

Pharmacological Treatment of Type-2-Diabetes and Cardiovascular Comorbidities: Differences between Undocumented Migrants and Natives in Italy

 ,
,  , , ,
, , ,  and
and
Abstract
1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Medicine
2.3. Statistical Analysis
3. Results
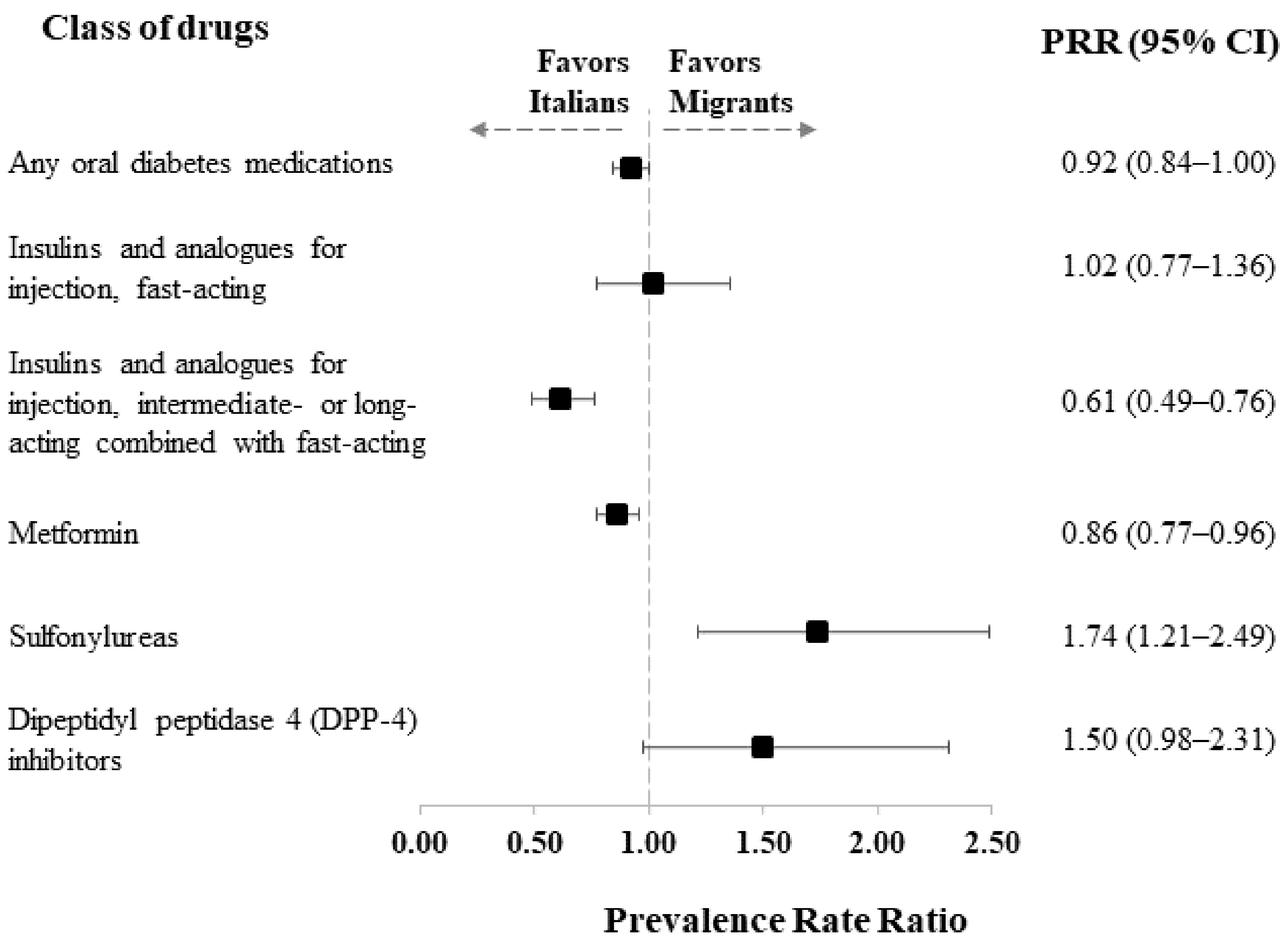
3.1. Antidiabetic Drugs
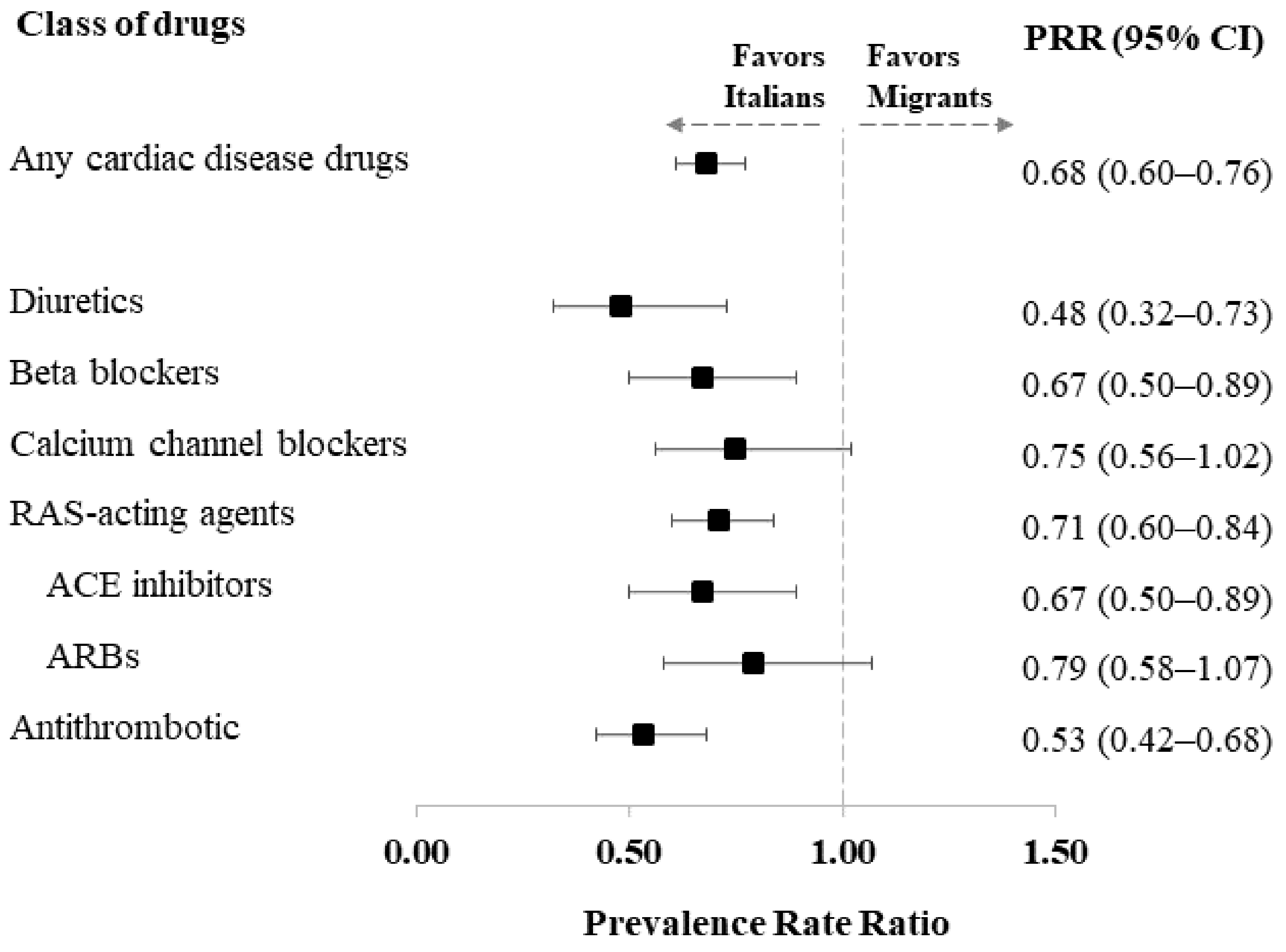
3.2. Cardiovascular Drugs
3.3. Sensitivity Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ogurdtova, K.; da Roch Fernandes, J.D.; Huang, Y.; Linnenkamp, U.; Guariguata, L.; Cho, N.H.; Cavan, D.; Shaw, J.E.; Makaroff, L.E. 2017 IDF Diabetes Atlas: Global Estimates for the Prevalence of Diabetes for 2015 and 2040. Diabetes Res. Clin. Pract. 2017, 128, 40–50. [Google Scholar] [CrossRef]
- Einarson, T.R.; Acs, A.; Ludwig, C.; Panton, U.H. Prevalence of cardiovascular disease in type 2 diabetes: A systematic literature review of scientific evidence from across the world in 2007–2017. Cardiovasc. Diabetol. 2018, 17, 83. [Google Scholar] [CrossRef] [PubMed]
- Damaskos, C.; Garmpis, N.; Kollia, P.; Mitsiopoulos, G.; Barlampa, D.; Drosos, A.; Patsouras, A.; Gravvanis, N.; Antoniou, V.; Litos, A.; et al. Assessing Cardiovascular Risk in Patients with Diabetes: An Update. Curr. Cardiol. Rev. 2020, 16, 266–274. [Google Scholar] [CrossRef] [PubMed]
- Petrie, J.R.; Guzik, T.; Touyz, R.M. Diabetes, Hypertension, and Cardiovascular Disease: Clinical Insights and Vascular Mechanisms. Can. J. Cardiol. 2018, 34, 575–584. [Google Scholar] [CrossRef] [PubMed]
- Jia, G.; Sowers, J.R. Hypertension in diabetes: An update of basic mechanisms and clinical disease. Hypertension 2021, 78, 1197–1205. [Google Scholar] [CrossRef] [PubMed]
- Fox, C.S. Cardiovascular disease risk factors, type 2 diabetes melliyus, and the Framingham heart study. Trends Cardiovasc. Med. 2010, 20, 90–95. [Google Scholar] [CrossRef]
- Sowers, J.R. Diabetes mellitus and vascular diseases. Hypertension 2013, 61, 943–947. [Google Scholar] [CrossRef]
- Carson, A.P.; Howard, G.; Burke, G.L.; Shea, S.; Levitan, E.B.; Muntner, P. Ethnic differences in hypertension incidence among middle-aged and older adults: The multi-ethnic study of atherosclerosis. Hypertension 2011, 57, 1101–1107. [Google Scholar] [CrossRef]
- Piccolo, R.S.; Subramanina, S.V.; Pearce, N.; Florez, J.C.; MvKinlay, J.B. Relative Contributions of Socioeconomic, Local Environmental, Psychosocial, Lifestyle/Behavioral, Biophysiological, and Ancestral Factors to Racial/Ethnic Disparities in Type 2 Diabetes. Diabetes Care 2016, 39, 1208–1217. [Google Scholar] [CrossRef]
- American Diabetes Association. Cardiovascular disease and risk management: Standards of Medical Care in Diabetes—2022. Diabetes Care 2022, 45 (Suppl. 1), S144–S174. [Google Scholar] [CrossRef]
- Sarria-Santamera, A.; Alexeyeva, Z.; Yen Chan, M.; Ortega, M.A.; Asunsolo-Del-Barco, A.; Navarro-García, C. Direct and Indirect Costs Related to Physical Activity Levels in Patients with Diabetes Mellitus in Spain: A Cross-Sectional Study. Healthcare 2022, 10, 752. [Google Scholar] [CrossRef]
- Fiorini, G.; Cerri, C.; Bini, S.; Rigamonti, A.E.; Perlini, S.; Marazzi, N.; Sartorio, A.; Cella, S.G. The burden of chronic noncommunicable diseases in undocumented migrants: A 1-year survey of drugs dispensation by a non-governmental organization in Italy. Public Health 2016, 141, 26–31. [Google Scholar] [CrossRef]
- Fiorini, G.; Milani, S.; Pincelli, A.I.; Calella, D.; Galliani, S.; Badalamenti, S.; Rigamonti, A.E.; Marazzi, N.; Sartorio, A.; Cella, S.G. Will undocumented migrants contribute to change epidemiology, presentation and pharmacologic treatment of diabetes in Western countries? Prim. Care Diabetes 2020, 14, 21–28. [Google Scholar] [CrossRef]
- Rossi, M.C.; Lucisano, G.; Comaschi, M.; Coscelli, C.; Cucinotta, D.; Di Blasi, P.; Bader, G.; Pellegrini, F.; Valentini, U.; Vespasiani, G.; et al. Quality of diabetes care predicts the development of cardiovascular events: Results of the AMD-QUASAR Study. Diabetes Care 2011, 34, 347–352. [Google Scholar] [CrossRef]
- Mannucci, E.; Candido, R.; Delle Monache, L.; Gallo, M.; Giaccari, A.; Masini, M.L.; Mazzone, A.; Medea, G.; Pintaudi, B.; Targher, G.; et al. Italian guidelines for the treatment of type 2 diabetes. Acta Diabetol. 2022, 59, 579–622. [Google Scholar] [CrossRef]
- NICE Guideline NG28. Type 2 Diabetes in Adults: Management. Last Updated 29 June 2022. NICE, 2022. Available online: nice.org.uk/guidance/ng28 (accessed on 29 June 2022).
- American Diabetes Association Professional Practice Committee; Draznin, B.; Aroda, V.R.; Bakris, G.; Benson, G.; Brown, F.M.; Freeman, R.; Green, J.; Huang, E.; Isaacs, D.; et al. Pharmacologic Approaches to Glycemic Treatment: Standards of Medical Care in Diabetes—2022. Diabetes Care 2022, 45 (Suppl. 1), S125–S143. [Google Scholar] [CrossRef]
- Thulé, P.M.; Umpierrez, G. Sulfonylureas: A new look at old therapy. Curr. Diab. Rep. 2014, 14, 473. [Google Scholar] [CrossRef]
- Liu, H.; Guo, L.; Xing, J.; Li, P.; Sang, H.; Hu, X.; Du, Y.; Zhao, L.; Song, R.; Gu, H. The protective role of DPP4 inhibitors in atherosclerosis. Eur. J. Pharmacol. 2020, 15, 875–173037. [Google Scholar] [CrossRef]
- Al-Rubeaan, K.; Alsayed, M.; Ben-Nakhi, A.; Bayram, F.; Echtay, A.; Hadaoui, A.; Hafidh, K.; Kennedy, K.; Kok, A.; Malek, R.; et al. Characteristics and Treatment Patterns of Patients with Type 2 Diabetes Mellitus in the Middle East and Africa Cohort of the DISCOVER Study Program: A Prospective Study. Diabetes Ther. 2022, 13, 1339–1352. [Google Scholar] [CrossRef]
- Verma, S.; McGuire, D.K.; Bain, S.C.; Bhatt, D.L.; Leiter, L.A.; Mazer, C.D.; Monk Fries, T.; Pratley, R.E.; Rasmussen, S.; Vrazic, H.; et al. Effects of glucagon-like peptide-1 receptor agonists liraglutide and semaglutide on cardiovascular and renal outcomes across body mass index categories in type 2 diabetes: Results of the LEADER and SUSTAIN 6 trials. Diabetes Obes. Metab. 2020, 22, 2487–2492. [Google Scholar] [CrossRef]
- Ahlqvist, E.; Storm, P.; Käräjämäki, A.; Martinell, M.; Dorkhan, M.; Carlsson, A.; Vikman, P.; Prasad, R.B.; Aly, D.M.; Almgren, P.; et al. Novel subgroups of adult-onset diabetes and their association with outcomes: A data-driven cluster analysis of six variables. Lancet Diabetes Endocrinol. 2018, 6, 361–369. [Google Scholar] [CrossRef] [PubMed]
- Fiorini, G.; Cortinovis, I.; Corrao, G.; Franchi, M.; Pincelli, A.I.; Perotti, M.; Rigamonti, A.E.; Sartorio, A.; Cella, S.G. Current Pharmacological Treatment of Type 2 Diabetes Mellitus in Undocumented Migrants: Is It Appropriate for the Phenotype of the Disease? Int. J. Environ. Res. Public Health 2020, 17, 8169. [Google Scholar] [CrossRef] [PubMed]
- Mannino, G.C.; Andreozzi, F.; Sesti, G. Pharmacogenetics of type 2 diabetes mellitus, the route toward tailored medicine. Diabetes Metab. Res. Rev. 2019, 35, e3109. [Google Scholar] [CrossRef] [PubMed]
- Bonora, E.; Cataudella, S.; Marchesini, G.; Miccoli, R.; Vaccaro, O.; Fadini, G.P.; Martini, N.; Rossi, E.; Mandate of the Italian Diabetes Society. Initial treatment of diabetes in Italy. A nationwide population-based study from of the ARNO Diabetes Observatory. Nutr. Metab. Cardiovasc. Dis. 2021, 31, 2661–2668. [Google Scholar] [CrossRef] [PubMed]
- Wright, A.; Burden, A.C.; Paisey, R.B.; Cull, C.A.; Holman, R.R.; U.K. Prospective Diabetes Study Group. Sulfonylurea inadequacy: Efficacy of addition of insulin over 6 years in patients with type 2 diabetes in the U.K. Prospective Diabetes Study (UKPDS 57). Diabetes Care 2002, 25, 330–336. [Google Scholar] [CrossRef]
- Khunti, K.; Gomes, M.B.; Pocock, S.; Shestakova, M.V.; Pintat, S.; Fenici, P.; Hammar, N.; Medina, J. Therapeutic inertia in the treatment of hyperglycaemia in patients with type 2 diabetes: A systematic review. Diabetes Obes. Metab. 2018, 20, 427–437. [Google Scholar] [CrossRef]
- Saleh, J. Glycated hemoglobin and its spinoffs: Cardiovascular disease markers or risk factors? World J. Cardiol. 2015, 7, 449–453. [Google Scholar] [CrossRef]
- Rezende, P.C.; Hlatky, M.A.; Hueb, W.; Garcia, R.M.R.; da Silva Selistre, L.; Lima, E.G.; Garzillo, C.L.; Scudeler, T.L.; Boros, G.A.B.; Ribas, F.F.; et al. Association of Longitudinal Values of Glycated Hemoglobin With Cardiovascular Events in Patients With Type 2 Diabetes and Multivessel Coronary Artery Disease. JAMA Netw. Open 2020, 3, e1919666. [Google Scholar] [CrossRef]
- Saeedi, P.; Petersohn, I.; Salpea, P.; Malanda, B.; Karuranga, S.; Unwin, N.; Colagiuri, S.; Guariguata, L.; Motala, A.A.; Ogurtsova, K.; et al. IDF Diabetes Atlas Committee. Global and regional diabetes prevalence estimates for 2019 and projections for 2030 and 2045: Results from the International Diabetes Federation Diabetes Atlas, 9th edition. Diabetes Res. Clin. Pract. 2019, 157, 107843. [Google Scholar] [CrossRef]
- Wolf, R.M.; Nagpal, M.; Magge, S.N. Diabetes and cardiometabolic risk in South Asian youth: A review. Pediatr. Diabetes 2021, 22, 52–66. [Google Scholar] [CrossRef]
- Agyemang, C.; van der Linden, E.L.; Bennet, L. Type 2 diabetes burden among migrants in Europe: Unravelling the causal pathways. Diabetologia 2021, 64, 2665–2675. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Characteristics | Total Subjects | Undocumented Migrants | Italians | Missing Data | p-Value |
|---|---|---|---|---|---|
| n = 838 | n = 413 | n = 425 | |||
| Age in years, median (IQR) | 60.0 (15) | 54 (15) | 65 (14) | <0.0001 | |
| <50 | 160 (19.1) | 138 (33.4) | 22 (8.2) | <0.0001 | |
| 50–59 | 245 (29.2) | 155 (37.5) | 90 (21.2) | ||
| 60–69 | 246 (29.1) | 85 (20.6) | 161 (37.9) | ||
| ≥70 | 187 (22.3) | 35 (8.5) | 152 (35.8) | ||
| Age at diagnosis, median (IQR) | 49 (15) | 45 (15) | 52 (14) | 72 | <0.0001 |
| Female | 334 (39.9) | 171 (41.4) | 163 (38.4) | 0.3671 | |
| Nationality, n (%) | - | ||||
| Italian | 425 (51.2) | - | 425 (100.0) | ||
| Eastern Europe | 95 (11.5) | 95 (23.5) | - | ||
| Mediterranean Africa | 63 (8.6) | 63 (15.6) | - | ||
| Sub-Saharan Africa | 37 (4.5) | 37 (9.2) | - | ||
| Central Asia | 1 (0.1) | 1 (0.3) | - | ||
| South Asia | 80 (9.6) | 80 (19.8) | - | ||
| East Asia | 28 (3.4) | 28 (6.9) | - | ||
| Latin America | 101 (12.2) | 101 (24.9) | - | ||
| BMI, mean (SD) | 29.4 (6.4) | 28.6 (6.9) | 30.2 (5.9) | 30 | 0.0003 |
| Familiarity for diabetes | 509 (65.3) | 181 (43.8) | 328 (77.2) | 58 | <0.0001 |
| Cardiovascular disease risk factors | 731 (88.0) | 329 (79.7) | 402 (94.6) | 7 | <0.0001 |
| Risk behaviors | 253 (30.2) | 114 (27.6) | 139 (32.7) | 142 | <0.0001 |
| Hospitalization for diabetes | 141 (17.0) | 129 (31.2) | 12 (2.8) | 7 | <0.0001 |
| HbA1C, mean (SD) | 7.8 (1.8) | 8.6 (2.1) | 7.2 (1.1) | 66 | <0.0001 |
| Glycosuria | 238 (31.8) | 148 (35.8) | 90 (21.2) | 90 | <0.0001 |
| Ketonuria | 18 (2.3) | 14 (3.4) | 4 (0.9) | 96 | 0.0030 |
| Cardiovascular disease | 195 (23.3) | 79 (19.1) | 116 (27.3) | 2 | 0.0058 |
| Diabetic nephropathy | 131 (16.3) | 80 (19.4) | 51 (12.4) | 34 | 0.0025 |
| Diabetic retinopathy | 166 (21.2) | 79 (19.1) | 87 (20.5) | 54 | 0.7353 |
| Diabetic neuropathy | 82 (11.6) | 29 (7.0) | 53 (17.2) | 129 | <0.0001 |
| Ulcers | 50 (6.1) | 41 (9.9) | 9 (2.1) | 15 | <0.0001 |
| Q-score, mean (SD) | 23.3 | 22.2 (9.3) | 24.4 (8.6) | 0.0005 |
| Type of Drug | ATC Code | Total Subjects | Undocumented Migrants | Italians | p-Value |
|---|---|---|---|---|---|
| n = 838 | n = 413 | n = 425 | |||
| Any oral diabetes medications | 643 (76.9) | 299 (72.6) | 344 (81.1) | 0.0033 | |
| Insulins and analogues for injection, fast-acting | A10AB | 216 (25.8) | 111 (26.9) | 105 (24.8) | 0.4850 |
| Insulins and analogues for injection, intermediate- or long-acting combined with fast-acting | A10AE, A10AD | 344 (41.1) | 139 (33.7) | 205 (48.4) | <0.0001 |
| Metformin | A10BA02 | 581 (69.3) | 263 (63.7) | 318 (74.8) | 0.0005 |
| Sulfonylureas | A10BB, A10BC, A10BD01, A10BD02, A10BD04, A10BD06 | 143 (17.1) | 85 (20.6) | 58 (13.7) | 0.0076 |
| Glinides | A10BX02, A10BX03, A10BX08, A10BD14 | 13 (1.6) | 2 (0.5) | 11 (2.6) | 0.0137 |
| Alpha glucosidase inhibitors | A10BF | 16 (1.9) | 6 (1.5) | 10 (2.4) | 0.3411 |
| Thiazolidinediones | A10BG | 11 (1.3) | 3 (0.7) | 8 (1.9) | 0.1416 |
| Dipeptidyl peptidase 4 (DPP-4) inhibitors | A10BH, A10BD07, A10BD08; A10BD10, A10BD11, A10BD13, A10BD18 | 96 (11.5) | 54 (13.1) | 42 (9.9) | 0.1468 |
| Glucagon-like peptide-1 (GLP-1) analogues | A10BJ, A10BX04, A10BX07, A10BX10, A10BX13, A10BX14 | 59 (7.0) | 0 (0.0) | 59 (13.9) | <0.0001 |
| Sodium–glucose co-transporter 2 (SGLT2) inhibitors | A10BK, A10BX09, A10BX11, A10BX12, A10BD15, A10BD16, A10BD20 | 52 (6.2) | 7 (1.7) | 45 (10.6) | <0.0001 |
| Other blood glucose-lowering drugs, excl. insulins | A10BX | 31 (3.7) | 16 (3.9) | 15 (3.5) | 0.7916 |
| Disease | ATC Code | Total Subjects | Undocumented Migrants | Italians | p-Value |
|---|---|---|---|---|---|
| n = 838 | n = 413 | n = 425 | |||
| Any heart and vessels disease drugs | C01, C02, C03, C05, C07, C08, C09, B01 | 564 (67.3) | 210 (50.9) | 354 (83.3) | <0.0001 |
| Cardiac therapy | C01 | 53 (6.3) | 17 (4.1) | 36 (8.5) | 0.0096 |
| Antihypertensives | C02 | 35 (4.2) | 3 (0.8) | 32 (7.5) | <0.0001 |
| Diuretics | C03 | 136 (16.2) | 30 (7.3) | 106 (24.9) | <0.0001 |
| Vasoprotectives | C05 | 0 | - | - | - |
| Beta blockers | C07 | 205 (24.5) | 69 (16.7) | 136 (32.0) | <0.0001 |
| Calcium channel blockers | C08 | 198 (23.6) | 80 (19.4) | 118 (27.8) | 0.0042 |
| Renin–angiotensin system (RAS)-acting agents | C09 | 440 (52.5) | 166 (40.2) | 274 (64.5) | <0.0001 |
| ACE inhibitors | C09A, C09B | 234 (27.9) | 85 (20.6) | 149 (35.1) | <0.0001 |
| ARBs | C09C, C09D | 212 (25.3) | 84 (20.3) | 128 (30.1) | 0.0011 |
| Antithrombotics | B01 | 271 (32.3) | 73 (17.7) | 198 (46.6) | <0.0001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fiorini, G.; Pellegrini, G.; Franchi, M.; Pincelli, A.I.; Rigamonti, A.E.; Corrao, G.; Sartorio, A.; Cella, S.G. Pharmacological Treatment of Type-2-Diabetes and Cardiovascular Comorbidities: Differences between Undocumented Migrants and Natives in Italy. Healthcare 2023, 11, 4. https://doi.org/10.3390/healthcare11010004
Fiorini G, Pellegrini G, Franchi M, Pincelli AI, Rigamonti AE, Corrao G, Sartorio A, Cella SG. Pharmacological Treatment of Type-2-Diabetes and Cardiovascular Comorbidities: Differences between Undocumented Migrants and Natives in Italy. Healthcare. 2023; 11(1):4. https://doi.org/10.3390/healthcare11010004
Chicago/Turabian StyleFiorini, Gianfrancesco, Giacomo Pellegrini, Matteo Franchi, Angela Ida Pincelli, Antonello Emilio Rigamonti, Giovanni Corrao, Alessandro Sartorio, and Silvano Gabriele Cella. 2023. "Pharmacological Treatment of Type-2-Diabetes and Cardiovascular Comorbidities: Differences between Undocumented Migrants and Natives in Italy" Healthcare 11, no. 1: 4. https://doi.org/10.3390/healthcare11010004
APA StyleFiorini, G., Pellegrini, G., Franchi, M., Pincelli, A. I., Rigamonti, A. E., Corrao, G., Sartorio, A., & Cella, S. G. (2023). Pharmacological Treatment of Type-2-Diabetes and Cardiovascular Comorbidities: Differences between Undocumented Migrants and Natives in Italy. Healthcare, 11(1), 4. https://doi.org/10.3390/healthcare11010004