Biomechanical Assessments in Woodwind Musicians: A Systematic Review

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Strategies
2.2. Elegibility Criteria
2.3. Study Selection
2.4. Data Extraction
2.5. Quality Assessment of Included Studies
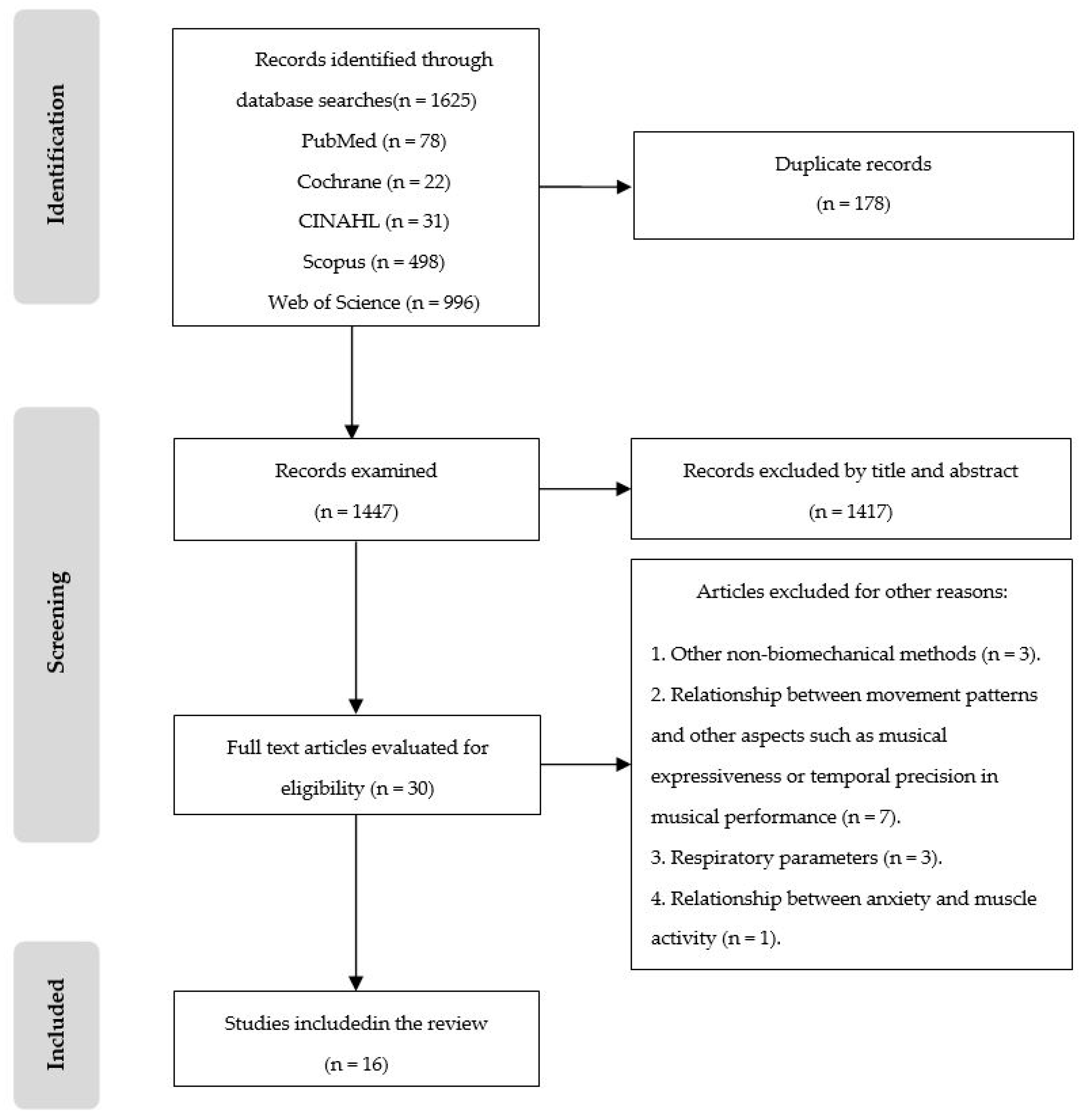
3. Results
3.1. Selected Studies
3.2. Characteristics of the Participants of the Included Studies
3.3. Summary of Selected Studies

{kind=link}
| Authors (Year) | N | Age | Gender | Estate of Health | Type/Group of Instrument | Professional, Student, Amateur | Years of Practice |
|---|---|---|---|---|---|---|---|
| Ackermann et al. (2014) [34] | 113 | 34.1 * | 68M/45F | N/A | Clarinet (12), bass clarinet (2), oboe (11), English horn (3), saxophone (3), flute (23), recorder (1), piccolo (2), shakuhachi (1), bassoon (11), contrabassoon (3), french horn (10), trombone (9), bass trombone (2), trumpet (16), and tuba (4) | Professionals and students | N/A |
| Baadjou et al. (2017) [35] | 20 | 18–60 | 9M/11F | Healthy | Clarinet | Professionals and students | 19.4 * |
| Barros et al. (2018) [25] | 30 | 18–49 25.5 * | N/A | N/A | Clarinet | Professionals and students | 8–37 |
| Clemente et al. (2018) [29] | 1 | N/A | F | Periapical lesion (tooth 21) | Saxophone | Professional | N/A |
| Clemente et al. (2018) [30] | 1 | N/A | M | TMD | English horn and oboe | N/A | N/A |
| Clemente et al. (2018) [31] | 1 | 30 | F | TMD | Clarinet | N/A | N/A |
| Clemente et al. (2019) [26] | 28 | N/A | N/A | No pain | Clarinet (7), oboe (2), saxophone (7), bassoon (4), trumpet (6), french horn (1), trombone (1). Transverse flute (1) and bisel flute (1) | Students | N/A |
| Clemente et al. (2019) [27] | 3 | >18 | N/A | Malocclusion | Clarinet (1), tuba (1), and bassoon (1) | N/A | >10 |
| Clemente et al. (2019) [28] | 10 | N/A | N/A | No pain | Clarinet (5) and saxophone (5) | Students | N/A |
| Clemente et al. (2020) [39] | 77 | 18–31 | 41M/36F | N/A | Woodwind (27), brass (22), and strings (28) | Students | >10 |
| Franz et al. (2020) [36] | 8 | 20.0 * (students)– 33.0 * (professionals) | 3M/5F | Healthy | Clarinet | Professionals and students | N/A |
| Gotouda et al. (2007) [32] | 33 | 15–27 | 12M/21F | Pain in TMJ and jaw muscles. | Clarinet (7), oboe (3), saxophone (2), bassoon (2), trumpet (8), french horn (4), trombone (4), tuba (2), and euphonium (1) | N/A | N/A |
| Hofmann y Goebl (2016) [37] | 23 | 19–45 27 * | 13M/10F | N/A | Clarinet | Professionals and students | N/A |
| Piatek et al. (2018) [40] | 14 | 18–38 25.86 * | 7M/7F | No MSD | Saxophone | Students and amateurs | <5 to >8 |
| Smyth y Mirka (2021) [33] | 8 | 18–30 | 1M/7F | Healthy | Clarinet | N/A | >5 |
| Young y Winges (2017) [38] | 20 | 26.2 * | 7M/13F | Healthy | Clarinet | Professionals and students | N/A |
3.4. Biomechanical Methods
3.5. Muscles Analyzed by SEMG
4. Discussion
4.1. Pressure Sensors
4.2. Surface Electromyography
4.3. Infrared Thermography
4.4. Kinematic Studies
4.5. Implications for Future Research
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kelleher, L.K.; Campbell, K.R.; Dickey, J.P. Biomechanical research on bowed string musicians: A scoping study. Med. Probl. Perform. Art. 2013, 28, 212–218. [Google Scholar] [CrossRef] [PubMed]
- Chan, C.; Ackermann, B. Evidence-informed physical therapy management of performance related musculoskeletal disorders in musicians. Front. Psychol. 2014, 5, 706. [Google Scholar] [CrossRef] [PubMed]
- de Greef, M.; van Wijck, R.; Reynders, K.; Toussaint, J.; Hesseling, R. Impact of the Groningen Exercise Therapy for Symphony Orchestra Musicians Program on Perceived Physical Competence and Playing-Related Musculoskeletal Disorders of Professional Musicians. Med. Probl. Perform. Art. 2003, 18, 156–160. [Google Scholar] [CrossRef]
- Chan, C.; Driscoll, T.; Ackermann, B.J. Effect of a Musicians’ Exercise Intervention on Performance-Related Musculoskeletal Disorders. Med. Probl. Perform. Art. 2014, 29, 181–188. [Google Scholar] [CrossRef]
- Schemmann, H.; Rensing, N.; Zalpour, C. Musculoskeletal Assessments Used in Quantitatively Based Studies About Posture and Movement in High String Players: A Systematic Review. Med. Probl. Perform. Art. 2018, 33, 56–71. [Google Scholar] [CrossRef]
- Herrmann, N.; Just, M.; Zalpour, C.; Möller, D. Musculoskeletal and psychological assessments used in quantitatively based studies about musicians’ health in brass players: A systematic literature review. J. Bodyw. Mov. Ther. 2021, 28, 376–390. [Google Scholar] [CrossRef]
- Moraes, G.F.; Antunes, A.P. Musculoskeletal disorders in professional violinists and violists. Systematic review. Acta Ortop. Bras. 2012, 20, 43–47. [Google Scholar] [CrossRef]
- Brandfonbrener, A.G. Musculoskeletal problems of instrumental musicians. Hand Clin. 2003, 19, 231–239. [Google Scholar] [CrossRef]
- Rodríguez-Lozano, F.J.; Sáez-Yuguero, M.R.; Bermejo-Fenoll, A. Orofacial problems in musicians: A review of the literature. Med. Probl. Perform. Art. 2011, 26, 150–156. [Google Scholar] [CrossRef]
- Kok, L.M.; Huisstede, B.M.A.; Voorn, V.M.A.; Schoones, J.W.; Nelissen, R.G.H.H. The occurrence of musculoskeletal complaints among professional musicians: A systematic review. Int. Arch. Occup. Environ. Health 2016, 89, 373–396. [Google Scholar] [CrossRef]
- Lederman, R.J. Neuromuscular and musculoskeletal problems in instrumental musicians. Muscle Nerve 2003, 27, 549–561. [Google Scholar] [CrossRef]
- García-Gómez, M. Las enfermedades profesionales de los músicos: El precio de la perfección [Occupational diseases of musicians: The price of perfection]. Arch. Prev. Riesgos Labor. 2018, 21, 11–17. [Google Scholar] [PubMed]
- Yeo, D.K.; Pham, T.P.; Baker, J.; Porters, S.A. Specific orofacial problems experienced by musicians. Aust. Dent. J. 2002, 47, 2–11. [Google Scholar] [CrossRef] [PubMed]
- Storms, P.R.; Elkins, C.P.; Strohecker, E.M. Embouchure Dysfunction in Air Force Band Brass Musicians. Med. Probl. Perform. Art. 2016, 31, 110–116. [Google Scholar] [CrossRef]
- Jankovic, J.; Ashoori, A. Movement disorders in musicians. Mov. Disord. 2008, 23, 1957–1965. [Google Scholar] [CrossRef]
- Kjelland, J.M. Application of Electromyography and Electromyographic Biofeedback in Music Performance Research: A Review of the Literature since 1985. Med. Probl. Perform. Art. 2000, 15, 115–118. [Google Scholar] [CrossRef]
- Overton, M.; Du Plessis, H.; Sole, G. Electromyography of neck and shoulder muscles in instrumental musicians with musculoskeletal pain compared to asymptomatic controls: A systematic review and meta-analysis. Musculoskelet. Sci. Pract. 2018, 36, 32–42. [Google Scholar] [CrossRef] [PubMed]
- Nishiyama, A.; Tsuchida, E. Relationship Between Wind Instrument Playing Habits and Symptoms of Temporomandibular Disorders in Non-Professional Musicians. Open Dent. J. 2016, 10, 411–416. [Google Scholar] [CrossRef]
- Branco, J.H.L.; Branco, R.L.L.; Siqueira, T.C.; de Souza, L.C.; Dalago, K.M.S.; Andrade, A. Clinical applicability of infrared thermography in rheumatic diseases: A systematic review. J. Therm. Biol. 2022, 104, 103172. [Google Scholar] [CrossRef]
- Ring, E.F.J.; Ammer, K. Infrared thermal imaging in medicine. Physiol. Meas. 2012, 33, R33. [Google Scholar] [CrossRef]
- Sillero-Quintana, M.; Gómez-Carmona, P.; Fernández-Cuevas, I. Infrared thermography as a means of monitoring and preventing sports injuries. In Innovative Research in Termal Imaging for Biology and Medicine; IGI Global: Hershey, PA, USA, 2017; pp. 165–198. [Google Scholar] [CrossRef]
- Attallah, M.M.; Visscher, C.M.; van Selms, M.K.A.; Lobbezoo, F. Is there an association between temporomandibular disorders and playing a musical instrument? A review of literature. J. Oral Rehabil. 2014, 41, 532–541. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.; Akl, E.; Brennan, S.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: Guidelines for reporting observational studies. Lancet 2007, 370, 1453–1457. [Google Scholar] [CrossRef] [PubMed]
- Barros, A.; Mendes, J.; Moreira, A.; Vardasca, R.; Pais-Clemente, M.; Pinhão-Ferreira, A. Thermographic Study of the Orofacial Structures Involved in Clarinetists Musical Performance. Dent. J. 2018, 6, 62. [Google Scholar] [CrossRef] [PubMed]
- Clemente, M.P.; Moreira, A.; Mendes, J.; Ferreira, A.P.; Amarante, J.M. Wind Instrumentalist Embouchure and the Applied Forces on the Perioral Structures. Open Dent. J. 2019, 13, 107–114. [Google Scholar] [CrossRef]
- Clemente, M.P.; Amarante, J.M.; Moreira, A.; Ferreira, A.P.; Vardasca, R.; Mendes, J. The Functional Interdependence of Wind Instrumentalists’ Embouchure and Their Craniofacial Features. Int. J. Online Biomed. Eng. 2019, 15, 17–33. [Google Scholar] [CrossRef]
- Pais-Clemente, M.; Mendes, J.; Cerqueira, J.; Moreira, A.; Vasconcelos, M.; Pinhão-Ferreira, A.; Amarante, J.M. Integrating piezoresistive sensors on the embouchure analysis of the lower lip in single reed instrumentalists: Implementation of the lip pressure appliance (LPA). Clin. Exp. Dent. Res. 2019, 5, 491–496. [Google Scholar] [CrossRef]
- Clemente, M.; Mendes, J.; Moreira, A.; Ferreira, A.P.; Amarante, J.M. A Prosthodontic Treatment Plan for a Saxophone Player: A Conceptual Approach. Dent. J. 2018, 6, 33. [Google Scholar] [CrossRef]
- Clemente, M.P.; Mendes, J.G.; Vardasca, R.; Ferreira, A.P.; Amarante, J.M. Combined Acquisition Method of Image and Signal Technique (CAMIST) for Assessment of Temporomandibular Disorders in Performing Arts Medicine. Med. Probl. Perform. Art. 2018, 33, 205–212. [Google Scholar] [CrossRef]
- Clemente, M.P.; Mendes, J.; Moreira, A.; Vardasca, R.; Ferreira, A.P.; Amarante, J.M. Wind Instrumentalists and Temporomandibular Disorder: From Diagnosis to Treatment. Dent. J. 2018, 6, 41. [Google Scholar] [CrossRef]
- Gotouda, A.; Yamaguchi, T.; Okada, K.; Matsuki, T.; Gotouda, S.; Inoue, N. Influence of playing wind instruments on activity of masticatory muscles. J. Oral Rehabil. 2007, 34, 645–651. [Google Scholar] [CrossRef]
- Smyth, C.; Mirka, G.A. Impact of a Neck Strap Intervention on Perceived Effort, Thumb Force, and Muscle Activity of Clarinetists. Med. Probl. Perform. Art. 2021, 36, 225–232. [Google Scholar] [CrossRef] [PubMed]
- Ackermann, B.J.; O’Dwyer, N.; Halaki, M. The difference between standing and sitting in 3 different seat inclinations on abdominal muscle activity and chest and abdominal expansion in woodwind and brass musicians. Front. Psychol. 2014, 5, 913. [Google Scholar] [CrossRef] [PubMed]
- Baadjou, V.A.; van Eijsden-Besseling, M.; Verbunt, J.; de Bie, R.A.; Geers, R.; Smeets, R.; Seelen, H. Playing the Clarinet: Influence of Body Posture on Muscle Activity and Sound Quality. Med. Probl. Perform. Art. 2017, 32, 125–131. [Google Scholar] [CrossRef] [PubMed]
- Franz, L.; Travan, L.; Isola, M.; Marioni, G.; Pozzo, R. Facial Muscle Activity Patterns in Clarinet Players: A Key to Understanding Facial Muscle Physiology and Dysfunction in Musicians. Ann. Otol. Rhinol. Laryngol. 2020, 129, 1078–1087. [Google Scholar] [CrossRef]
- Hofmann, A.; Goebl, W. Finger Forces in Clarinet Playing. Front. Psychol. 2016, 7, 1140. [Google Scholar] [CrossRef] [PubMed]
- Young, K.E.; Winges, S.A. Thumb-Rest Position and its Role in Neuromuscular Control of the Clarinet Task. Med. Probl. Perform. Art. 2017, 32, 71–77. [Google Scholar] [CrossRef] [PubMed]
- Clemente, M.P.; Mendes, J.; Vardasca, R.; Moreira, A.; Branco, C.A.; Ferreira, A.P.; Amarante, J.M. Infrared thermography of the crânio-cervico-mandibular complex in wind and string instrumentalists. Int. Arch. Occup. Environ. Health 2020, 93, 645–658. [Google Scholar] [CrossRef]
- Piatek, S.; Hartmann, J.; Günther, P.; Adolf, D.; Seidel, E.J. Influence of Different Instrument Carrying Systems on the Kinematics of the Spine of Saxophonists. Med. Probl. Perform. Art. 2018, 33, 251–257. [Google Scholar] [CrossRef]
- Riley, K. Helping Musicians Achieve Peak Performance with Surface Electromyography/Video. Biofeedback 2011, 39, 31–34. [Google Scholar] [CrossRef]

| Authors (Year) | Biomechanical Methods Used | Objectives | Method (Musical Activity) | Other Evaluations | Results | Conclusions | STROBE Total Score |
|---|---|---|---|---|---|---|---|
| Ackermann et al. (2014) [34] | SEMG | Investigate respiratory movements and abdominal muscle activity. | Playing five musical excerpts in four different postures (sitting flat, sitting inclined forward, sitting inclined backward and standing). | RIP | Higher chest cavity expansion standing (p < 0.01) and lower abdominal cavity expansion in sitting postures (p < 0.01). Lower activation in seated postures in comparison to standing posture (p < 0.01). | Significant differences in respiratory mechanics between sitting and standing postures. | 12 |
| Baadjou et al. (2017) [35] | 2D Goniometry SEMG | Analyze the relationship between body posture, muscle activity, and sound quality. | Playing a 60-s musical excerpt in two different postures (habitual sitting posture and experimental sitting posture). | Not carried out. | Smaller low thoracic angle, smaller high thoracic angle, and larger pelvic tilt angle in the experimental posture (p < 0.001). More activity of the erector spinal and lower trapezius muscles and less activity of the left upper trapezius and right brachioradialis muscles in the experimental sitting posture. | Postural exercise therapy may change muscle activity patterns. | 13 |
| Barros et al. (2018) [25] | IT | Analyze and record the thermal patterns of the CCMC to evaluate its structures. | Before and after playing a musical piece (“Vingt Etudes”) for 10 min. | Questionnaire (musical and clinical history of the participant) and clinical examination. | Statistically significant differences (p < 0.05) between before and after musical in the left temporal muscle, orbicularis muscle, perioral teguments, and teeth 11 and 21. Asymmetries ≥0.3 °C in the temporal and the orbicularis muscles at rest position and after the musical performance. | IT has been proven to be an effective complementary diagnostic tool in the monitorization of the CCMC. | 10 |
| Clemente et al. (2018) [29] | Pressure sensors | Quantify the pressure applied to the central incisors during embouchure. | Playing three times three different pitches (high, medium, and low). | Clinical and radiographic examination. | Greater force was applied during lower-pitched notes, especially to tooth 11 (108 g). | Pressure sensors are acceptable for identifying the tooth where the greatest pressure is applied. | 10 |
| Clemente et al. (2018) [30] | Pressure sensors IT | Analyze the morphological and functional aspects of the CCMC with and without a mouthpiece. | Force: playing three times three pitches (high, medium, and low). IT: after playing Ode to Joy during 5 min. | Clinical examination. Cephalometric analysis. | Greater pressure on the lower lip with the English horn and in the upper lip with the oboe. Difference of 0.3 °C between the right TMJ (34.7 °C) and the left TMJ (35 °C). Difference of 0.3 °C between the right masseter (35.4 °C) and the left masseter (35.1 °C). | Pressure sensors and IT can beuseful screening tools forthe diagnosis of TMDs. | 9 |
| Clemente et al. (2018) [31] | Pressure sensors IT | Describe the steps in the diagnosis and treatment of TMDs. | Pressure: performing three times three different pitches (high, medium, and low). IT: before and after using an occlusal splint during 6 months. | Clinical examination. | Higher pressure in higher pitches (94 g in tooth 11 y 408 g in tooth 21). Thermic difference between left and right side of the masseter muscle of 0.7 °C before and 0.3 °C after the use of the splint. | Pressure sensors and IT are useful in the diagnosis and monitoring of TMDs. | 10 |
| Clemente et al. (2019) [26] | Pressure sensors | Quantify the applied forces of the perioral structures during embouchure. | Playing three times three different pitches (high, medium, and low). | Not carried out. | F-mean (upper sensor/lower sensor) in clarinet (58 g/54.1 g), oboe (23 g/17 g), saxophone (38.9 g/62.7 g), bassoon (6.3 g/10.3 g). F-mean (lower sensor) in bisel flute (73 g) and transverse flute (220 g). F-mean (upper sensor/lower sensor) in trumpet (62.7 g/89.2 g), french horn (56 g/86 g), and trombone (201 g/220 g). | Brass players apply greater force than woodwind players during embouchure. | 8 |
| Clemente et al. (2019) [27] | Pressure sensors IT | Demostrate the usefulness of pressure sensors and IT as complementary diagnostic tools during embouchure. | Force (clarinet): playing a musical piece in a high pitch. IT (tuba): N/A. | Clinical examination. Cephalometric analysis (bassoon). | Asymmetric force in the two upper central incisors (2.5 N in tooth 21). Asymmetries of 0.4 °C between the left masseter muscle (32.6 °C) and the right one (33.0 °C). Difference of 0.3 °C between the left temporal muscle (33.3 °C) and the right one (33.6 °C). Difference of 0.3 °C between the left TMJ (32.6 °C) and the right TMJ (32.9 °C). | Pressure sensors and IT can be considered as complementary diagnostic tool. | 9 |
| Clemente et al. (2019) [28] | Pressure sensors | Measure forces at the lower lip during embouchure. | Playing three times three different pitches (high, medium, and low). | Clinical examination. | F-mean (lower sensor) in clarinet (58.8 g). F-mean (lower sensor) in saxophone(94 g). | Pressure sensors allow measuring the forces at the lower lip. | 8 |
| Clemente et al. (2020) [39] | IT | Assess regions of interest of the CCMC to evaluate muscular hyperactivity. | N/A | Not carried out. | Asymmetries ≥0.3 °C in the anterior temporal muscle between wind and string instrumentalists. Statistical significant differences (p = 0.044) in the anterior triangle of the neck between wind and string instrumentalists. | IT can be considered as a complementary diagnostic method. | 12 |
| Franz et al. (2020) [36] | SEMG | Identify the facial muscle activity patterns involved in playing and compare them between students and professionals. | Playing a musical piece and two scales | Not carried out. | Higher activity for the masseter (p = 0.0007), buccinator (p = 0.0001) and mylohyoid (p = 0.000) in students and for the mentalis in professionals (p = 0.000). | Significantly higher facial muscle activity in students. | 17 |
| Gotouda et al. (2007) [32] | SEMG | Analyze the influence of pitch changes on the activity of jaw-closing muscles. Elucidate the effect of sustained playing on fatigue of the jaw-closing muscles. | Test 1 (N = 33): playing a tuning tone and a pitch an octave higher and under other conditions (rest, clenching, and open-mouthed). Test 2 (N = 18): before and after playing non-stop for 90 min. | Questionnaire to measure the prevalence of musculoskeletal symptoms. | Test 1: higher RMS in high pitch in brass (p < 0.05). Higher RMS in high pitch in woodwind. Test 2: non-significant differences between groups. | Contraction load to jaw-closing muscles when playing a wind instrument is very small. Playing for a long time does not obviously induce fatigue. | 14 |
| Hofmann y Goebl (2016) [37] | Pressure sensors | Measure finger force while playing. | Test 1: playing eight selected excerpts from the first Weber concerto under controlled different performing conditions. Test 2 (technical exercise): playing an isochronous 23-tone melody in different tempos. | Articulatory tongue-reed interactions (with strain gauge sensors). Questionnaire (self-evaluation of finger forces; discomfort). | Test 1: F-mean = 1.17 N. Test 2: F-mean = 0.64 N (0.54 N in professionals and 0.68 N in students; p = 0.213). | Sensor-equipped instruments help to understand fine motor actions. | 16 |
| Piatek et al. (2018) [40] | 3D UT | Examine the influence of three different saxophone-carrying systems (neck-strap, shoulder-strap, and Saxholder) on the kinematics of the spine. | Playing 3-min pieces of music with and without each carrying system. Exam 1 (N = 14): alto saxophone. Exam 2 (N = 1): saxophone (alto, tenor, and baritone). | BMI | Head bows forward at a greater angle (3.35°) using a shoulderstrap than using a Saxholder (p = 0.02). | UT allows to investigate the influence of instrument-carrying systems on the kinematics of the spine. | 12 |
| Smyth y Mirka (2021) [33] | SEMG Pressure sensors | Determine the impact of the neck strap on thumb force while measuring the thenar, cervical, and shoulder muscle activity. | After playing a set of exercises during 3 min with and without a neckstrap. | Perceived effort survey using a scale from 0 (no effort) to 5 (severe effort). | Non-statistically significant increases in the muscle activity of any muscles of the neck, the shoulder, or the thenar muscles with the neck strap (p > 0.05). Significant decrease in average thumb force with the neck strap (p < 0.05). | The use of a neck strap significantly decreases the average force of the right thumb. | 12 |
| Young y Winges (2017) [38] | SEMG | Address the impact of the thumb-rest position on the neuromuscular control of holding the instrument. | Performing 10 held notes and 10 exercises on three different thumb-rest positions (low, traditional, and high). | Not carried out. | Significantly decreased activity of the abductor pollicis brevis and the flexor carpi ulnaris in a high thumb-rest position. | Adjustment of the thumb-rest position may alleviate discomfort in the supporting limb. | 13 |
| Category | Method | Number of Studies | Reference |
|---|---|---|---|
| Kinetics | Pressure sensors | 8 | Clemente et al. (2018) [29]; Clemente et al. (2018) [30]; Clemente et al. (2018) [31]; Clemente et al. (2019) [26]; Clemente et al. (2019) [27]; Clemente et al. (2019) [28]; Hofmann and Goebl (2016) [37]; Smyth and Mirka (2021) [33] |
| Kinematics | 2D Goniometry | 1 | Baadjou et al. (2017) [35] |
| 3D UT | 1 | Piatek et al. (2018) [40] | |
| Physiology | SEMG | 6 | Ackermann et al. (2014) [34]; Baadjou et al. (2017) [35]; Franz et al. (2020) [36]; Gotouda et al. (2007) [32]; Smyth and Mirka (2021) [33]; Young and Winges (2017) [38] |
| IT | 5 | Barros et al. (2018) [25]; Clemente et al. (2018) [30]; Clemente et al. (2018) [31]; Clemente et al. (2019) [27]; Clemente et al. (2020) [39] |
| Muscles | Reference |
|---|---|
| Abdominal muscles. | Ackermann et al. (2014) [34] |
| Erector espinae, latissimus dorsi, low trapezius, upper trapezius, pectoralis major (clavicular head), biceps brachii (short head), and brachioradialis. | Baadjou et al. (2017) [35] |
| Sternocleidomastoid, masseter, mentalis, mylohyoid and right side buccinator | Franz et al. (2020) [36] |
| Masseter, temporal, orbicularis oris, and left side digastric (test 1); left masseter (test 2). | Gotouda et al. (2007) [32] |
| Trapezius, semispinalis, and sternocleidomastoid; thenar muscle group of the right thumb. | Smyth and Mirka (2021) [33] |
| Triceps brachii, biceps brachii, extensor carpi radialis longus, flexor carpi ulnaris, brachioradialis, extensor pollicis brevis, abductor pollicis brevis, and first dorsal interosseou muscle of the right hand. | Young and Winges (2017) [38] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
López-Pineda, J.; Rodríguez-Martínez, M.C.; Gómez-Rodríguez, R.; García-Casares, L.; García-Casares, N. Biomechanical Assessments in Woodwind Musicians: A Systematic Review. Healthcare 2023, 11, 1621. https://doi.org/10.3390/healthcare11111621
López-Pineda J, Rodríguez-Martínez MC, Gómez-Rodríguez R, García-Casares L, García-Casares N. Biomechanical Assessments in Woodwind Musicians: A Systematic Review. Healthcare. 2023; 11(11):1621. https://doi.org/10.3390/healthcare11111621
Chicago/Turabian StyleLópez-Pineda, Javier, María Carmen Rodríguez-Martínez, Rosa Gómez-Rodríguez, Lucía García-Casares, and Natalia García-Casares. 2023. "Biomechanical Assessments in Woodwind Musicians: A Systematic Review" Healthcare 11, no. 11: 1621. https://doi.org/10.3390/healthcare11111621
APA StyleLópez-Pineda, J., Rodríguez-Martínez, M. C., Gómez-Rodríguez, R., García-Casares, L., & García-Casares, N. (2023). Biomechanical Assessments in Woodwind Musicians: A Systematic Review. Healthcare, 11(11), 1621. https://doi.org/10.3390/healthcare11111621