A Systematic Review of Psychometric Properties of Knee-Related Outcome Measures Translated, Cross-Culturally Adapted, and Validated in Arabic Language

 , ,
, ,  , and
, and
Abstract
1. Introduction
2. Materials and Methods
2.1. Registration and Protocol
2.2. Eligibility Criteria
2.3. Information Sources
2.4. Search Strategy
2.5. Selection Process
2.6. Data Collection Process
2.7. Data Items
2.8. Study Risk of Bias in Individual Studies
2.9. Effect Measures
2.10. Synthesis Methods
3. Results
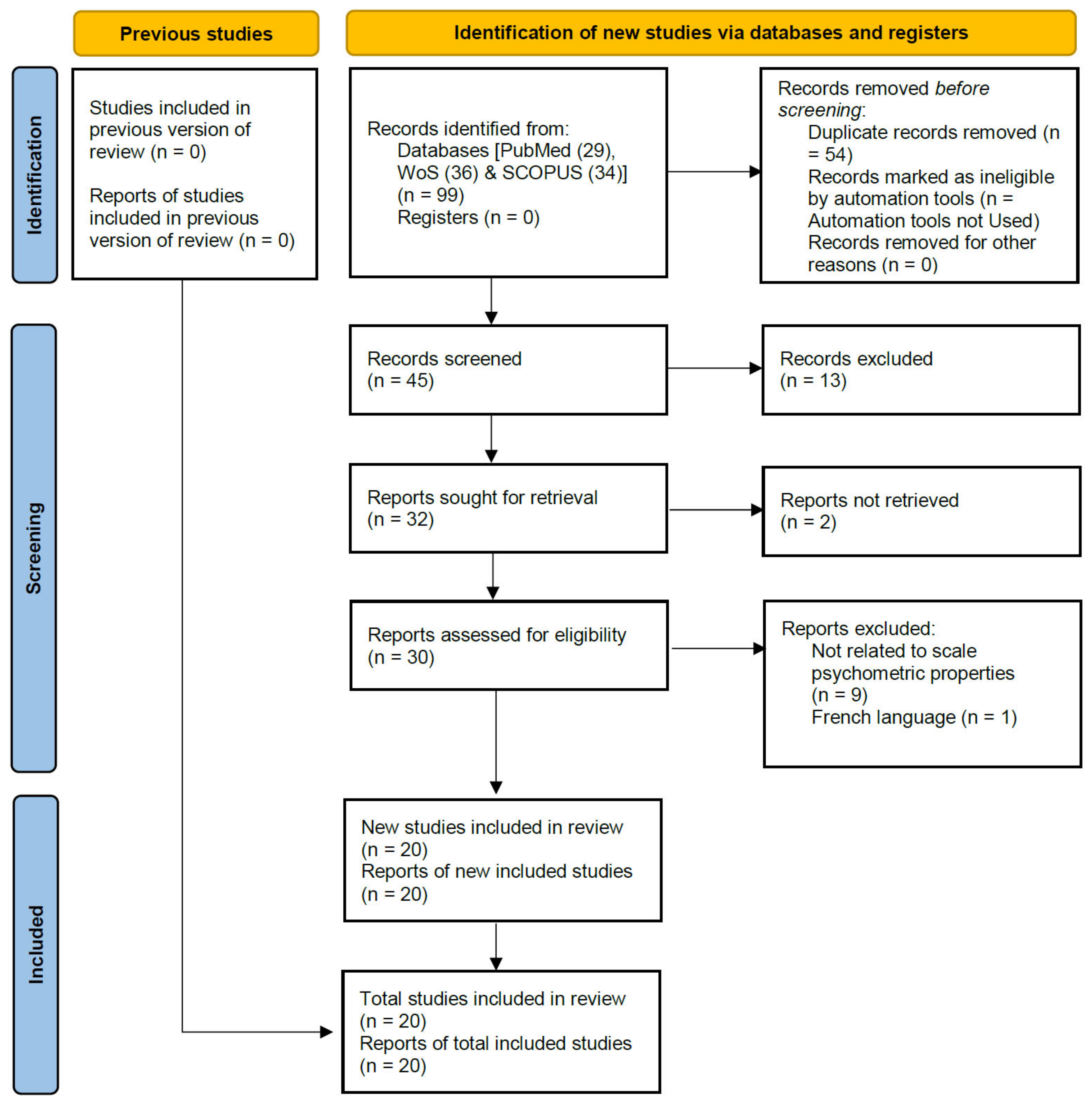
3.1. Study Selection
3.2. Study Characteristics
3.3. Risk of Bias within Studies
3.4. Results of Individual Studies
3.5. Results of Synthesis

{kind=link}
| Population | Disease Characteristics | Instrument Administration | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| PROM * | Ref | N | Age Mean (SD, Range) yr. | Gender % Female | Disease | Disease Duration Means (SD) yr. | Disease Severity | Setting | Country | Language | Response Rate |
| Reduced WOMAC | Alghadir et al. 2016 [28] | 140 | Mean 52.95 SD 9.31 Range 40–80 | 53.7% | Knee OA | K/L 1 15.7% K/L 2 45.5% K/L 3 29.8% K/L 4 09.1% | Physiotherapy OP | Saudi Arabia | Arabic | 86.43% | |
| KOOS | Alfadhel et al. 2018 [43] | 136 | Mean 58.77 SD 9.1 Range | 66.91% | Knee OA | Mean 5.91 SD 5.3 | Mild 15% Moderate 33% Severe 52% | Physiotherapy Outpatient | Saudi Arabia | Arabic | 89.71% |
| KOS-ADLS | Algarni et al. 2017 [30] | 280 | Mean 54.6 SD 10.5 Range | 57.14% | Various Knee conditions (Knee OA 88.2%) | Knee OA 88.2% Patellofemoral syndrome 7.9% RA 3.9% | Outpatient Clinic | Saudi Arabia | Arabic | NR | |
| Oxford Knee Score | Alghadir et al. 2017 [29] | 97 | Mean 57.55 SD 11.49 Range 40–80 | 0% | Knee OA | NR | Saudi Arabia | Arabic | 100% | ||
| Anterior Knee Pain Scale | Alshehri et al. 2017 [31] | 40 | Mean 34.7 SD 9.3 Range | 35% | Patellofemoral pain syndrome | Longer than 2 months | Hospital | Saudi Arabia | Arabic | NR | |
| Moroccan WOMAC | Faik et al. 2008 [37] | 71 | Mean 56.83 SD 8.28 Range 36–84 | 94.4% | Knee OA | Mean 6.24 SD 5.04 | Morocco | Arabic (Moroccan) | NR | ||
| Moroccan OAKHQoL | Serhier et al. 2012 [36] | 135 | Mean 56 SD 10 Range | 89% | Knee and Hip OA | Clinic and Rehabilitation setting | Morocco | Arabic (Moroccan) | 97% | ||
| Sfax Mod WOMAC | Guermazi et al. 2004 [14] | 103 | Mean 55.9 SD 7.67 Range 40–78 | 75.73% | Knee OA | Mean 4.0 SD 4.12 | Mean K/L 2.74 SD 0.77 Range 1–4 | NR | Tunisia | Arabic (North African dialect) | NR |
| KOOS | Almangoush et al. 2013 [39] | 129 | Mean 30.8 SD Range | 23.3% | ACL, meniscal, and combined injury | 7.2 months (Range 1–36 months) | ACL 38.0% Meniscal 27.9% Combined 34.1% | Knee centre | Egypt | Arabic | 87% |
| KOS-ADLS | Bouzubar et al. 2018 [42] | 108 | Mean 44.3 SD 14.5 Range 19–71 | 48.1% | Various Knee clinical and post-surgical conditions | OA 34.9% PFPS 13.2% Ligament reconstruction 12.2% Arthroplasty 10.4% | Govt hospital and physiotherapy department | Kuwait | Arabic | 4 weeks- 90.74% | |
| Kujala PFPSS | Hamdan et al. 2019 [40] | 97 | Mean 43.34 SD 14.50 Range 40–80 | 69.1% | PFPS | Anterior knee pain | Orthopaedic surgery clinic | Jordan | Arabic | 76.4% | |
| LKS | Ahmed et al. 2019 [38] | 100 | ACL tear (Mean: 21.5; Range: 18–25), meniscus tear (Mean: 27.3; Range: 25–30) and OA (Mean: 50.7; Range: 40–70) | 45% | ACL tear, meniscus tear, and knee OA | 15 days Pre-OP, 1 day Pre-OP, and 6 months post-OP | ACL tear (n = 30), meniscus tear (n = 20) and knee OA (n = 50) | University Hospital | Egypt | Arabic | 98% |
| OKS | Ahmed et al. 2019 [38] | 100 | ACL tear (Mean: 21.5; Range: 18-25), meniscus tear (Mean: 27.3; Range: 25–30) and OA (Mean: 50.7; Range: 40–70) | 45% | ACL tear, meniscus tear, and knee OA | 15 days Pre-OP, 1 day Pre-OP, and 6 months post-OP | ACL tear (n = 30), meniscus tear (n = 20) and knee OA (n = 50) | University hospital | Egypt | Arabic | 95% |
| IKDC | Ahmed et al. 2019 [38] | 100 | ACL tear (Mean: 21.5; Range: 18–25), meniscus tear (Mean: 27.3; Range: 25–30) and OA (Mean: 50.7; Range: 40–70) | 45% | ACL tear, meniscus tear, and knee OA | 15 days Pre-OP, 1 day Pre-OP and 6 months post-OP | ACL tear (n = 30), meniscus tear (n = 20) and knee OA (n = 50) | University hospital | Egypt | Arabic | 97% |
| Knee ICOPQ | Alageel et al. 2020 [25] | 90 | 51.1 | orthopaedic surgery clinic | |||||||
| KOOS-PF | Ateef 2020 [33] | 95 | Mean 49.75 SD 9.87 Range 40–80 | 0 | PFPS | Anterior knee pain | Outpatient departments | KSA | Arabic | 88.4% | |
| OKS | Bodor et al. 2020 [34] | 100 | Mean: 62 SD: 11.3 | TKR | KSA | Arabic | |||||
| OAQoL | Al-Ajmi and Al-Ghamdi 2021 [32] | 59 | Mean: 48.4 SD: 11.3 | 47.5% | OA | OA | KSA | Arabic | 100% | ||
| Kujala score | Haddad et al. 2021 [41] | 94 | Mean 43.67 SD 14.46 | 70.2% | PFPS | Anterior knee pain | Orthopedic OP clinic | Jordan | Arabic | 70.1% | |
| ACL-RSI | ACL-RSI Alzhrani et al. 2022 [26] | 60 | Mean 11.22 SD 3.84 | 0% | ACL Reconstruction | Mean 11.22 SD 3.84 | ACL injury | Online mode Via Google Forms | KSA | Arabic | 100% |
| TAS | Alzhrani et al. 2022 [27] | 75 | Mean 32.31 SD 7.28 | 0% | ACL Reconstruction | >3 month Post ACL Reconstruction | ACL injury | Online mode Via SurveyMonkey | KSA | Arabic | 100% |
| KOOS-PF-F | Alzhrani et al. 2022 [35] | 105 | Mean 51.62 SD 8.49 Range 34–66 | 100% | PFPS | NR | Anterior knee pain | PT OPD, University hospital | KSA | Arabic | 87.6% |
| PROM (ref) | Distribution of Scores in the Study Population | Percentage of Missing Items and Percentage of Missing Total Scores | Floor and Ceiling Effects | Scores and Change Scores Available for Relevant (sub) Groups | Minimal Important Change (MIC) or Minimal Important Difference (MID) |
|---|---|---|---|---|---|
| Reduced WOMAC (Alghadir et al. 2016) [28] | Pain 1–16 Function 1–27 Total 3–43 | NR | NR | NR | Pain 3.80 Function 5.24 Total 8.15 |
| KOOS (Alfadhel et al. 2018) [43] | Pin 45.6 ± 18.7 Symptom 52.9 ± 21 ADL 47.4 ± 20.1 Sports 17.7 ± 18.9 Knee QOL 31 ± 17 | ? | Floor Pain 0.7% Sports 26.5% Knee QOL 3.7% Ceiling Symptoms 0.7% | NR | Pain 13.91 Symptoms 14.25 ADL 13.46 Sports 14.56 Knee QOL 12.57 |
| KOS-ADLS (Algarni et al. 2017) [30] | NR | NR | NR | NR | NR |
| Oxford Knee Score (OKS) (Alghadir et al. 2017) [29] | Function 12–59 | NR | Floor 2.1% Ceiling 1% | NR | Function 6.2 |
| Anterior Knee Pain Scale (Alshehri et al. 2017) [31] | Total 59.3 ± 17.3 | NR | 0% each | NR | NR |
| Moroccan WOMAC (Faik et al. 2008) [37] | Pain 10.7 ± 3.9 Stiffness 4.45 ± 1.95 ADL 38.48 ± 11.65 Total 53.59 ± 16.32 | NR | NR | NR | NR |
| Moroccan OAKHQoL (Serhier et al. 2012) [36] | PA 42.5 ± 21.6 Mental health 52.8 ± 20.7 Pain 45.0 ± 27.8 Social support 59.4 ± 24.0 Social function 60.8 ± 27.5 | Reported Average 2.1% Range 0–52% | Reported Floor (individual item range) 2.6–65.6% Ceiling (individual item range) 7.7–56.5% | Reported Age, sex, and joints involved | NR |
| Sfax Modif WOMAC (Guermazi et al. 2004) [14] | Pain 3–19 Stiffness 0–8 Function 2–27 | Reported 3 questions (function subscale) removed | Ceiling 0% Floor 0% | NR | NR |
| KOOS (Almangoush et al. 2013) [39] | Pain 3–72 Symptoms 4–64 ADL 0–62 Sport 5–100 QOL 3–72 | 0.21% of all answered items | Ceiling- 3.1% in ADL subscale Floor- 1.6% in sport subscale | NR | NR |
| KOS-ADLS (Bouzubar et al., 2018) [42] | Total 50.4 ± 18.1 | NR | Ceiling 0% Floor 0% | NR | MID 14% MIC 8.7 |
| Kujala PFPSS (Hamdan et al. 2019) [40] | 62.38 ± 17.78 to 64.02 ± 18.47 | NR | NR | NR | NR |
| OKS, LKS, IKDC (Ahmed et al. 2019) [38] | NR | NR | NR | NR | NR |
| Knee ICOPQ (Alageel et al. 2020) [25] | NR | NR | NR | NR | NR |
| KOOS-PF (Ateef 2020) [33] | NR | NR | NR | NR | NR |
| OKS (Bodor et al. 2020) [34] | NR | NR | NR | NR | NR |
| OAQoL (Al-Ajmi and Al-Ghamdi 2021) [32] | 35.63 ± 12.25 | Floor–4,7% to 13.9%; ceiling–2.2% to 13.4% | MDC: 16.91% | ||
| Kujala score (Haddad et al. 2021) [41] | 63.91 ± 16.32 to 66.52 ± 17.50 | NR | NR | NR | NR |
| ACL-RSI (Alzhrani et al. 2022) [26] | 29.72 ± 9.91 | NR | Floor—5%; Ceiling—0%; | NR | MDCIndividual: 20.08; MDCGroup: 3.44 |
| TAS (Alzhrani et al., 2022) [27] | 4.60 ± 2.75 | NR | Floor—0%; ceiling 2.7.6% | NR | MDCIndividual: 2.39; MDCGroup: 0.41 |
| KOOS-PF-F (Alzhrani et al., 2022) [35] | 29.72 ± 9.91 | NR | Floor—0.9% to 13.9%; ceiling—3.8% to 13.6% | NR | MDC: 22.96% |
| PROM (Ref) | Country (Language) in which the PROM Was Evaluated | Modifications | Internal Consistency | Construct Validity | Reproducibility | Floor/Ceiling Effect (%) | Responsiveness | Quality COSMIN |
|---|---|---|---|---|---|---|---|---|
| Reduced WOMAC (Alghadir et al. 2016) [28] | Saudi Arabia (Arabic) | Cultural adaptations | ? | NR | Pain 0.89 Function 0.90 Total 0.91 | NR | NR | ? |
| KOOS (Alfadhel et al. 2018) [43] | Saudi Arabia (Arabic) | Cultural adaptations | Pain 0.87 Sym 0.91 ADL 0.88 Sport 0.92 QOL 0.90 | NR | Pain 0.93 Symptom 0.94 ADL 0.94 Sport 0.92 Knee QOL 0.93 | Floor Pain 0.7% Sports 26.5% Knee QOL 3.7% Ceiling Symptoms 0.7% | NR | ? |
| KOS-ADLS (Algarni et al. 2017) [30] | Saudi Arabia (Arabic) | Cultural adaptations | Total 0.902 | NR | NR | NR | NR | ? |
| Oxford Knee Score (OKS) (Alghadir et al. 2017) [29] | Saudi Arabia (Arabic) | Cultural adaptations | Total 0.98 | NR | Total 0.973 | Floor 2.1% Ceiling 1% | NR | ? |
| Anterior Knee Pain Scale (Alshehri et al. 2017) [31] | Saudi Arabia | Cultural adaptations | Total 0.81 | NR | Total 0.96 | 0% each | NR | ? |
| Moroccan WOMAC (Faik et al. 2008) [37] | Morocco (Arabic- Moroccan dialect) | Cultural adaptations | Pain 0.76 Stiff 0.76 ADL 0.90 Total 0.92 | NR | Pain 0.80 Stiffness’ 0.77 ADL 0.89 Total 0.91 | NR | NR | ? |
| Moroccan OAKHQoL (Serhier et al. 2012) [36] | Morocco (Arabic- Moroccan dialect) | Cultural adaptations | PA 0.93 Mental heal 0.84 Pain 0.88 Social sup 0.50 Social function 0.60 | Age- no diff except PA Sex- no differ Joint involves- no differ | PA Inter 0.90 Intra 0.83 Mental health Inter 0.83 Intra 0.65 Pain Inter 0.81 Intra 0.70 Social support Inter 0.64 Intra 0.71 Social function Inter 0.58 Intra 0.54 | Reported Floor (individual item range) 2.6–65.6% Ceiling (individual item range) 7.7–56.5% | NR | ? |
| Sfax Modif WOMAC (Guermazi et al. 2004) [14] | Tunisia (North African dialect) | Cultural adaptations | NR | NR | Pain 0.84 Stiffness 0.84 Function 0.92 | Ceiling 0% Floor 0% | NR | ? |
| KOOS (Almangoush et al. 2013) [39] | Arabic | Cultural adaptations | Pain 0.92 Symptom 0.82 ADL 0.95 Sport 0.91 QOL 0.80 | NR | Pain 0.954 Symptom 0.931 ADL 0.957 Sport 0.941 QOL 0.875 | Ceiling- 3.1% in ADL subscale Floor- 1.6% in sport subscale | NR | ? |
| KOS-ADLS (Bouzubar et al., 2018) [42] | Arabic | Cultural adaptations | Total 0.97 | NR | Total 0.97 | Ceiling 0% Floor 0% | ES 1.12 Improvement in 86.7% AUC 0.73 Functional improvement 14% | ? |
| Kujala PFPSS (Hamdan et al. 2019) [40] | Arabic | Translations | Total: 0.824 | Total: ICC = 0.948 (0.923–0.965) | NR | Improvement in 47.4% | ? | |
| LKS (Ahmed et al. 2019) [38] | Arabic | Cultural adaptations | Total: 0.9 | KOOS: 0.7 | Total: ICC = 0.8 | NR | NR | ? |
| OKS (Ahmed et al. 2019) [38] | Arabic | Cultural adaptations | Total: 0.9 | KOOS: 0.913 | Total: ICC = 0.85 | NR | NR | ? |
| IKDC (Ahmed et al. 2019) [38] | Arabic | Cultural adaptations | Total: 0.89 | KOOS: 0.58 | Total: ICC = 0.95 | NR | NR | ? |
| Knee ICOPQ (Alageel et al. 2020) [25] | Arabic | Cultural adaptations | Total: 0.88 | KOOS: 0.235 | Total: ICC = 0.841 | NR | NR | ? |
| KOOS-PF (Ateef 2020) [33] | Arabic | Cultural adaptations | Total: 0.81 | −0.568 | Total: ICC = 0.959 (0.855–0.965) | Ceiling: 2.2–13.4% Floor: 4.7–13.9% | NR | + |
| OKS (Bodor et al. 2020) [34] | Arabic | Cultural adaptations | Total: 0.85 | KOOS-Ar: rs = 0.73 | Total: rs = 0.94 | Ceiling 0% Floor 0% | 3.09 | ? |
| OAQoL (Al-Ajmi and Al-Ghamdi 2021) [32] | Saudi Arabia (Arabic) | Cultural adaptations | Total: 0.93 | NR | Total: ICC = 0.93 | NR | NR | ? |
| Kujala score (Haddad et al., 2021) [41] | Arabic | Cultural adaptations | Total: 0.806 | NR | Total: ICC = 0.806 (0.742–0.859) | NR | Improvement in 45.7% | ? |
| ACL-RSI (Alzhrani et al., 2022) [26] | Arabic | Cultural adaptations | Total: 0.734 | IKDC-Ar: rs = 0.515; KOOS-Ar: rs = 0.542 | Total: ICC = 0.871 (0.743–0.935) | Ceiling—0%; Floor—5% | NR | - |
| TAS (Alzhrani et al., 2022) [27] | Arabic | Cultural adaptations | NR | IKDC-Ar: rs = 0.476; KOOS-Ar: rs = 0.469 | Total: ICC = 0.836 (0.687–0.914) | Ceiling—2.7.6%; Floor—0% | NR | - |
| KOOS-PF-F (Alzhrani et al., 2022) [35] | Arabic | Cultural adaptations | Total: 0.93 | −0.783 | Total: ICC = 0.893 (0.889–0.970) | Ceiling: 0.9%–13.9% Floor: 3.8%–13.6% | NR | ? |
| PROM (ref) | Structural Validity | Internal Consistency | Reliability | MEASUREMENT Error | Hypothesis Testing for Construct Validity | Cross-Cultural Validity | Criterion Validity | RESPONSIVENESS | Final |
|---|---|---|---|---|---|---|---|---|---|
| Reduced WOMAC (Alghadir et al. 2016) [28] | + | + | + | + | ? | ? | ? | ? | ? |
| KOOS (Alfadhel et al. 2018) [43] | + | + | + | + | ? | ? | ? | ? | ? |
| KOS-ADLS (Algarni et al. 2017) [30] | + | + | + | + | + | + | + | + | - |
| Oxford Knee Score (OKS) (Alghadir et al. 2017) [29] | + | + | + | + | ? | ? | ? | ? | ? |
| Anterior Knee Pain Scale (Alshehri et al. 2017) [31] | + | + | + | ? | ? | ? | ? | ? | ? |
| Moroccan WOMAC (Faik et al. 2008) [37] | + | + | + | + | + | ? | ? | ? | ? |
| Moroccan OAKHQoL (Serhier et al. 2012) [36] | + | + | + | - | + | ? | ? | ? | ? |
| Sfax Modif WOMAC (Guermazi et al. 2004) [14] | + | + | + | + | + | + | + | + | - |
| KOOS (Almangoush et al. 2013) [39] | + | + | + | + | + | + | + | + | - |
| KOS-ADLS (Bouzubar et al. 2018) [42] | + | + | + | + | ? | ? | ? | + | ? |
| Kujala PFPSS (Hamdan et al. 2019) [40] | + | + | + | - | ? | ? | ? | ? | ? |
| LKS (Ahmed et al. 2019) [38] | + | + | + | - | ? | ? | ? | ? | ? |
| OKS (Ahmed et al. 2019) [38] | + | + | + | - | ? | ? | ? | ? | ? |
| IKDC (Ahmed et al. 2019) [38] | + | + | + | - | + | ? | ? | ? | ? |
| Knee ICOPQ (Alageel et al. 2020) [25] | + | + | + | - | + | ? | ? | ? | ? |
| KOOS-PF (Ateef 2020) [33] | + | + | + | + | + | + | - | + | - |
| OKS (Bodor et al. 2020) [34] | + | + | + | ? | ? | ? | ? | ? | ? |
| OAQoL (Al-Ajmi and Al-Ghamdi 2021) [32] | + | + | + | ? | ? | ? | ? | ? | ? |
| Kujala score (Haddad et al., 2021) [41] | - | + | ? | - | ? | ? | ? | ? | - |
| ACL-RSI (Alzhrani et al., 2022) [26] | - | + | + | + | + | ? | - | ? | - |
| TAS (Alzhrani et al., 2022) [27] | - | ? | + | + | + | ? | - | ? | - |
| KOOS-PF-F (Alzhrani et al., 2022) [35] | + | + | + | + | + | + | + | ? | ? |
3.6. Reporting Risk of Bias across Studies
3.7. Summary of Evidence
3.7.1. Responsiveness to Treatment Properly
3.7.2. Minimal Important Change (MIC) or Minimal Important Difference (MID)
3.7.3. Floor/Ceiling Effect (%)
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Alghadir, A.; Anwer, S. Prevalence of musculoskeletal pain in construction workers in Saudi Arabia. Sci. World J. 2015, 2015, 529873. [Google Scholar] [CrossRef] [PubMed]
- Kulandaivelan, S.; Tigdania, N.; Ateef, M.; Chaturvedi, R.; Joshi, S.; Malik, A.; Pahinian, A. Prevalence of knee pain and its correlates with specific emphasis on CVD risk factors in Hisar urban population. Int. J. Clin. Rheumtol. 2017, 12, 91–96. [Google Scholar]
- Ismail, A.I.; Al-Abdulwahab, A.H.; Al-Mulhim, A.S. Osteoarthritis of knees and obesity in Eastern Saudi Arabia. Saudi Med. J. 2006, 27, 1742–1744. [Google Scholar] [PubMed]
- Sacitharan, P.K. Ageing and Osteoarthritis. Subcell. Biochem. 2019, 91, 123–159. [Google Scholar] [CrossRef]
- Safiri, S.; Kolahi, A.-A.; Smith, E.; Hill, C.; Bettampadi, D.; Mansournia, M.A.; Hoy, D.; Ashrafi-Asgarabad, A.; Sepidarkish, M.; Almasi-Hashiani, A.; et al. Global, regional and national burden of osteoarthritis 1990–2017: A systematic analysis of the Global Burden of Disease Study 2017. Ann. Rheum. Dis. 2020, 79, 819–828. [Google Scholar] [CrossRef]
- Hunter, D.J.; Bierma-Zeinstra, S. Osteoarthritis. Lancet 2019, 393, 1745–1759. [Google Scholar] [CrossRef]
- Shamekh, A.; Alizadeh, M.; Nejadghaderi, S.A.; Sullman, M.J.M.; Kaufman, J.S.; Collins, G.S.; Kolahi, A.-A.; Safiri, S. The Burden of Osteoarthritis in the Middle East and North Africa Region From 1990 to 2019. Front. Med. 2022, 9, 881391. [Google Scholar] [CrossRef]
- Ateef, M.; Kulandaivelan, S.; Tahseen, S. Test & retest reliability and correlates of 6-minute walk test in patients with primary osteoarthritis of knees. Indian J. Rheumatol. 2016, 11, 192–196. [Google Scholar] [CrossRef]
- Ateef, M.; Kulandaivelan, S.; Alqahtani, M. Cross-Cultural Validation of Urdu Version KOOS in Indian Population with Primary Knee Osteoarthritis. Int. J. Rheumatol. 2017, 2017, 1206706. [Google Scholar] [CrossRef]
- Li, Q.; Qi, X.; Zhang, Z. Intra-articular oxygen-ozone versus hyaluronic acid in knee osteoarthritis: A meta-analysis of randomized controlled trials. Int. J. Surg. 2018, 58, 3–10. [Google Scholar] [CrossRef]
- Anwer, S.; Alghadir, A.; Zafar, H.; Brismée, J.-M. Effects of orthopaedic manual therapy in knee osteoarthritis: A systematic review and meta-analysis. Physiotherapy 2018, 104, 264–276. [Google Scholar] [CrossRef]
- Green, A.; Liles, C.; Rushton, A.; Kyte, D.G. Measurement properties of patient-reported outcome measures (PROMS) in Patellofemoral Pain Syndrome: A systematic review. Man. Ther. 2014, 19, 517–526. [Google Scholar] [CrossRef]
- Gagnier, J.J.; Mullins, M.; Huang, H.; Marinac-Dabic, D.; Ghambaryan, A.; Eloff, B.; Mirza, F.; Bayona, M. A Systematic Review of Measurement Properties of Patient-Reported Outcome Measures Used in Patients Undergoing Total Knee Arthroplasty. J. Arthroplast. 2017, 32, 1688–1697.e7. [Google Scholar] [CrossRef]
- Guermazi, M.; Poiraudeau, S.; Yahia, M.; Mezganni, M.; Fermanian, J.; Habib Elleuch, M.; Revel, M. Translation, adaptation and validation of the Western Ontario and McMaster Universities osteoarthritis index (WOMAC) for an Arab population: The Sfax modified WOMAC. Osteoarthr. Cartil. 2004, 12, 459–468. [Google Scholar] [CrossRef][Green Version]
- Harris, K.; Dawson, J.; Gibbons, E.; Lim, C.R.; Beard, D.J.; Fitzpatrick, R.; Price, A.J. Systematic review of measurement properties of patient-reported outcome measures used in patients undergoing hip and knee arthroplasty. Patient Relat. Outcome Meas. 2016, 7, 101–108. [Google Scholar] [CrossRef]
- Wang, D.; Jones, M.H.; Khair, M.M.; Miniaci, A. Patient-reported outcome measures for the knee. J. Knee Surg. 2010, 23, 137–151. [Google Scholar] [CrossRef]
- Guillemin, F.; Bombardier, C.; Beaton, D. Cross-cultural adaptation of health-related quality of life measures: Literature review and proposed guidelines. J. Clin. Epidemiol. 1993, 46, 1417–1432. [Google Scholar] [CrossRef]
- Beaton, D.E.; Bombardier, C.; Guillemin, F.; Ferraz, M.B. Guidelines for the process of cross-cultural adaptation of self-report measures. Spine 2000, 25, 3186–3191. [Google Scholar] [CrossRef]
- Wang, W.-L.; Lee, H.-L.; Fetzer, S.J. Challenges and strategies of instrument translation. West. J. Nurs. Res. 2006, 28, 310–321. [Google Scholar] [CrossRef]
- Kamusella, T. The Arabic Language: A Latin of Modernity? J. Natl. Mem. Lang. Polit. 2017, 11, 117–145. [Google Scholar] [CrossRef]
- Prinsen, C.A.C.; Mokkink, L.B.; Bouter, L.M.; Alonso, J.; Patrick, D.L.; De Vet, H.C.W.; Terwee, C.B. COSMIN guideline for systematic reviews of patient-reported outcome measures. Qual. Life Res. Int. J. Qual. Life Asp. Treat. Care Rehabil. 2018, 27, 1147–1157. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [PubMed]
- Mokkink, L.B.; De Vet, H.C.W.; Prinsen, C.A.C.; Patrick, D.L.; Alonso, J.; Bouter, L.M.; Terwee, C.B. COSMIN Risk of Bias checklist for systematic reviews of Patient-Reported Outcome Measures. Qual. Life Res. Int. J. Qual. Life Asp. Treat. Care Rehabil. 2018, 27, 1171–1179. [Google Scholar] [CrossRef] [PubMed]
- Terwee, C.B.; Prinsen, C.A.C.; Chiarotto, A.; Westerman, M.J.; Patrick, D.L.; Alonso, J.; Bouter, L.M.; De Vet, H.C.W.; Mokkink, L.B. COSMIN methodology for evaluating the content validity of patient-reported outcome measures: A Delphi study. Qual. Life Res. Int. J. Qual. Life Asp. Treat. Care Rehabil. 2018, 27, 1159–1170. [Google Scholar] [CrossRef]
- Alageel, M.; Al Turki, A.; Alhandi, A.; Alohali, R.; Alsalem, R.; Aleissa, S. Cross-Cultural Adaptation and Validation of the Arabic Version of the Intermittent and Constant Osteoarthritis Pain Questionnaire. Sport. Med. Int. Open 2020, 4, E8–E12. [Google Scholar] [CrossRef] [PubMed]
- Alzhrani, M.; Alzahrani, H.; Alshehri, Y.S. Arabic Version of the Short Anterior Cruciate Ligament–Return to Sport After Injury Scale: Translation, Cross-cultural Adaptation, and Validation. Orthop. J. Sport. Med. 2021, 10, 23259671211066509. [Google Scholar] [CrossRef] [PubMed]
- Alzhrani, M.; Alzahrani, H.; Alshehri, Y.S. The Arabic Version of the Tegner Activity Scale in Patients with Anterior Cruciate Ligament Reconstruction: Translation, Validation, and Cross-Cultural Adaptation. Int. J. Environ. Res. Public Health 2022, 19, 1987. [Google Scholar] [CrossRef] [PubMed]
- Alghadir, A.; Anwer, S.; Iqbal, Z.A.; Alsanawi, H.A. Cross-cultural adaptation, reliability and validity of the Arabic version of the reduced Western Ontario and McMaster Universities Osteoarthritis index in patients with knee osteoarthritis. Disabil. Rehabil. 2016, 38, 689–694. [Google Scholar] [CrossRef]
- Alghadir, A.H.; Al-Eisa, E.S.; Anwer, S. Cross-cultural adaptation and psychometric analysis of the Arabic version of the oxford knee score in adult male with knee osteoarthritis. BMC Musculoskelet. Disord. 2017, 18, 190. [Google Scholar] [CrossRef]
- Algarni, A.D.; Alrabai, H.M.; Al-Ahaideb, A.; Kachanathu, S.J.; AlShammari, S.A. Arabic translation, cultural adaptation, and validation study of Knee Outcome Survey: Activities of Daily Living Scale (KOS-ADLS). Rheumatol. Int. 2017, 37, 1585–1589. [Google Scholar] [CrossRef]
- Alshehri, A.; Lohman, E.; Daher, N.S.; Bahijri, K.; Alghamdi, A.; Altorairi, N.; Arnons, A.; Matar, A. Cross-Cultural Adaptation and Psychometric Properties Testing of the Arabic Anterior Knee Pain Scale. Med. Sci. Monit. Int. Med. J. Exp. Clin. Res. 2017, 23, 1559–1582. [Google Scholar] [CrossRef][Green Version]
- AlAjmi, M.; Al-Ghamdi, S. Translation and validation of the Arabic version of the osteoarthritis quality of life questionnaire (OAQoL) in Saudi patients with osteoarthritis. Health Qual. Life Outcomes 2021, 19, 91. [Google Scholar] [CrossRef]
- Ateef, M. Measurement properties of the knee injury and osteoarthritis outcome score patello-femoral questionnaire in saudi arabians. PeerJ 2020, 8, e9323. [Google Scholar] [CrossRef]
- Bin Sheeha, B.; Williams, A.; Johnson, D.S.; Granat, M.; Bin Nasser, A.; Jones, R. Responsiveness, Reliability, and Validity of Arabic Version of Oxford Knee Score for Total Knee Arthroplasty. J. Bone Jt. Surg. Am. 2020, 102, e89. [Google Scholar] [CrossRef]
- Alzhrani, M. Knee Injury and Osteoarthritis Outcome Score Patellofemoral Questionnaire: Psychometric Properties among Females of Kingdom of Saudi Arabia. Int. J. Environ. Res. Public Health 2022, 19, 6058. [Google Scholar] [CrossRef]
- Serhier, Z.; Harzy, T.; ELfakir, S.; Diouny, S.; El Rhazi, K.; Bennani Othmani, M.; Salmi, L.R.; Nejjari, C. Cross-cultural adaptation and validation of the knee and hip health-related quality of life (OAKHQoL) in a Moroccan Arabic-speaking population. Rheumatol. Int. 2012, 32, 1015–1023. [Google Scholar] [CrossRef]
- Faik, A.; Benbouazza, K.; Amine, B.; Maaroufi, H.; Bahiri, R.; Lazrak, N.; Aboukal, R.; Hajjaj-Hassouni, N. Translation and validation of Moroccan Western Ontario and McMaster Universities (WOMAC) osteoarthritis index in knee osteoarthritis. Rheumatol. Int. 2008, 28, 677–683. [Google Scholar] [CrossRef]
- Ahmed, K.M.; Said, H.G.; Ramadan, E.K.A.; Abd El-Radi, M.; El-Assal, M.A. Arabic translation and validation of three knee scores, Lysholm Knee Score (LKS), Oxford Knee Score (OKS), and International Knee Documentation Committee Subjective Knee Form (IKDC). Sicot-J 2019, 5, 6. [Google Scholar] [CrossRef]
- Almangoush, A.; Herrington, L.; Attia, I.; Jones, R.; Aldawoudy, A.; Abdul Aziz, A.; Waley, A. Cross-cultural adaptation, reliability, internal consistency and validation of the Arabic version of the knee injury and osteoarthritis outcome score (KOOS) for Egyptian people with knee injuries. Osteoarthr. Cartil. 2013, 21, 1855–1864. [Google Scholar] [CrossRef]
- Hamdan, M.; Haddad, B.; Isleem, U.; Hamad, A.; Hussein, L.; Shawareb, Y.; Hadidi, F.; Alryalat, S.A.; Samarah, O.; Khanfar, A.; et al. Validation of the Arabic version of the Kujala patellofemoral pain scoring system. J. Orthop. Sci. 2019, 24, 290–293. [Google Scholar] [CrossRef]
- Haddad, B.I.; Hamdan, M.; Isleem, U.; Al-Saber, M.G.; Al-Hadidi, F.A.; AlRyalat, S.A.; Alnaimat, F. Validation of the cultural adaptation of the Kujala score in Arabic. J. Orthop. Surg. Res. 2021, 16, 323. [Google Scholar] [CrossRef]
- Bouzubar, F.F.; Aljadi, S.H.; Alotaibi, N.M.; Irrgang, J.J. Cross-cultural adaptation and validation of the Arabic version of the knee outcome survey-activities for daily living scale. Disabil. Rehabil. 2018, 40, 1817–1828. [Google Scholar] [CrossRef]
- Alfadhel, S.A.; Vennu, V.; Alnahdi, A.H.; Omar, M.T.; Alasmari, S.H.; AlJafri, Z.; Bindawas, S.M. Cross-cultural adaptation and validation of the Saudi Arabic version of the Knee Injury and Osteoarthritis Outcome Score (KOOS). Rheumatol. Int. 2018, 38, 1547–1555. [Google Scholar] [CrossRef]
- Oorschot, S.; Chiwaridzo, M.; CM Smits-Engelsman, B. Psychometric evaluation of commonly used game-specific skills tests in rugby: A systematic review. BMJ Open Sport Exerc. Med. 2017, 3, e000281. [Google Scholar] [CrossRef]
- Zaccagnini, M.; Ataman, R.; Nonoyama, M.L. The Withdrawal Assessment Tool to identify iatrogenic withdrawal symptoms in critically ill paediatric patients: A COSMIN systematic review of measurement properties. J. Eval. Clin. Pract. 2021, 27, 976–988. [Google Scholar] [CrossRef]
- Harrison, J.L.; Brownlow, C.L.; Ireland, M.J.; Piovesana, A.M. Empathy Measurement in Autistic and Nonautistic Adults: A COSMIN Systematic Literature Review. Assessment 2022, 29, 332–350. [Google Scholar] [CrossRef]
- Climent-Sanz, C.; Marco-Mitjavila, A.; Pastells-Peiró, R.; Valenzuela-Pascual, F.; Blanco-Blanco, J.; Gea-Sánchez, M. Patient Reported Outcome Measures of Sleep Quality in Fibromyalgia: A COSMIN Systematic Review. Int. J. Environ. Res. Public Health 2020, 17, 2992. [Google Scholar] [CrossRef] [PubMed]

| PROM | Target Population | Mode of Administration (e.g., self-Report, Interview-Based, Parent/Proxy Report, etc.) | Recall Period | (Sub)Scale (s) (Number of Items) | Response Options | Range of Scores/Scoring | Original Language | Available Translations |
|---|---|---|---|---|---|---|---|---|
| Reduced WOMAC (Alghadir et al. 2016) [28] | Knee OA | Self-report | 48 h | Pain (5); Function (7) | 0–4 | Pain 0–20 Function 0–28 Overall 0–48 | English | Arabic (Saudi) |
| KOOS (Alfadhel et al. 2018) [43] | Knee OA | Self-report | 1 week | Pain (9); Symptom (7); ADL (17); Sports (5); Knee QOL (4) | 0–4 | 0–100 for each scale where a higher score indicates better health | English | Arabic (Saudi) |
| KOS-ADLS (Algarni et al. 2017) [30] | Various Knee complaints (Knee OA 88.2%) | Self-report | Within 1 week | Symptom (6); Function (8) | 0–5 | 0–100 | English | Arabic (Saudi) |
| Oxford Knee Score (OKS) (Alghadir et al. 2017) [29] | Knee OA | Self-report | Within 1 week | Function (12) | 0–4 | 0–48 | English | Arabic (Saudi) |
| Anterior Knee Pain Scale (Alshehri et al. 2017) [31] | Patellofemoral Pain | Self-report | 2–3 days | Symptom and Function (13) | Varying | 0–100 | English | Arabic (Saudi) |
| Moroccan WOMAC (Faik et al. 2008) [37] | Knee OA | Self-report | 1–2 days | Pain (5); Stiffness (2); ADL (17); | 0–4 | Pain 0–20 Stiffness 0–8 ADL 0–68 Total 0–96 | English | Arabic (Moroccan) |
| Moroccan OAKHQoL (Serhier et al. 2012) [36] | Knee and Hip OA | Self-report | 3–10 days | PA (16); Mental Health (13); Pain (4); Social support (4); Social function (3); 3 items; | Individual items 1–10 | Subscales 0–100 100 mean best QOL | French | Arabic (Moroccan) |
| Sfax Modif WOMAC (Guermazi et al. 2004) [14] | Knee OA | Interviewer | 24 h | Pain (5); Stiffness (2); Function (9); | 0–4 | Pain 0–20 Stiffness 0–8 Function 0–36 | English | Arabic (Tunisia) |
| KOOS (Almangoush et al. 2013) [39] | ACL, Meniscal, and combined injury | Self-report | 1 week | Pain (9); Symptom (7); ADL (17); Sport (5); QOL (4) | 0–4 | 0–100 in which 100 means no Knee problem | English | Arabic (Egypt) |
| KOS-ADLS (Bouzubar et al., 2018) [42] | Various Knee conditions (63%) and post-surgery (37%)- Knee OA 35% | Self-report | 2–4 days | Symptom (6); Function (8) | 0–5 | 0–100 in which 100 means perfect health | English | Arabic (Kuwait) |
| Kujala PFPSS (Hamdan et al. 2019) [40] | Patellofemoral pain syndrome | Self-report | 2 Weeks | The severity of symptoms (13 factors) | 0–10 | 0–100 in which 100 means good Knee function | English | Arabic (Jordan) |
| OKS, LKS, IKDC (Ahmed et al. 2019) [38] | ACL tear, meniscus tear, and knee osteoarthritis | Self-report | 15 days | Instability (25); Pain (25); Catching (15); Stair climbing (10); Swelling (10); Support (5); Squatting (5); Limping (5) | 0–5/10/15/25 | 0–100 in which 100 means symptoms | English | Arabic (Egypt) |
| Knee ICOPQ (Alageel et al. 2020) [25] | Arabic (Saudi) | |||||||
| KOOS-PF (Ateef 2020) [33] | Patellofemoral pain syndrome | Self-report | 48 h | Symptom (1); Pain (9); QoL (1) | 0–4 | 0–100 in which 100 means no Knee problem | English | Arabic (Saudi) |
| OKS (Bodor et al. 2020) [34] | TKA | Self-report | 7–10 days | Arabic (Saudi) | ||||
| OAQoL (Al-Ajmi and Al-Ghamdi 2021) [32] | Osteoarthritis | Self-report | English | Arabic (Saudi) | ||||
| Kujala score (Haddad et al., 2021) [41] | Patellofemoral pain syndrome | Self-report | 2 Weeks | The severity of symptoms (13 factors) | 0–10 | 0–100 in which 100 means good Knee function | English | Arabic (Jordan) |
| ACL-RSI (Alzhrani et al., 2022) [26] | ACL Reconstruction | Self-report | <1–month | Emotions; Confidence; Risk evaluation; | 1–100 | English | Arabic (Saudi) | |
| TAS (Alzhrani et al., 2022) [27] | ACL Reconstruction | Self-report | <1–month | Sedentary jobs to heavy manual (1–5); Recreational to competitive sports (6–9); Elite sports (10 | Varying | 0–100 in which 100 means good Knee function | English | Arabic (Saudi) |
| KOOS-PF-F (Alzhrani et al., 2022) [35] | Patellofemoral pain syndrome | Self-report | 48 h | Symptom (1); Pain (9); QoL (1) | 0–4 | 0–100 in which 100 means no Knee problem | English | Arabic (Saudi) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ateef, M.; Alqahtani, M.; Alzhrani, M.; Alkathiry, A.A.; Alanazi, A.; Alshewaier, S.A. A Systematic Review of Psychometric Properties of Knee-Related Outcome Measures Translated, Cross-Culturally Adapted, and Validated in Arabic Language. Healthcare 2022, 10, 1631. https://doi.org/10.3390/healthcare10091631
Ateef M, Alqahtani M, Alzhrani M, Alkathiry AA, Alanazi A, Alshewaier SA. A Systematic Review of Psychometric Properties of Knee-Related Outcome Measures Translated, Cross-Culturally Adapted, and Validated in Arabic Language. Healthcare. 2022; 10(9):1631. https://doi.org/10.3390/healthcare10091631
Chicago/Turabian StyleAteef, Mahamed, Mazen Alqahtani, Msaad Alzhrani, Abdulaziz A. Alkathiry, Ahmad Alanazi, and Shady Abdullah Alshewaier. 2022. "A Systematic Review of Psychometric Properties of Knee-Related Outcome Measures Translated, Cross-Culturally Adapted, and Validated in Arabic Language" Healthcare 10, no. 9: 1631. https://doi.org/10.3390/healthcare10091631
APA StyleAteef, M., Alqahtani, M., Alzhrani, M., Alkathiry, A. A., Alanazi, A., & Alshewaier, S. A. (2022). A Systematic Review of Psychometric Properties of Knee-Related Outcome Measures Translated, Cross-Culturally Adapted, and Validated in Arabic Language. Healthcare, 10(9), 1631. https://doi.org/10.3390/healthcare10091631