



Effectiveness of Digital Physiotherapy Practice Compared to Usual Care in Long COVID Patients: A Systematic Review
 ,
,  ,
,  and
and
Abstract
1. Introduction
2. Materials and Methods
2.1. Identification Data Sources and Search Strategy
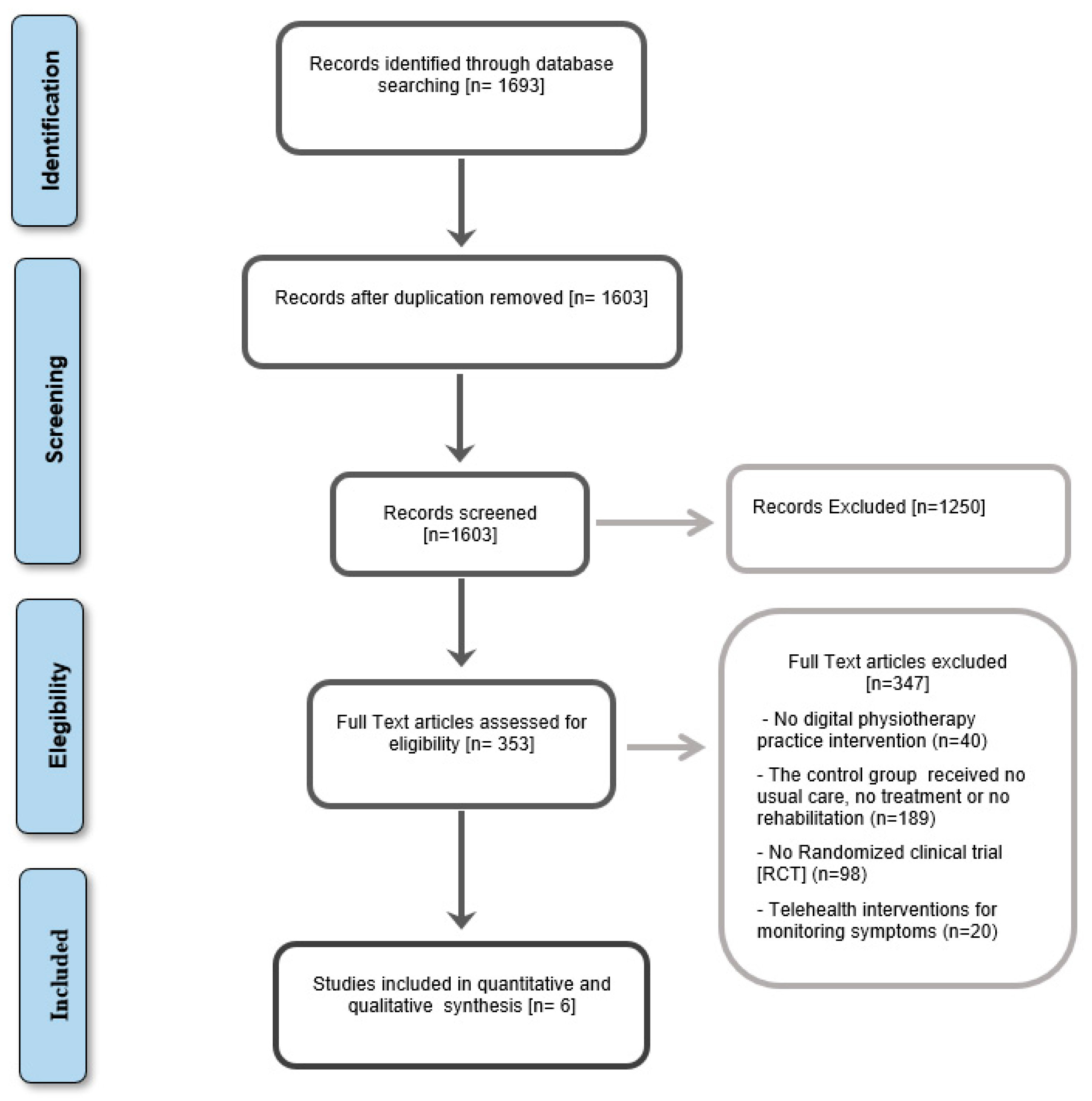
2.2. Study Selection
- Patients:
- Intervention:
- Comparison:
- Outcomes:
- Study Design:
2.3. Data Extraction
2.4. Evaluation of Methodological Quality and Risk of Bias
2.5. Data Synthesis and Analysis
3. Results
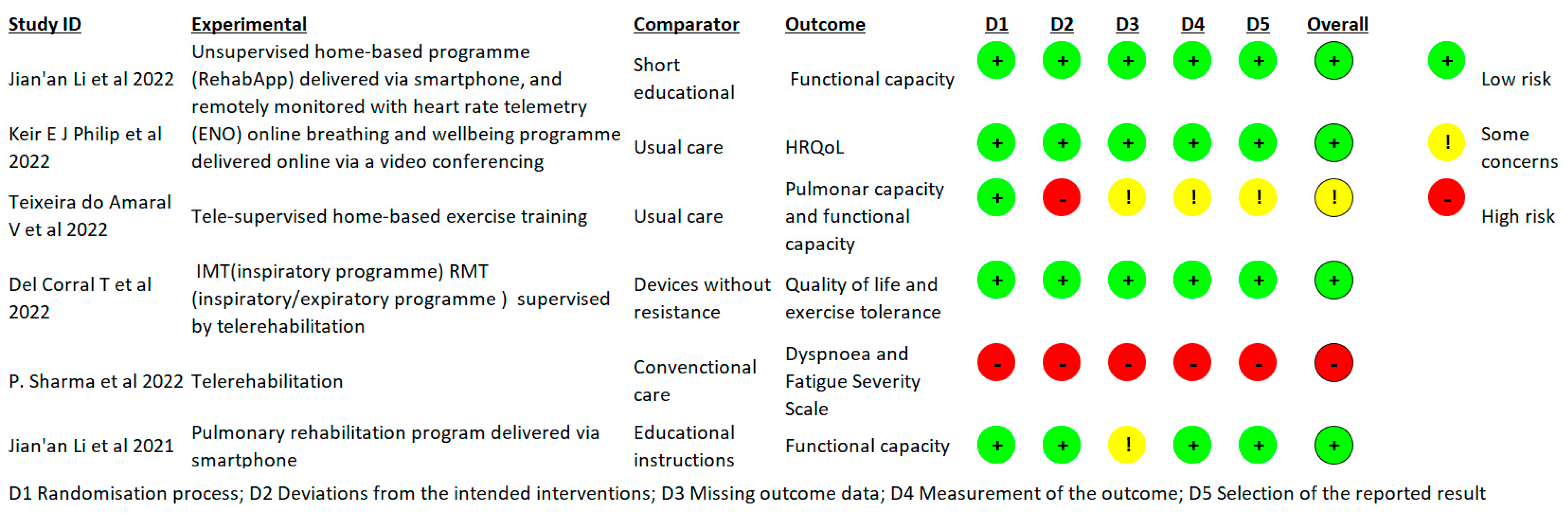
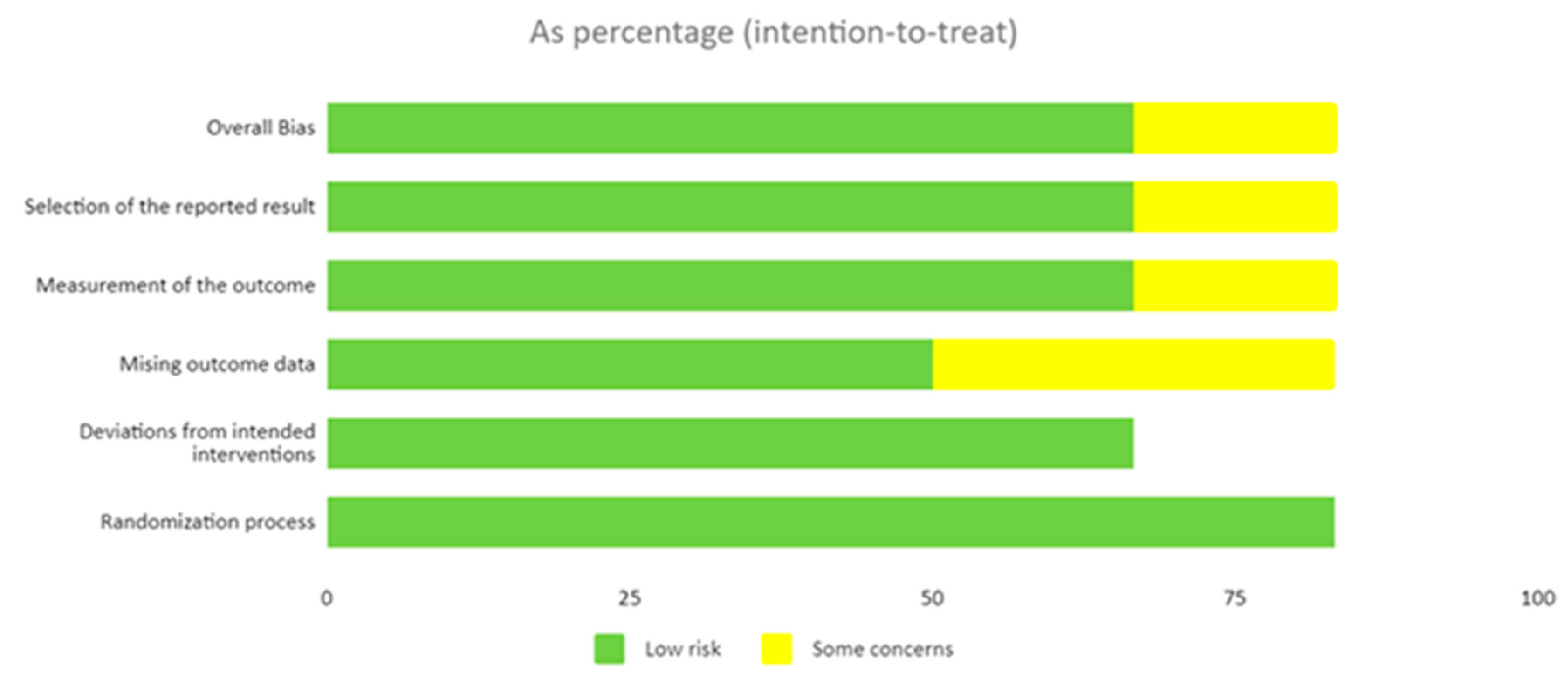
3.1. Risk of Bias and Methodological Quality
3.2. Characteristics of the Included Trials
3.2.1. Interventions
3.2.2. Outcomes
3.2.3. Results of Articles
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A


| Database | Search Terms |
|---|---|
| MEDLINE (n = 1648); PeDro (n = 2); Trip database (n = 0); Cochrane (n = 28) Google Schollar (n = 3); Embase (n = 6); CINAHL/EBSCO (n = 1); Scopus (n = 5) NICE (n = 0) Prospero (n = 0) | (“Long COVID” or “post COVID-19” or “persistent COVID syndrome”) AND (“Telemedicine” OR “Telerehabilitation” OR Digital Physiotherapy Practice”) |
References
- Coronavirus Disease (COVID-19): Post COVID-19 Condition. Available online: https://www.who.int/news-room/questions-and-answers/item/coronavirus-disease-(covid-19)-post-covid-19-condition (accessed on 15 June 2023).
- NHS England. National Commissioning Guidance for Post COVID Services. Available online: https://www.england.nhs.uk/publication/national-commissioning-guidance-for-post-covid-services/ (accessed on 15 June 2023).
- Afecciones Persistentes Al COVID-19 Y Afecciones Posteriores Al COVID-19|CDC. Available online: https://espanol.cdc.gov/coronavirus/2019-ncov/long-term-effects/index.html (accessed on 11 January 2023).
- Long COVID or Post-COVID Conditions|CDC. Available online: https://www.cdc.gov/coronavirus/2019-ncov/long-term-effects/index.html (accessed on 11 January 2023).
- Titler, M.G. The Evidence for Evidence-Based Practice Implementation. In Patient Safety and Quality: An Evidence-Based Handbook for Nurses; Agency for Healthcare Research and Quality: Rockville, MD, USA, 2008. [Google Scholar]
- Matriz-Eisenhower.Jpg (560 × 397). Available online: https://images.squarespace-cdn.com/content/v1/5538a145e4b0a3d5e6f58f96/1519291451739-RCFXNB5TFUGUSNBHOV9O/ke17ZwdGBToddI8pDm48kF4-X2XhqtJN7c5IlWAn_IRZw-zPPgdn4jUwVcJE1ZvWQUxwkmyExglNqGp0IvTJZUJFbgE-7XRK3dMEBRBhUpxctm9o8f6K7MioOda3A72qPDwAxCSbfak35Bet1U2ds-JcwNCOzjT0vX_uiFCjGD4/matriz-eisenhower.jpg?format=750w (accessed on 4 December 2020).
- Clinical Management of Severe Acute Respiratory Infection when Novel Coronavirus (2019-nCoV) Infection is Suspected: Interim Guidance. 28 January 2020. Available online: https://apps.who.int/iris/handle/10665/330893 (accessed on 5 May 2022).
- WHO. Report of the WHO-China Joint Mission on Coronavirus Disease 2019 (COVID-19). Available online: https://www.Who.Int/Publications-Detail/Report-of-the-Who-China-Joint-Mission-on-Coronavirus-Disease-2019-(Covid-19) (accessed on 21 May 2020).
- Coronavirus » Post-COVID Syndrome (Long COVID). Available online: https://www.england.nhs.uk/coronavirus/post-covid-syndrome-long-covid/ (accessed on 14 June 2023).
- COVID.gov—What Is Long COVID. Available online: https://www.covid.gov/longcovid/definitions (accessed on 14 June 2023).
- Prevalence of Ongoing Symptoms Following Coronavirus (COVID-19) Infection in the UK—Office for National Statistics. Available online: https://www.ons.gov.uk/peoplepopulationandcommunity/healthandsocialcare/conditionsanddiseases/bulletins/prevalenceofongoingsymptomsfollowingcoronaviruscovid19infectionintheuk/1april2021 (accessed on 23 August 2022).
- Hama Amin, B.J.; Kakamad, F.H.; Ahmed, G.S.; Ahmed, S.F.; Abdulla, B.A.; Mohammed, S.H.; Mikael, T.M.; Salih, R.Q.; Ali, R.K.; Salh, A.M.; et al. Post COVID-19 Pulmonary Fibrosis; a Meta-Analysis Study. Ann. Med. Surg. 2022, 77, 103590. [Google Scholar] [CrossRef] [PubMed]
- Harenwall, S.; Heywood-Everett, S.; Henderson, R.; Godsell, S.; Jordan, S.; Moore, A.; Philpot, U.; Shepherd, K.; Smith, J.; Bland, A.R. Post-COVID-19 Syndrome: Improvements in Health-Related Quality of Life Following Psychology-Led Interdisciplinary Virtual Rehabilitation. J. Prim. Care Community Health 2021, 12, 215013192110676. [Google Scholar] [CrossRef] [PubMed]
- Sivan, M.; Taylor, S. NICE Guideline on Long Covid. BMJ 2020, 371, m4938. [Google Scholar] [CrossRef] [PubMed]
- Report of The Wcpt/Inptra Digital Physical Therapy Practice Task Force; WCPT: Chicago, IL, USA, 2020.
- Turan, Z.; Topaloglu, M.; Ozyemisci Taskiran, O. Is Tele-Rehabilitation Superior to Home Exercise Program in COVID-19 Survivors Following Discharge from Intensive Care Unit?—A Study Protocol of a Randomized Controlled Trial. Physiother. Res. Int. 2021, 26, e1920. [Google Scholar] [CrossRef]
- Besnier, F.; Bérubé, B.; Malo, J.; Gagnon, C.; Grégoire, C.-A.A.; Juneau, M.; Simard, F.; L’Allier, P.; Nigam, A.; Iglésies-Grau, J.; et al. Cardiopulmonary Rehabilitation in Long-COVID-19 Patients with Persistent Breathlessness and Fatigue: The COVID-Rehab Study. Int. J. Environ. Res. Public Health 2022, 19, 4133. [Google Scholar] [CrossRef]
- Rogante, M.; Grigioni, M.; Cordella, D.; Giacomozzi, C. Ten Years of Telerehabilitation: A Literature Overview of Technologies and Clinical Applications. NeuroRehabilitation 2010, 27, 287–304. [Google Scholar] [CrossRef]
- Seid, A.A.; Aychiluhm, S.B.; Mohammed, A.A. Effectiveness and Feasibility of Telerehabilitation in Patients with COVID-19: A Systematic Review and Meta-Analysis. BMJ Open 2022, 12, e063961. [Google Scholar] [CrossRef]
- Fugazzaro, S.; Contri, A.; Esseroukh, O.; Kaleci, S.; Croci, S.; Massari, M.; Facciolongo, N.C.; Besutti, G.; Iori, M.; Salvarani, C.; et al. Rehabilitation Interventions for Post-Acute COVID-19 Syndrome: A Systematic Review. Int. J. Environ. Res. Public Health 2022, 19, 5185. [Google Scholar] [CrossRef]
- Huang, J.; Fan, Y.; Zhao, K.; Yang, C.; Zhao, Z.; Chen, Y.; Yang, J.; Wang, T.; Qu, Y. Do Patients with and Survivors of COVID-19 Benefit from Telerehabilitation? A Meta-Analysis of Randomized Controlled Trials. Front. Public Health 2022, 10, 954754. [Google Scholar] [CrossRef]
- Janjua, S.; Banchoff, E.; Threapleton, C.J.D.; Prigmore, S.; Fletcher, J.; Disler, R.T. Digital Interventions for the Management of Chronic Obstructive Pulmonary Disease. Cochrane Database Syst. Rev. 2021, 4, CD013246. [Google Scholar] [CrossRef]
- Zischke, C.; Simas, V.; Hing, W.; Milne, N.; Spittle, A.; Pope, R. The Utility of Physiotherapy Assessments Delivered by Telehealth: A Systematic Review. J. Glob. Health 2021, 11, 04072. [Google Scholar] [CrossRef]
- Handbook Integrated Care; Amelung, V., Stein, V., Goodwin, N., Balicer, R., Nolte, E., Suter, E., Eds.; Springer International Publishing: Cham, Switzerland, 2017. [Google Scholar] [CrossRef]
- McLean, S.; Nurmatov, U.; Liu, J.L.Y.; Pagliari, C.; Car, J.; Sheikh, A. Telehealthcare for Chronic Obstructive Pulmonary Disease: Cochrane Review and Meta-Analysis. Br. J. Gen. Pract. 2012, 62, e739–e749. [Google Scholar] [CrossRef]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.A.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA Statement for Reporting Systematic Reviews and Meta-Analyses of Studies That Evaluate Health Care Interventions: Explanation and Elaboration. PLoS Med. 2009, 6, e1000100. [Google Scholar] [CrossRef]
- Thomas, J.; Kneale, D.; McKenzie, J.E.; Brennan, S.E.; Bhaumik, S. Determining the Scope of the Review and the Questions It Will Address. In Cochrane Handbook for Systematic Reviews of Interventions; Wiley: Hoboken, NJ, USA, 2019; pp. 13–31. [Google Scholar] [CrossRef]
- Emergency Use ICD Codes for COVID-19 Disease Outbreak. Available online: https://www.who.int/standards/classifications/classification-of-diseases/emergency-use-icd-codes-for-covid-19-disease-outbreak (accessed on 11 January 2023).
- Policy Statement: Description of Physical Therapy|World Physiotherapy. Available online: https://world.physio/policy/ps-descriptionPT (accessed on 11 January 2023).
- Verhagen, E.; Engbers, L. The Physical Therapist’s Role in Physical Activity Promotion. Br. J. Sports Med. 2008, 43, 99–101. [Google Scholar] [CrossRef]
- de Morton, N.A. The PEDro Scale Is a Valid Measure of the Methodological Quality of Clinical Trials: A Demographic Study. Aust. J. Physiother. 2009, 55, 129–133. [Google Scholar] [CrossRef]
- Escala PEDro—PEDro. Available online: https://pedro.org.au/spanish/resources/pedro-scale/ (accessed on 11 January 2023).
- Manual Cochrane de Revisiones Sistemáticas de Intervenciones|Cochrane Training. Available online: https://training.cochrane.org/es/manual-cochrane-de-revisiones-sistemáticas-de-intervenciones (accessed on 26 January 2023).
- Cumpston, M.; Li, T.; Page, M.J.; Chandler, J.; Welch, V.A.; Higgins, J.P.; Thomas, J. Updated Guidance for Trusted Systematic Reviews: A New Edition of the Cochrane Handbook for Systematic Reviews of Interventions. Cochrane Database Syst. Rev. 2019, 10, ED000142. [Google Scholar] [CrossRef]
- Sterne, J.A.C.; Savović, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.Y.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2: A Revised Tool for Assessing Risk of Bias in Randomised Trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef]
- Yepes-Nuñez, J.J.; Urrútia, G.; Romero-García, M.; Alonso-Fernández, S. Declaración PRISMA 2020: Una Guía Actualizada Para La Publicación de Revisiones Sistemáticas. Rev. Española Cardiol. 2021, 74, 790–799. [Google Scholar] [CrossRef]
- Li, J.; Xia, W.; Zhan, C.; Liu, S.; Yin, Z.; Wang, J.; Chong, Y.; Zheng, C.; Fang, X.; Cheng, W.; et al. A Telerehabilitation Programme in Post-Discharge COVID-19 Patients (TERECO): A Randomised Controlled Trial. Thorax 2022, 77, 697–706. [Google Scholar] [CrossRef]
- Philip, K.E.J.; Owles, H.; McVey, S.; Pagnuco, T.; Bruce, K.; Brunjes, H.; Banya, W.; Mollica, J.; Lound, A.; Zumpe, S.; et al. An Online Breathing and Wellbeing Programme (ENO Breathe) for People with Persistent Symptoms Following COVID-19: A Parallel-Group, Single-Blind, Randomised Controlled Trial. Lancet Respir. Med. 2022, 10, 851–862. [Google Scholar] [CrossRef]
- Teixeira Do Amaral, V.; Viana, A.A.; Heubel, A.D.; Linares, S.N.; Martinelli, B.; Witzler, P.H.C.; Orikassa de Oliveira, G.Y.; Zanini, G.D.S.; Borghi Silva, A.; Mendes, R.G.; et al. Cardiovascular, Respiratory, and Functional Effects of Home-Based Exercise Training after COVID-19 Hospitalization. Med. Sci. Sports Exerc. 2022, 54, 1795–1803. [Google Scholar] [CrossRef] [PubMed]
- del Corral, T.; Garrido, R.F.; Plaza-Manzano, G.; Fernández-de-las-Peñas, C.; Navarro-Santana, M.; López-de-Uralde-Villanueva, I. Home-Based Respiratory Muscle Training on Quality of Life and Exercise Tolerance in Long-Term Post-COVID-19: Randomized Controlled Trial. Ann. Phys. Rehabil. Med. 2022, 66, 101709. [Google Scholar] [CrossRef] [PubMed]
- Sharma, P.; Goswami, S.K. Pulmonary Tele-Rehabilitation in Patients (Post COVID-19) With Respiratory Complications: A Randomized Controlled Trial. Indian J. Physiother. Occup. Ther. 2022, 16, 182–189. [Google Scholar] [CrossRef]
- Li, J.; Xia, W.; Zhan, C.; Liu, S.; Yin, Z.; Wang, J.; Chong, Y.; Zheng, C.; Fang, X.; Cheng, W.; et al. Effectiveness of a Telerehabilitation Program for COVID-19 Survivors (TERECO) on Exercise Capacity, Pulmonary Function, Lower Limb Muscle Strength, and Quality of Life: A Randomized Controlled Trial. medRxiv 2021. [Google Scholar] [CrossRef]
- Day, S.J.; Altman, D.G. Statistics Notes: Blinding in Clinical Trials and Other Studies. BMJ Br. Med. J. 2000, 321, 504. [Google Scholar] [CrossRef]
- Escrig Sos, V.J.; Llueca Abella, J.A.; Granel Villach, L.; Bellver Oliver, M. Meta-Analysis: A Basic Way To Understand And Interpret Your Evidence. Rev. Senol. Y Patol. Mamar. 2021, 34, 44–51. [Google Scholar] [CrossRef]
- Vieira, A.G.D.S.; Pinto, A.C.P.N.; Garcia, B.M.S.P.; Eid, R.A.C.; Mól, C.G.; Nawa, R.K. Telerehabilitation Improves Physical Function and Reduces Dyspnoea in People with COVID-19 and Post-COVID-19 Conditions: A Systematic Review. J. Physiother. 2022, 68, 90–98. [Google Scholar] [CrossRef]
- Cashin, A.G.; McAuley, J.H. Clinimetrics: Physiotherapy Evidence Database (PEDro) Scale. J. Physiother. 2020, 66, 59. [Google Scholar] [CrossRef]
- Estebanez-Pérez, M.-J.; Pastora-Bernal, J.-M.; Martín-Valero, R. The Effectiveness of a Four-Week Digital Physiotherapy Intervention to Improve Functional Capacity and Adherence to Intervention in Patients with Long COVID-19. Int. J. Environ. Res. Public Health 2022, 19, 9566. [Google Scholar] [CrossRef]
- Carson, G.; Carson, G.; Sigfrid, L.; Olliaro, P.; Norton, A.; Paparella, G.; Matulevics, R.; Gillesen, A.; Horby, P.; Hastie, C.; et al. Research Priorities for Long Covid: Refined through an International Multi-Stakeholder Forum. BMC Med. 2021, 19, 84. [Google Scholar] [CrossRef]
- Crook, H.; Raza, S.; Nowell, J.; Young, M.; Edison, P. Long Covid—Mechanisms, Risk Factors, and Management. BMJ 2021, 374, n1648. [Google Scholar] [CrossRef]
- Day, H.L.S. Exploring Online Peer Support Groups for Adults Experiencing Long COVID in the United Kingdom: Qualitative Interview Study. J. Med. Internet Res. 2022, 24, e37674. [Google Scholar] [CrossRef]
- Alwan, N.A. The Road to Addressing Long Covid. Science 2021, 373, 491–493. [Google Scholar] [CrossRef]
- Hoaas, H.; Andreassen, H.K.; Lien, L.A.; Hjalmarsen, A.; Zanaboni, P. Adherence and Factors Affecting Satisfaction in Long-Term Telerehabilitation for Patients with Chronic Obstructive Pulmonary Disease: A Mixed Methods Study EHealth/ Telehealth/ Mobile Health Systems. BMC Med. Inform. Decis. Mak. 2016, 16, 26. [Google Scholar] [CrossRef]
- Peretti, A.; Amenta, F.; Tayebati, S.K.; Nittari, G.; Mahdi, S.S. Telerehabilitation: Review of the State-of-the-Art and Areas of Application. JMIR Rehabil. Assist. Technol. 2017, 4, e7. [Google Scholar] [CrossRef]
- Groenveld, T.; Achttien, R.; Smits, M.; de Vries, M.; van Heerde, R.; Staal, B.; van Goor, H.; Steemers, B.; Brink, L.; van den Rijk, T.; et al. Feasibility of Virtual Reality Exercises at Home for Post–COVID-19 Condition: Cohort Study. JMIR Rehabil. Assist. Technol. 2022, 9, e36836. [Google Scholar] [CrossRef]
- Pallavicini, F.; Pepe, A.; Mantovani, F. The Effects of Playing Video Games on Stress, Anxiety, Depression, Loneliness, and Gaming Disorder During the Early Stages of the COVID-19 Pandemic: PRISMA Systematic Review. Cyberpsychol. Behav. Soc. Netw. 2022, 25, 334–354. [Google Scholar] [CrossRef]
- Adamidi, E.S.; Mitsis, K.; Nikita, K.S. Artificial Intelligence in Clinical Care amidst COVID-19 Pandemic: A Systematic Review. Comput. Struct. Biotechnol. J. 2021, 19, 2833–2850. [Google Scholar] [CrossRef]
- Connor, J.; Madhavan, S.; Mokashi, M.; Amanuel, H.; Johnson, N.R.; Pace, L.E.; Bartz, D. Health Risks and Outcomes That Disproportionately Affect Women during the COVID-19 Pandemic: A Review. Soc. Sci. Med. 2020, 266, 113364. [Google Scholar] [CrossRef]
- Kumar, G.N.P.; Urs, A.N.R.; Undi, M.; Bakkannavar, S.M. Online Viva Voce as a Formative Assessment Method in Forensic Medicine during COVID-19 Pandemic. J. Educ. Health Promot. 2022, 11, 160. [Google Scholar] [CrossRef]
- Bernal-Utrera, C.; Montero-Almagro, G.; Anarte-Lazo, E.; Gonzalez-Gerez, J.J.; Rodriguez-Blanco, C.; Saavedra-Hernandez, M. Therapeutic Exercise Interventions through Telerehabilitation in Patients with Post COVID-19 Symptoms: A Systematic Review. J. Clin. Med. 2022, 11, 7521. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}

| Jian’an Li et al., 2022 [37] | Keir E J Philip et al., 2022 [38] | Teixeira do Amaral V et al., 2022 [39] | Del Corral T et al., 2022 [40] | P. Sharma et al., 2022 [41] | Jian’an Li et al., 2021 [42] | |
|---|---|---|---|---|---|---|
| Eligibility criteria | Y | Y | Y | Y | Y | Y |
| Randomization | Y | Y | Y | Y | Y | Y |
| Allocation concealed | Y | Y | N | Y | N | Y |
| Baseline comparability | Y | Y | Y | Y | N | Y |
| Subject blinding | N | N | N | Y | N | N |
| Therapist blinding | N | N | N | Y | N | N |
| Evaluator blinding | Y | Y | Y | Y | Y | Y |
| Adequate follow-up | Y | Y | N | Y | N | N |
| Intention to treat | Y | Y | N | Y | N | Y |
| Comparison between groups | Y | Y | Y | Y | N | Y |
| Point estimates and variability | Y | Y | Y | Y | N | Y |
| Total PeDro Score | 8 | 8 | 5 | 9 | 2 | 7 |
| Author [Year] | Population | Participants [n], Type of Evidence | PeDro Score, Risk of Bias | Intervention | Outcome Measure | Intervention Duration [Weeks] | Follow-Up [Month] | Results |
|---|---|---|---|---|---|---|---|---|
| Jian’an Li et al., 2022 [37] | Long COVID Patients |
| 8/10—Low |
|
| 6 | 28 | TERECO program was superior to control group with regard to functional exercise capacity, LMS and physical HRQOL. The effects could be maintained for a period of 7 months. No differentiation was found in pulmonary function. Improvements were found in the physical component of the SF-12 scale, with effects at post-treatment and follow-up. |
| Keir E J Philip et al., 2022 [38] | Long COVID Patients |
| 8/10—Low |
|
| 6 | -- | Improvements in the MHC of quality of life were observed compared to usual care. VAS for breathlessness (running) favored ENO Breathe participation. In the secondary outcomes, no statistically significant differences were observed between the groups. Thematic analysis of participants’ perceptions of the intervention identified three key themes: (1) symptom improvement; (2) the sense that the program complemented standard care; and (3) the particular suitability of singing and music to address their needs. Mind, body, and music-focused practices could influence participants’ recovery. |
| Teixeira do Amaral V et al., 2022 [39] | Long COVID Patients |
| 5/10—Some Concerns |
|
| 12 | -- | Both the intervention and control groups increased (p < 0.001) forced vital capacity (absolute and % of predicted), forced expiratory volume in the first second (absolute and % of predicted) and hand grip strength during follow-up. However, only the intervention group reduced carotid–femoral pulse wave velocity and increased (p < 0.05) resting oxygen saturation, mean inspiratory pressure, mean expiratory pressure and % of predicted mean expiratory pressure during follow-up. No significant changes were observed in any other variable during follow-up. |
| ||||||||
| Del Corral T et al., 2022 [40] | Long COVID Patients |
| 9/10—Low |
|
| 8 | -- | Statistically significant improvement in quality of life, but not in exercise tolerance, in the two training groups compared to the sham groups. The two training groups developed a large statistically significant increase in inspiratory muscle strength and endurance and lower extremity muscle strength compared to the two sham groups. Expiratory muscle strength and peak expiratory flow showed a large, statistically significant increase in the training group. |
| ||||||||
| P. Sharma et al., 2022 [41] | Long COVID Patients |
| 2/10—High |
|
| 6 | -- | Results showed that there was a statistically significant difference between IG (MBDS) and CG (MBDS) (p = 0.005605 and p = 0.01121) and statistically significant difference was found between IG (VAS-F) and CG (VAS-F) (p = 0.01818 and p = 0.036359). |
| ||||||||
| Jian’an Li et al., 2021 [42] | Long COVID Patients |
| 7/10—Low |
|
| 6 | 28 | The adjusted between-group difference in change in 6-MWD from baseline was 65.45 m at post-treatment and 68.62 m at follow-up. Treatment effects for LMS were 20.12 s post-treatment and 22.23 s at follow-up. No group differences were found for lung function apart from post-treatment MVV. Increase in SF-12 PCS was greater in the TERECO group, with treatment effects estimated at 3.79 at post-treatment and 2.69 at follow-up. No significant between-group differences were found for improvements in SF-12 in mental component. At post-treatment, 90.4% endorsed a favorable outcome for mMRC dyspnea in the TERECO group vs. 61.7% in control. |
| Intervention | Authors and References | Number of Articles | Participants (n), | Low Risk of Bias (% of Total Articles by Intervention) | Risk of Bias: Some Concerns (% of Total Articles by Intervention) | High Risk of Bias (% of Total Articles by Intervention) |
|---|---|---|---|---|---|---|
| Tele-supervised home-based exercise training | Jian’an Li et al., 2022 [37]/Keir E J Philip et al., 2022 [38]/Teixeira do Amaral V et al., 2022 [39]/Del Corral T et al., 2022 [40] | 4 | 233 | 3 (75%) | 1 (25%) | - |
| Unsupervised home-based program | Jian’an Li et al., 2021 [42]/P. Sharma et al., 2022 [41] | 2 | 74 | 1 (50%) | - | 1 (50%) |
| Short educationalinstructions | Jian’an Li et al., 2022 [37]/Jian’an Li et al., 2021 [42] | 2 | 121 | 2 (100%) | - | - |
| Usual care | Keir E J Philip et al., 2022 [38]/Teixeira do Amaral V et al., 2022 [39]/P. Sharma et al., 2022 [41] | 3 | 111 | 1 (33.33%) | 1 (33.33%) | 1 (33.33%) |
| Outcomes | Authors and References | Number of Articles | Participants (n) | Low Risk of Bias (% of Total Articles by Outcome) | Risk of Bias: Some Concerns (% of Total Articles by Outcome) | High Risk of Bias (% of Total Articles by Outcome) |
|---|---|---|---|---|---|---|
| Pulmonary capacity | Jian’an Li et al., 2022 [37]/Keir E J Philip et al., 2022 [38]/Teixeira do Amaral V et al., 2022 [39]/Del Corral T et al., 2022 [40]/Jian’an Li et al., 2021 [42] | 5 | 510 | 4 (80%) | 1 (20%) | - |
| HRQoL (Quality of Life) | Jian’an Li et al., 2022 [37]/Keir E J Philip et al., 2022 [38]/Del Corral T et al., 2022 [40]/Jian’an Li et al., 2021 [42] | 4 | 478 | 4 (100%) | - | - |
| Dyspnea | Jian’an Li et al., 2022 [37]/Keir E J Philip et al., 2022 [38]/P. Sharma et al., 2022 [41]/Jian’an Li et al., 2021 [42] | 4 | 420 | 3 (75%) | - | 1 (25%) |
| Functional capacity | Jian’an Li et al., 2022 [37]/Teixeira do Amaral V et al., 2022 [39]/Del Corral T et al., 2022 [40]/Jian’an Li et al., 2021 [42] | 4 | 358 | 3 (75%) | 1 (25%) | - |
| Cognitive and psychological status | Keir E J Philip et al., 2022 [38]/Del Corral T et al., 2022 [40] | 2 | 238 | 2 (100%) | - | - |
| Fatigue | P. Sharma et al., 2022 [41] | 1 | 30 | - | - | 1 (100%) |
| Exercise Tolerance | Del Corral T et al., 2022 [40] | 1 | 88 | 1 (100%) | - | - |
| Participants’ experiences | Keir E J Philip et al., 2022 [38] | 1 | 150 | 1 (100%) | - | - |
| Jian’an Li et al., 2022 [37] | Keir E J Philip et al., 2022 [38] | Teixeira do Amaral V et al., 2022 [39] | Del Corral T et al., 2022 [40] | P. Sharma et al., 2022 [41] | Jian’an Li et al., 2021 [42] | |
|---|---|---|---|---|---|---|
| Pulmonary capacity | (+) | (++) | (++) | (++) | (+) | |
| HRQoL (Quality of Life) P (Physical component) M (Mental component) | (++P) (+M) | (+P) (++M) | (++) | (++P) (+M) | ||
| Dyspnea | (+) | (+) | (++) | (+) | ||
| Functional capacity | (++) | (+) | (++) | (++) | ||
| Cognitive and psychological status | (+) | (+) | ||||
| Fatigue | (++) | |||||
| Exercise Tolerance | (+) | |||||
| Cardiovascular function | (++) | |||||
| Participants’ experiences | (+) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Estebanez-Pérez, M.-J.; Martín-Valero, R.; Vinolo-Gil, M.J.; Pastora-Bernal, J.-M. Effectiveness of Digital Physiotherapy Practice Compared to Usual Care in Long COVID Patients: A Systematic Review. Healthcare 2023, 11, 1970. https://doi.org/10.3390/healthcare11131970
Estebanez-Pérez M-J, Martín-Valero R, Vinolo-Gil MJ, Pastora-Bernal J-M. Effectiveness of Digital Physiotherapy Practice Compared to Usual Care in Long COVID Patients: A Systematic Review. Healthcare. 2023; 11(13):1970. https://doi.org/10.3390/healthcare11131970
Chicago/Turabian StyleEstebanez-Pérez, María-José, Rocío Martín-Valero, Maria Jesus Vinolo-Gil, and José-Manuel Pastora-Bernal. 2023. "Effectiveness of Digital Physiotherapy Practice Compared to Usual Care in Long COVID Patients: A Systematic Review" Healthcare 11, no. 13: 1970. https://doi.org/10.3390/healthcare11131970
APA StyleEstebanez-Pérez, M.-J., Martín-Valero, R., Vinolo-Gil, M. J., & Pastora-Bernal, J.-M. (2023). Effectiveness of Digital Physiotherapy Practice Compared to Usual Care in Long COVID Patients: A Systematic Review. Healthcare, 11(13), 1970. https://doi.org/10.3390/healthcare11131970