
Decision Making in Addictive Behaviors Based on Prospect Theory: A Systematic Review
 ,
,  , , and
, , and
Abstract
1. Introduction
The Current Study
2. Materials and Methods
2.1. Search Strategy and Information Sources
2.2. Eligibility Criteria and Selection Process
2.3. Ethical Considerations
2.4. Data Collection Process
3. Results
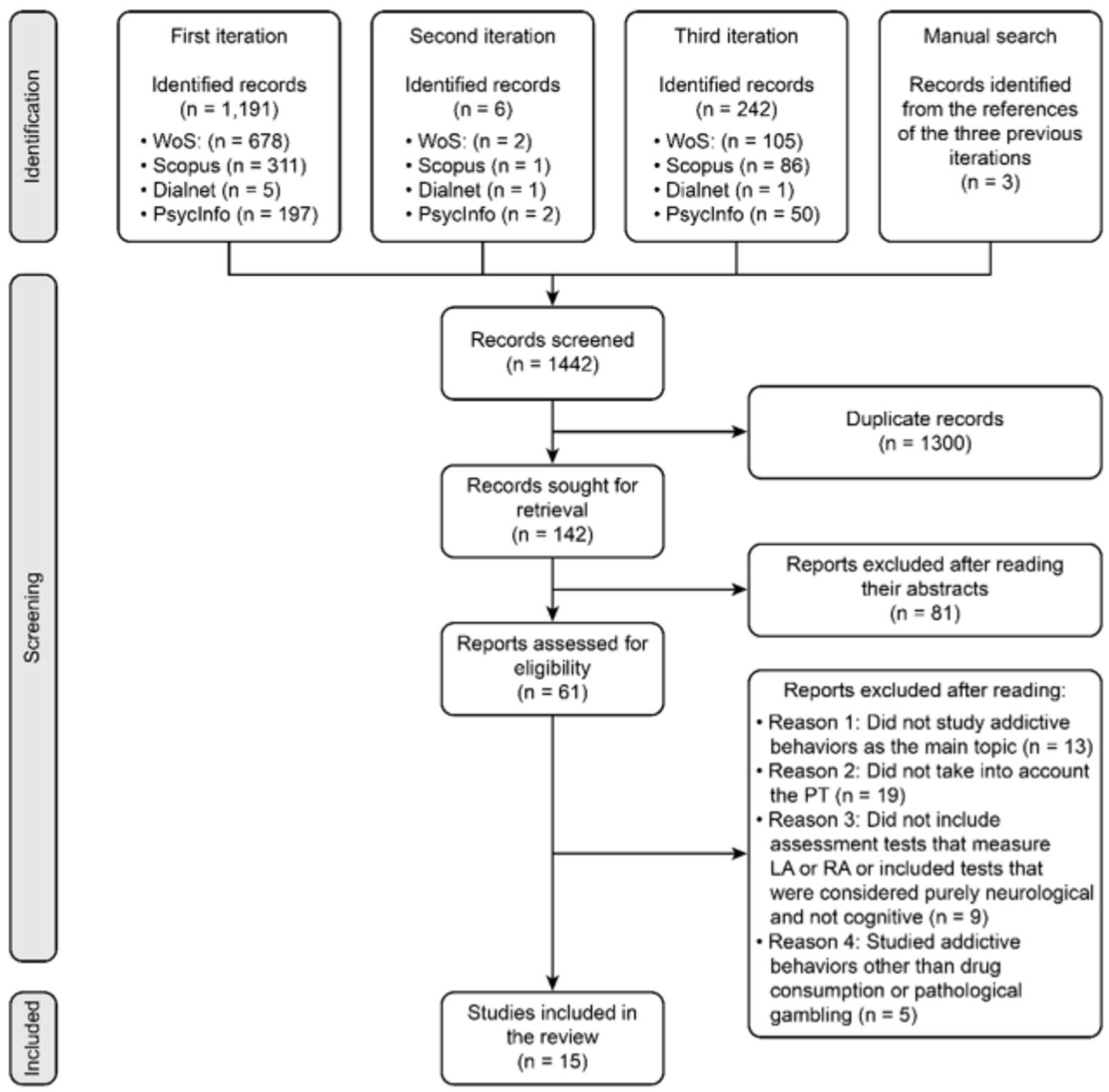
3.1. Study Selection and Study Characteristics
3.2. Results of Syntheses
4. Discussion
4.1. Future Research
4.2. Limitations
4.3. Practical Implications
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| PT | Prospect theory |
| LA | Loss aversion |
| RA | Risk aversion |
| PRISMA | Preferred reported items for systematic reviews and meta-analyses |
| PROSPERO | International prospective register of systematic reviews |
| WoS | Web of science |
| EMCDDA | European monitoring center for drugs and drug addiction |
| EDADES | Encuesta sobre alcohol y otras drogas en España |
| ESTUDES | Encuesta sobre uso de drogas en enseñanzas secundarias en España |
References
- Coates, J.M.; Gullo, M.J.; Feeney, G.F.X.; Young, R.M.; Dingle, G.A.; Clark, P.J.; Connor, J.P. Craving mediates the effect of impulsivity on lapse-risk during alcohol use disorder treatment. Addict. Behav. 2020, 105, 106286. [Google Scholar] [CrossRef] [PubMed]
- Kale, D.; Pickering, A.; Cooper, A. Examining the relationship between impulsivity-related personality traits and e-cigarette use in adults. Addict. Behav. 2020, 106, 106348. [Google Scholar] [CrossRef] [PubMed]
- Meikle, S.; Carter, O.; Bedi, G. Individual differences in distress, impulsivity, and coping motives for use as predictors of problematic ecstasy use. Addict. Behav. 2020, 108, 106397. [Google Scholar] [CrossRef] [PubMed]
- Verdejo-García, A.; Lawrence, A.J.; Clark, L. Impulsivity as a vulnerability marker for substance-use disorders: Review of findings from high-risk research, problem gamblers and genetic association studies. Neurosci. Biobehav. Rev. 2008, 32, 777–810. [Google Scholar] [CrossRef]
- Martino, F.; Caselli, G.; Felicetti, F.; Rampioni, M.; Romanelli, P.; Troiani, L.; Sassaroli, S.; Albery, I.P.; Spada, M.M. Desire thinking as a predictor of craving and binge drinking: A longitudinal study. Addict. Behav. 2017, 64, 118–122. [Google Scholar] [CrossRef]
- Martino, F.; Caselli, G.; Fiabane, E.; Felicetti, F.; Trevisani, C.; Menchetti, M.; Mezzaluna, C.; Sassaroli, S.; Albery, I.P.; Spada, M.M. Desire thinking as a predictor of drinking status following treatment for alcohol use disorder: A prospective study. Addict. Behav. 2019, 95, 70–76. [Google Scholar] [CrossRef]
- Fernández-Serrano, M.J.; Perales, J.C.; Moreno-López, L.; Pérez-García, M.; Verdejo-García, A. Neuropsychological profiling of impulsivity and compulsivity in cocaine dependent individuals. Psychopharmacology 2012, 219, 673–683. [Google Scholar] [CrossRef]
- Moreno-López, L.; Catena, A.; Fernández-Serrano, M.J.; Delgado-Rico, E.; Stamatakis, E.A.; Pérez-García, M.; Verdejo-García, A. Trait impulsivity and prefrontal gray matter reductions in cocaine dependent individuals. Drug Alcohol Depend. 2012, 125, 208–214. [Google Scholar] [CrossRef]
- Fernández-Serrano, M.J.; Perales, J.C.; Moreno-López, L.; Santos-Ruiz, A.; Pérez-García, M.; Verdejo-García, A. Impulsivity and Compulsivity in Cocaine Dependent Individuals. Adicciones 2012, 24, 105–113. Available online: https://www.proquest.com/scholarly-journals/impulsivity-compulsivity-cocaine-dependent/docview/1609097399/se-2 (accessed on 10 July 2022). [CrossRef]
- Contreras-Rodríguez, O.; Albein-Urios, N.; Vilar-López, R.; Perales, J.C.; Martínez-Gonzáles, J.M.; Fernández-Serrano, M.J.; Lozano-Rojas, O.; Clark, L.; Verdejo-García, A. Increased coticolimbic connectivity in cocaine dependence versus pathological gambling is associated with drug severity and emotion-related impulsivity. Addict. Biol. 2016, 21, 709–718. [Google Scholar] [CrossRef]
- Volkow, N.D.; Fowler, J.S.; Wang, G.J.; Swanson, J.M. Dopamine in drug abuse and addiction: Results from imaging studies and treatment implications. Mol. Psychiatry 2004, 9, 557–569. [Google Scholar] [CrossRef] [PubMed]
- Volkow, N.D.; Wise, R.A.; Baler, R. The dopamine motive system: Implications for drug and food addiction. Nat. Rev. Neurosci. 2017, 18, 741–752. [Google Scholar] [CrossRef] [PubMed]
- Wiers, C.E.; Cunningham, S.I.; Tomasi, D.G.; Ernst, T.; Chang, L.; Shokri-Kojori, E.; Wang, G.-J.; Volkow, N.D. Elevated thalamic glutamate levels and reduced water diffusivity in alcohol use disorder. Association with impulsivity. Psychiatry Res. Neuroimagin 2020, 305, 111185. [Google Scholar] [CrossRef]
- Hall, W.; Carter, A.; Forlini, C. Brain disease model of addiction: Misplaced priorities? Lancet Psychiatry 2015, 2, 867. [Google Scholar] [CrossRef]
- Carmona-Perera, M.; Verdejo-García, A.; Young, L.; Molina-Fernández, A.; Pérez-García, M. Moral decision-making in polysubstance dependent individuals. Drug Alcohol Depend. 2012, 126, 389–392. [Google Scholar] [CrossRef]
- Carmona-Perera, M.; Clark, L.; Young, L.; Pérez-García, M.; Verdejo-García, A. Impaired decoding of fear and disgust predicts utilitarian moral judgement in alcohol-dependent individuals. Alcohol. Clin. Exp. Res. 2014, 38, 179–185. [Google Scholar] [CrossRef][Green Version]
- Kahneman, D.; Tversky, A. Prospect theory: An analysis of decision under risk. Econometrica 1979, 47, 263–291. [Google Scholar] [CrossRef]
- Kahneman, D. Thinking, Fast and Slow; Macmillan: New York, NY, USA, 2011. [Google Scholar]
- Meyerowitz, B.E.; Chaiken, S. The effect of message framing on breast self-examination attitudes, intentions, and behavior. J. Pers. Soc. Psychol. 1987, 52, 500–510. [Google Scholar] [CrossRef]
- Prochaska, J.O.; DiClemente, C.C. Transtheoretical therapy: Toward a more integrative model of change. Psychother. Theory Res. Pract. 1982, 19, 276–288. [Google Scholar] [CrossRef]
- Curry, S.; Marlatt, G.A.; Gordon, J.R. Abstinence violation effect: Validation of an attributional construct with smoking cessation. J. Consult. Clin. Psychol. 1987, 55, 145–149. [Google Scholar] [CrossRef]
- Becker, G.S.; Murphy, K.M. A theory of rational addiction. J. Polit. Econ. 1988, 96, 675–700. [Google Scholar] [CrossRef]
- Tversky, A.; Kahneman, D. The framing of decisions and the psychology of choice. Science 1981, 211, 453–458. [Google Scholar] [CrossRef] [PubMed]
- Bickel, W.K.; Marsch, L.A. Toward a behavioral economic understanding of drug dependence: Delay discounting processes. Addiction 2001, 96, 73–86. [Google Scholar] [CrossRef] [PubMed]
- Goodie, A.S.; Fortune, E.E. Measuring cognitive distortions in pathological gambling: Review and meta-analyses. Psychol. Addict. Behav. 2013, 27, 730–743. [Google Scholar] [CrossRef]
- d’Astous, A.; Di Gaspero, M. Heuristic and analytic processing in online sports betting. J. Gambl. Stud. 2015, 31, 455–470. [Google Scholar] [CrossRef]
- Genauck, A.; Andrejevic, M.; Brehm, K.; Matthis, C.; Heinz, A.; Weinreich, A.; Kathmann, N.; Romanczuk-Seiferth, N. Cue-induced effects on decision-making distinguish subjects with gambling disorder from healthy controls. Addict. Biol. 2020, 25, e12841. [Google Scholar] [CrossRef] [PubMed]
- Kluwe-Schiavon, B.; Kexel, A.; Manenti, G.; Cole, D.M.; Baumgartner, M.R.; Grassi-Oliveira, R.; Tobler, P.N.; Quednow, B.B. Sensitivity to gains during risky decision-making differentiates chronic cocaine users from stimulant-naïve controls. Behav. Brain Res. 2020, 379, 112386. [Google Scholar] [CrossRef]
- Kräplin, A.; Höfler, M.; Pooseh, S.; Wolff, M.; Krönke, K.-M.; Goschke, T.; Bühringer, G.; Smolka, M.N. Impulsive decision-making predicts the course of substance-related and addictive disorders. Psychopharmacology 2020, 237, 2709–2724. [Google Scholar] [CrossRef]
- Thaikill, E.A.; DeSarno, M.; Higgins, S.T. Loss aversion and risk for cigarette smoking and other substance use. Drug Alcohol Depend. 2022, 232, 109307. [Google Scholar] [CrossRef]
- Canessa, N.; Basso, G.; Poggi, P.; Gianelli, C. Altered striatal-opercular intrinsic connectivity reflects decreased aversion to losses in alcohol use disorder. Neuropsychologia. 2022, 172, 108258. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- Urrútia, G.; Bonfill, X. Declaración PRISMA: Una propuesta para mejorar la publicación de revisiones sistemáticas y metaanálisis. Med. Clín. 2010, 135, 507–511. [Google Scholar] [CrossRef] [PubMed]
- Tversky, A.; Kahneman, D. Advances in prospect theory: Cumulative representation of uncertainty. J. Risk Uncertain. 1992, 5, 297–323. [Google Scholar] [CrossRef]
- de Psicología, S.M. Ethical Code of the Psychologist. In Código Ético del Psicólogo; Trillas: Mexico City, Mexico, 2010. [Google Scholar]
- American Psychiatric Association. Ethical Principles of Psychologists and Code of Conduct. With the 2016 Amendment to Standard 3.04; American Psychological Association Press: Washington, DC, USA, 2017. [Google Scholar]
- World Medical Association. World medical association declaration of helsinki. JAMA 2013, 310, 2191–2194. [Google Scholar] [CrossRef] [PubMed]
- Blondel, S.; Lohéac, Y.; Rinaudo, S. Rationality and drug use: An experimental approach. J. Health Econ. 2007, 26, 643–658. [Google Scholar] [CrossRef]
- Ida, T.; Goto, R.; Takahashi, Y.; Nishimura, S. Can economic-psychological parameters predict successful smoking cessation? J. Soc.-Econ. 2011, 40, 285–295. [Google Scholar] [CrossRef]
- Ligneul, R.; Sescousse, G.; Barbalat, G.; Domenech, P.; Dreher, J.C. Shifted risk preferences in pathological gambling. Psychol. Med. 2013, 43, 1059–1068. [Google Scholar] [CrossRef]
- Romanowich, P.; Lamb, R.J. The effect of framing incentives as either losses or gains with contingency management for smoking cessation. Addict. Behav. 2013, 38, 2084–2088. [Google Scholar] [CrossRef]
- Ahn, W.-Y.; Vasilev, G.; Lee, S.-H.; Busemeyer, J.R.; Kruschke, J.K.; Bechara, A.; Vassileva, J. Decision-making in stimulant and opiate addicts in protracted abstinence: Evidence from computational modeling with pure users. Front. Psychol. 2014, 5, 849. [Google Scholar] [CrossRef]
- Giorgetta, C.; Grecucci, A.; Rattin, A.; Guerreschi, C.; Sanfey, A.G.; Bonini, N. To play or not to play: A personal dilemma in pathological gambling. Psychiatry Res. 2014, 219, 562–569. [Google Scholar] [CrossRef]
- Lorains, F.K.; Dowling, N.A.; Enticott, P.G.; Bradshaw, J.L.; Trueblood, J.S.; Stout, J.C. Strategic and non-strategic problem gamblers differ on decision-making under risk and ambiguity. Addiction 2014, 109, 1128–1137. [Google Scholar] [CrossRef] [PubMed]
- Takeuchi, H.; Kawada, R.; Tsurumi, K.; Yokoyama, N.; Takemura, A.; Murao, T.; Murai, T.; Takahashi, H. Heterogeneity of loss aversion in pathological gambling. J. Gambl. Stud. 2016, 32, 1143–1154. [Google Scholar] [CrossRef]
- Gelskov, S.V.; Madsen, K.H.; Ramsøy, T.Z.; Siebner, H.R. Aberrant neural signatures of decision-making: Pathological gamblers display cortico-striatal hypersensitivity to extreme gambles. NeuroImage 2016, 128, 342–352. [Google Scholar] [CrossRef] [PubMed]
- Strickland, J.C.; Beckmann, J.S.; Rush, C.R.; Stoops, W.W. A pilot study of loss aversion for drug and non-drug commodities in cocaine users. Drug Alcohol Depend. 2017, 180, 223–226. [Google Scholar] [CrossRef] [PubMed]
- Bernhardt, N.; Nebe, S.; Pooseh, S.; Sebold, M.; Sommer, C.; Birkenstock, J.; Zimmermann, U.S.; Heinz, A.; Smolka, M.N. Impulsive decision making in young adult social drinkers and detoxified alcohol-dependent patients: A cross-sectional and longitudinal study. Alcohol. Clin. Exp. Res. 2017, 41, 1794–1807. [Google Scholar] [CrossRef] [PubMed]
- Genauck, A.; Quester, S.; Wüstenberg, T.; Mörsen, C.; Heinz, A.; Romanczuk-Seiferth, N. Reduced loss aversion in pathological gambling and alcohol dependence is associated with differential alterations in amygdala and prefrontal functioning. Sci. Rep. 2017, 7, 16306. [Google Scholar] [CrossRef] [PubMed]
- Meade, C.S.; Addicott, M.; Hobkirk, A.L.; Towe, S.L.; Chen, N.-K.; Sridharan, S.; Huettel, S.A. Cocaine and HIV are independently associated with neural activation in response to gain and loss valuation during economic risky choice. Addict. Biol. 2018, 23, 796–809. [Google Scholar] [CrossRef]
- Ring, P.; Probst, C.C.; Neyse, L.; Wolff, S.; Kaernbach, C.; van Eimeren, T.; Camerer, C.F.; Schmidt, U. It’s all about gains: Risk preferences in problem gambling. J. Exp. Psychol. Gen. 2018, 147, 1241–1255. [Google Scholar] [CrossRef]
- Ojala, K.E.; Janssen, L.K.; Hashemi, M.M.; Timmer, M.H.M.; Geurts, D.E.M.; Ter Huurne, N.P.; Cools, R.; Sescousse, G. Dopaminergic drug effects on probability weighting during risky decision making. eNeuro 2018, 5, ENEURO.0330-18. [Google Scholar] [CrossRef]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 4th ed.; American Psychiatric Association: Washington, DC, USA, 1994. [Google Scholar]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 4th ed. text rev.; American Psychiatric Association: Washington, DC, USA, 2000. [Google Scholar]
- Pellín, M.C.; Gimeno, C.; Esteban, J. Diferencias en los criterios diagnósticos DSM-IV y DSM-IV-TR de los trastornos relacionados con sustancias y comentarios sobre términos utilizados. Salud Drog. 2002, 2, 57–88. [Google Scholar] [CrossRef][Green Version]
- Jantarakolica, K.; Kaweewitayawong, H.; Jantarakolica, T. Factors determining decision on purchasing lottery: A case study in greater Bangkok. Procedia Soc. Behav. Sci. 2012, 40, 746–750. [Google Scholar] [CrossRef]
- Breslin, F.C.; Sobell, M.B.; Cappell, H.; Vakili, S.; Poulos, C.X. The effects of alcohol, gender, and sensation seeking on the gambling choices of social drinkers. Psychol. Addict. Behav. 1999, 13, 243–252. [Google Scholar] [CrossRef]
- European Monitoring Center for Drugs and Drug Addiction. Available online: https://www.emcdda.europa.eu/system/files/publications/14644/EDR_2022_18-ONLINE.pdf (accessed on 10 July 2022).
- Portal Nacional Sobre Drogas—Encuestas y Estudios. La Encuesta Sobre Alcohol y Otras Drogas en España, EDADES. Available online: https://pnsd.sanidad.gob.es/profesionales/sistemasInformacion/sistemaInformacion/encuestas_EDADES.htm (accessed on 6 April 2022).
- Portal Nacional Sobre Drogas—Encuestas y Estudios. La Encuesta Sobre Uso de Drogas en Enseñanzas Secundarias en España, ESTUDES. Available online: https://pnsd.sanidad.gob.es/profesionales/sistemasInformacion/sistemaInformacion/encuestas_ESTUDES.htm (accessed on 6 April 2022).
- del Castillo, J.A.G. Concepto de percepción de riesgo y su repercusión en las adicciones. Salud Drog. 2012, 12, 133–151. [Google Scholar] [CrossRef]
- Erku, D.A.; Bauld, L.; Dawkins, L.; Gartner, C.E.; Steadman, K.J.; Noar, S.M.; Shrestha, S.; Morphett, K. Does the content and source credibility of health and risk messages related to nicotine vaping products have an impact on harm perception and behavioural intentions? A systematic review. Addiction 2021, 116, 3290–3303. [Google Scholar] [CrossRef]
- Goh, M.C.W.; Kelly, P.J.; Deane, F.P.; Raftery, D.K.; Ingram, I. Communication of health risk in substance-dependent populations: A systematic review of randomised controlled trials. Drug Alcohol Rev. 2021, 40, 920–936. [Google Scholar] [CrossRef]
- National Institute of Drug Abuse. Available online: https://nida.nih.gov/publications/drugfacts/comorbidity-substance-use-disorders-other-mental-illnesses (accessed on 10 July 2022).
- Baron, R.; Byrne, D. Psicología Social; Prentice-Hall: Madrid, Spain, 2002. [Google Scholar]
- Miller, W.R.; Rollnick, S. La Entrevista Motivacional; Paidós: Barcelona, Spain, 1999. [Google Scholar]
- Lin, S.; Ma, Y.; Zou, H. A brief metric framework for patient adherence to doctor’s advice based on behavioral economics. Patient Prefer. Adherence 2020, 14, 371–381. [Google Scholar] [CrossRef] [PubMed]
- Chivers, L.L.; Higgins, S.T. Some observations from behavioral economics for consideration in promoting money management among those with substance use disorders. Am. J. Drug Alcohol Abuse 2012, 38, 8–19. [Google Scholar] [CrossRef][Green Version]
- Lejarraga, T.; Woike, J.K.; Hertwig, R. Description and experience: How experimental investors learn about booms and busts affects their financial risk taking. Cognition 2016, 157, 365–383. [Google Scholar] [CrossRef]
- Freeman, D.; Reeve, S.; Robinson, A.; Ehlers, A.; Clark, D.; Spanlang, B.; Slater, M. Virtual reality in the assessment, understanding, and treatment of mental health disorders. Psychol. Med. 2017, 47, 2393–2400. [Google Scholar] [CrossRef]
- Li, J.; Chai, L.; Nordstrom, O.; Tanpong, C.; Hung, K.T. Development of a Loss Aversion Scale. J. Manag. Issues 2021, 33, 69–89. Available online: https://www.researchgate.net/publication/351334891_Development_of_a_Loss_Aversion_Scale (accessed on 10 July 2022).
- Harrington, N.G.; Kerr, A.M. Rethinking risk: Prospect theory application in health message framing research. Health Commun. 2017, 32, 131–141. [Google Scholar] [CrossRef] [PubMed]
- Ma, Z.; Nan, X. Positive facts, negative stories: Message framing as a moderator of narrative persuasion in antismoking communication. Health Commun. 2019, 34, 1454–1460. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Authorship | Study Design | Objectives | Sample | Control Group | Methods | Results | Limitations |
|---|---|---|---|---|---|---|---|
| Blondel et al. (2007) [38] | Empirical research | To study decision-making under risk and with temporality in former heroin users. | N = 34. Age: = 35; SD = 5.8 Former heroin users, under the effects of methadone. 62.86% male. | Yes. (N = 23 nonusers. Only men. Age: = 37; SD = 10.4) | Blanqui game (7 items) and Stockholm game (14 items). | Consumers are less risk averse than nonconsumers. Both groups are similar in time. | The results cannot be generalized to other addictive behaviors since the study contemplates only one type (heroin use). |
| Ida et al. (2011) [39] | Empirical research | To analyze the relationship between risk aversion in a population trying to quit tobacco smoking. | N = 608. Successful smoking cessation: 321; 54,5% men; Age: = 35. Failure to quit smoking: 287; 58.2% men; Age: = 35.1. | No. | Associated analysis questionnaire, which offered alternatives to evaluate risk aversion, among other variables. | Successful quitters had lower loss aversion than unsuccessful quitters, both before and after 5 months of follow-up. There were no differences between the beginning and the end of the experiment within each group. | The cause of quitting smoking was not studied. The sample comprised people who managed to stop smoking for one week before joining the study. |
| Ligneul et al. (2013) [40] | Empirical research | To test the possible cognitive distortion of pathological gamblers in their perception of winning probabilities. | N = 18. Age: = 33,2; SD = 11.5 Men, pathological gamblers. | Yes. (N = 20 men, nongamblers. Age: = 31; SD = 7.3) | 3 questionnaires: Barratt Impulsiveness Scale version 11, 40-item Sensation Seeking Scale and Gambling Attitudes and Beliefs Survey. | Greater loss aversion in pathological gamblers. Higher scores in attentional and motor impulsivity and in disinhibition and adventurousness. | Their exposure to pathological gambling behavior itself may affect their decision making. The choice of the sample is questionable. The experiment needs to be extended to other addictive behaviors. |
| Romanowich and Lamb (2013) [41] | Empirical research | To test whether the cumulative prospective theory is applicable to tobacco addicts. To test whether losses work better than gains for learning a behavior. | N = 25. Group of losses: 4% women. Age: = 43; SD = 14. Group of gains: 5% women. Age: = 39; SD = 13 Tobacco smokers, not intending to quit smoking. | No. | Smokers are divided into two groups: 1: they will lose $75 if they have smoked the day before a visit (they start with $375). 2: they will gain $75 if they have not smoked the day before a visit (they start with $0). | Consistent with cumulative prospective theory, the loss group quit smoking faster, but the gain group maintained it better over time. | The CO2 test is assumed to be reliable. There are differences between salary and the average number of cigarettes consumed per day in some participants. |
| Ahn et al. (2014) [42] | Empirical research | To test possible differences in the decision-making processes of consumers and ex-consumers. | n = 38 amphetamine addicts and detoxified (76.3% men. Age: = 22.7; SD = 3.7). n= 43 “pure” heroin addicts and detoxified (81.4% male. Age = 29.7; SD = 5). No gender distinction indicated. | Yes. (N = 48 nonconsumers. 79.2% men. Age: = 24.7; SD = 4.9) | Iowa Gambling Task. Subsequently, their results were compared according to prospect valence learning with delta and decay learning rule and according to the value-plus-perseverance model. | Deficits in decision making were observed. Former heroin users had lower loss aversion and former amphetamine users had higher reward sensitivity than the control group. | The majority were male. Sociodemographic factors were not reported. Opioids and stimulants may be responsible for this decision making. |
| Giorgetta et al. (2014) [43] | Empirical research | To examine differences in the loss aversion of pathological gamblers and nongamblers, according to the stage of treatment of pathological gamblers. | N = 20 (17 were men). Age: = 36.45; SD = 9.1. Pathological gamblers (n = 10 in treatment less than 6 months and n = 10 in treatment more than 18 months). | Yes. (N = 20 nonplayers; 17 are male. Age: = 37.15; SD = 10.86) | A “decision under risk” task to assess loss aversion in gain and lose choices at 50% probability. In addition, the Baratt Impulsiveness Scale. | Pathological gamblers in treatment for more than 18 months presented greater loss aversion than the rest. There were no differences between the sample and the control group as a whole. Pathological gambling can be reduced with clinical treatment. | The sample was small. Pre and post measurements should be performed. Variables such as time discount or reward should be introduced. |
| Lorains et al. (2014) [44] | Empirical research | To observe differences in the decision making of the control group and the group of pathological players and between pathological players of strategic and nonstrategic games. | N = 39 (20 women). Age: = 46.64; DT = 9.46. Pathological gamblers (n = 15 strategic gamblers; n = 24 nonstrategic gamblers). | Yes. (N = 41 nongamblers; 21 men. Age: = 44.34; SD = 11.43) | Loss aversion task, which offered a 50% chance of winning or losing a variable amount of money. In addition, the Iowa Gambling Task. | Nonstrategic pathological players are less sensitive to losses. The nonstrategic group presented lower risk aversion than the control group and the group of strategic pathological gamblers. | The sample of pathological gamblers was seeking treatment. There was comorbidity with other mental disorders that may have affected their decision making but were not accounted for. The control group should present regular nonpathological gamblers. |
| Takeuchi et al. (2016) [45] | Empirical research | To test whether pathological gamblers differ from each other in terms of risk bias. | N = 31. Age: = 33.4; SD = 7.5 Men, pathological gamblers, who have completed a cycle of 12-step therapy. | Yes. (N = 26 nongamblers. Age: = 34.8; SD = 6.3) | Risky choice task. | Pathological gamblers should be divided into very aversive (emotionally vulnerable) or very aversive (impulsivist) groups for study, as there are significant differences between them. | Nonreal money was used. Some players were enrolled in an addiction treatment program. |
| Gelskov et al. (2016) [46] | Empirical research | To analyze the differences, at the cognitive and neuronal level between pathological gamblers and healthy subjects when making decisions. | N = 14. Age: = 29.43; SD = 6.05. Men, pathological gamblers. | Yes. (N = 15 nongamblers, all of them were men. Age: = 29.87; SD = 6.06) | A mixed play test that depended on whether the gain or loss situation came before or after, while performing an fMRI. | There were no significant differences in loss aversion between groups, but there was a tendency for pathological gamblers to have lower values. | Small sample. Pathological gamblers came from a treatment center. Events were presented quickly, which avoided delays between choices. |
| Strickland et al. (2017) [47] | Empirical research | To assess loss aversion in active cocaine users. | N = 38. Age: = 45.7; SD = 5.8 All of them were cocaine users. 42% women. At the time of the experiment, they were not under the effects of this drug. | No. | 3 questionnaires: valuation task, mixed gambles task and risk aversion task. They were given 30 dollars to carry out the experiment. At the end of the experiment, they received 10 dollars. | Less loss aversion among cocaine users. A rigid aversion to loss can generate a poor choice regarding cocaine consumption. Hence, being sensitive to this during treatment can help reduce drug consumption. | There was no control group. The possible influence of sociodemographic factors was not tested. |
| Bernhardt et al. (2017) [48] | Empirical research | To study probability discounting and loss aversion in alcohol consumers. | Study 1: N = 198. Age: = 18.38; SD = 0.2 Men. Social alcohol users. Study 2: N = 114. Age: = 44.77; SD = 10.56 18 women and 96 men, diagnosed with alcohol use disorder. | Study 1: No. Study 2: 17 women and 81 men. Age: = 43.75; SD = 10.86 | Two studies: Study 1: Value-based decision making for the study 1 sample. Study 2: Value-based decision making for the study 2 sample and the control group. | Study 1: Loss aversion does not predict changes in alcohol consumption. Study 2: Lower loss aversion in abstinent alcohol users. Subjects’ attitudes toward risk and loss make them more likely to relapse into binge drinking. | The used method needs to be verified. The rewards were of little value. Consumers were seeking treatment. Little female representation. |
| Genauk et al. (2017) [49] | Empirical research | To test, at a neuronal and cognitive level, whether people with alcohol use disorder and pathological gamblers show less loss aversion than a healthy population. | N = 34. n = 19 men, pathological gamblers. Age: = 32.9; SD = 10. n = 15 men, diagnosed of alcohol use disorder. Age: = 45.4; SD = 10.2. | Yes. (N = 17, nongamblers, neither alcohol users, all of them were men. Age: = 38.8; SD = 11.5) | Both the loss aversion task, which asks about desire to gamble, and a fMRI. | The subjects showed a lower aversion to loss than the healthy control group, both cognitively and neuronally. Pathological gamblers showed differences in severity, with more severity resulting in less aversion. | The sample was small and only included men. People with comorbidities were not included in the sample. |
| Meade et al. (2018) [50] | Empirical research | To analyze decision making in cocaine users and HIV-diagnosed individuals independently and in combination at the cognitive and neural levels. | N = 69 (47 men). Age: = 44.13; SD = 8.08. 16 non-HIV-positive cocaine users and 15 HIV-positive cocaine users. 21 non-HIV-positive cocaine users and 17 HIV-positive cocaine users. | No. | A loss aversion task and an fMRI administered at the same time. | Cocaine users have lower loss aversion, which is even lower among those with HIV. Neurologically, it seems that the pathways responsible for such aversion differ between cocaine users and people with HIV. | Subtle differences between groups could not be measured. Loss and gain situations were studied separately and connections between them were not analyzed. Cocaine users may have used other “soft” drugs. |
| Ring et al. (2018) [51] | Empirical research | To study risk perceptions in gain and loss situations, probability weighting and the level of loss aversion of pathological gamblers. | N = 48. Total mean age (sample and control group) is 38.9; SD = 14.7. Pathological gamblers group (n = 25; 3 are women). Habitual gamblers group (n = 23; 4 are women). | Yes. (N = 26; 6 are female. Played at most less than once a month). | 4 tests: Risk elicitation task, time preference elicitation task, threat-of-shock task and fMRI. | No significant differences were found in loss aversion. Pathological gamblers took greater risks and were less sensitive to changes than those in the control group. No significant differences were found in the shock task. | Higher stakes were not measured. Only two observations were used to assess loss aversion. The money was not real. No sociodemographic differences were studied. The sample was very small. The isolation effect cannot be assumed to be completely true. |
| Ojala et al. (2018) [52] | Empirical research | To observe whether blocking dopamine D2/D3 receptors decreased probability-weighting biases in gain and loss situations in a sample of pathological gamblers and nongamblers. | N = 16. Men, pathological gamblers (age: = 35.8; SD = 8.8). | Yes. (N = 21, men, nongamblers. Age: = 32.1; SD = 11.4). | An equivalent certainty task in decision making. The entire group performed the task 2 times, at least 1 week apart, once after taking the placebo and once after taking a dose of dogmatil 400 mg (which acts as a dopamine D2/D3 receptor antagonist). | No differences between groups were found, except in the loss situation, wherein the pathological gambler group showed devalued loss probabilities compared to the nongambler group in the placebo situation. | The sample was small and composed exclusively of men. Moderate test–retest reliability in decision making in addictive behaviors. Individual risk perceptions varied substantially between tests. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cabedo-Peris, J.; González-Sala, F.; Merino-Soto, C.; Pablo, J.Á.C.; Toledano-Toledano, F. Decision Making in Addictive Behaviors Based on Prospect Theory: A Systematic Review. Healthcare 2022, 10, 1659. https://doi.org/10.3390/healthcare10091659
Cabedo-Peris J, González-Sala F, Merino-Soto C, Pablo JÁC, Toledano-Toledano F. Decision Making in Addictive Behaviors Based on Prospect Theory: A Systematic Review. Healthcare. 2022; 10(9):1659. https://doi.org/10.3390/healthcare10091659
Chicago/Turabian StyleCabedo-Peris, Javier, Francisco González-Sala, César Merino-Soto, José Ángel Cahua Pablo, and Filiberto Toledano-Toledano. 2022. "Decision Making in Addictive Behaviors Based on Prospect Theory: A Systematic Review" Healthcare 10, no. 9: 1659. https://doi.org/10.3390/healthcare10091659
APA StyleCabedo-Peris, J., González-Sala, F., Merino-Soto, C., Pablo, J. Á. C., & Toledano-Toledano, F. (2022). Decision Making in Addictive Behaviors Based on Prospect Theory: A Systematic Review. Healthcare, 10(9), 1659. https://doi.org/10.3390/healthcare10091659