Sexual Function, Physical Activity, Mean Amplitudes and Maximal Voluntary Contraction of Pelvic Floor Muscles Are Related to Handgrip Strength: A Cross-Sectional Study

 ,
, 
Abstract
1. Introduction
2. Methods
2.1. Study Design
2.2. Setting and Period of Study
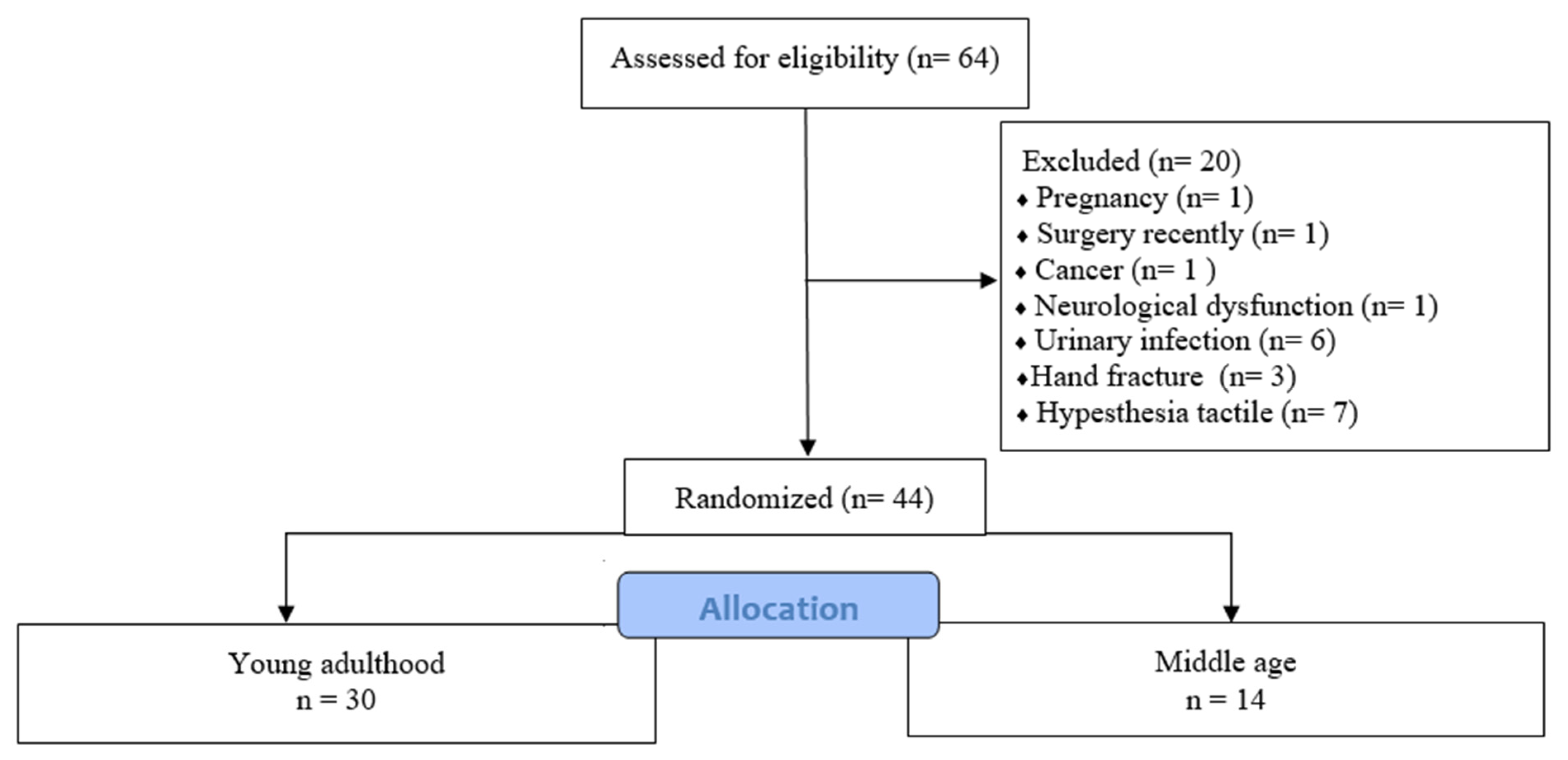
2.3. Population
2.4. Eligibility Criteria
2.5. Sampling
2.6. Sample Size
2.7. Data Collection and Variables
2.8. Primary Outcomes
2.8.1. Handgrip Strength (HGS)
2.8.2. Level of Strength of the Pelvic Floor Muscles
2.8.3. Bioelectrical Activity of the Pelvic Floor Muscles
2.9. Secondary Outcomes
2.9.1. Physical Activity
2.9.2. The Sexual Quotient—Female Version (SQ-F) Questionnaire
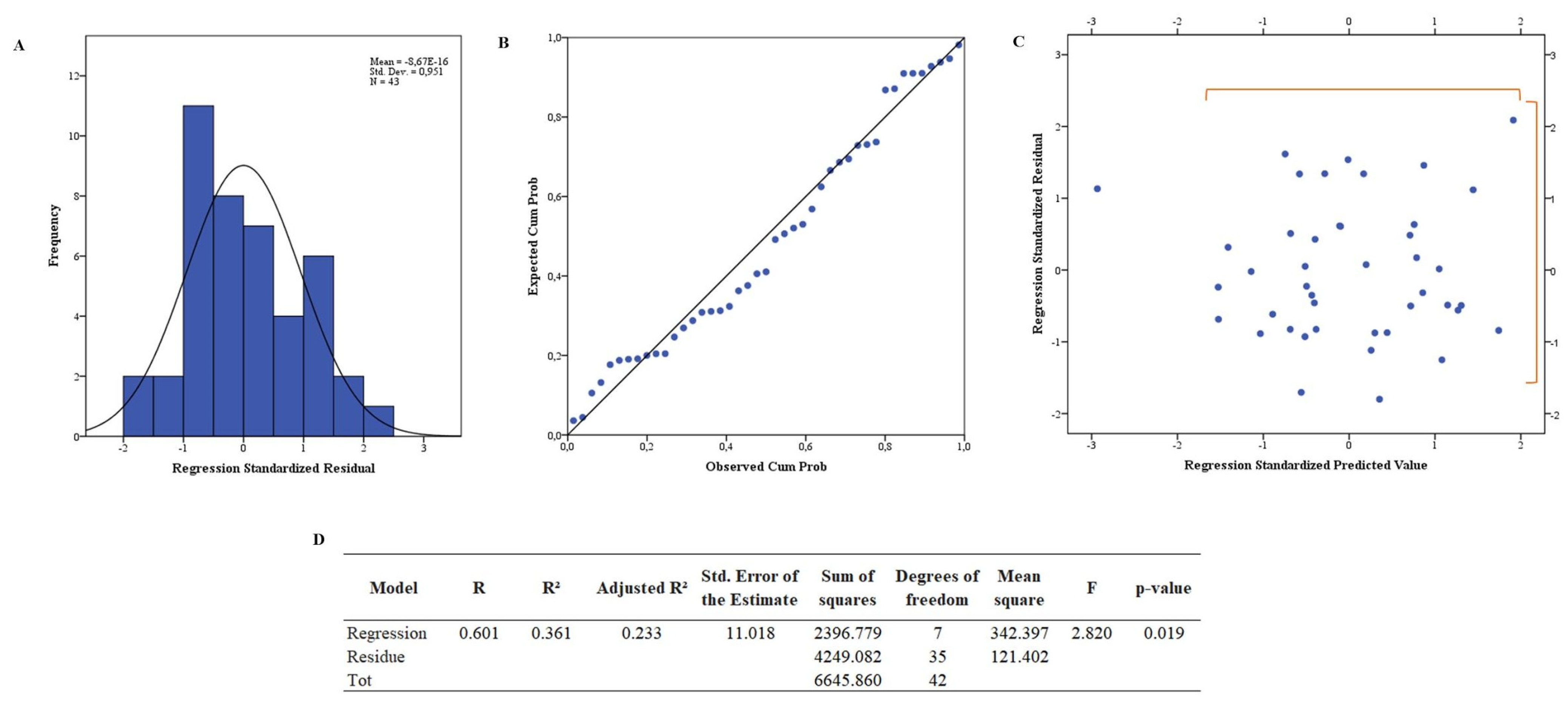
2.10. Statistical Analysis
3. Results
4. Discussion
5. Limitations of the Study
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Eickmeyer, S.M. Anatomy and Physiology of the Pelvic Floor. Phys. Med. Rehabil. Clin. N. Am. 2017, 28, 455–460. [Google Scholar] [CrossRef] [PubMed]
- Moore, K.L.; Daley, A.F., II. Anatomia Orientada Para a Clínica, 7th ed.; Guanabara Koogan: Rio de Janeiro, Brasil, 2014. [Google Scholar]
- Ubukata, H.; Maruyama, H.; Huo, M. Reliability of measuring pelvic floor elevation with a diagnostic ultrasonic imaging device. J. Phys. Ther. Sci. 2015, 27, 2495–2497. [Google Scholar] [CrossRef] [PubMed]
- Staskin, D.; Kelleher, C.; Avery, K.; Bosch, R.; Cotterill, N.; Coyne, K.; Emmanuel, A.; Yoshida, M.; Kopp, Z. Initial assessment of urinary and faecal incontinence in adult male and female patients. In Incontinence: 4th International Consultation on Incontinence; Health Publications: Paris, France, 2009; pp. 311–412. [Google Scholar]
- Pereira, V.S.; Hirakawa, H.S.; Oliveira, A.B.; Driusso, P. Relationship among vaginal palpation, vaginal squeeze pressure, electromyographic and ultrasonographic variables of female pelvic floor muscles. Braz. J. Phys. Ther. 2014, 18, 428–434. [Google Scholar] [CrossRef] [PubMed]
- Rantanen, T.; Volpato, S.; Ferrucci, L.; Heikkinen, E.; Fried, L.P.; Guralnik, J.M. Handgrip strength and cause-specific and total mortality in older disabled women: Exploring the mechanism. J. Am. Geriatr. Soc. 2003, 51, 636–641. [Google Scholar] [CrossRef] [PubMed]
- Baschung, P.P.; de Bruin, E.D.; Sterkele, I.; Maurer, B.; de Bie, R.A.; Knols, R.H. Manual muscle testing and hand-held dynamometry in people with inflammatory myopathy: An intra- and interrater reliability and validity study. PLoS ONE 2018, 13, e0194531. [Google Scholar] [CrossRef]
- Nascimento, M.D.; Benassi, R.; Caboclo, F.D.; Salvador, A.D.S.; Gonçalves, L.C.O. Valores de referência de força de preensão manual em ambos os gêneros e diferentes grupos etários. Um estudo de revisão. Lect. Educ. Física Y Deport. 2010, 15, 151. [Google Scholar]
- Saraiva, W.S.; Prestes, J.; Funghetto, S.S.; Navalta, J.W.; Tibana, R.A.; da Cunha Nascimento, D. Relation Between Relative Handgrip Strength, Chronological Age and Physiological Age with Lower Functional Capacity in Older Women. J. Sports Med. 2019, 20, 185–190. [Google Scholar] [CrossRef]
- dos Reis Ferreira, T.C.; Godinho, A.A.; de MELO, A.R.; Rezende, R.T. Avaliação da força muscular do assoalho pélvico em mulheres sedentárias e que praticam atividade física. Rev. Da Univ. Val. Do Rio Verde 2015, 13, 450–464. [Google Scholar]
- Gonçalves, M.L.C.; Fernandes, S.; Batista, S.J. Do moderate aerobic exercise and strength training influence electromyographic biofeedback of the pelvic floor muscles in female non-athletes? J. Phys. Ther. Sci. 2018, 30, 313–319. [Google Scholar] [CrossRef]
- Martinez, C.S.; Ferreira, F.V.; Castro, A.A.; Gomide, L.B. Women with greater pelvic floor muscle strength have better sexual function. Acta Obs. Gynecol. Scand. 2014, 93, 497–502. [Google Scholar] [CrossRef]
- Franco, M.D.M.; Driusso, P.; Bø, K.; de Abreu, D.C.C.; Lara, L.A.D.S.; Silva, A.C.J.D.S.R.E.; Ferreira, C.H.J. Relationship between pelvic floor muscle strength and sexual dysfunction in postmenopausal women: A cross-sectional study. Int. Urogynecol. J. 2017, 28, 931–936. [Google Scholar] [CrossRef]
- Petry, N.M.A. Comparison of young, middle-aged, and older adult treatment-seeking pathological gamblers. Gerontologist 2002, 42, 92–99. [Google Scholar] [CrossRef]
- Baden, W.F.; Walker, T.A.; Lindsey, J.H. The vaginal profile. Tex. Med. 1968, 5, 56–58. [Google Scholar]
- Hwang, U.; Lee, M.; Jung, S.; Ahn, S.; Kwon, O. Relationship Between Sexual Function and Pelvic Floor and Hip Muscle Strength in Women With Stress Urinary Incontinence. Sex. Med. 2021, 9, 100325. [Google Scholar] [CrossRef]
- Longstreth, G.F.; Thompson, W.G.; Chey, W.D.; Houghton, L.A.; Mearin, F.; Spiller, R.C. Functional bowel disorders. Gastroenterology 2006, 130, 1480–1491. [Google Scholar] [CrossRef]
- Laycock, J.; Jerwood, D. Pelvic Floor Muscle Assessment: The PERFECT Scheme. Physiother. J. 2001, 87, 631–642. [Google Scholar] [CrossRef]
- Sch, B.; Laycock, J.; Norton, P.A.; Stanton, S.L. Pelvic Floor Re-Education: Principles and Practice; Springer Science & Business Media: Berlin/Heidelberg, Germany, 1994. [Google Scholar]
- Chevalier, F.; Fernandez-Lao, C.; Cuesta-Vargas, A.I. Normal reference values of strength in pelvic floor muscle of women: A descriptive and inferential study. BMC Women’s Health 2014, 14, 143. [Google Scholar] [CrossRef][Green Version]
- Madill, S.J.; McLean, L. Quantification of abdominal and pelvic floor muscle synergies in response to voluntary pelvic floor muscle contractions. J. Electromyogr. Kinesiol. 2008, 18, 955–964. [Google Scholar] [CrossRef]
- Matsudo, S.; Araújo, T.; Marsudo, V.; Andrade, D.; Andrade, E.; Braggion, G. Questionário Internacional de Atividade Física (IPAQ): Estudo de validade e reprodutibilidade no Brasil. Rev. Bras. Ativ. Fís. Saúde 2001, 6, 5–12. [Google Scholar]
- Abdo, C. Quociente sexual feminino: Um questionário brasileiro para avaliar a atividade sexual da mulher. Diagn. Tratamento 2009, 14, 89–90. [Google Scholar]
- Vianna, L.C.; Oliveira, R.B.; Araújo, C.G.S. Age-related decline in handgrip strength differs according to gender. J. Strength Cond. Res. 2007, 21, 1310–1314. [Google Scholar]
- Bocardi, D.A.S.; Pereira-Baldon, V.S.; Ferreira, C.H.J.; Avila, M.A.; Beleza, A.C.S.; Driusso, P. Pelvic floor muscle function and EMG in nulliparous women of different ages: A cross-sectional study. Climacteric 2018, 21, 462–466. [Google Scholar] [CrossRef]
- Swenson, C.W.; Masteling, M.; DeLancey, J.O.; Nandikanti, L.; Schmidt, P.; Chen, L. Aging Effects on Pelvic Floor Support: A Pilot Study Comparing Young versus Older Nulliparous Women. Int. Uroginecol. J. 2020, 31, 535–543. [Google Scholar] [CrossRef]
- Soytas, R.B.; Soytas, M.; Danacioglu, Y.O.; Citgez, S.; Yavuzer, H.; Can, G.; Onal, B.; Doventas, A. Relationship between the types of urinary incontinence, handgrip strength, and pelvic floor muscle strength in adult women. Neurourol. Urodyn. 2021, 40, 1532–1538. [Google Scholar] [CrossRef]
- Haslam, J.; Laycock, J. Therapeutic Management of Incontinence and Pelvic Pain: Pelvic Organ Disorders, 2nd ed.; Springer: London, UK, 2008. [Google Scholar]
- Farina, D.; Merletti, R.; Enoka, R.M. The extraction of neural strategies from the surface EMG: An update. J. Appl. Physiol. 2014, 117, 1215–1230. [Google Scholar] [CrossRef]
- De Luccas Batista, N.M.T.; Oliveira, N.A.; Nunes, E.F.C.; Latorre, G.F.S. Força e coordenação motora da musculatura do assoalho pélvico e a função sexual feminina. IJHE-Interdiscip. J. Health Educ. 2017, 2, 10–15. [Google Scholar] [CrossRef]
- Sartori, D.V.B.; Kawano, P.R.; Yamamoto, H.A.; Guerra, R.; Pajolli, P.R.; Amaro, J.L. Pelvic floor muscle strength is correlated with sexual function. Investig. Clin. Urol. 2021, 62, 79–84. [Google Scholar] [CrossRef]
- Omar, S.Z.; Mohktar, M.S.; Ibrahim, F.; Rozi, N.F.M.; Yusof, J.M.; Ahmad, S.A.; Yen, K.S. A quantitative approach to measure women’s sexual function using electromyography: A preliminary study of the Kegel exercise. Med. Sci. Monit. 2013, 19, 1159–1166. [Google Scholar] [CrossRef]
- Sartori, D.V.B.; de Souza, J.P.; Carneiro, P.R. A influência da obesidade na musculatura do assoalho pélvico em mulheres continentes. Ensaios e Ciência Ciências Biológicas, Agrárias e da Saúde 2011, 15, 3. [Google Scholar]
- Bø, K.; Nygaard, I.E. Is Physical Activity Good or Bad for the Female Pelvic Floor? A Narrative Review. Sports Med. 2020, 50, 471–484. [Google Scholar] [CrossRef] [PubMed]
- Nygaard, I.; Girts, T.; Fultz, N.H.; Kinchen, K.; Pohl, G.; Sternfeld, B. Is urinary incontinence a barrier to exercise in women? Obstet. Gynecol. 2005, 106, 307–314. [Google Scholar] [CrossRef] [PubMed]
- Carvalhais, A.; Da Roza, T.; Vilela, S.; Jorge, R.N.; Bø, K. Association Between Physical Activity Level and Pelvic Floor Muscle Variables in Women. Int. J. Sports Med. 2018, 39, 995–1000. [Google Scholar] [CrossRef] [PubMed]
- Frezza, E.E.; Shebani, K.O.; Robertson, J.; Wachtel, M.S. Morbid obesity causes chronic increase of intraabdominal pressure. Dig. Dis. Sci. 2007, 52, 1038–1041. [Google Scholar] [CrossRef]
- Bordoni, B.; Sugumar, K.; Leslie, S.W. Anatomy, Abdomen and Pelvis, Pelvic Floor; StatPearls Publishing: Treasure Island, FL, USA, 2022. [Google Scholar]



{kind=link}
{kind=link}
| Young Adulthood (n = 30) | Middle Age (n = 14) | t or Z or χ2 | p-Value | |
|---|---|---|---|---|
| Age (years) | 24.3 ± 3.28 | 43.36 ± 7.28 | −9.359 | <0.0001 # |
| Race/color (%) | 2.598 | 0.458 | ||
| Black | 13.33 | 7.14 | ||
| Brown | 60.00 | 64.29 | ||
| White | 26.66 | 21.43 | ||
| Yellow | 0.00 | 7.14 | ||
| Scholarity (%) | 4.490 | 0.106 | ||
| Elementary school | 0.00 | 14.28 | ||
| Secondary school | 50.00 | 42.86 | ||
| Higher education | 50.00 | 42.86 | ||
| Marital status (%) | 22.269 | <0.0001 * | ||
| Single | 86.66 ▀ | 14.28 | ||
| Stable union | 0.00 | 14.28 ▀ | ||
| Divorced | 13.33 | 71.43 ▀ | ||
| Family income (%) | 0.496 | 0.920 | ||
| <1 minimum wage | 20.00 | 21.43 | ||
| >1 and ≤2 minimum wages | 20.00 | 21.43 | ||
| >3 and ≤4 minimum wages | 23.33 | 14.28 | ||
| >4 minimum wage | 36.66 | 42.86 | ||
| Height (m) | 1.60 (0.11) | 1.56 (0.12) | −2.008 | 0.045 ♰ |
| Weight (kg) | 62.06 ± 10.27 | 63.92 ± 9.64 | −0.554 | 0.583 |
| BMI (kg/m2) | 23.03 (4.31) | 26.22 (4.06) | −1.933 | 0.053 |
| Young Adulthood (%) | Middle Age (%) | χ2 | p-Value | |
|---|---|---|---|---|
| Hormone replacement | 6.66 | 7.14 | 0.003 | 0.953 |
| Pregnancy | 25.611 | <0.0001 * | ||
| 0 | 83.33 ▀ | 14.28 | ||
| 1 | 13.33 | 21.43 | ||
| 2 | 3.33 | 42.86 ▀ | ||
| 3 | 0.00 | 21.43 | ||
| Abortion | ||||
| 0 | 0.00 | 7.14 | 6.267 | 0.044 * |
| 1 | 3.33 | 21.43 ▀ | ||
| 2 | 0.00 | 7.14 | ||
| Active sexual life | 86.66 | 64.29 | 2.939 | 0.086 |
| Urinary disorders | ||||
| Nocturia | 33.33 | 35.71 | 0.024 | 0.877 |
| Preventive urination | 50.00 | 64.29 | 0.786 | 0.375 |
| Urinary tenesmus | 43.33 | 64.29 | 1.676 | 0.195 |
| Urinary tract infection (last 3 months) | 6.66 | 14.28 | 0.003 | 0.953 |
| Enuresis | 23.33 | 50.00 | 3.129 | 0.077 |
| Urinary urgency | 30.00 | 28.57 | 0.009 | 0.923 |
| Urge urinary incontinence | 6.66 | 14.28 | 0.670 | 0.413 |
| Stress urinary incontinence | 43.33 | 57.14 | 0.730 | 0.393 |
| Dysuria | 10.00 | 7.14 | 0.094 | 0.759 |
| Anal dysfunctions | ||||
| Constipation (ROMA III) | 40.00 | 42.86 | 0.032 | 0.858 |
| Fecal urgency | 10.00 | 28.57 | 2.461 | 0.117 |
| Fecal tenesmus | 36.66 | 21.43 | 1.022 | 0.312 |
| Soiling | 13.33 | 21.43 | 0.468 | 0.494 |
| Fecal leakage | 0.00 | 7.14 | 2.193 | 0.139 |
| Hemorrhoids | 13.33 | 7.14 | 0.363 | 0.547 |
| Young Adulthood (n = 30) | Middle Age (n = 14) | t or U or χ2 | p-Value | |
|---|---|---|---|---|
| Handgrip strength | 53.27 ± 10.46 | 53.14 ± 17.01 | 0.025 | 0.980 |
| Power/Pressure | 3 (1) | 3 (2) | −1.747 | 0.081 |
| sEMG | ||||
| MVC (µv) | 36.5 (18) | 31 (25) | −1.152 | 0.250 |
| Peak (0 to 10 s) | 101.90 ± 14.56 | 101.38 ± 12.44 | 0.118 | 0.907 |
| Peak (%MCV) | 101 (16.75) | 99 (20) | −0.053 | 0.958 |
| Mean amplitudes (0 to 10 s) | 69.77 ± 15.51 | 63.00 ± 17.34 | 1.213 | 0.239 |
| Mean amplitudes (%MVC) | 70.5 (15.75) | 61 (26) | −1.350 | 0.177 |
| IPAQ (%) | 1.102 | 0.894 | ||
| Active | 40.00 | 35.71 | ||
| Irregularly active A | 10.00 | 21.43 | ||
| Irregularly active B | 16.66 | 14.29 | ||
| Very active | 26.66 | 21.43 | ||
| Sedentary | 6.66 | 7.14 | ||
| SQ-F | 74 (22) | 50 (43) | −1.640 | 0.101 |
| Collinearity Statistics | |||||
|---|---|---|---|---|---|
| Standardized Coefficients β | t | p-Value | Tolerance | VIF | |
| sEMG | |||||
| Peak (%MCV) | 0.338 | 1.582 | 0.123 | 0.399 | 2.503 |
| Mean amplitudes (0 to 10 s) | −0.566 | −2.220 | 0.033 * | 0.281 | 3.555 |
| Mean amplitudes (%MVC) | −0.068 | −0.330 | 0.743 | 0.424 | 2.359 |
| MVC (µv) | 0.516 | 2.105 | 0.043 * | 0.304 | 3.286 |
| Power/Pressure | 0.190 | 1.179 | 0.246 | 0.704 | 1.420 |
| SQ-F | 0.319 | 2.037 | 0.049 * | 0.747 | 1.338 |
| Self-declared physical activity | −0.442 | −3.081 | 0.004 * | 0.886 | 1.129 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Duarte, N.d.S.; Bittencourt, K.C.; Soares, C.O.; Ferreira, C.R.G.; Soares, W.M.; Tavares, V.B.; da Silva, A.S.A.; da Costa Priante, C.H.; das Neves, P.F.M.; da Silva Souza, G.; et al. Sexual Function, Physical Activity, Mean Amplitudes and Maximal Voluntary Contraction of Pelvic Floor Muscles Are Related to Handgrip Strength: A Cross-Sectional Study. Healthcare 2023, 11, 129. https://doi.org/10.3390/healthcare11010129
Duarte NdS, Bittencourt KC, Soares CO, Ferreira CRG, Soares WM, Tavares VB, da Silva ASA, da Costa Priante CH, das Neves PFM, da Silva Souza G, et al. Sexual Function, Physical Activity, Mean Amplitudes and Maximal Voluntary Contraction of Pelvic Floor Muscles Are Related to Handgrip Strength: A Cross-Sectional Study. Healthcare. 2023; 11(1):129. https://doi.org/10.3390/healthcare11010129
Chicago/Turabian StyleDuarte, Natália de Souza, Kayonne Campos Bittencourt, Cleuma Oliveira Soares, Clicia Raiane Galvão Ferreira, Wenderk Martins Soares, Victória Brioso Tavares, Amanda Suzane Alves da Silva, Caren Heloise da Costa Priante, Pablo Fabiano Moura das Neves, Givago da Silva Souza, and et al. 2023. "Sexual Function, Physical Activity, Mean Amplitudes and Maximal Voluntary Contraction of Pelvic Floor Muscles Are Related to Handgrip Strength: A Cross-Sectional Study" Healthcare 11, no. 1: 129. https://doi.org/10.3390/healthcare11010129
APA StyleDuarte, N. d. S., Bittencourt, K. C., Soares, C. O., Ferreira, C. R. G., Soares, W. M., Tavares, V. B., da Silva, A. S. A., da Costa Priante, C. H., das Neves, P. F. M., da Silva Souza, G., de Campos Gomes, F., Carneiro Nunes, E. F., Rodrigues, C. N. C., & de Melo Neto, J. S. (2023). Sexual Function, Physical Activity, Mean Amplitudes and Maximal Voluntary Contraction of Pelvic Floor Muscles Are Related to Handgrip Strength: A Cross-Sectional Study. Healthcare, 11(1), 129. https://doi.org/10.3390/healthcare11010129