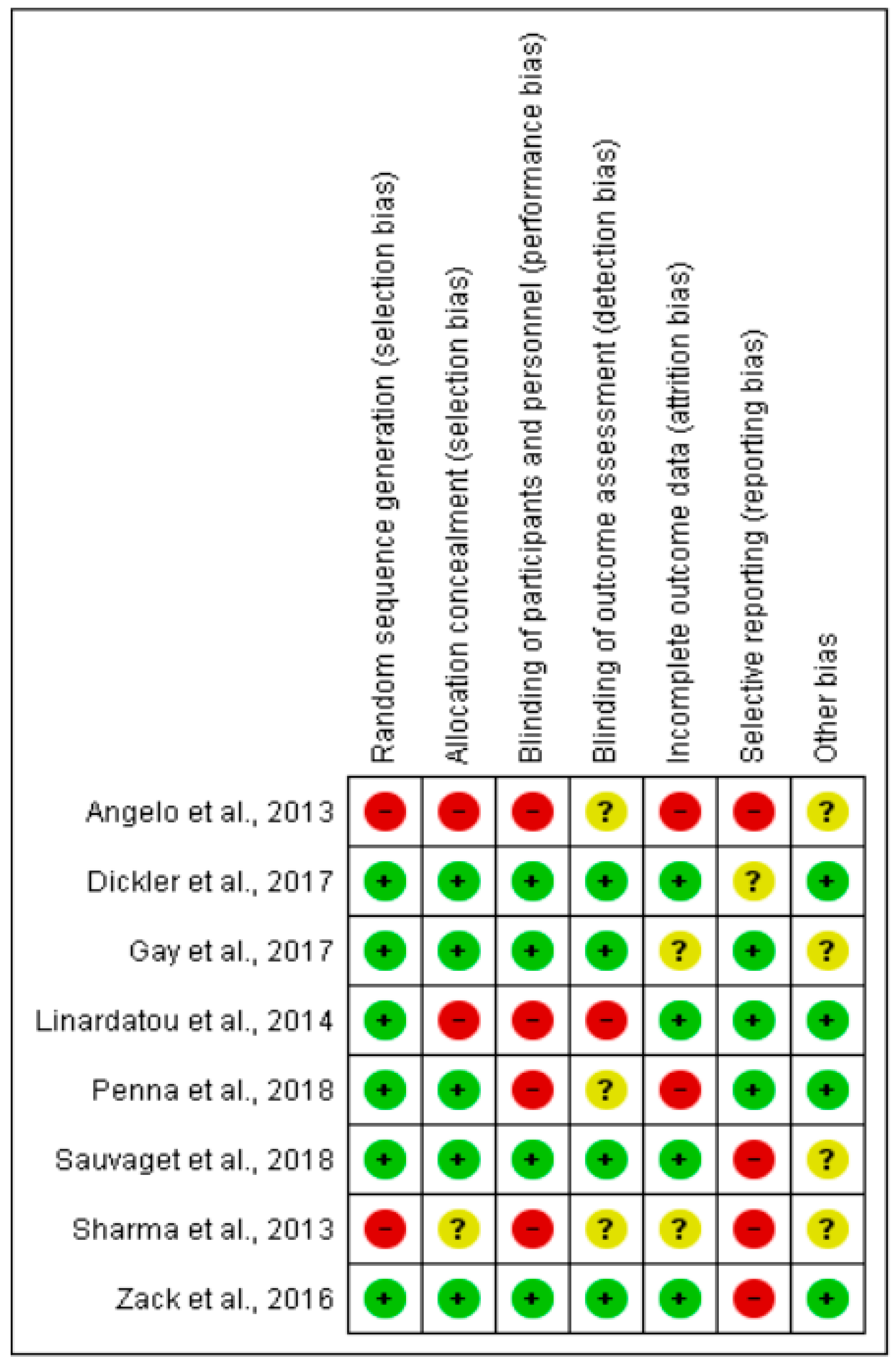
3.6. Risk of Bias of Cochrane
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Calado, F.; Griffiths, M.D. Problem gambling worldwide: An update and systematic review of empirical research (2000–2015). J. Behav. Addict. 2016, 5, 592–613. [Google Scholar] [CrossRef]
- ESPAD Group. ESPAD Report 2019: Results from the European School Survey Project on Alcohol and Other Drugs, EMCDDA Joint Publications; Publications Office of the European Union: Luxembourg, 2020.
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders-5 (DSM-5), 5th ed.; American Psychiatric Association: Arlington, TX, USA, 2013. [Google Scholar]
- World Health Organization. International Classification of Diseases 11th Revision (ICD-11), 11th ed.; World Health Organization: Geneva, Switzerland, 2019. [Google Scholar]
- Mestre-Bach, G.; Valenciano-Mendoza, E.; Mora-Maltas, B.; Fernández-Aranda, F.; Jiménez-Murcia, S. Adicción al juego: ¿mito o realidad? Evidencias científicas sobre el trastorno de juego. Mètode SSJ 2021, 2, 73–80. [Google Scholar] [CrossRef]
- Black, D.W.; Shaw, M.C.; McCormick, B.A.; Allen, J. Marital status, childhood maltreatment, and family dysfunction: A controlled study of pathological gambling. J. Clin. Psychiatry 2012, 73, 1293–1297. [Google Scholar] [CrossRef]
- Fong, T.W. The biopsychosocial consequences of pathological gambling. Psychiatry 2005, 2, 22–30. [Google Scholar]
- Gainsbury, S.; Hing, N.; Suhonen, N. Professional help-seeking for gambling problems: Awareness, barriers and motivators for treatment. J. Gambl. Stud. 2014, 30, 503–519. [Google Scholar] [CrossRef] [PubMed]
- Penna, A.C.; Kim, H.S.; Cabrita de Brito, A.; Tavares, H. The impact of an exercise program as a treatment for gambling disorder: A randomized controlled trial. Ment. Health Phys. Act. 2018, 15, 53–68. [Google Scholar] [CrossRef]
- Martínez, M.K.; Agost-Felip, M.R.; Martin, A.L. Prevalence of Pathological Gambling in the University Population from Valencian Community, Spain. Rev. Hosp. Psiq. Hab. 2019, 16, 15–31. [Google Scholar]
- Hakansson, A.; Karlsson, A. Suicide attempt in patients with gambling disorder-associations with comorbidity including substance use disorder. Front. Psychiatry 2020, 11, 593533. [Google Scholar] [CrossRef]
- Battersby, M.; Tolchard, B.; Scurrah, M.; Thomas, L. Suicide ideation and Behavior in People with Pathological Gambling Attending a Treatment Service. Int. J. Ment. Health Addict. 2006, 4, 233–246. [Google Scholar] [CrossRef]
- Kim, H.S.; Salmon, M.; Wohl, M.J.A.; Young, M. A dangerous cocktail: Alcohol consumption increases suicidal ideations among problem gamblers in the general population. Addict. Behav. 2016, 55, 50–55. [Google Scholar] [CrossRef]
- Linardatou, C.; Parios, A.; Varvogli, L.; Chrousos, G.; Darviri, C. An 8-week stress management program in pathological gamblers: A pilot randomized controlled trial. J. Psychiatr. Res. 2014, 56, 137–143. [Google Scholar] [CrossRef] [PubMed]
- Antons, S.; Müller, S.M.; Liebherr, M.; Brand, M. Gaming disorder: How to translate behavioral neuroscience into public health advances. Curr. Behav. Neurosci. Rep. 2020, 7, 267–277. [Google Scholar] [CrossRef]
- Schluter, M.G.; Hodgins, D.C. Reward-related decision-making in current and past disordered gambling: Implications for impulsive choice and risk preference in the maintenance of gambling disorder. Front. Behav. Neurosci. 2021, 15, 758329. [Google Scholar] [CrossRef] [PubMed]
- Limbrick-Oldfield, E.H.; Mick, I.; Cocks, R.E.; McGonigle, J.; Sharman, S.P.; Goldstone, A.P.; Stokes, P.R.A.; Waldman, A.; Erritzoe, D.; Bowden-Jones, H.; et al. Neural substrates of cue reactivity and craving in gambling disorder. Transl. Psychiatry 2017, 7, e992. [Google Scholar] [CrossRef] [PubMed]
- Volkow, N.D.; Morales, M. The brain on drugs: From reward to addiction. Cell 2015, 162, 712–725. [Google Scholar] [CrossRef] [PubMed]
- Antons, S.; Brand, M.; Potenza, M.N. Neurobiology of cue-reactivity, craving, and inhibitory control in non-substance addictive behaviors. J. Neurol. Sci. 2020, 415, 116952. [Google Scholar] [CrossRef]
- Bodor, D.; Ricijas, N.; Filipcic, I. Treatment of gambling disorder: Review of evidence-based aspects for best practice. Curr. Opin. Psychiatry 2021, 34, 508–513. [Google Scholar] [CrossRef]
- Sam-Wok, C.; Young-Chul, S.; Dai-Jin, K.; Jung-Seok, C.; Seohee, K.; Seung-Hyun, K.; HyunChl, Y. Treatment modalities for patients with gambling disorder. Ann. Gen. Psychiatry 2017, 16, 23. [Google Scholar] [CrossRef]
- Di Nicola, M.; De Crescenzo, F.; D’Alò, G.L.; Remondi, C.; Panaccione, I.; Moccia, L.; Molinaro, M.; Dattoli, L.; Lauriola, A.; Martinelli, S.; et al. Pharmacological amd Psychosocial treatment of adults with gambling disorder: A meta-review. J. Addict. Med. 2020, 14, e15–e23. [Google Scholar] [CrossRef]
- Cowlishaw, S.; Merkouris, S.; Dowling, N.; Anderson, C.; Jackson, A.; Thomas, S. Psychological therapies for pathological and problem gambling. Cochrane Database Syst. Rev. 2012, 11, CD008937. [Google Scholar] [CrossRef]
- Gooding, P.; Tarrier, N. A systematic review and meta-analysis of cognitive-behavioural interventions to reduce problem gambling: Hedging our bets? Behav. Res. Ther. 2009, 47, 592–607. [Google Scholar] [CrossRef]
- Yakovenko, I.; Quigley, L.; Hemmelgarn, B.R.; Hodgins, D.C.; Ronksley, P. The efficacy of motivational interviewing for disordered gambling: Systematic review and meta-analysis. Addict. Behav. 2015, 43, 72–82. [Google Scholar] [CrossRef] [PubMed]
- Catalán, D.J. Fisioterapia en Salud Mental: Antecedentes históricos. Rev. Colomb. Rehabil. 2019, 18, 162–180. [Google Scholar] [CrossRef]
- Estruch, R.; Sacanella, E. Alcohol: ¿tónico o tóxico cardiovascular? Clin. Investig. Arterioscl. 2005, 17, 183–195. [Google Scholar] [CrossRef]
- Donaghy, M.; Durward, B. A Report on the Clinical Effectiveness of Physiotherapy in Mental Health; Chartered Society of Physiotherapy: London, UK, 2000. [Google Scholar]
- Limsanon, T.; Kalayasiri, R. Preliminary effects of progressive muscle relaxation on cigarette craving and withdrawal symptoms in experienced smokers in acute cigarette abstinence: A randomized controlled trial. Behav. Ther. 2015, 46, 166–167. [Google Scholar] [CrossRef]
- Zhang, P.; Li, Z.; Yang, Q.; Zhou, J.; Ma, X. Effects of Taijiquan and Qigong exercises on depression and anxiety levels in patients with substance use disorders: A systematic review and meta-analysis. Sports Med. Health Sci. 2021, 4, 85–94. [Google Scholar] [CrossRef] [PubMed]
- Colledge, F.; Gerber, M.; Puhse, U.; Ludyga, S. Anaerobic exercise training in the therapy of substance use disorders: A systematic review. Front. Psychiatry 2018, 9, 644. [Google Scholar] [CrossRef] [PubMed]
- Gupta, S.; Jhanjee, S.; Dhawan, A. Effectiveness of Interventions Based on Yogic Breathing Practices (IB-YBP) on Substance Use Disorders-A Systematic Review of the Randomized Control Trials and Quasi-Experimental Trials. Subst. Use Misuse 2021, 56, 1624–1641. [Google Scholar] [CrossRef]
- Kedzior, K.K.; Gerkensmeier, I.; Schuchinsky, M. Can deep transcranial magnetic stimulation (DTMS) be used to treat substance use disorders (SUD)? A systematic review. BMC Psychiatry 2018, 18, 137. [Google Scholar] [CrossRef]
- Zhang, J.J.Q.; Fong, K.N.K.; Ouyang, R.; Siu, A.M.H.; Kranz, G.S. Effects of repetitive transcranial magnetic stimulation (rTMS) on craving and substance consumption in patients with substance dependence: A systematic review and meta-analysis. Addiction 2019, 114, 2137–2149. [Google Scholar] [CrossRef]
- Lardier, D.T.; Coakley, K.E.; Holladay, K.R.; Amorim, F.T.; Zuhl, M.N. Exercise as a Useful Intervention to Reduce Alcohol Consumption and Improve Physical Fitness in Individuals with Alcohol Use Disorder: A Systematic Review and Meta-Analysis. Front. Psychol. 2021, 12, 675285. [Google Scholar] [CrossRef]
- Catalán-Matamoros, D.J.; Gómez-Conesa, A.A. Physiotherapy and substance misuse. In Physiotherapy in Mental Health and Psychiatry: A Scientific and Clinical Based Approach, 1st ed.; Probst, M., Skjaerven, L., Eds.; Elsevier Health Sciences: Amsterdam, The Netherlands, 2017; pp. 234–240. ISBN 978-070-207-268-0. [Google Scholar]
- Korehpaz-Mashhadi, F.; Ahmadzadeh, H.; Rashidlamir, A.; Saffari, N. Change in metabolites level in internet-addicted adolescents through exercise. J. Bodyw. Mov. Ther. 2022, 31, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Liu, S.; Xiao, T.; Yang, L.; Loprinzi, P.D. Exercise as an alternative approach for treating smartphone addiction: A systematic review and meta-analysis of random controlled trials. Int. J. Environ. Res. Public Health 2019, 16, 3912. [Google Scholar] [CrossRef]
- Sauvaget, A.; Benoit, T.; Bulteau, S.; Jimenez-Murcia, S.; Fernandez-Aranda, F.; Wolz, I.; Menchón, J.M.; Achab, S.; Vanelle, J.M.; Grall-Bronnec, M. Transcranial direct current stimulation (tDCS) in behavioral and food addiction: A systematic review of efficacy, technical, and methodological issues. Front. Neurosci. 2015, 9, 349. [Google Scholar] [CrossRef] [PubMed]
- Pettorruso, M.; Miuli, A.; di Natale, C.; Montemitro, C.; Zoratto, F.; de Risio, L.; d’Andrea, G.; Dannon, P.N.; Martinotti, G.; di Giannantonio, M. Non-invasive brain stimulation targets and approaches to modulate gambling-related decisions: A systematic review. Addict. Behav. 2021, 112, 106657. [Google Scholar] [CrossRef]
- Zucchella, C.; Mantovani, E.; Federico, A.; Lugoboni, F.; Tamburin, S. Non-invasive brain stimulation for gambling disorder: A systematic review. Front. Neurosci. 2020, 14, 729. [Google Scholar] [CrossRef] [PubMed]
- Ribeiro, E.O.; Alfonso, N.H.; Morgado, P. Non-pharmacological treatment of gambling disorder: A systematic review of randomized controlled trials. BMC Psychiatry 2021, 21, 105. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; The PRISMA GROUP. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef]
- Paje, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Higgins, J.P.; Altman, D.G.; Gotzsche, P.C.; Juni, P.; Moher, D.; Oxman, A.D.; Savovic, J.; Schulz, K.; Weeks, L.; Sterne, J.A.C.; et al. The Cochrane Collaboration’s tool for assessing risk of bias in randomized trials. BMJ 2011, 343, d5928. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.T.; Green, S. Assessing risk of bias in included studies. In Cochrane Handbook for Systematic Reviews of Interventions, 2nd ed.; Higgins, J.P.T., Churchill, R., Chandler, J., Cumpston, M.S., Eds.; John Wiley & Sons: Chichester, UK, 2008; pp. 187–241. [Google Scholar]
- Sauvaget, A.; Bulteau, S.; Guilleux, A.; Leboucher, J.; Pichot, A.; Valrivière, P.; Vanelle, J.M.; Sébille-Rivain, V.; Grall-Bronnec, M. Both active and sham low-frequency rTMS single sessions over the right DLPFC decrease cue-induced cravings among pathological gamblers seeking treatment: A randomized, double-blind, sham-controlled crossover trial. J. Behav. Addict. 2018, 7, 126–136. [Google Scholar] [CrossRef]
- Gay, A.; Boutet, C.; Sigaud, T.; Kamgoue, A.; Sevos, J.; Brunelin, J.; Massoubre, C. A single session of repetitive transcranial magnetic stimulation of the prefrontal cortex reduces cue-induced craving in patients with gambling disorder. Eur. Psychiatry 2017, 41, 68–74. [Google Scholar] [CrossRef] [PubMed]
- Dickler, M.; Lenglos, C.; Renauld, E.; Ferland, F.; Edden, R.A.; Leblond, J.; Fecteau, S. Online effects of transcranial direct current stimulation on prefrontal metabolites in gambling disorder. Neuropharmacology 2018, 131, 51–57. [Google Scholar] [CrossRef] [PubMed]
- Zack, M.; Cho, S.S.; Parlee, J.; Jacobs, M.; Li, C.; Boileau, I.; Strafella, A. Effects of high frequency repeated transcranial magnetic stimulation and continuous theta burst stimulation on gambling reinforcement, delay discounting and stroop interference in men with pathological gambling. Brain Stimul. 2016, 9, 867–875. [Google Scholar] [CrossRef]
- Sharma, M.G.; Upadhyay, A.; Sharma, V. Mental health management of pathological gamblers by counseling and relaxation practices. J. Evid. Based Soc. Work 2013, 10, 505–508. [Google Scholar] [CrossRef]
- Angelo, D.L.; Tavares, H.; Zilberman, M.L. Evaluation of physical activity program for pathological gamblers in treatment. J. Gambl. Stud. 2013, 29, 589–599. [Google Scholar] [CrossRef] [PubMed]
- Angelo, D.L.; Tavares, H.; Bottura, H.M.; Zilberman, M.L. Physical exercise for pathological gamblers. Braz. J. Psychiatry 2009, 31, 76. [Google Scholar] [CrossRef]
- Abrantes, A.M.; Battle, C.L.; Strong, D.R.; Ing, E.; Dubreuil, M.E.; Gordon, A.; Brown, R.A. Exercise preferences of patients in substance abuse treatment. Ment. Health Phys. Act. 2011, 4, 79–87. [Google Scholar] [CrossRef]
- Lefaucheur, J.P.; Aleman, A.; Baeken, C.; Benninger, D.H.; Brunelin, J.; di Lazzaro, V.; Filipovic, S.R.; Grefkes, C.; Hasan, A.; Hummel, F.C.; et al. Evidence-based guidelines on the therapeutic use of repetitive transcranial magnetic stimulation (rTMS): An update (2014–2018). Clin. Neurophysiol. 2020, 131, 474–528. [Google Scholar] [CrossRef]
- Lefaucheur, J.P.; Antal, A.; Ayache, S.S.; Benninger, D.H.; Brunelin, J.; Cogiamanian, F.; Cotelli, M.; de Ridder, D.; Ferrucci, R.; Langguth, B.; et al. Evidence-based guidelines on the therapeutic use of transcranial direct current stimulation (tDCS). Clin. Neurophysiol. 2017, 128, 56–92. [Google Scholar] [CrossRef]
- Slutske, W.S. Natural recovery and treatment-seeking in pathological gambling: Results of two U.S. national surveys. Am. J. Psychiatry 2006, 163, 297–302. [Google Scholar] [CrossRef]
- Tucker, J.A.; Chandler, S.D.; Witkiewitz, K. Epidemiology of recovery from alcohol use disorder. Alcohol Res. 2020, 40, 2. [Google Scholar] [CrossRef]
- Blaszczynski, A.; Ladouceur, R.; Shaffer, H.J. A science-based framework for responsible gambling: The Reno model. J. Gambl. Stud. 2004, 20, 301–317. [Google Scholar] [CrossRef] [PubMed]
- Pfund, R.A.; Peter, S.C.; McAfee, N.W.; Ginley, M.K.; Whelan, J.P.; Meyers, A.W. Dropout from face-to-face, multi-session psychological treatment for problem and disordered gambling: A systematic review and meta-analysis. Psychol. Addict. Behav. 2021, 35, 901–913. [Google Scholar] [CrossRef] [PubMed]
- Serrano, O.; Cuesta, V. Proposal of variables for the design of a model about the TECHNO-ADDICTION to sex in the youth population. Rev. Esp. Comun. Salud. 2018, 9, 64–71. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Databases | Search Terms | Results | Select Articles | ||
|---|---|---|---|---|---|
| PUBMED | Gambler Gambling | AND | Physiotherapy | 37 | 4 |
| Physical therapy | |||||
| Physical therapy modalities | |||||
| Physical activity | |||||
| Exercise | |||||
| BBAT | |||||
| Basic body awareness therap | |||||
| Psychomotor therapy | |||||
| Massage | |||||
| Transcranial direct current stimulation Transcranial magnetic stimulation | |||||
| Electric stimulation therapy | |||||
| Relaxation | |||||
| Relaxation therapy | |||||
| Yoga | |||||
| EMBASE | Gambling Gambler | AND | Physiotherapy | 22 | 5 |
| Exercise | |||||
| Physical activity | |||||
| Massage | |||||
| Transcranial direct current stimulation | |||||
| Transcranial magnetic stimulation | |||||
| Electric stimulation therapy | |||||
| Yoga | |||||
| Relaxation | |||||
| PEDro | Gambling Gambler | 2 | 1 | ||
| Scopus | Gambler Gambling | AND | Physiotherapy | 241 | 5 |
| Physical therapy | |||||
| Physical therapy modalities | |||||
| Physical activity | |||||
| Exercise | |||||
| BBAT | |||||
| Basic body awareness therapy | |||||
| Psychomotor therapy | |||||
| Massage | |||||
| Transcranial direct current stimulation Transcranial magnetic stimulation | |||||
| Electric stimulation therapy | |||||
| Relaxation | |||||
| Relaxation therapy | |||||
| Yoga | |||||
| Web Of Science | Gambler Gambling | AND | Physiotherapy | 335 | 5 |
| Physical therapy | |||||
| Physical therapy modalities | |||||
| Physical activity | |||||
| Exercise | |||||
| BBAT | |||||
| Basic body awareness therapy | |||||
| Psychomotor therapy | |||||
| Massage | |||||
| Transcranial direct current stimulation Transcranial magnetic stimulation | |||||
| Electric stimulation therapy | |||||
| Relaxation | |||||
| Relaxation therapy | |||||
| Yoga | |||||
| Cochrane Library | Gambler Gambling | AND | Physiotherapy | 59 | 6 |
| Physical therapy | |||||
| Physical therapy modalities | |||||
| Physical activity | |||||
| Exercise | |||||
| BBAT | |||||
| Basic body awareness therapy | |||||
| Psychomotor therapy | |||||
| Massage | |||||
| Transcranial direct current stimulation | |||||
| Transcranial magnetic stimulation | |||||
| Electric stimulation therapy | |||||
| Relaxation | |||||
| Relaxation therapy | |||||
| Yoga | |||||
| Psycarticles | Gambler Gambling | AND | Physiotherapy | 1 | - |
| Physical therapy | |||||
| Physical therapy modalities | |||||
| Physical activity | |||||
| Exercise | |||||
| BBAT | |||||
| Basic body awareness therapy | |||||
| Psychomotor therapy | |||||
| Massage | |||||
| Transcranial direct current stimulation | |||||
| Transcranial magnetic stimulation | |||||
| Electric stimulation therapy | |||||
| Relaxation | |||||
| Relaxation therapy | |||||
| Yoga | |||||
| Scielo | Gambler Gambling | AND | Physiotherapy | 2 | - |
| Physical therapy | |||||
| Physical therapy modalities | |||||
| Physical activity | |||||
| Exercise | |||||
| BBAT | |||||
| Basic body awareness therapy | |||||
| Psychomotor therapy | |||||
| Massage | |||||
| Transcranial direct current stimulation | |||||
| Transcranial magnetic stimulation | |||||
| Electric stimulation therapy | |||||
| Relaxation | |||||
| Relaxation therapy | |||||
| Yoga | |||||
| Psicodoc | Gambler Gambling | AND | Physiotherapy | 0 | - |
| Physical therapy | |||||
| Physical therapy modalities | |||||
| Physical activity | |||||
| Exercise | |||||
| BBAT | |||||
| Basic body awareness therapy | |||||
| Psychomotor therapy | |||||
| Massage | |||||
| Transcranial direct current stimulation | |||||
| Transcranial magnetic stimulation | |||||
| Electric stimulation therapy | |||||
| Relaxation | |||||
| Relaxation therapy | |||||
| Yoga | |||||
| CINAHL | Gambler Gambling | AND | Physiotherapy | 80 | 2 |
| Physical therapy | |||||
| Physical therapy modalities | |||||
| Physical activity | |||||
| Exercise | |||||
| BBAT | |||||
| Basic body awareness therapy | |||||
| Psychomotor therapy | |||||
| Massage | |||||
| Transcranial direct current stimulation | |||||
| Transcranial magnetic stimulation | |||||
| Electric stimulation therapy | |||||
| Relaxation | |||||
| Relaxation therapy | |||||
| Yoga | |||||
| Author, Year | Type of Study Population (m/f) | Intervention | Outcomes (Outcomes Instruments) | Results |
|---|---|---|---|---|
| Penna, 2018 [9] | RCT n = 59 (34/25) IG: 32 CG: 27 | IG: 10’ stretching and 40’ running at 70–85% MHR CG: 50’ stretching 2 times/week, 8 weeks. |
| There was a significant improvement in relation to the severity of the gambling disorder (p = 0.01) and psychiatric comorbidities in both groups (IG: p = 0.005; CG: p = 0.015). |
| Sauvaget, 2018 [47] | CCT n = 31 (27/4) G1: 15 G2: 16 | G1: low-frequency rTMS/sham rTMS G2: sham rTMS/low-frequency rTMS 2 sessions of 6’ (1 active rTMS session and 1 sham rTMS session) over the right DLPFC with a 1–2 weeks interval. |
| After rTMS sessions, a significant craving decrease was found when active rTMS (p < 0.01) and sham rTMS (p < 0.01) were applied. There were no statistically significant differences between applying active rTMS or sham rTMS (p = 0.18). |
| Gay, 2017 [48] | CCT n = 22 (14/8) G1:11 G2:11 | G1: HF rTMS/sham rTMS G2: sham TMS/HF rTMS 2 sessions of 20’ (1 session of active rTMS and 1 of sham rTMS) over the left DLPFC with a 1-week interval. |
| There was a craving decrease after active rTMS (p = 0.04). Nevertheless, no significant changes were found regarding the behavior of the game (p = 0.68). |
| Dickler, 2017 [49] | CCT n = 18 (11/7) G1:18 | G1: 2 sessions of 30’ (1 active session and 1 sham session) tDCS over the right DLPFC with a 1-week interval. |
| Significantly higher GABA levels were found in DLPFC after tDCS than sham stimulation in the right DLPFC (p = 0.039); but there were no significant differences regarding Glx (p = 0.733) and NAA (p = 0.779) in the right DLPFC. There were no significant differences in the right striatum for GABA (p = 0.072), Glx (p = 0.839) and NAA (p = 0.222). A positive correlation was observed between risk-taking and prefrontal Glx (p = 0.050) and striatal GABA (p = 0.045); secondly, a correlation was found between the impulsiveness and the striatal NAA (p = 0.036); and finally, there was a positive correlation between the craving and the striatal Glx (p = 0.045). |
| Zack, 2016 [50] | RCT n = 9 (9/0) IG1: 3 IG2: 3 GC: 3 | IG1: HF rTMS over mPFC IG2: HF cTBS over right DLPFC CG: sham stimulation over mPFC 3 sessions each group with a 1-week interval. |
| The craving decreased for the rTMS group (IG1) compared to the sham stimulation (CG) (p = 0.032); secondly, there were no improvements in the cTBS group (IG2) compared to the sham group (CG) (p > 0.07). The ARCI of the cTBS group (GI2) decreased significantly compared to the sham group (CG) (p = 0.014); there were no differences for the rTMS group (GI1) compared to the sham group (CG) (p > 0.10). Diastolic BP decreased significantly for the cTBS group (GI2) compared to the sham group (CG) (p = 0.007). |
| Linardatau 2014 [14] | RCT pilot n = 45 (42/3) IG: 23 GC: 22 | IG: RB and PMR + education on diet, exercise, and stress (PMR and RB twice/day 25 min session) CG: diet, exercise, and stress education 8 weeks. |
| A statistically significant improvement was obtained in the IG on symptoms of stress (p < 0.01), anxiety (p < 0.01), and depression (p < 0.01) in the Dass-21. There was also a significant improvement in the IG on self-reported stress (p < 0.01), in life satisfaction (p < 0.01), and an improvement in quality of sleep (p < 0.01) and daily routine (p < 0.01). |
| Sharma, 2013 [51] | CT n = 110 IG: 55 GC: 55 | IG: advice and PMR (begins with 4 times/week and ends with 1 time every 15 days), 60’/90’ in duration CG: no treatment 6 months. |
| The IG significantly improved differences on the Death Anxiety Scale (p = 0.01) and on symptoms of anxiety (p = 0.01), depression (p = 0.01), obsession (p = 0.01), somatization (p = 0.01), and hysteria (p = 0.01); however, phobia worsened (p = 0.01). |
| Angelo, 2013 [52] | CT n = 63 (38/25) IG: 33 GC: 30 | IG: 10’ stretching and 40’ running at 65–70% HR CG: no intervention 8 sessions in 4 or 8 weeks. |
| Statistically significant improvements were found in the IG regarding the psychiatric comorbidities of depression (p = 0.015) and anxiety (p = 0.026), and in the severity of the GD (p = 0.042). A craving reduction (on the Visual Analogue Scale of Craving) was also observed in the IG after each physical activity session (p = 0.003) and at the end of the program in relation to the last 24 h (p < 0.001) and the last 7 days (p < 0.001). A positive correlation was observed between before and after session anxiety with BAI (p = 0.004), PCS (p < 0.001), and CQ (p < 0.001). |
| Item PEDro Scale | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | Total Score |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Penna et al., 2018 [9] | X | X | X | NO | NO | NO | X | NO | X | X | X | 6/10 |
| Sauvaget et al., 2018 [47] | X | X | X | NO | X | NO | X | NO | X | X | X | 7/10 |
| Gay et al., 2017 [48] | X | X | X | NO | X | NO | X | NO | NO | X | X | 6/10 |
| Dickler et al., 2017 [49] | X | X | X | NO | X | NO | X | NO | NO | X | X | 6/10 |
| Zack et al., 2016 [50] | X | X | X | NO | X | NO | X | NO | NO | X | X | 6/10 |
| Linardatou et al., 2014 [14] | X | X | X | X | NO | NO | NO | NO | NO | X | X | 5/10 |
| Sharma et al., 2013 [51] | NO | NO | NO | NO | NO | NO | NO | NO | NO | X | X | 2/10 |
| Angelo et al., 2013 [52] | X | NO | NO | X | NO | NO | NO | NO | NO | X | X | 3/10 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Carrascosa-Arteaga, P.; López-Liria, R.; Catalán-Matamoros, D.; Rocamora-Pérez, P. Effectiveness of Physiotherapy in Managing Symptomatology in Gambling Disorder Patients: A Systematic Review. Healthcare 2023, 11, 2055. https://doi.org/10.3390/healthcare11142055
Carrascosa-Arteaga P, López-Liria R, Catalán-Matamoros D, Rocamora-Pérez P. Effectiveness of Physiotherapy in Managing Symptomatology in Gambling Disorder Patients: A Systematic Review. Healthcare. 2023; 11(14):2055. https://doi.org/10.3390/healthcare11142055
Chicago/Turabian StyleCarrascosa-Arteaga, Pablo, Remedios López-Liria, Daniel Catalán-Matamoros, and Patricia Rocamora-Pérez. 2023. "Effectiveness of Physiotherapy in Managing Symptomatology in Gambling Disorder Patients: A Systematic Review" Healthcare 11, no. 14: 2055. https://doi.org/10.3390/healthcare11142055
APA StyleCarrascosa-Arteaga, P., López-Liria, R., Catalán-Matamoros, D., & Rocamora-Pérez, P. (2023). Effectiveness of Physiotherapy in Managing Symptomatology in Gambling Disorder Patients: A Systematic Review. Healthcare, 11(14), 2055. https://doi.org/10.3390/healthcare11142055