

Effects of Tai Chi on Postural Control in People with Peripheral Neuropathy: A Systematic Review with Meta-Analysis



Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Literature Search Strategy
2.3. Literature Inclusion and Exclusion Criteria
2.3.1. Literature Inclusion Criteria
Participants
Intervention
Comparison
Outcome Measures
2.3.2. Literature Exclusion Criteria
2.4. Literature Selection and Data Extraction
2.5. Assessment of Methodological Quality of Studies
2.6. Statistical Analysis
3. Results
3.1. Literature Search Results
3.2. Basic Characteristics of Included Studies
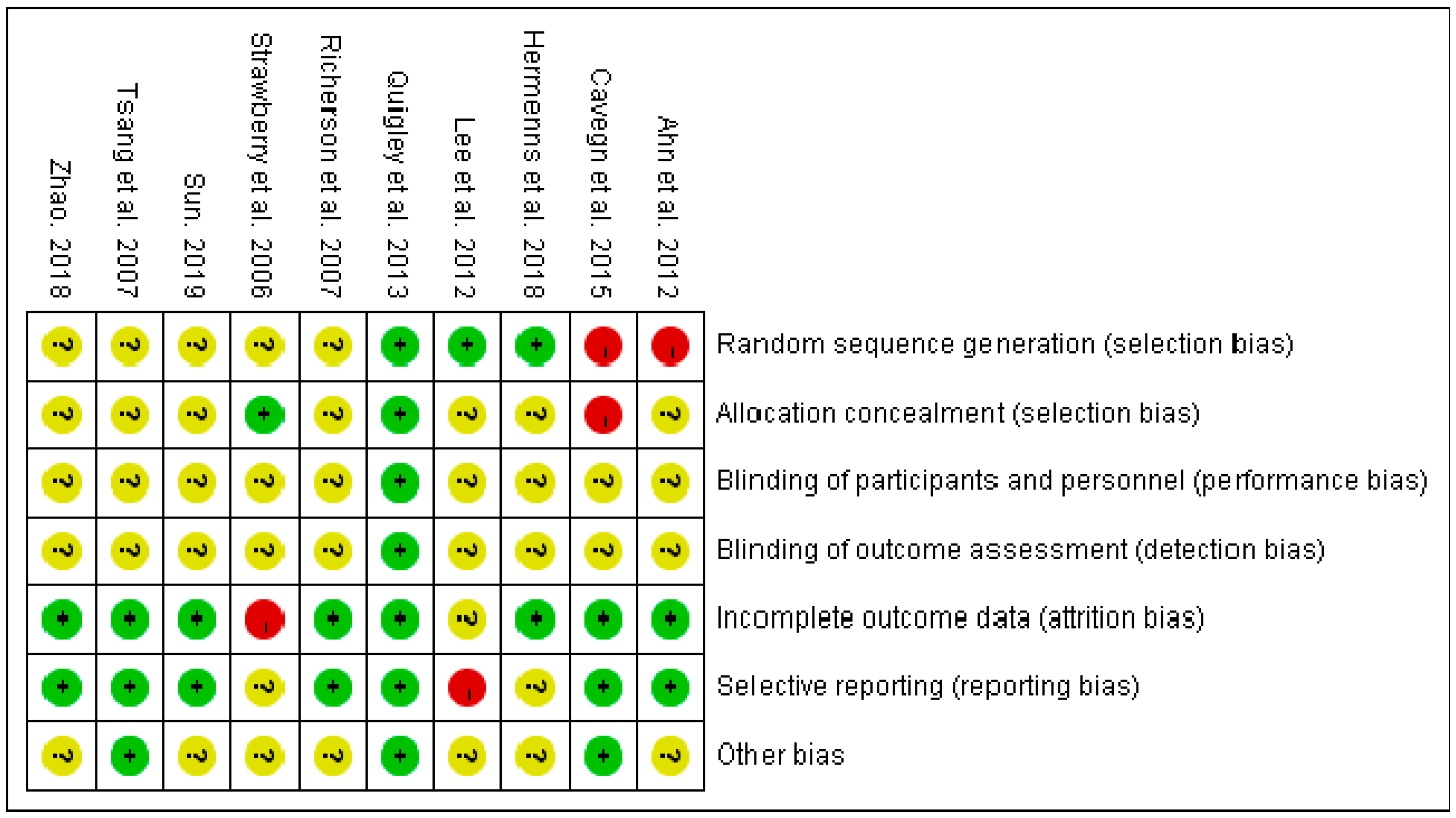
3.3. Literature Quality Evaluation
3.4. Meta-Analysis of Measured Outcomes
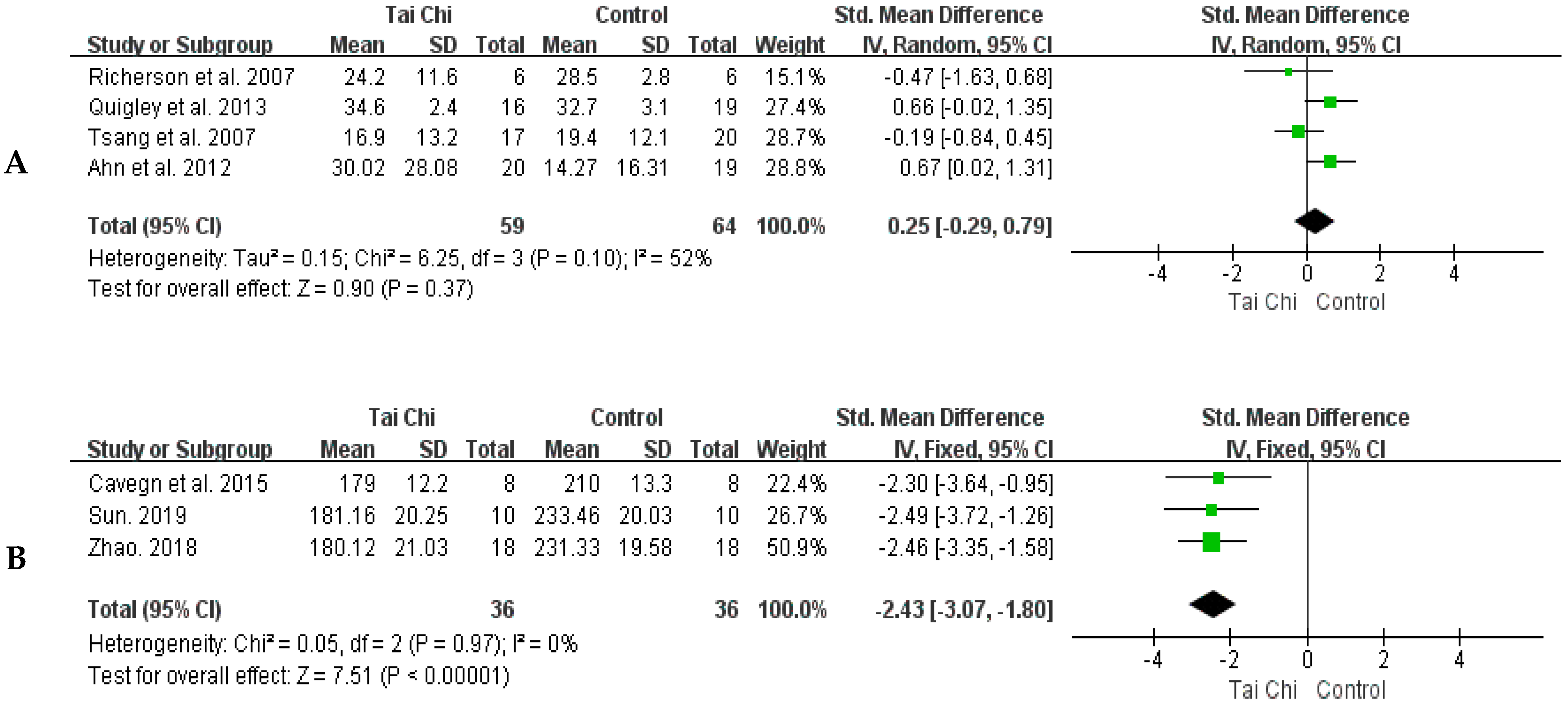
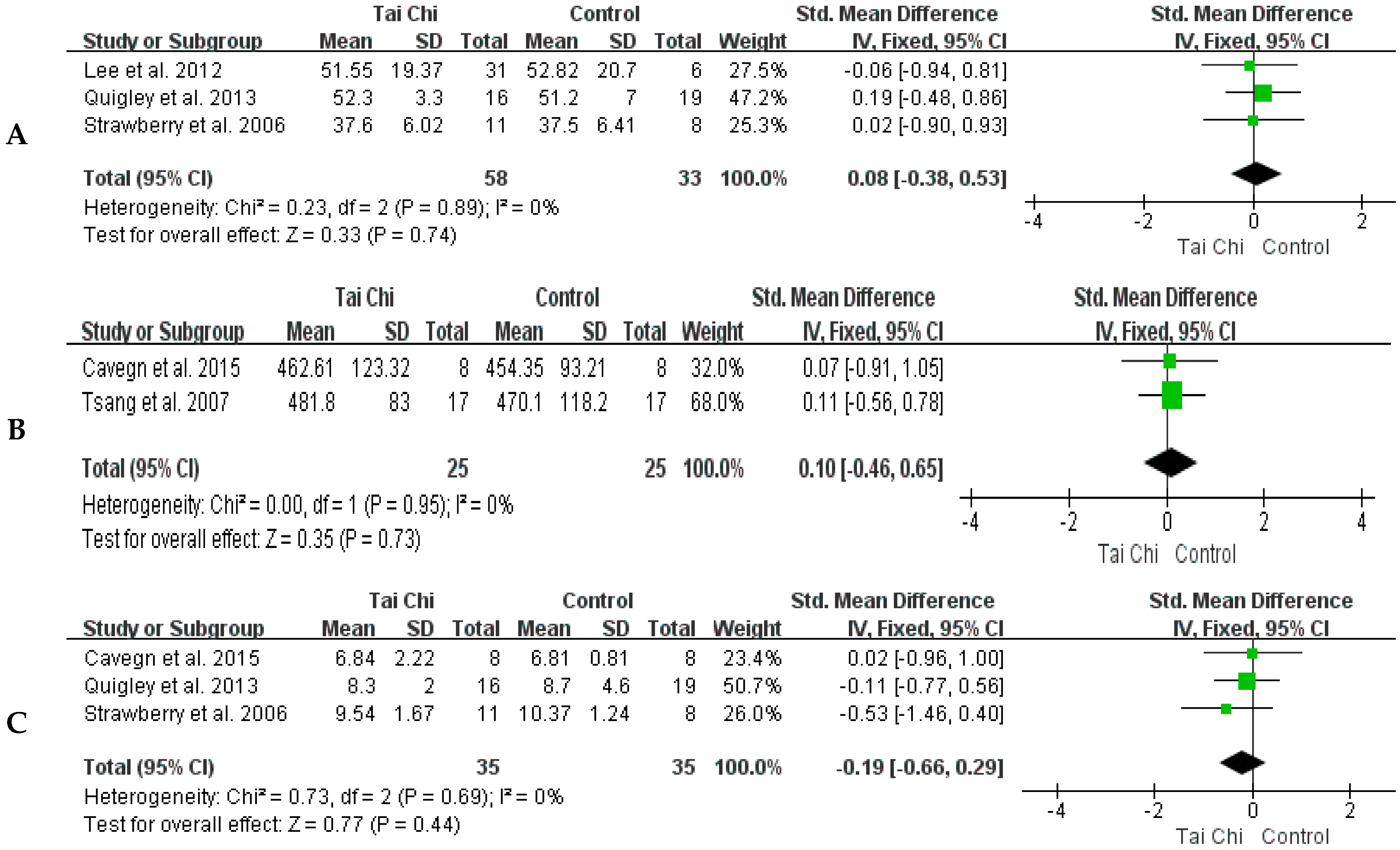
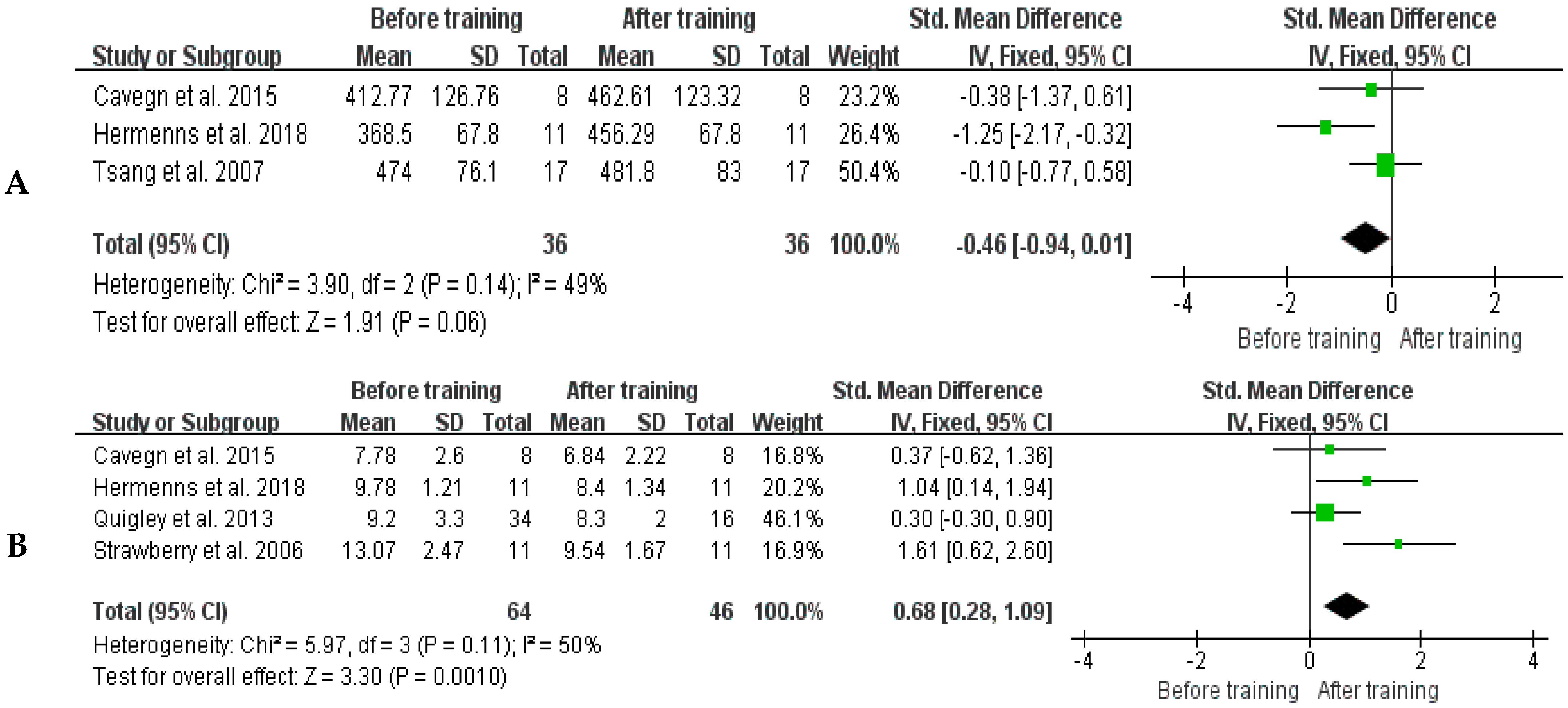
3.4.1. Static Postural Control
3.4.2. Dynamic Postural Control
4. Discussion
4.1. Basic Characteristics of Included Studies
4.2. Included Literature Quality
4.3. Static Postural Control
4.4. Dynamic Postural Control
4.5. Limitation
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Richardson, J.K. The clinical identification of peripheral neuropathy among older persons. Arch. Phys. Med. Rehabil. 2002, 83, 1553–1558. [Google Scholar] [CrossRef] [PubMed]
- Li, L.; Zhang, S.; Dobson, J. The contribution of small and large sensory afferents to postural control in patients with peripheral neuropathy. J. Sport Health Sci. 2019, 8, 218–227. [Google Scholar] [CrossRef] [PubMed]
- Alam, U.; Riley, D.R.; Jugdey, R.S.; Azmi, S.; Rajbhandari, S.; D’août, K.; Malik, R.A. Diabetic neuropathy and gait: A review. Diabetes Ther. 2017, 8, 1253–1264. [Google Scholar] [CrossRef] [PubMed]
- Hicks, C.W.; Selvin, E. Epidemiology of peripheral neuropathy and lower extremity disease in diabetes. Curr. Diabetes Rep. 2019, 19, 1–8. [Google Scholar] [CrossRef]
- Oh, T.J.; Kang, S.; Lee, J.-E.; Moon, J.H.; Choi, S.H.; Lim, S.; Jang, H.C. Association between deterioration in muscle strength and peripheral neuropathy in people with diabetes. J. Diabetes Its Complicat. 2019, 33, 598–601. [Google Scholar] [CrossRef]
- Camargo, M.R.; Barela, J.A.; Nozabieli, A.J.; Mantovani, A.M.; Martinelli, A.R.; Fregonesi, C.E. Balance and ankle muscle strength predict spatiotemporal gait parameters in individuals with diabetic peripheral neuropathy. Diabetes Amp. Metab. Syndr. Clin. Res. Amp. Rev. 2015, 9, 79–84. [Google Scholar] [CrossRef]
- DeMott, T.K.; Richardson, J.K.; Thies, S.B.; Ashton-Miller, J.A. Falls and gait characteristics among older persons with peripheral neuropathy. Am. J. Phys. Med. Rehabil. 2007, 86, 125–132. [Google Scholar] [CrossRef]
- Richardson, J.K.; Ching, C.; Hurvitz, E.A. The relationship between electromyographically documented peripheral neuropathy and falls. J. Am. Geriatr. Soc. 1992, 40, 1008–1012. [Google Scholar] [CrossRef]
- Zang, X.; Bai, J. Research progress on risk assessment and intervention of fall in elderly patients with diabetic peripheral neuropathy. J. Nurs. Sci. 2015, 30, 93–97. [Google Scholar]
- Reeves, N.D.; Orlando, G.; Brown, S.J. Sensory-motor mechanisms increasing falls risk in diabetic peripheral neuropathy. Medicina 2021, 57, 457. [Google Scholar] [CrossRef]
- Alsubiheen, A.; Petrofsky, J.; Daher, N.; Lohman, E.; Balbas, E. Effect of Tai Chi exercises combined with mental imagery theory in improving balance in a diabetic and elderly population. Med. Sci. Monit. 2015, 21, 3054–3061. [Google Scholar] [CrossRef] [PubMed]
- Hewston, P.; Deshpande, N. Falls and balance impairments in older adults with type 2 diabetes: Thinking beyond diabetic peripheral neuropathy. Can. J. Diabetes 2016, 40, 6–9. [Google Scholar] [CrossRef] [PubMed]
- Strawberry, K.G.; Woollacott, M.H. Neural mechanisms underlying balance improvement with short-term Tai Chi training. Aging Clin. Exp. Res. 2006, 18, 7–19. [Google Scholar] [CrossRef]
- Li, L.; Hondzinski, J.M. Select exercise modalities may reverse movement dysfunction because of peripheral neuropathy. Exerc. Sport Sci. Rev. 2012, 40, 133–137. [Google Scholar] [CrossRef]
- Gallant, M.P.; Tartaglia, M.; Hardman, S.; Burke, K. Using Tai Chi to reduce fall risk factors among older adults: An evaluation of a community-based implementation. J. Appl. Gerontol. 2019, 38, 983–998. [Google Scholar] [CrossRef]
- Nyman, S.R. Tai Chi for preventing falls among older adults: A critical analysis of the evidence. J. Aging Phys. Act. 2021, 29, 343–352. [Google Scholar] [CrossRef]
- Bubela, D.; Sacharko, L.; Chan, J.; Brady, M. Balance and functional outcomes for older community-dwelling adults who practice Tai Chi and those who do not. J. Geriatr. Phys. Ther. 2019, 42, 209–215. [Google Scholar] [CrossRef]
- Lomas-Vega, R.; Obrero-Gaitán, E.; Molina-Ortega, F.J.; Del-Pino-Casado, R. Tai Chi for risk of falls. a meta-analysis. J. Am. Geriatr. Soc. 2017, 65, 2037–2043. [Google Scholar] [CrossRef]
- Holmes, M.L.; Manor, B.; Hsieh, W.-H.; Hu, K.; Lipsitz, L.A.; Li, L. Tai Chi training reduced the coupling between respiration and postural control. Neurosci. Lett. 2016, 610, 60–65. [Google Scholar] [CrossRef]
- Pan, J.; Liu, C.; Zhang, S.; Li, L. Tai Chi can improve postural stability as measured by resistance to perturbation related to upper limb movement among healthy older adults. Evid.-Based Complement. Altern. Med. 2016, 2016, 1–9. [Google Scholar] [CrossRef]
- Pan, J.; Liu, C.; Li, L.; Zhang, S. The effect of Tai Chi exercises on postural time-to-contact in manual fitting tasks among older adults. Gait Posture 2020, 82, 61–67. [Google Scholar] [CrossRef] [PubMed]
- Li, L.; Manor, B. Long-term Tai Chi exercise improves physical performance among people with peripheral neuropathy. Am. J. Chin. Med. 2010, 38, 449–459. [Google Scholar] [CrossRef] [PubMed]
- Ahn, S.; Song, R. Effects of Tai Chi Exercise on glucose control, neuropathy scores, balance, and quality of life in patients with type 2 diabetes and neuropathy. J. Altern. Complement. Med. 2012, 18, 1172–1178. [Google Scholar] [CrossRef] [PubMed]
- Cavegn, E.I.; Riskowski, J.I. The Effects of Tai Chi on peripheral somatosensation, balance, and fitness in Hispanic older adults with type 2 diabetes: A pilot and feasibility study. Evid.-Based Complement. Altern. Med. 2015, 2015, 1–9. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Zhou, J.; Chang, S.; Cong, Y.; Qin, M.; Sun, W.; Lian, J.; Yao, J.; Li, W.; Hong, Y. Effects of 24 weeks of Tai Chi exercise on postural control among elderly women. Res. Sport. Med. 2015, 23, 302–314. [Google Scholar] [CrossRef] [PubMed]
- Xu, D.; Li, J.; Hong, Y. Effect of regular Tai Chi and jogging exercise on neuromuscular reaction in older people. Age Ageing 2005, 34, 439–444. [Google Scholar] [CrossRef]
- Varghese, R.; Hui-Chan, C.W.Y.; Bhatt, T. Reduced cognitive-motor interference on voluntary balance control in older Tai Chi practitioners. J. Geriatr. Phys. Ther. 2016, 39, 190–199. [Google Scholar] [CrossRef]
- Tsang, W.W.N.; Hui-Chan, C.W.Y.; Fu, S.N. Effects of Tai Chi on pre-landing muscle response latency during stepping down while performing a concurrent mental task in older adults. Eur. J. Appl. Physiol. 2012, 112, 2663–2669. [Google Scholar] [CrossRef]
- Tsang, T.; Orr, R.; Lam, P.; Comino, E.J.; Singh, M.F. Health benefits of Tai Chi for older patients with type 2 diabetes: The “Move It For Diabetes study”—A randomized controlled trial. Clin. Interv. Aging 2007, 2, 429–439. [Google Scholar] [CrossRef]
- Richerson, S.; Rosendale, K. Does Tai Chi improve plantar sensory ability? a pilot study. Diabetes Technol. Ther. 2007, 9, 276–286. [Google Scholar] [CrossRef]
- Quigley, P.A.; Bulat, T.; Schulz, B.; Friedman, Y.; Hart-Hughes, S.; Richardson, J.K.; Barnett, S. Exercise interventions, gait, and balance in older subjects with distal symmetric polyneuropathy: A three-group randomized clinical trial. Am. J. Phys. Med. Rehabil. 2013, 93, 1–16. [Google Scholar] [CrossRef] [PubMed]
- Hermanns, M.; Haas, B.K.; Rath, L.; Murley, B.; Arce-Esquivel, A.A.; Ballard, J.E.; Wang, Y.T. Impact of Tai Chi on peripheral neuropathy revisited: A mixed-methods study. Gerontol. Geriatr. Med. 2018, 4, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. Int. J. Surg. 2021, 88, 105906. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; Moher, D.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. PRISMA 2020 explanation and elaboration: Updated guidance and exemplars for reporting systematic reviews. BMJ 2021, 29, 160–372. [Google Scholar] [CrossRef] [PubMed]
- Giacomozzi, C.; Caselli, A.; Macellari, V.; Giurato, L.; Lardieri, L.; Uccioli, L. Walking strategy in diabetic patients with peripheral neuropathy. Diabetes Care 2002, 25, 1451–1457. [Google Scholar] [CrossRef]
- Higgins, J.P.; Savović, J.; Page, M.J.; Elbers, R.G.; Sterne, J.A. Chapter 8: Assessing risk of bias in a randomized trial. In Cochrane Handbook for Systematic Reviews of Interventions; Version 6.3; Wiley: Hoboken, NJ, USA, 2022. [Google Scholar] [CrossRef]
- Hopkins, W.G. A Scale of Magnitudes for Effect Statistics. A New View of Statistics. 2006. Available online: http://sportsci.org/resource/stats/index.html (accessed on 1 May 2023).
- Sun, X. Effects of high-intensity interval training and continuous aerobic training on body composition and cardiopulmonary fitness in healthy and obese adolescents: A meta-analysis. Sport. Sci. Res. 2021, 42, 77–85+93. [Google Scholar]
- Lee, P.S.; Jung, M.; Abraham, A.; Lei-Rivera, L.; Kim, A.H. Efficacy of Tai Chi as a technique for vestibular rehabilitation—A preliminary quasi-experimental study. J. Phys. Ther. 2012, 5, 6–13. [Google Scholar]
- Zhao, Y. Study on the Intervention Effect of 24-Style Taijiquan on the Gait of Type 2 Diabetes Patients. Master’s Thesis, Liaoning Normal University, Dalian, China, 2018. [Google Scholar]
- Sun, X. Effect of Taijiquan and Taijiquan Combined with Resistance Exercise on the Gait of T2DM Patients. Master’s Thesis, Liaoning Normal University, Dalian, China, 2019. [Google Scholar]
- Wong, A.M.K.; Lan, C. Tai Chi, and balance control. Tai Chi Chuan 2008, 52, 115–123. [Google Scholar]
- Hackney, M.E.; Earhart, G.M. Tai Chi improves balance and mobility in people with Parkinson disease. Gait Posture 2008, 28, 456–460. [Google Scholar] [CrossRef]
- Xu, D.; Hong, Y.; Li, J.; Chan, K. Effect of Tai Chi exercise on proprioception of ankle and knee joints in old people. Br. J. Sport. Med. 2004, 38, 50–54. [Google Scholar] [CrossRef]
- Yu, X.; Hou, L.; Guo, J.; Wang, Y.; Han, P.; Fu, L.; Song, P.; Chen, X.; Yu, H.; Zhang, Y.; et al. The combined effect of osteoporosis and poor dynamic balance on the incidence of sarcopenia in elderly Chinese community suburban-dwelling individuals. J. Nutr. Health Aging 2020, 24, 71–77. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.; Ye, M.; Xiong, J.; Wang, X.; Wu, J.; Zheng, G. Optimal exercise parameters of Tai Chi for balance performance in older adults: A meta-analysis. J. Am. Geriatr. Soc. 2021, 69, 2000–2010. [Google Scholar] [CrossRef] [PubMed]
- Lee, M.S.; Jun, J.H.; Lim, H.-J. A systematic review and meta-analysis of tai chi for treating type 2 diabetes. Maturitas 2015, 80, 14–23. [Google Scholar] [CrossRef] [PubMed]
- Elkins, M. Tai Chi improves balance and prevents falls in people with Parkinson’s disease. J. Physiother. 2015, 61, 44. [Google Scholar] [CrossRef]
- Kim, H.; Kim, Y.L.; Lee, S.M. Effects of therapeutic Tai Chi on balance, gait, and quality of life in chronic stroke patients. Int. J. Rehabil. Res. 2015, 38, 156–161. [Google Scholar] [CrossRef]
- Tsang, W.W.; Hui-Chan, C.W. Comparison of muscle torque, balance, and confidence in older tai chi and healthy adults. Med. Sci. Sport. Exerc. 2005, 37, 280–289. [Google Scholar] [CrossRef]
- Liu, H.; Frank, A. Tai chi as a balance improvement exercise for older adults: A systematic review. J. Geriatr. Phys. Ther. 2010, 33, 103–109. [Google Scholar] [CrossRef]
- Wu, W.; Liu, X.; Wang, L.; Wang, Z.; Hu, J.; Yan, J. Effects of Tai Chi on exercise capacity and health-related quality of life in patients with chronic obstructive pulmonary disease: A systematic review and meta-analysis. Int. J. Chronic Obstr. Pulm. Dis. 2014, 9, 1253–1263. [Google Scholar] [CrossRef]
- Konig, P.R.; Galarza, E.; Goulart, N.B.A.; Lanferdini, F.J.; Tiggeman, C.L.; Dias, C.P. Effects of Tai Chi Chuan on the elderly balance: A semi-experimental study. Rev. Bras. Deger. Egerontol. 2014, 17, 373–381. [Google Scholar] [CrossRef]
- Zou, L.; Loprinzi, P.D.; Yu, J.J.; Yang, L.; Li, C.; Yeung, A.S.; Kong, Z.; Chiou, S.-Y.; Xiao, T. Superior Effects of Modified Chen-Style Tai Chi versus 24-Style Tai Chi on Cognitive Function, Fitness, and Balance Performance in Adults over 55. Brain Sci. 2019, 9, 102. [Google Scholar] [CrossRef]
- Li, Y.; Devault, C.N.; Oteghen, S.V. Effects of extended Tai Chi intervention on balance and selected motor functions of the elderly. The American Journal of Chinese Medicine 2007, 35, 383–391. [Google Scholar] [CrossRef] [PubMed]
- Lu, X.; Hui-Chan, C.W.Y.; Tsang, W.W.N. Effects of Tai Chi training on arterial compliance and muscle strength in female seniors: A randomized clinical trial. European J. Prev. Cardiol. 2012, 20, 238–245. [Google Scholar] [CrossRef] [PubMed]
- Sattin, R.W.; Easley, K.; Wolf, S.L.; Chen, Y.; Kutner, M.H. Reduction in fear of falling through intense Tai Chi exercise training in older, transitionally frail adults. J. Am. Geriatr. Soc. 2005, 53, 1168–1178. [Google Scholar] [CrossRef] [PubMed]
- Galantino, M.L.; Shepard, K.; Krafft, L.; LaPerriere, A.; Ducette, J.; Sorbello, A.; Barnish, M.; Condoluci, D.; Farrar, J.T. The effect of group aerobic exercise and Tai Chi on functional outcomes and quality of life for persons living with acquired immunodeficiency syndrome. J. Altern. Complement. Med. 2005, 11, 1085–1092. [Google Scholar] [CrossRef] [PubMed]
- Pei, Y.-C.; Chou, S.-W.; Lin, P.-S.; Lin, Y.-C.; Hsu, T.H.; Wong, A.M. Eye-hand coordination of elderly people who practice Tai Chi Chuan. J. Formos. Med. Assoc. 2008, 107, 103–110. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author | Location | Participants | Tai Chi Group | The Intervention of the Control Group | Duration | Outcome | ||||
|---|---|---|---|---|---|---|---|---|---|---|
| Age (Duration of Disease, Year) | Sample Size | Gender (M/F) | Intervention | Duration per Time (min) | Frequency (Times/Week) | |||||
| Tsang et al., 2007 [29] | Australia | T66 ± 8 (8.5 ± 2.0) C65 ± 8 (9.0 ± 0.7) | T18 C20 | T14/4 C14/6 | Tai Chi | 60 | 2 | Aerobics, gentle stretching, routine nursing | 16 weeks | ①; ⑤ |
| Richerson et al., 2007 [30] | United States | T72.92 ± 5.21 C74.50 ± 7.72 | T12 C6 | T12/0 C6/0 | Yang Tai Chi | 60 | 1 | Routine rehabilitation | 24 weeks | ① |
| Ahn et al., 2012 [23] | Korea | T66.05 ± 6.42 (7.66 ± 2.51) C62.73 ± 7.53 (7.97 ± 2.64) | T20 C19 | T12/8 C8/11 | Tai Chi | 60 | 2 | Routine rehabilitation | 12 weeks | ① |
| Quigley et al., 2013 [31] | United States | T68.4 ± 9.3 (7.9 ± 4.2) C167.6 ± 10.6 (8.0 ± 4.8) C267.5 ± 10.2 (10.1 ± 5.4) | T34 C134 C231 | T5/29 C14/30 C26/25 | Tai Chi | 60 | 1 | C1: Routine rehabilitation C2: Balance training | 10 weeks | ②; ⑥ |
| Cavegn et al., 2015 [24] | United States | T65.5 ± 7.4 (18.63 ± 9.21) C63.8 ± 5.7 | T8 C8 | T2/6 C2/6 | Yang Tai Chi | 60 | 3 | Routine rehabilitation | 8 weeks | ⑤; ⑥ |
| Zhao 2018 [40] | China | T57.51 ± 6.85 (6.17 ± 3.65) C56.92 ± 5.61 (5.64 ± 3.81) | T18 C18 | T14/4 C15/3 | 24-style Tai Chi | 60 | 7 | Routine rehabilitation | 12 weeks | ③; |
| Sun 2019 [41] | China | T58.78 ± 6.21 (7.96 ± 2.45) C157.86 ± 5.66 (7.75 ± 2.30) C258.55 ± 6.15 (7.28 ± 2.65) | T10 C110 C210 | T10/0 C110/0 C210/0 | 24-style Tai Chi | 60 | 7 | C1: Medication C2: 24-style Tai Chi with resistance training | 16 weeks | ①; |
| Strawberry et al., 2006 [13] | United States | T77.6 ± 7.0 C77.5 ± 5.5 | T11 C8 | T10/1 C7/1 | 27-style Tai Chi | 90 | 5 | Routine rehabilitation | 12 weeks | ②; ⑥ |
| Hermenns et al., 2018 [32] | United States | T74.5 (13.3) | T12 | T7/5 | Yang Tai Chi | 60 | 2 | Routine rehabilitation | 16 weeks | ①; ⑥ |
| Lee et al., 2012 [39] | United States | T70.2 ± 9.81 C72.7 ± 7.6 | T20 C17 | T17/3 C14/3 | 16-style Tai Chi | 45 | 1 | Routine rehabilitation | 8 weeks | ④ |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mao, W.; Wang, T.; Sun, M.; Zhang, F.; Li, L. Effects of Tai Chi on Postural Control in People with Peripheral Neuropathy: A Systematic Review with Meta-Analysis. Healthcare 2023, 11, 1559. https://doi.org/10.3390/healthcare11111559
Mao W, Wang T, Sun M, Zhang F, Li L. Effects of Tai Chi on Postural Control in People with Peripheral Neuropathy: A Systematic Review with Meta-Analysis. Healthcare. 2023; 11(11):1559. https://doi.org/10.3390/healthcare11111559
Chicago/Turabian StyleMao, Wenhui, Ting Wang, Mengzi Sun, Fangtong Zhang, and Li Li. 2023. "Effects of Tai Chi on Postural Control in People with Peripheral Neuropathy: A Systematic Review with Meta-Analysis" Healthcare 11, no. 11: 1559. https://doi.org/10.3390/healthcare11111559
APA StyleMao, W., Wang, T., Sun, M., Zhang, F., & Li, L. (2023). Effects of Tai Chi on Postural Control in People with Peripheral Neuropathy: A Systematic Review with Meta-Analysis. Healthcare, 11(11), 1559. https://doi.org/10.3390/healthcare11111559