


Effects of Target Variables on Interpersonal Distance Perception for Young Taiwanese during the COVID-19 Pandemic


Abstract
1. Introduction
2. Methods
2.1. Participants
2.2. Experimental Design
2.3. Experimental Setting
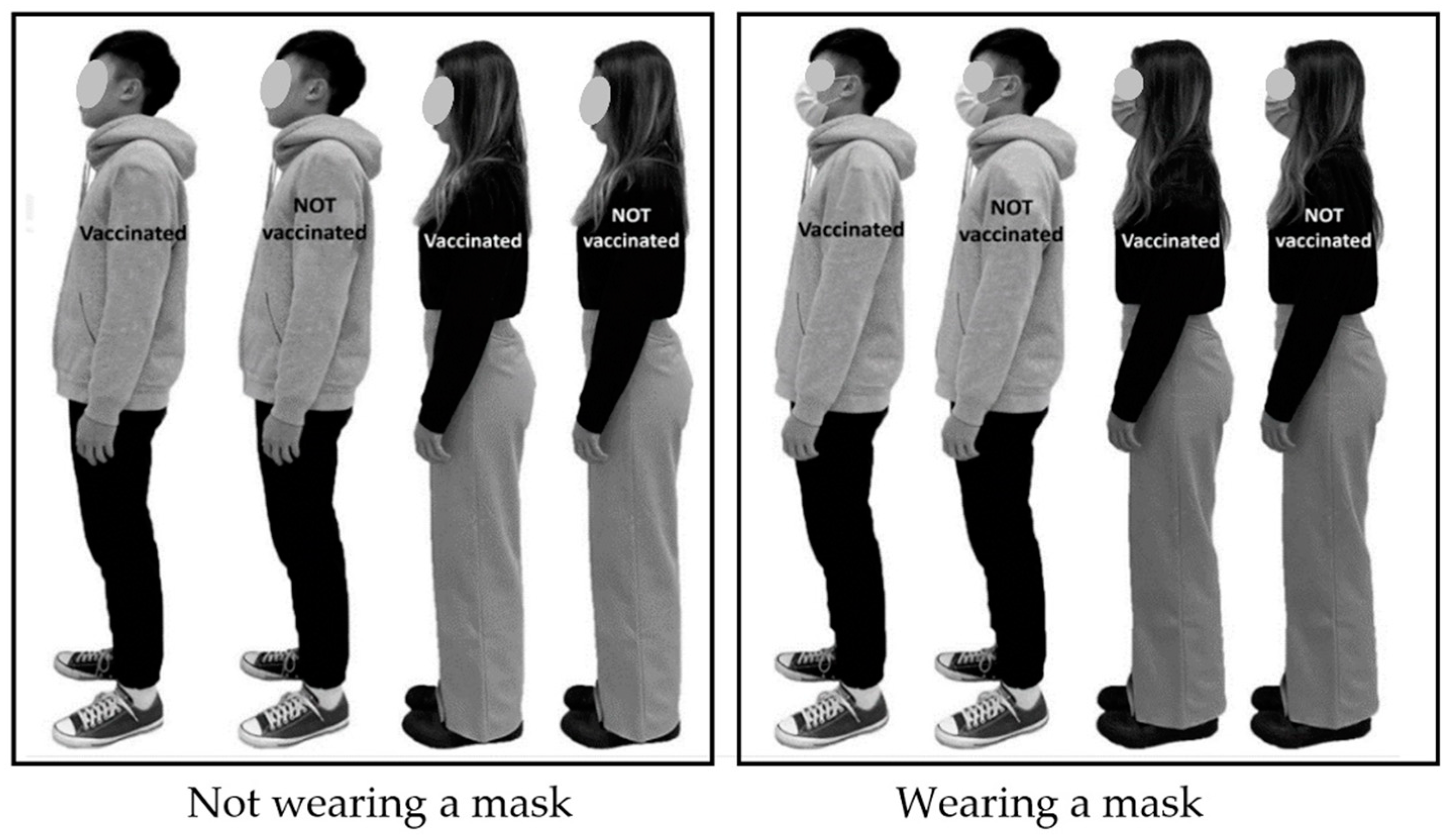
2.4. Targets
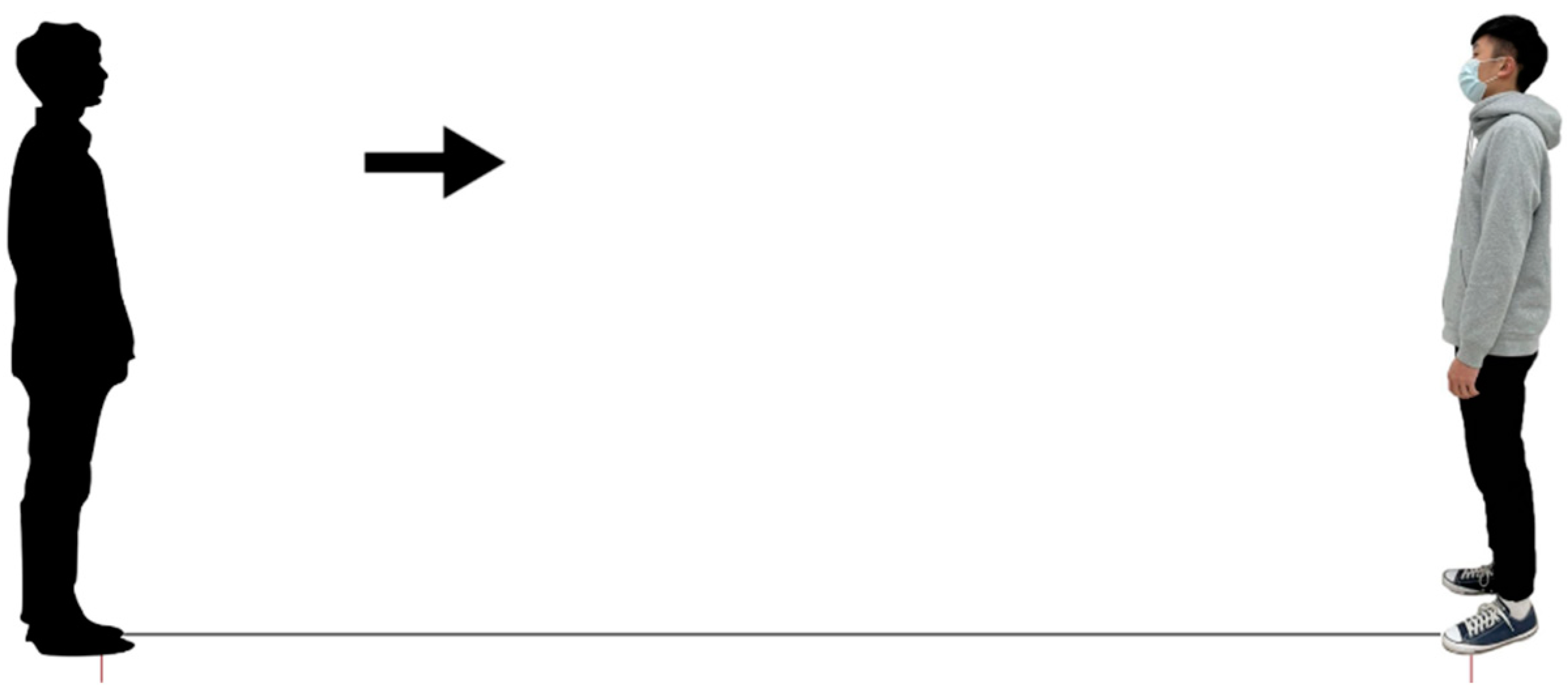
2.5. Procedure
2.6. Statistical Analysis
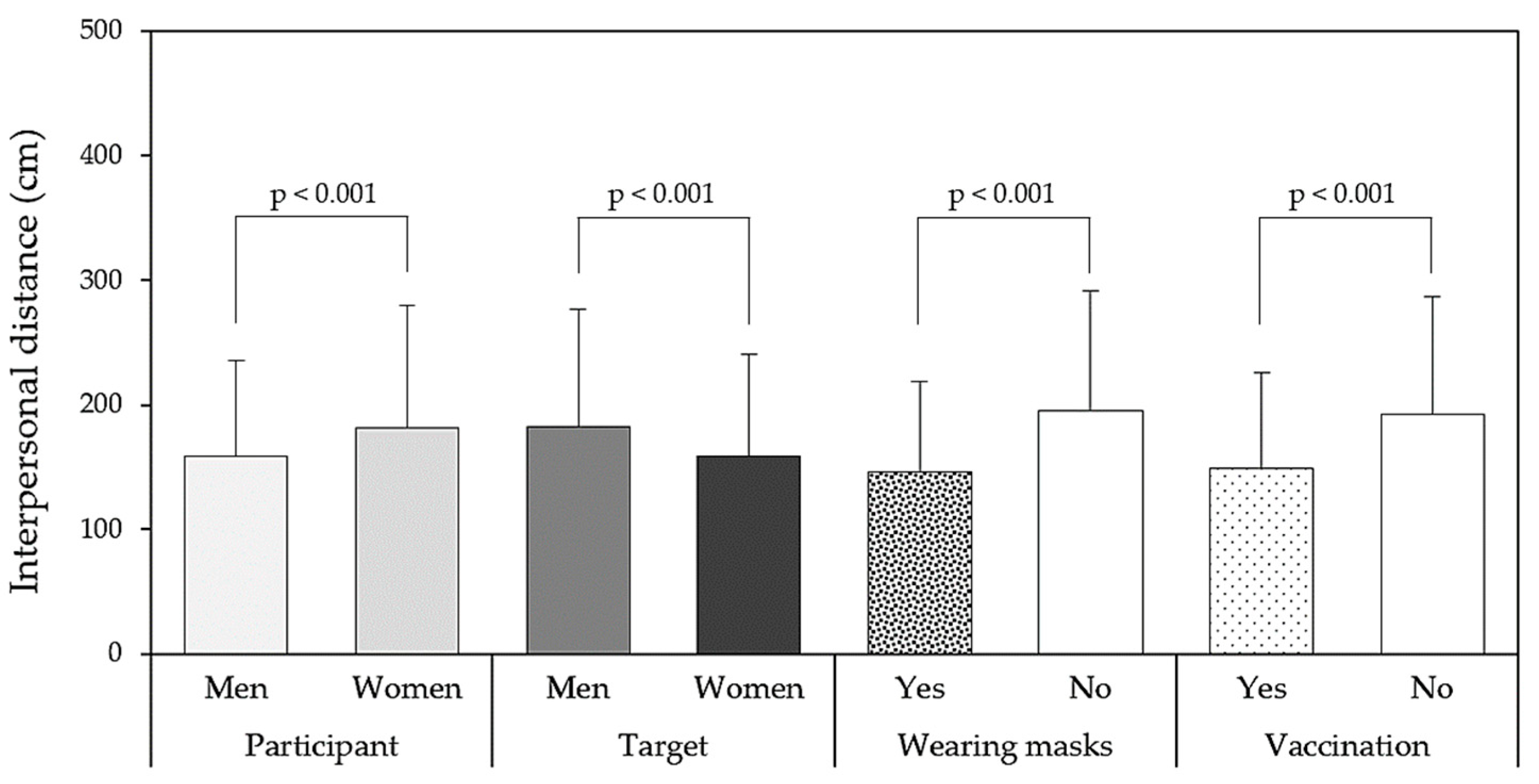
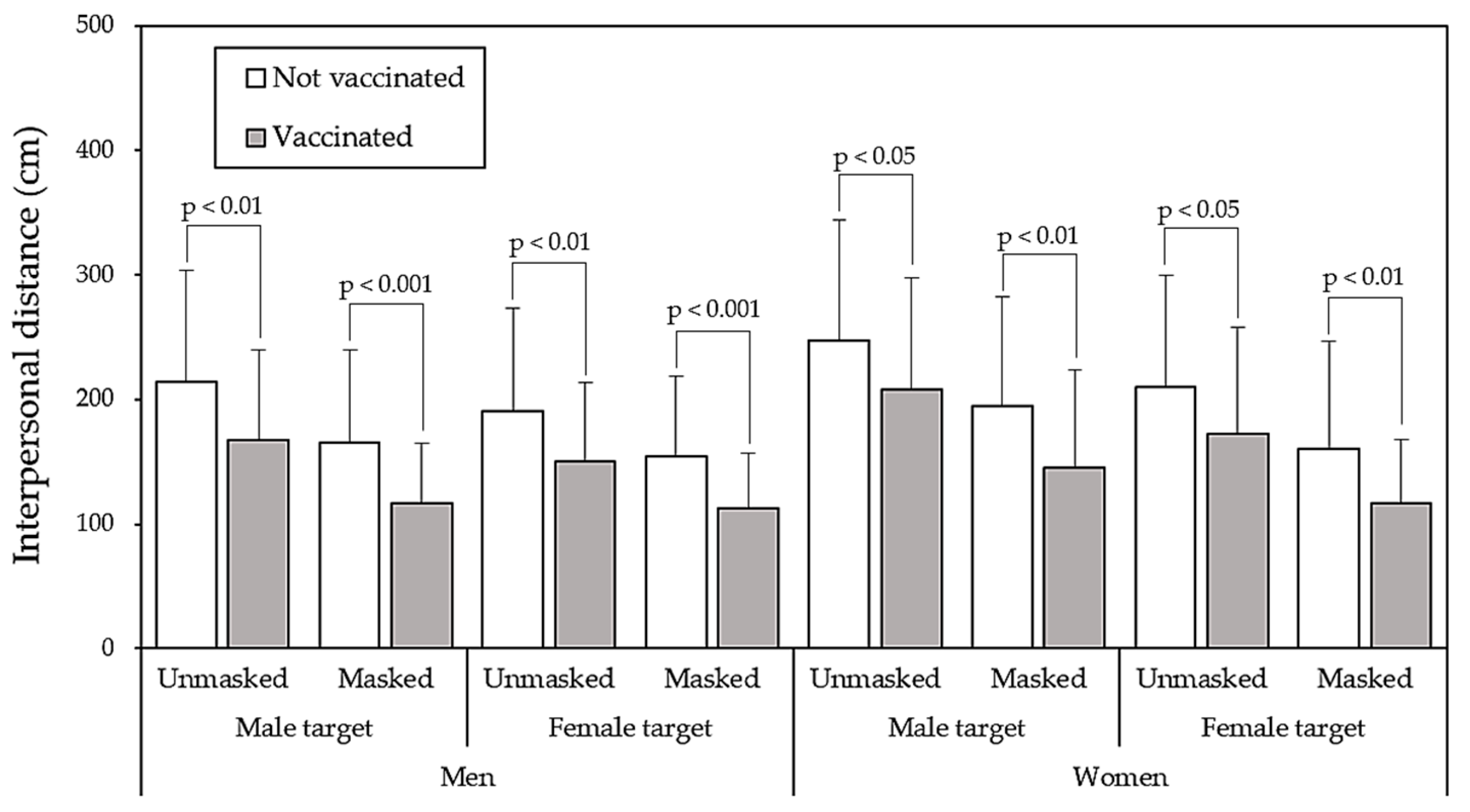
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Biggio, M.; Bisio, A.; Bruno, V.; Garbarini, F.; Bove, M. Wearing a mask shapes interpersonal space during COVID-19 pandemic. Brain Sci. 2022, 12, 682. [Google Scholar] [CrossRef] [PubMed]
- Nerlich, B.; Jaspal, R. Social representations of ‘social distancing’ in response to COVID-19 in the UK media. Curr. Sociol. 2021, 69, 566–583. [Google Scholar] [CrossRef]
- Lee, Y.C.; Chen, Y.L. Influence of wearing surgical mask on interpersonal space perception between Mainland Chinese and Taiwanese people. Front. Psychol. 2021, 12, 692404. [Google Scholar] [CrossRef] [PubMed]
- Sajed, A.; Amgain, K. Corona Virus Disease (COVID-19) outbreak and the strategy for prevention. Eurasian J. Med. Sci. 2020, 2, 1–3. [Google Scholar] [CrossRef]
- Chu, D.K.; Akl, E.A.; Duda, S.; Solo, K.; Yaacoub, S.; Schünemann, H.J. SARS-CoV-2 Systematic Urgent Review Group Effort (SURGE) study authors. Physical distancing, face masks, and eye protection to prevent person-to-person transmission of SARS-CoV-2 and SARS-COV-2: A systematic review and meta-analysis. Lancet 2020, 395, 1973–1987. [Google Scholar] [CrossRef]
- Johnson, D.F.; Druce, J.D.; Birch, C.; Grayson, M.L. A quantitative assessment of the efficacy of surgical and N95 masks to filter influenza virus in patients with acute influenza infection. Clin. Infect. Dis. 2009, 49, 275–277. [Google Scholar] [CrossRef] [PubMed]
- Bae, S.; Kim, M.C.; Kim, J.Y.; Cha, H.H.; Lim, J.S.; Jung, J.; Oh, D.K.; Lee, M.-K.; Choi, S.-H.; Sung, M.; et al. Effectiveness of surgical and cotton masks in blocking SARS–CoV-2: A controlled comparison in 4 patients. Ann. Intern. Med. 2020, M20, 1342. [Google Scholar] [CrossRef]
- Matuschek, C.; Moll, F.; Fangerau, H.; Fischer, J.C.; Zänker, K.; van Griensven, M.; Schneider, M.; Kindgen-Milles, D.; Knoefel, W.T.; Lichtenberg, A.; et al. Face masks: Benefits and risks during the COVID-19 crisis. Eur. J. Med. Res. 2020, 25, 1–8. [Google Scholar] [CrossRef]
- Brooks, S.K.; Webster, R.K.; Smith, L.E.; Woodland, L.; Wessely, S.; Greenberg, N.; Rubin, G.J. The psychological impact of quarantine and how to reduce it: Rapid review of the evidence. Lancet 2020, 395, 912–920. [Google Scholar] [CrossRef]
- Clemente-Suárez, V.J.; Dalamitros, A.A.; Beltran-Velasco, A.I.; Mielgo-Ayuso, J.; Tornero-Aguilera, J.F. Social and psychophysiological consequences of the COVID-19 pandemic: An extensive literature review. Front. Psychol. 2020, 11, 3077. [Google Scholar] [CrossRef]
- Cartaud, A.; Quesque, F.; Coello, Y. Wearing a face mask against COVID-19 results in a reduction of social distancing. PLoS ONE 2020, 15, e0243023. [Google Scholar] [CrossRef]
- Welsch, R.; Wessels, M.; Bernhard, C.; Thönes, S.; Von Castell, C. Physical distancing and the perception of interpersonal distance in the COVID-19 crisis. Sci. Rep. 2021, 11, 11485. [Google Scholar] [CrossRef] [PubMed]
- Hall, E.T. The Hidden Dimension (Vol. xii); Doubleday & Co.: New York, NY, USA, 1966. [Google Scholar]
- Iachini, T.; Coello, Y.; Frassinetti, F.; Senese, V.P.; Galante, F.; Ruggiero, G. Peripersonal and interpersonal space in virtual and real environments: Effects of gender and age. J. Environ. Psychol. 2016, 45, 154–164. [Google Scholar] [CrossRef]
- Remland, M.S.; Jones, T.S.; Brinkman, H. Interpersonal distance, body orientation, and touch: Effects of culture, gender, and age. J. Soc. Psychol. 1995, 135, 281–297. [Google Scholar] [CrossRef]
- Yu, X.; Xiong, W.; Lee, Y.C. An investigation into interpersonal and peripersonal spaces of Chinese people for different directions and genders. Front. Psychol. 2020, 11, 981. [Google Scholar] [CrossRef]
- Sicorello, M.; Stevanov, J.; Ashida, H.; Hecht, H. Effect of gaze on personal space: A Japanese–German cross-cultural study. J. Cross-Cult. Psychol. 2019, 50, 8–21. [Google Scholar] [CrossRef]
- Sorokowska, A.; Sorokowski, P.; Hilpert, P.; Cantarero, K.; Frackowiak, T.; Ahmadi, K.; Alghraibeh, A.M.; Aryeetey, R.; Bertoni, A.; Bettache, K.; et al. Preferred interpersonal distances: A global comparison. J. Cross-Cult. Psychol. 2017, 48, 577–592. [Google Scholar] [CrossRef]
- Ruggiero, G.; Frassinetti, F.; Coello, Y.; Rapuano, M.; di Cola, A.S.; Iachini, T. The effect of facial expressions on peripersonal and interpersonal spaces. Psychol. Res. 2017, 81, 1232–1240. [Google Scholar] [CrossRef]
- Cartaud, A.; Ruggiero, G.; Ott, L.; Iachini, T.; Coello, Y. Physiological response to facial expressions in peripersonal space determines interpersonal distance in a social interaction context. Front. Psychol. 2018, 9, 657. [Google Scholar] [CrossRef]
- Abney, K. “Containing” tuberculosis, perpetuating stigma: The materiality of N95 respirator masks. Anthropol. S. Afr. 2018, 41, 270–283. [Google Scholar] [CrossRef]
- Burgess, A.; Horii, M. Risk, ritual and health responsibilisation: Japan’s ‘safety blanket’ of surgical face mask-wearing. Sociol. Health Illn. 2012, 34, 1184–1198. [Google Scholar] [CrossRef] [PubMed]
- Kühne, K.; Fischer, M.H.; Jeglinski-Mende, M.A. During the COVID-19 pandemic participants prefer settings with a face mask, no interaction and at a closer distance. Sci. Rep. 2022, 12, 12777. [Google Scholar] [CrossRef] [PubMed]
- Bodas, M.; Adini, B.; Jaffe, E.; Kaim, A.; Peleg, K. Lockdown efficacy in controlling the spread of COVID-19 may be waning due to decline in public compliance, especially among unvaccinated individuals: A cross-sectional study in Israel. Int. J. Environ. Res. Public Health 2022, 19, 4943. [Google Scholar] [CrossRef] [PubMed]
- Huang, Y.Z.; Kuan, C.C. Vaccination to reduce severe COVID-19 and mortality in COVID-19 patients: A systematic review and meta-analysis. Eur. Rev. Med. Pharmacol. Sci. 2022, 26, 1770–1776. [Google Scholar]
- Palamenghi, L.; Barello, S.; Boccia, S.; Graffigna, G. Mistrust in biomedical research and vaccine hesitancy: The forefront challenge in the battle against COVID-19 in Italy. Eur. J. Epidemiol. 2020, 35, 785–788. [Google Scholar] [CrossRef] [PubMed]
- Patterson, N.J.; Paz-Soldan, V.A.; Oberhelman, R.; Moses, L.; Madkour, A.; Miles, T.T. Exploring perceived risk for COVID-19 and its role in protective behavior and COVID-19 vaccine hesitancy: A qualitative study after the first wave. BMC Public Health 2022, 22, 503. [Google Scholar] [CrossRef] [PubMed]
- Lipsitch, M.; Dean, N.E. Understanding COVID-19 vaccine efficacy. Science 2020, 370, 763–765. [Google Scholar] [CrossRef]
- Lin, L.; Zhao, Y.; Chen, B.; He, D. Multiple COVID-19 waves and vaccination effectiveness in the United States. Int. J. Environ. Res. Public Health 2022, 19, 2282. [Google Scholar] [CrossRef]
- Zachreson, C.; Chang, S.L.; Cliff, O.M.; Prokopenko, M. How will mass-vaccination change COVID-19 lockdown requirements in Australia? Lancet Reg. Health West Pac. 2021, 14, 100224. [Google Scholar] [CrossRef]
- Si, R.; Yao, Y.; Zhang, X.; Lu, Q.; Aziz, N. Investigating the links between vaccination against COVID-19 and public attitudes toward protective countermeasures: Implications for public health. Front. Public Health 2021, 9, 702699. [Google Scholar] [CrossRef]
- Chen, M.; Yuan, Y.; Zhou, Y.; Deng, Z.; Zhao, J.; Feng, F.; Zou, H.; Sun, C. Safety of SARS-CoV-2 vaccines: A systematic review and meta-analysis of randomized controlled trials. Infect. Dis. Poverty 2021, 10, 94. [Google Scholar] [CrossRef] [PubMed]
- Mouter, N.; de Ruijter, A.; de Wit, G.A.; Lambooij, M.S.; van Wijhe, M.; van Exel, J.; Kessels, R. “Please, you go first!” preferences for a COVID-19 vaccine among adults in the Netherlands. Soc. Sci. Med. 2022, 292, 114626. [Google Scholar] [CrossRef] [PubMed]
- Blanchard-Rohner, G.; Caprettini, B.; Rohner, D.; Voth, H.J. Impact of COVID-19 and intensive care unit capacity on vaccination support: Evidence from a two-leg representative survey in the United Kingdom. J. Virus Erad. 2021, 7, 100044. [Google Scholar] [CrossRef] [PubMed]
- Katz, M.; Azrad, M.; Glikman, D.; Peretz, A. COVID-19 vaccination compliance and associated factors among medical students during an early phase of vaccination rollout—A survey from Israel. Vaccines 2021, 10, 27. [Google Scholar] [CrossRef] [PubMed]
- Calbi, M.; Langiulli, N.; Ferroni, F.; Montalti, M.; Kolesnikov, A.; Gallese, V.; Umiltà, M.A. The consequences of COVID-19 on social interactions: An online study on face covering. Sci. Rep. 2021, 11, 2601. [Google Scholar] [CrossRef]
- Hayduk, L.A. Personal space: Where we now stand. Psychol. Bull. 1983, 94, 293. [Google Scholar] [CrossRef]
- Xiong, W.; Phillips, M.; Wang, Z.; Zhang, Y.; Cheng, H.; Link, B. Stigma and discrimination associated with mental illness and other stigmatizing conditions in China using two cultural-sensitive measures of stigma: Interpersonal distance and occupational restrictiveness. Psychol. Med. 2020, 51, 2804–2813. [Google Scholar] [CrossRef]
- Adams, L.; Zuckerman, D. The effect of lighting conditions on personal space requirements. J. Gen. Psychol. 1991, 118, 335–340. [Google Scholar] [CrossRef]
- Nandrino, J.L.; Ducro, C.; Iachini, T.; Coello, Y. Perception of peripersonal and interpersonal space in patients with restrictive-type anorexia. Eur. Eat. Disord. Rev. 2017, 25, 179–187. [Google Scholar] [CrossRef]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences, 2nd ed.; Erlbaum: Hillsdale, NJ, USA, 1988. [Google Scholar]
- Amodio, E.; Vella, G.; Restivo, V.; Casuccio, A.; Vitale, F. COVID-19 Surveillance Working Group of the University of Palermo, Effectiveness of mRNA COVID-19 vaccination on SARS-CoV-2 infection and COVID-19 in sicily over an eight-month period. Vaccines 2022, 10, 426. [Google Scholar] [CrossRef]
- Rackimuthu, S.; Hasan, M.M.; Bardhan, M.; Essar, M.Y. COVID-19 vaccination strategies and policies in India: The need for further re-evaluation is a pressing priority. Int. J. Health Plann. Manag. 2022, 37, 1847–1850. [Google Scholar] [CrossRef] [PubMed]
- Caplan, M.E.; Goldman, M. Personal space violations as a function of height. J. Soc. Psychol. 1981, 114, 167–171. [Google Scholar] [CrossRef]
- Aliakbari, M.; Faraji, E.; Pourshakibaee, P. Investigation of the proxemic behavior of Iranian professors and university students: Effects of gender and status. J. Pragmat. 2011, 43, 1392–1402. [Google Scholar] [CrossRef]
- Baxter, J.C. Interpersonal spacing in natural settings. Sociometry 1970, 33, 444–456. [Google Scholar] [CrossRef] [PubMed]
- Evans, G.W.; Howard, R.B. Personal space. Psychol. Bull. 1973, 80, 334–344. [Google Scholar] [CrossRef] [PubMed]
- Hecht, H.; Welsch, R.; Viehoff, J.; Longo, M.R. The shape of personal space. Acta Psychol. 2019, 193, 113–122. [Google Scholar] [CrossRef] [PubMed]
- Zhou, C.; Han, M.; Liang, Q.; Hu, Y.H.; Kuai, S.G. A social interaction field model accurately identifies static and dynamic social groupings. Nat. Hum. Behav. 2019, 3, 847–855. [Google Scholar] [CrossRef]
- Yang, Z. An experimental study of Chinese adult space zone. Psychol. Sci. 1988, 2, 24–28. [Google Scholar]
- Wilde, G.J.S. Critical issues in risk homeostasis theory. Risk Anal. 1982, 2, 249–258. [Google Scholar] [CrossRef]
- Sugimura, M.; Chimed-Ochir, O.; Yumiya, Y.; Ohge, H.; Shime, N.; Sakaguchi, T.; Tanaka, J.; Takafuta, T.; Mimori, M.; Kuwabara, M.; et al. The association between wearing a mask and COVID-19. Int. J. Environ. Res. Public Health 2021, 18, 9131. [Google Scholar] [CrossRef]
- Douglas, J.D.M.; McLean, N.; Horsley, C.; Higgins, G.; Douglas, C.M.; Robertson, E. COVID-19: Smoke testing of surgical mask and respirators. Occup. Med. 2020, 70, 556–563. [Google Scholar] [CrossRef] [PubMed]
- Sickbert-Bennett, E.E.; Samet, J.M.; Clapp, P.W.; Chen, H.; Berntsen, J.; Zeman, K.L. Filtration efficiency of hospital face mask alternatives available for use during the COVID-19 pandemic. JAMA Intern. Med. 2020, 180, 1607–1612. [Google Scholar] [CrossRef]
- Xi, J.; Barari, K.; Si, X.A.; Abdollahzadeh Jamalabadi, M.Y.; Park, J.H.; Rein, M. Inspiratory leakage flow fraction for surgical masks with varying gaps and filter materials. Phys. Fluids 2022, 34, 041908. [Google Scholar] [CrossRef]
- Siahaan, A.M.P.; Lubis, M.P.; Dalimunthe, D.A.; Nasution, M.R.; Lubis, H.P.R. Adherence to face mask and social distancing among residents in Medan during the COVID-19 pandemics. Bali Med. J. 2021, 10, 529–533. [Google Scholar] [CrossRef]
- Ganczak, M.; Pasek, O.; Duda–Duma, Ł.; Świstara, D.; Korzeń, M. Use of masks in public places in Poland during SARS-CoV-2 epidemic: A covert observational study. BMC Public Health 2021, 21, 393. [Google Scholar] [CrossRef]
- Sharma, S.K.; Mishra, M.; Mudgal, S. Efficacy of cloth face mask in prevention of novel coronavirus infection transmission: A systematic review and meta-analysis. J. Educ. Health Promot. 2020, 9, 192. [Google Scholar] [CrossRef]
- WHO. World Health Organization, Coronavirus Disease (COVID-19), Masks, Q & A, Newsroom. 2022. Available online: https://www.who.int/news-room/questions-and-answers/item/coronavirus-disease-covid-19-masks (accessed on 1 October 2022).
- Ren, X.; Zhou, J.; Guo, J.; Hao, C.; Zheng, M.; Zhang, R.; Huang, Q.; Yao, X.; Li, R.; Jin, Y. Reinfection in patients with COVID-19: A systematic review. Glo. Health Res. Policy 2022, 7, 12. [Google Scholar] [CrossRef]
- Kroczek, L.O.; Böhme, S.; Mühlberger, A. Face masks reduce interpersonal distance in virtual reality. Sci. Rep. 2022, 12, 2213. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Sources | SS | df | MS | F | p-Value | η2 |
|---|---|---|---|---|---|---|
| Participant sex (PS) | 106,775 | 1 | 106,775 | 15.769 | <0.001 | 0.020 |
| Target sex (TS) | 114,183 | 1 | 114,183 | 16.863 | <0.001 | 0.021 |
| Face mask (FM) | 482,778 | 1 | 482,778 | 71.300 | <0.001 | 0.083 |
| Vaccinated (V) | 379,316 | 1 | 379,316 | 56.020 | <0.001 | 0.067 |
| PS × TS | 19,369 | 1 | 19,369 | 2.860 | 0.091 | 0.004 |
| PS × FM | 7702 | 1 | 7702 | 1.138 | 0.287 | 0.001 |
| PS × V | 170 | 1 | 170 | 0.025 | 0.874 | <0.001 |
| TS × FM | 3972 | 1 | 3972 | 0.587 | 0.444 | 0.001 |
| TS × V | 1307 | 1 | 1307 | 0.193 | 0.661 | <0.001 |
| WM × V | 1313 | 1 | 1313 | 0.194 | 0.660 | <0.001 |
| PS × TS × FM | 592 | 1 | 592 | 0.087 | 0.768 | <0.001 |
| PS × TS × V | 94 | 1 | 94 | 0.014 | 0.906 | <0.001 |
| PS × FM × V | 510 | 1 | 510 | 0.075 | 0.784 | <0.001 |
| TS × FM × V | 39 | 1 | 39 | 0.006 | 0.940 | <0.001 |
| PS × TS × FM × V | 14 | 1 | 14 | 0.002 | 0.964 | <0.001 |
| Error | 5,308,530 | 784 | 6771 |
| Sources | SS | df | MS | F | p-Value | η2 |
|---|---|---|---|---|---|---|
| Men | ||||||
| Target sex (TS) | 19,748 | 1 | 19,748 | 3.844 | 0.051 | 0.010 |
| Face mask (FM) | 184,260 | 1 | 184,260 | 35.868 | <0.001 | 0.084 |
| Vaccinated (V) | 197,783 | 1 | 197,783 | 38.501 | <0.001 | 0.089 |
| TS × FM | 3815 | 1 | 3815 | 0.743 | 0.389 | 0.002 |
| TS × V | 1052 | 1 | 1052 | 0.205 | 0.651 | 0.001 |
| FM × V | 93 | 1 | 93 | 0.018 | 0.893 | <0.001 |
| TS × FM × V | 3 | 1 | 3 | 0.001 | 0.980 | <0.001 |
| Error | 2,013,754 | 392 | 5137 | |||
| Women | ||||||
| Target sex (TS) | 113,803 | 1 | 113,803 | 13.540 | <0.001 | 0.033 |
| Face mask (FM) | 306,221 | 1 | 306,221 | 36.433 | <0.001 | 0.085 |
| Vaccinated (V) | 181,704 | 1 | 181,704 | 21.618 | <0.001 | 0.052 |
| TS × FM | 749 | 1 | 749 | 0.089 | 0.766 | <0.001 |
| TS × V | 350 | 1 | 350 | 0.042 | 0.839 | <0.001 |
| FM × V | 1730 | 1 | 1730 | 0.206 | 0.650 | 0.001 |
| TS × FM × V | 49 | 1 | 49 | 0.939 | 0.939 | <0.001 |
| Error | 3,294,779 | 392 | 8405 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chen, Y.-L.; Rahman, A. Effects of Target Variables on Interpersonal Distance Perception for Young Taiwanese during the COVID-19 Pandemic. Healthcare 2023, 11, 1711. https://doi.org/10.3390/healthcare11121711
Chen Y-L, Rahman A. Effects of Target Variables on Interpersonal Distance Perception for Young Taiwanese during the COVID-19 Pandemic. Healthcare. 2023; 11(12):1711. https://doi.org/10.3390/healthcare11121711
Chicago/Turabian StyleChen, Yi-Lang, and Andi Rahman. 2023. "Effects of Target Variables on Interpersonal Distance Perception for Young Taiwanese during the COVID-19 Pandemic" Healthcare 11, no. 12: 1711. https://doi.org/10.3390/healthcare11121711
APA StyleChen, Y.-L., & Rahman, A. (2023). Effects of Target Variables on Interpersonal Distance Perception for Young Taiwanese during the COVID-19 Pandemic. Healthcare, 11(12), 1711. https://doi.org/10.3390/healthcare11121711