
Narratives on the Current Medical Situation in Japan According to Highly Specialized Foreign Professionals


Abstract
:1. Introduction
2. Participants and Methods
2.1. Participants
2.2. Methods
- Verbatim transcripts were divided into text segments by semantic content in NVivo by TM, and each segment with content relevant to the study was assigned a descriptive code.
- Following completion of all interviews, all researchers reviewed the content, selected the next potential participant, reviewed the interview guide and questions, and revised the content as needed.
- The derived codes were then repeatedly compared and grouped according to semantic content to extract each theme and subtheme (Table 2). From this point on, all researchers discussed and analyzed the data.
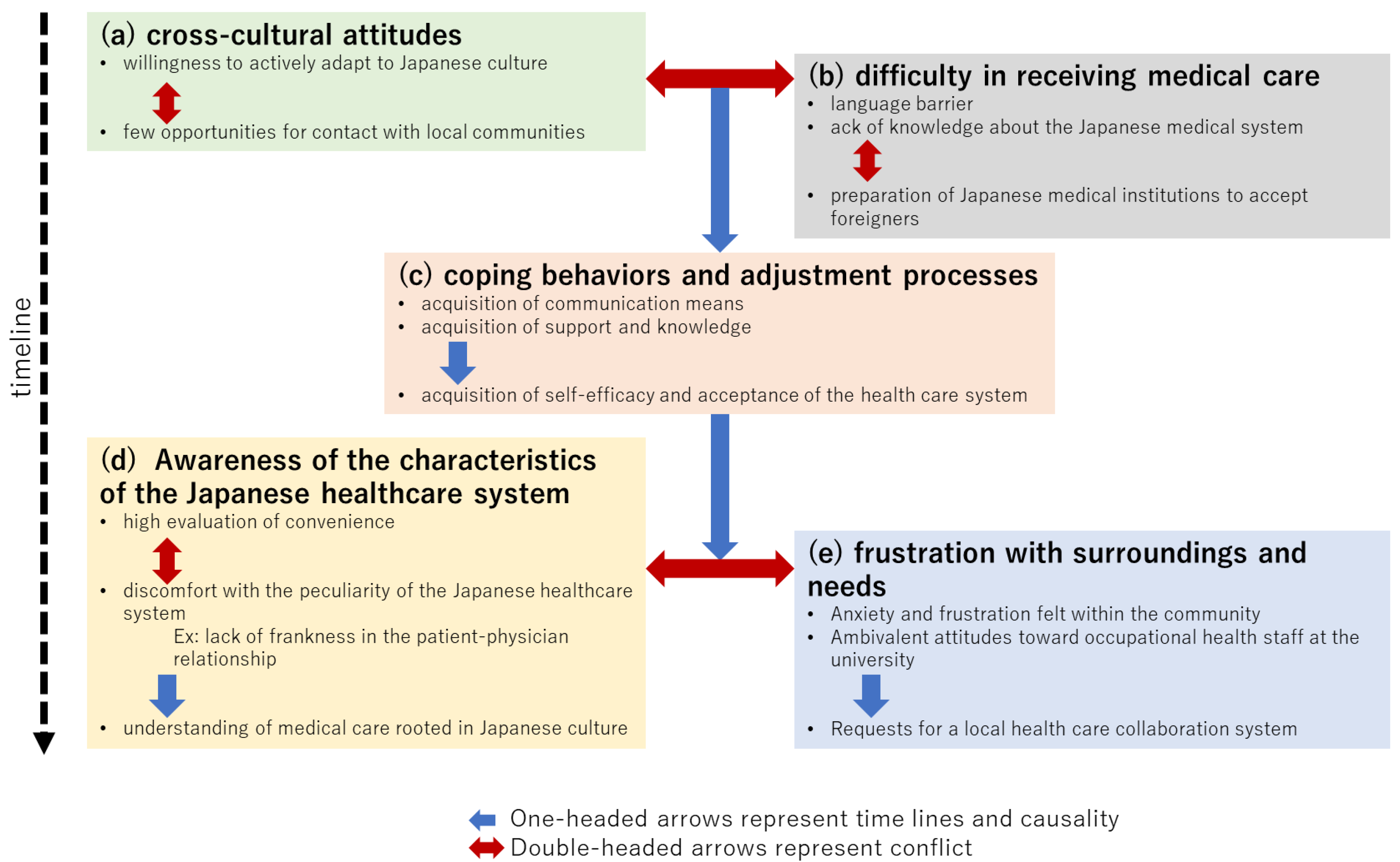
- By examining the contextual meaning of each code and examples of statements, a diagram of the relationship between categories and subcategories (causal and oppositional) was created (Figure 1).
- Based on the above analysis, we reconstructed the participant comments as a story.
- Since we were particularly interested in the gains and losses of language support methods, we separately extracted the relevant text segments and organized what was said about their characteristics and advantages and disadvantages (Table 3).
- 500 m: Clinic (interpreter software available for foreigners to use)
- 3.5 km: Clinic (for Japanese, but not restricted to foreigners)
- 6.5 km: Clinics of Psychiatry, Internal Medicine, and Otolaryngology
- 18 km: General hospital (2.5 tier)
- 17 km: General hospital (tertiary)
- 25 km: General hospital (certified as Japan Medical Service Accreditation for International Patients)
- 17.7 km: Radiotherapy and medical checkup clinic (outsourced medical examinations and acceptance of foreign nationals are also advocated)
3. Results
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ministry of Health, Labour and Welfare. FY2021 Survey of Medical Institutions Receiving Foreign Patients. Available online: https://www.mhlw.go.jp/stf/seisakunitsuite/bunya/0000202918_00022.html (accessed on 24 July 2022).
- Japan Association for the Promotion of Medical Education. Accreditation System for Medical Institutions Accepting Foreigners. Available online: http://jmip.jme.or.jp/ (accessed on 24 July 2022).
- International Society of Clinical Medicine. Available online: http://kokusairinshouigaku.jp/ (accessed on 24 July 2022).
- Jun, S.; Ball, A.D.; Gentry, J.W. Modes of consumer acculturation. ACR N. Am. Adv. 1993, 20, 76–82. [Google Scholar]
- Neto, F. Acculturation strategies among adolescents from immigrant families in Portugal. Int. J. Intercult. Relat. 2002, 26, 17–38. [Google Scholar] [CrossRef]
- Bierwiaczonek, K.; Waldzus, S. Socio-Cultural Factors as Antecedents of Cross-Cultural Adaptation in Expatriates, International Students, and Migrants: A Review. J. Cross-Cult. Psychol. 2016, 47, 767–817. [Google Scholar] [CrossRef]
- Frankenberg, E.; Kupper, K.; Wagner, R.; Bongard, S. Immigrant youth in Germany: Psychological and sociocultural adaptation. Eur. Psychol. 2013, 18, 158–168. [Google Scholar] [CrossRef]
- Ward, C.; Geeraert, N. Advancing acculturation theory and research: The acculturation process in its ecological context. Curr. Opin. Psychol. 2016, 8, 98–104. [Google Scholar] [CrossRef]
- Narayanasamy, A. Transcultural nursing: How do nurses respond to cultural needs? Br. J. Nurs. 2003, 12, 185–194. [Google Scholar] [CrossRef]
- Leishman, J. Perspectives of cultural competence in health care. Nurs. Stand. 2004, 19, 33–38. [Google Scholar] [CrossRef]
- Shepherd, S.M.; Willis-Esqueda, C.; Newton, D.; Sivasubramaniam, D.; Paradies, Y. The challenge of cultural competence in the workplace: Perspectives of healthcare providers. BMC Health Serv. Res. 2019, 19, 135. [Google Scholar] [CrossRef]
- Ikhilor, P.O.; Hasenberg, G.; Kurth, E.; Asefaw, F.; Pehlke-Milde, J.; Cignacco, E. Communication barriers in maternity care of allophone migrants: Experiences of women, healthcare professionals, and intercultural interpreters. J. Adv. Nurs. 2019, 75, 2200–2210. [Google Scholar] [CrossRef]
- Carrera, L.C.; Lévesque-Daniel, S.; Radjack, R.; Moro, M.R.; Lachal, J. Clinical Approaches to Cultural Diversity in Mental Health Care and Specificities of French Transcultural Consultations: A Scoping Review. Front. Psychiatry 2020, 11, 579147. [Google Scholar] [CrossRef]
- Pocock, N.S.; Chan, Z.; Loganathan, T.; Suphanchaimat, R.; Kosiyaporn, H.; Allotey, P.; Chan, W.K.; Tan, D. Moving towards culturally competent health systems for migrants? Applying systems thinking in a qualitative study in Malaysia and Thailand. PLoS ONE 2020, 15, e0231154. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alkhaled, R.; Rohde, G.; Lie, B.; Johannessen, B. Navigating the care between two distinct cultures: A qualitative study of the experiences of Arabic-speaking immigrants in Norwegian hospitals. BMC Health Serv. Res. 2022, 22, 400. [Google Scholar] [CrossRef] [PubMed]
- Nonaka, C.; Higuchi, M. The process of relationship building between foreign patients and nurses in Japan. Int. J. Health 2010, 25, 21–32. [Google Scholar]
- Kuwano, N.; Fukuda, H.; Murashima, S. Factors Affecting the Professional Autonomy of Japanese Nurses Caring for Culturally and Linguistically Diverse Patients in Japanese Hospitals. J. Transcult. Nurs. 2016, 27, 567–573. [Google Scholar] [CrossRef]
- Teraoka, M.; Muranaka, Y. Aspects of cross-cultural experiences in Japanese healthcare as perceived by foreigners living in Japan. J. Jpn. Acad. Nurs. Sci. 2017, 37, 35–44. [Google Scholar] [CrossRef]
- Ministry of Health, Labour and Welfare. Report on the Project for Promotion of Utilization of Highly Skilled Foreign Human Resources in Enterprises. Available online: https://www.mhlw.go.jp/bunya/koyou/oshirase/110301.html (accessed on 24 July 2022).
- Policy Assessment on the Acceptance of Highly Skilled Foreign Human Resources. Available online: https://www.soumu.go.jp/menu_news/s-news/hyouka_r010625_02.html (accessed on 24 July 2022).
- Okinawa Institute of Science and Technology Graduate University (OIST). Available online: https://www.oist.jp/ (accessed on 24 July 2022).
- Okinawa Institute of Science and Technology Graduate University. OIST Facts and Figures. Available online: https://www.oist.jp/facts-figures (accessed on 24 July 2022).
- Clarke, V.; Braun, V. Teaching Thematic Analysis. Overcoming challenges and developing strategies for effective learning. Psychologist 2013, 26, 120–123. [Google Scholar]
- Sanjari, M.; Bahramnezhad, F.; Fomani, F.K.; Shoghi, M.; Cheraghi, M.A. Ethical challenges of researchers in qualitative studies: The necessity to develop a specific guideline. J. Med. Ethics Hist. Med. 2014, 7, 14. [Google Scholar]
- Anderson, C.; Kirkpatrick, S. Narrative interviewing. Int. J. Clin. Pharm. 2016, 38, 631–634. [Google Scholar] [CrossRef]
- Durkin, J.; Jackson, D.; Usher, K. Qualitative research interviewing: Reflections on power, silence and assumptions. Nurse Res. 2020, 28, 31–35. [Google Scholar] [CrossRef]
- Mills, J.; Bonner, A.; Francis, K. Adopting a constructivist approach to grounded theory: Implications for research design. Int. J. Nurs. Pract. 2006, 12, 8–13. [Google Scholar] [CrossRef]
- Hardy, S.; Gregory, S.; Ramjeet, J. An exploration of intent for narrative methods of inquiry. Nurse Res. 2009, 16, 7–19. [Google Scholar] [CrossRef]
- Burleson, B.R. A Constructivist Approach to Listening. Int. J. Listening 2011, 25, 27–46. [Google Scholar] [CrossRef]
- Råheim, M.; Magnussen, L.H.; Sekse, R.J.T.; Lunde, Å.; Jacobsen, T.; Blystad, A. Researcher-researched relationship in qualitative research: Shifts in positions and researcher vulnerability. Int. J. Qual. Stud. Health Well-Being 2016, 11, 30996. [Google Scholar] [CrossRef]
- Berry, L.E. The research relationship in narrative enquiry. Nurse Res. 2016, 24, 10–14. [Google Scholar] [CrossRef]
- Zanchetta, M.S.; Poureslami, I.M. Health literacy in immigrant cultural and language realities. Can. J. Public Health 2006, 97 (Suppl. S2), s26–s30. [Google Scholar]
- Kostareva, U.; Albright, C.L.; Berens, E.M.; Polansky, P.; Kadish, D.E.; Ivanov, L.L.; Sentell, T.L. A multilingual integrative review of health literacy among migrants from the former Soviet Union and Russian-speaking countries. Int. J. Environ. Res. Public Health 2021, 18, 657. [Google Scholar] [CrossRef]
- Ministry of Health, Labour and Welfare. FY2021 Project to Support the Deployment of Medical Interpreters and Medical Coordinators for the Reception of Foreign Patients. Available online: https://www.mhlw.go.jp/stf/seisakunitsuite/bunya/0000202926_00003.html (accessed on 24 July 2022).

{kind=link}
| Participant No. | 1 | 2 | 3 | 4 | 5 | 6 | 7 |
| Age group (years) | 40–50 | 30–40 | 40–50 | 20–30 | 30–40 | 30–40 | 40–50 |
| Sex | Male | Male | Male | Male | Male | Female | Female |
| Occupation/Educational status | Faculty /Staff | Faculty /Staff | Faculty /Staff | Student, Herein-period government administration | Student, Herein-period government administration | Faculty /Staff | Faculty /Staff |
| Geographical area of origin | South Asia | Europe | South Africa * 1 | North America * 1 | Europe | North America * 1 | North America * 1 |
| Number of years since coming to Japan (years) | 20–25 | 5–10 | 5–10 | <5 | <1 | <5 | <5 |
| Japanese language proficiency | Fluent (language skill) | Ordinary (daily life) conversation | Ordinary (daily life) conversation | Ordinary (daily life) conversation | Greeting phrase only | Fluent (language skill) | Greeting phrase only |
| Number of codes created | 26 | 33 | 26 | 34 | 24 | 25 | 53 |
| Participant No. | 8 | 9 | 10 | 11 | 12 | 13 | |
| Age group (years) | 30–40 | 30–40 | 30–40 | 40–50 | 50–60 | 30–40 | |
| Sex | Female | Female | Female | Female | Male | Female | |
| Occupation/Educational status | Student, Herein-period government administration | Faculty /Staff | Student, Herein-period government administration | Faculty /Staff | Faculty /Staff | Faculty /Staff | |
| Geographical area of origin | Europe | North America * 1 | Near/Middle East | East Asia | Europe | North America * 1 | |
| Number of years since coming to Japan (years) | <5 | 5–10 | 5–10 | 5–10 | 5–10 | 5–10 | |
| Japanese language proficiency | Greeting phrase only | Ordinary (daily life) conversation | Ordinary (daily life) conversation | Ordinary (daily life) conversation | Ordinary (daily life) conversation | Ordinary (daily life) conversation | |
| Number of codes created | 32 | 29 | 38 | 23 | 57 | 34 |
|
| Theme | Subtheme | Code |
|---|---|---|
| Cultural adaptation | Willingness to adapt actively to Japanese culture | Abundant overseas experience as a high-level foreign human resource, and an international sense that enables them to relativize their own culture |
| Cultural criticism | ||
| Japanese character | ||
| Willingness to learn Japanese | ||
| Familiarity with the Japanese people and Japanese culture | ||
| Unexpected difficulties of living in a real Japanese language environment | ||
| Little contact with the community | Generous support from the university in terms of daily life | |
| Difficulties experienced in order to see a doctor | Language barrier | In medical institutions where patients are expected to speak Japanese and staff other than doctors do not speak English, so foreigners are at a loss at the hospital reception desk in the first place |
| Filling out medical forms written only in Japanese is difficult, and there is little multilingual support | ||
| It is unrealistic to expect foreigners to acquire a level of Japanese that will allow them to explain and understand healthcare | ||
| Especially for foreigners, it is difficult to communicate with medical personnel in case of sudden or serious illness | ||
| Differences in perception between foreigners who believe that the responsibility for language support lies with the medical institution and Japanese medical institutions that do not provide language support | ||
| Lack of knowledge about the Japanese healthcare system | In Japan, medical departments are subdivided, and medical institutions range from large hospitals to small clinics, making it difficult to know which medical institution to go to first | |
| Difficulties understanding the flow and payment procedures at general hospitals, from reception to payment and prescriptions | ||
| Readiness to accept | Experiences being told by psychiatrists and obstetricians that they cannot be treated because they are foreigners | |
| Experiences being required by medical institutions to bring their own interpreter in the event of a sudden illness or serious situation | ||
| Coping behaviors and adaptive processes | Individual participants’ narrative which is awkward especially on information | Family members and acquaintances are expected to accompany the patients to the hospital and assist them, allowing them to survive the emergency |
| The costs, risks, and benefits of hiring a professional or volunteer interpreter | ||
| Lack of English-language websites and distrust due to likely outdated content | ||
| While ICT equipment is inexpensive and easy to use, its applications are limited due to its low accuracy | ||
| Recognize the practical effectiveness of trying to communicate openly in both Japanese and English, even if imperfectly | ||
| Support and knowledge | Learn how to obtain healthcare from familiar sources, e.g., gather information from acquaintances, colleagues, and university health centers | |
| Experience the convenience of seeing a doctor at a medical institution with full-time interpreters and other language support | ||
| Familiarize oneself with the procedures and learn how to go to the hospital alone at non-emergent times | ||
| Achievement of self-efficacy and satisfaction with the healthcare system | By giving up or compromising, they feel a sense of security that they can manage to solve the problem and come to terms with the healthcare provided | |
| Perceptions of the characteristics of the Japanese healthcare system | High ratings for convenience | Positive evaluation of inexpensive and uniform medical costs |
| Favorable evaluation of easy access to advanced medical equipment such as CTs and MRIs, as well as access to medical specialists | ||
| Confidence that Japanese healthcare meets a certain standard regardless of the medical institution | ||
| Positive evaluation of not feeling discrimination against foreigners by healthcare workers | ||
| Discomfort with the peculiarities of the Japanese healthcare system | Discomfort with the Japanese healthcare system and feeling that it is inconvenient relative to that in one’s own country of origin | |
| Complexity of paperwork, bureaucratic inflexibility regarding procedures | ||
| Direct and open relationships | Difficulty in establishing a direct and open relationship between patients and physicians because of the still-prevalent stereotype of paternalism wherein physicians explain and patients follow their instructions without questioning | |
| Foreigners’ understanding of healthcare | An understanding and acceptance of the advantages, disadvantages, and inconveniences of Japanese medicine as a characteristic of Japanese culture | |
| Frustration | Anxiety and frustration felt in the community | The loneliness of living in a foreign land, far from home and family |
| Loneliness of not having someone close by to share the experience of illness or to talk to | ||
| Stigma due to fear of invasion of privacy and lack of understanding of surroundings | ||
| Ambivalent attitudes toward occupational health staff at universities | Trust in occupational health staff as a source of information about the Japanese healthcare system and distrust of workplaces that force employees to undergo health checkups and keep track of health information | |
| Requests for a regional medical cooperation system | The need for reliable primary care physicians who can address everyday problems of foreign patients and serve as a base for medical coordination |
| Type of Support | Features and Advantages/Disadvantages |
|---|---|
| Human interpreter | The individual skills of medical interpreters vary, they are difficult to secure at the last minute, they are expensive, they help with various hospital procedures, and they should be readily available at least in public hospitals and larger hospitals. |
| Translation apps and online interpreters | Translation apps are inexpensive (free) and easy to use, but lack accuracy and reliability and are limited to ancillary use. Online medical interpreters are inexpensive, reliable, and do not require an appointment. Online interpretation services provided by local governments are not well known and are rarely used in hospitals. |
| Information about the website and multilingual documentation | The English versions of hospital and government websites are often inaccurate because their content is more limited or outdated relative to the Japanese version. Multilingual documents in bilingual (English and Japanese) are very useful but not always available. |
| Medical professionals with foreign language skills | In psychiatric care, direct and accurate communication is critical. When choosing a medical institution, care options are often dependent on whether or not the doctor speaks English, and not by the doctor’s medical skills. There is a serious shortage of English-speaking physicians. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mori, T.; Deasy, Y.; Kanemoto, E.; Nakazawa, E.; Akabayashi, A. Narratives on the Current Medical Situation in Japan According to Highly Specialized Foreign Professionals. Healthcare 2022, 10, 1694. https://doi.org/10.3390/healthcare10091694
Mori T, Deasy Y, Kanemoto E, Nakazawa E, Akabayashi A. Narratives on the Current Medical Situation in Japan According to Highly Specialized Foreign Professionals. Healthcare. 2022; 10(9):1694. https://doi.org/10.3390/healthcare10091694
Chicago/Turabian StyleMori, Tomoari, Yoko Deasy, Eri Kanemoto, Eisuke Nakazawa, and Akira Akabayashi. 2022. "Narratives on the Current Medical Situation in Japan According to Highly Specialized Foreign Professionals" Healthcare 10, no. 9: 1694. https://doi.org/10.3390/healthcare10091694
APA StyleMori, T., Deasy, Y., Kanemoto, E., Nakazawa, E., & Akabayashi, A. (2022). Narratives on the Current Medical Situation in Japan According to Highly Specialized Foreign Professionals. Healthcare, 10(9), 1694. https://doi.org/10.3390/healthcare10091694