
Trends and Geographic Variabilities in Benzodiazepines Prescription in Primary Care to Older Adults: A 3-Year Population-Based Ecological Study in Portugal

 ,
,  , , ,
, , ,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Study Population
2.2. Benzodiazepines Studied
2.3. Data Source
2.4. Statistical Analysis
3. Results
3.1. Study Population
3.2. Total Benzodiazepine Prescription Share (%)
3.2.1. Benzodiazepine Prescription by Gender
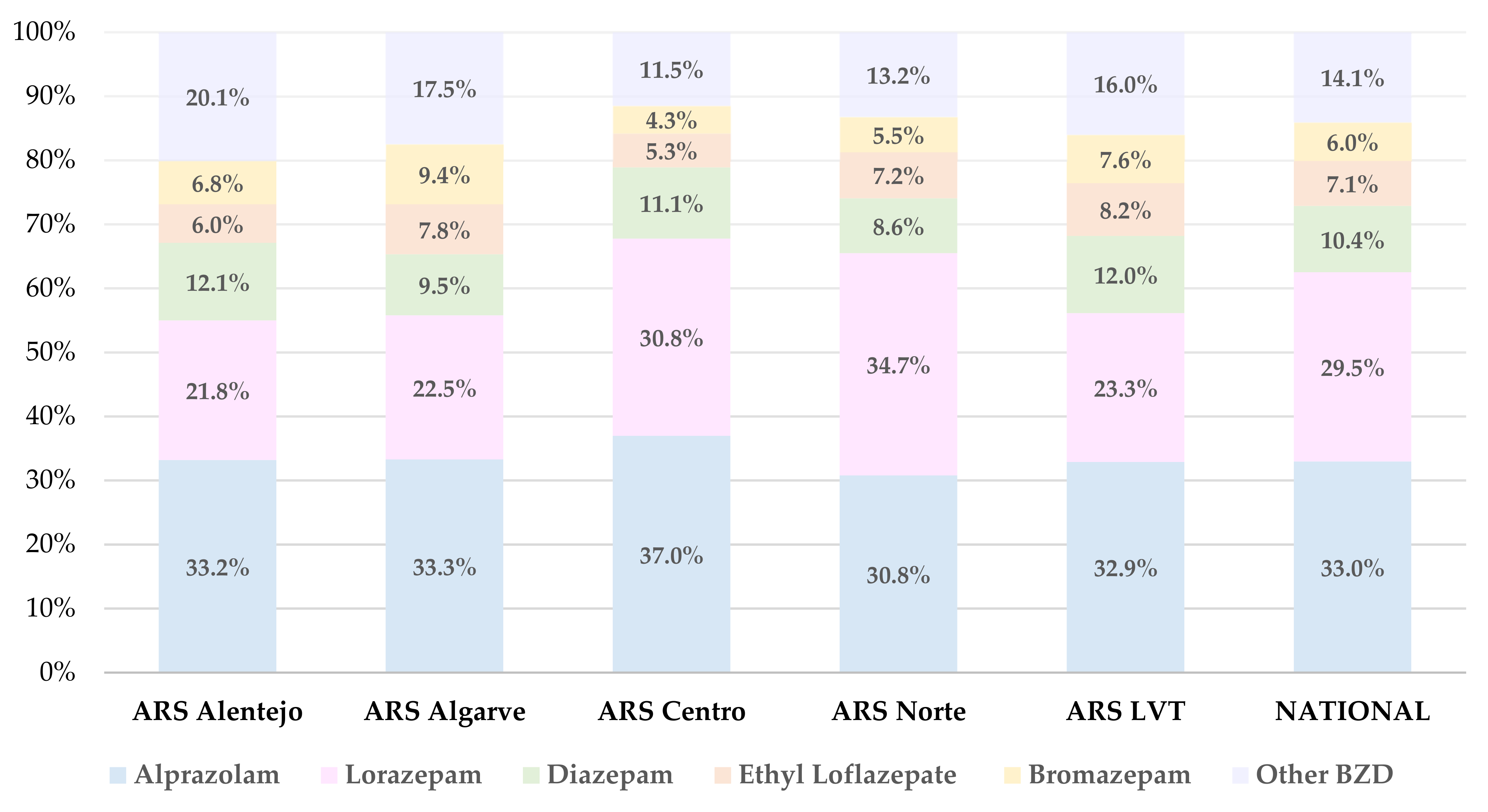
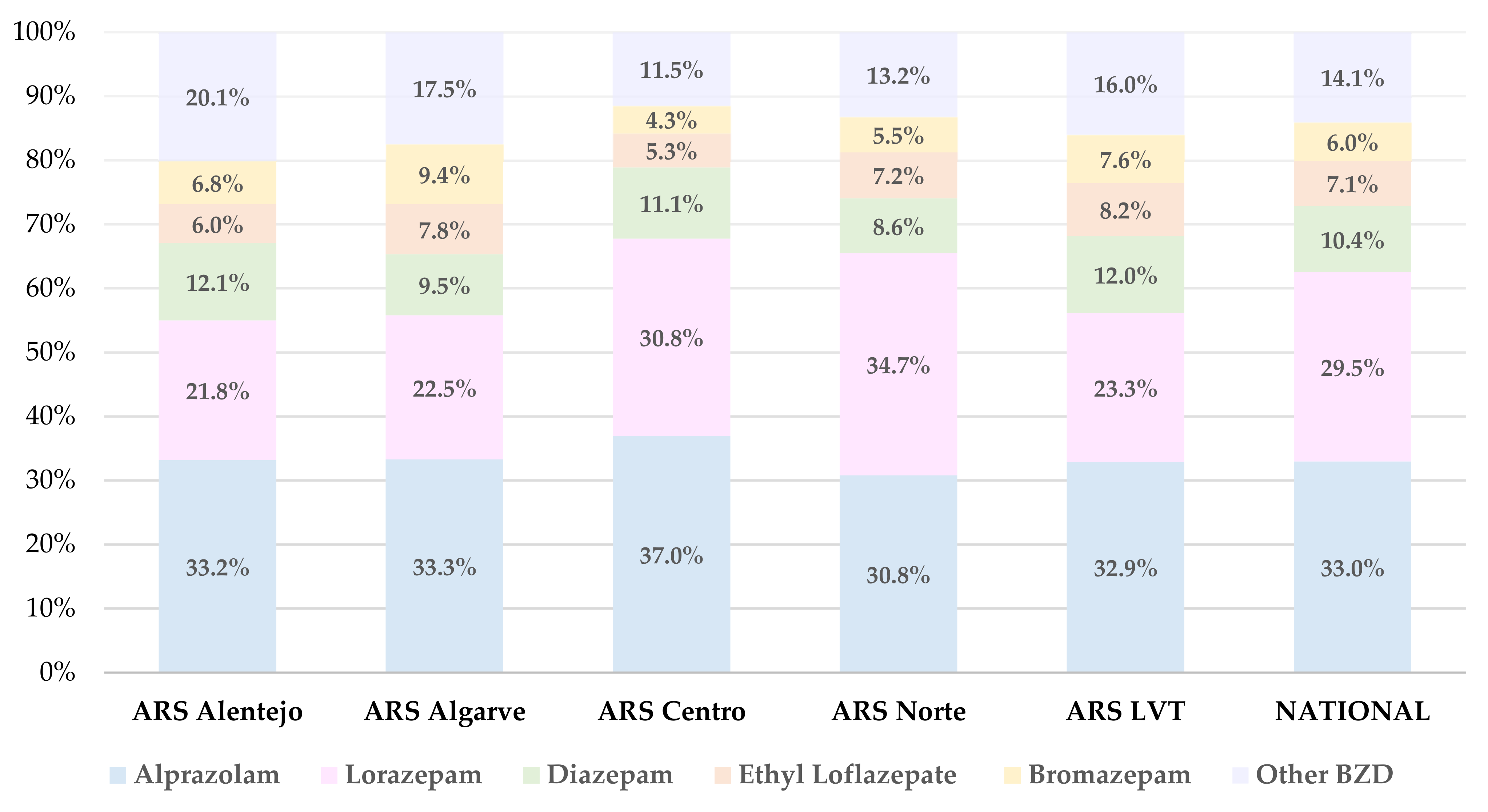
3.2.2. Analysis of Most Prescribed Benzodiazepines Drugs
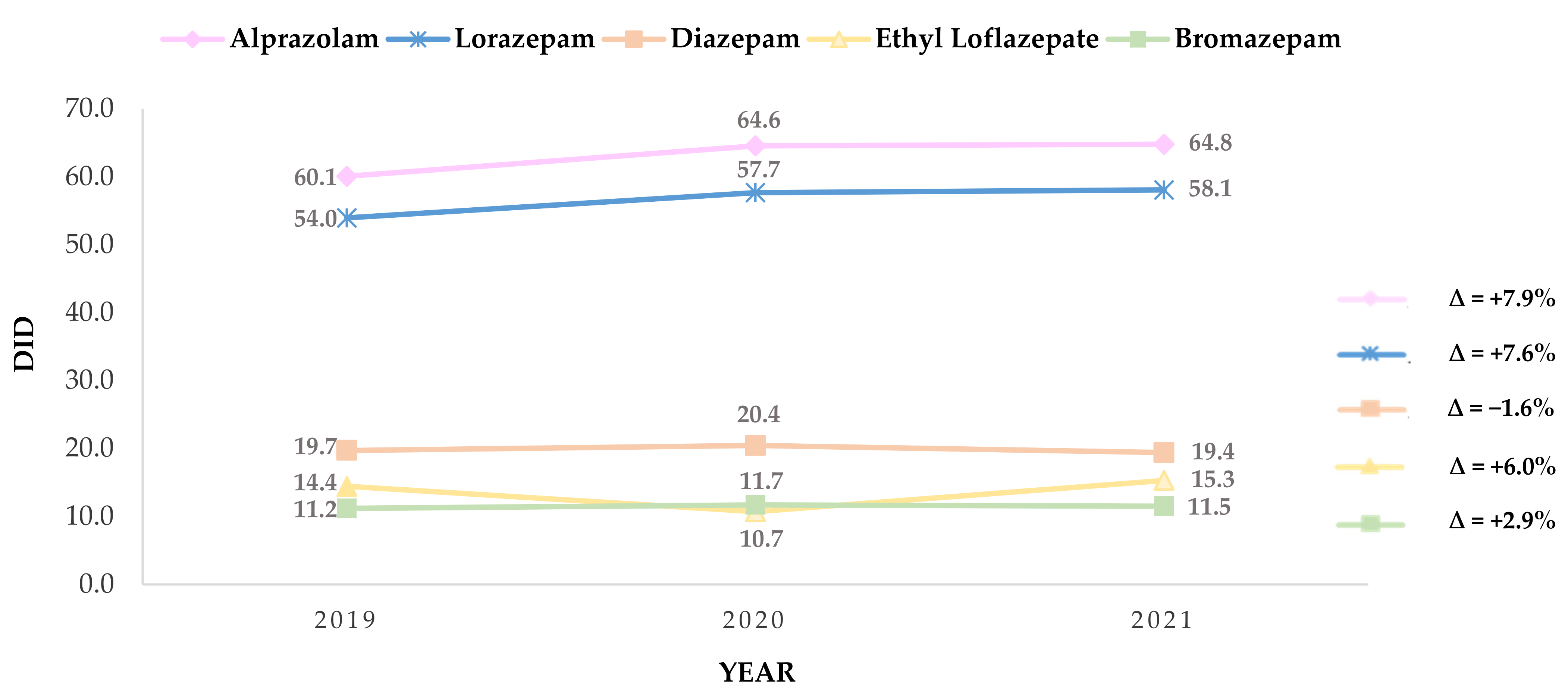
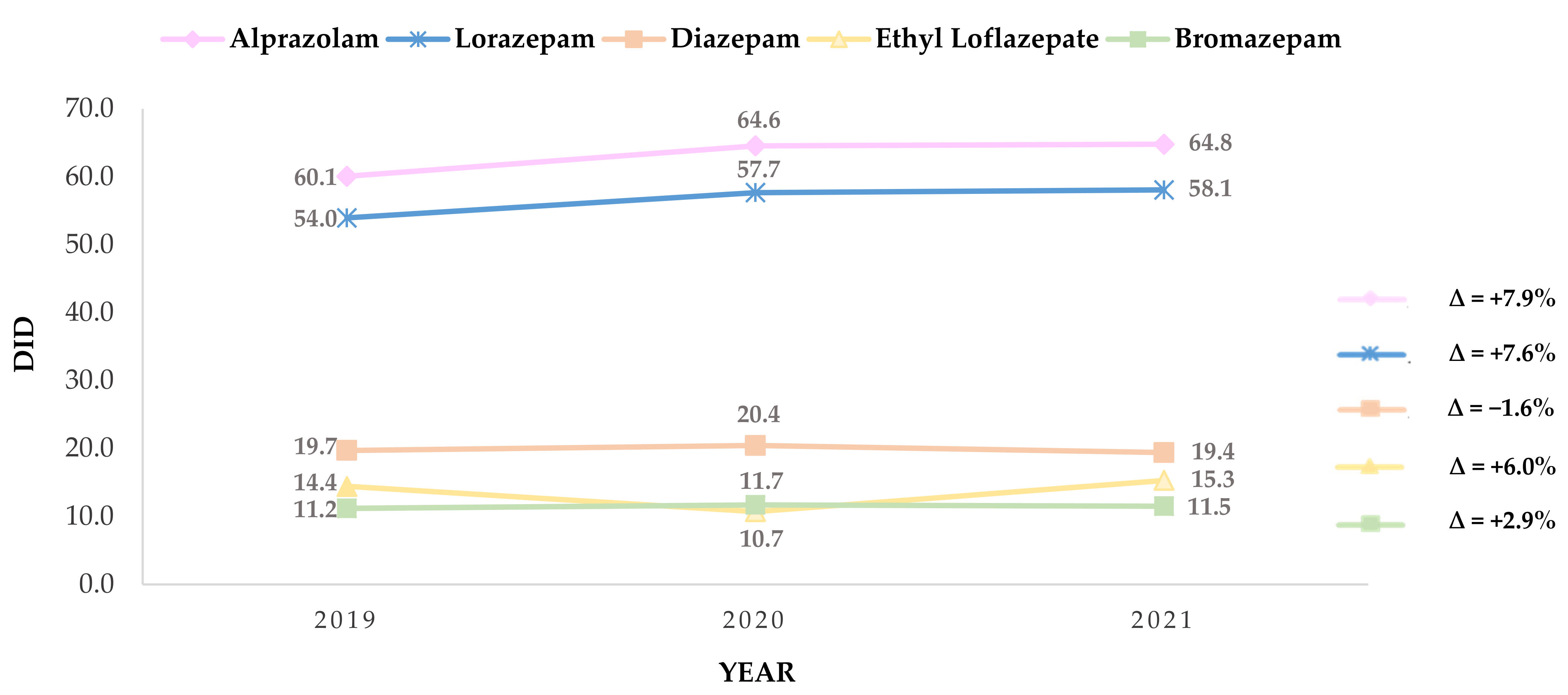
3.3. Trends and Change in the Prescription Rate of Benzodiazepines
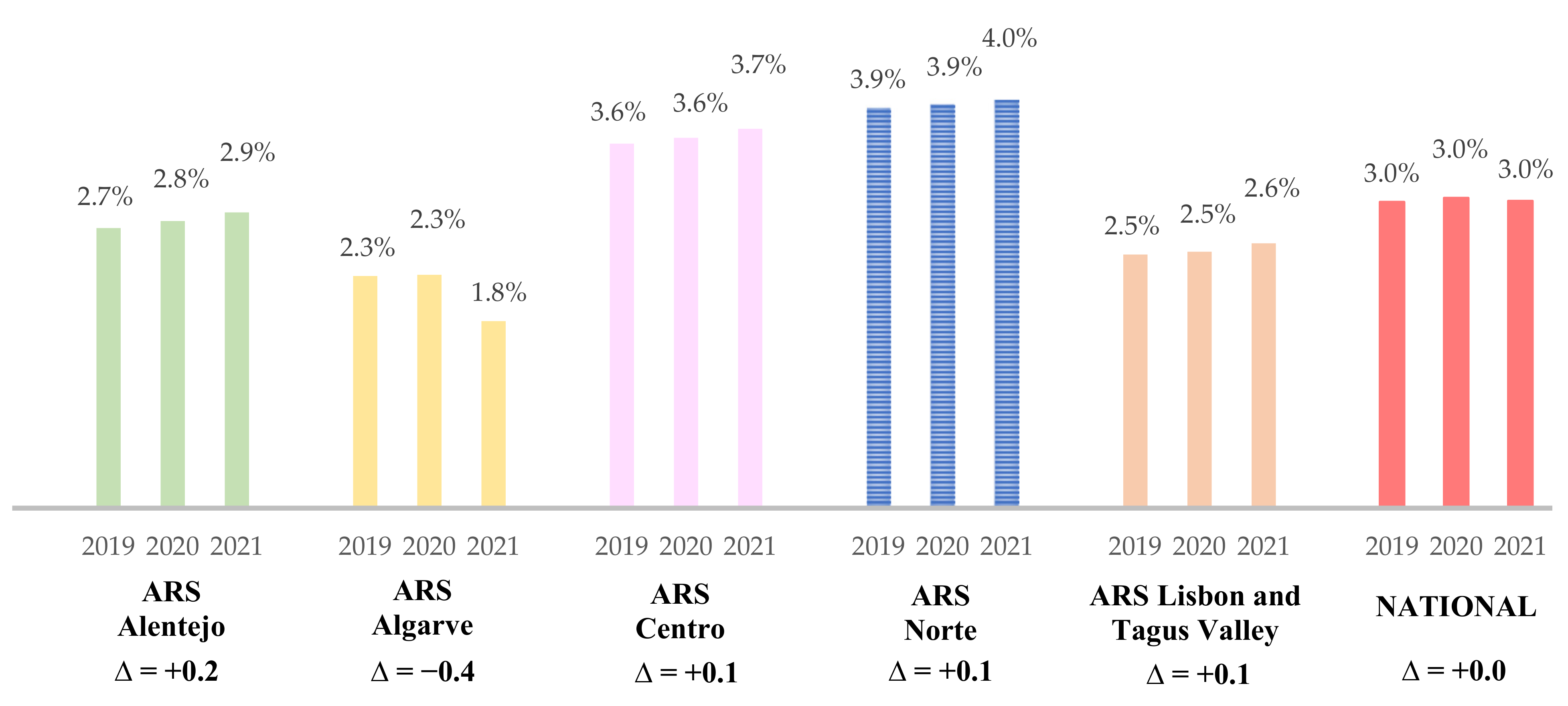
3.4. Geographic Variation in DID Benzodiazepine Prescription to Older Adults
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Gerlach, L.B.; Wiechers, I.R.; Maust, D.T. Prescription Benzodiazepine Use among Older Adults: A Critical Review. Harv. Rev. Psychiatry 2018, 26, 264–273. [Google Scholar] [CrossRef] [PubMed]
- Ng, B.J.; le Couteur, D.G.; Hilmer, S.N. Deprescribing Benzodiazepines in Older Patients: Impact of Interventions Targeting Physicians, Pharmacists, and Patients. Drugs Aging 2018, 35, 493–521. [Google Scholar] [CrossRef] [PubMed]
- Gould, R.L.; Coulson, M.C.; Patel, N.; Highton-Williamson, E.; Howard, R.J. Interventions for Reducing Benzodiazepine Use in Older People: Meta-Analysis of Randomised Controlled Trials. Br. J. Psychiatry 2014, 204, 98–107. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Direção-Geral da Saúde. Tratamento Sintomático Da Ansiedade e Insónia Com Benzodiazepinas e Fármacos Análogos. Anamnesis 2015, 24, 15. [Google Scholar]
- Reeve, E.; Ong, M.; Wu, A.; Jansen, J.; Petrovic, M.; Gnjidic, D. A Systematic Review of Interventions to Deprescribe Benzodiazepines and Other Hypnotics among Older People. Eur. J. Clin. Pharmacol. 2017, 73, 927–935. [Google Scholar] [CrossRef]
- Cumming, R.G.; le Couteur, D.G. Benzodiazepines and Risk of Hip Fractures in Older People: A Review of the Evidence. CNS Drugs 2003, 17, 825–837. [Google Scholar] [CrossRef]
- Renom-Guiteras, A.; Meyer, G.; Thürmann, P.A. The EU(7)-PIM List: A List of Potentially Inappropriate Medications for Older People Consented by Experts from Seven European Countries. Eur. J. Clin. Pharmacol. 2015, 71, 861–875. [Google Scholar] [CrossRef] [Green Version]
- Rodrigues, D.A.; Herdeiro, M.T.; Thurmann, P.A.; Figueiras, A.; Coutinho, P.; Roque, F. Operationalisation for Portugal of the EU(7)-PIM List for Identification of Potentially Inappropriate Medicines in Older Adults. Acta Med. Port. 2020, 33, 194–200. [Google Scholar] [CrossRef]
- Fick, D.M.; Semla, T.P.; Steinman, M.; Beizer, J.; Brandt, N.; Dombrowski, R.; DuBeau, C.E.; Pezzullo, L.; Epplin, J.J.; Flanagan, N.; et al. American Geriatrics Society 2019 Updated AGS Beers Criteria® for Potentially Inappropriate Medication Use in Older Adults. J. Am. Geriatr. Soc. 2019, 67, 674–694. [Google Scholar] [CrossRef]
- Mahony, D.O.; Sullivan, D.O.; Byrne, S.; O’Connor, M.N.; Ryan, C.; Gallagher, P. STOPP/START Criteria for Potentially Inappropriate Prescribing in Older People: Version 2. Age Ageing 2015, 44, 213–218. [Google Scholar] [CrossRef] [Green Version]
- OECD/European Union. Health at a Glance: Europe 2020: State of Health in the EU Cycle; OECD Publishing: Paris, France, 2020. [Google Scholar] [CrossRef]
- Direção-Geral da Saúde. Programa Nacional Para a Saúde Mental; Sistema Nacional de Saúde (SNS): Lisbon, Portugal, 2017. [Google Scholar]
- Administração Central do Sistema de Saúde. Protocolo de Desabituação Do Uso Crónico de Benzodiazepinas; Circular Informativa N. 8/2016/DPS/ACSS 2016; Administração Central do Sistema de Saúde: Lisbon, Portugal, 2016. [Google Scholar]
- Plácido, A.I.; Herdeiro, M.T.; Simões, J.L.; Amaral, O.; Figueiras, A.; Roque, F. Voices of Polymedicated Older Patients: A Focus Group Approach. Int. J. Environ. Res. Public Health 2020, 17, 6443. [Google Scholar] [CrossRef]
- Nunes, A.M.; Ferreira, D.C. Reforms in the Portuguese Health Care Sector: Challenges and Proposals. Int. J. Health Plan. Manag. 2019, 34, e21–e33. [Google Scholar] [CrossRef] [Green Version]
- Tavares, A.I.; Marques, I. Multi-Layer Health Insurance Coverage, Medical Services Use and Health in a Universal National Health System, the Case of Portugal. Eur. J. Health Econ. 2021, 22, 141–153. [Google Scholar] [CrossRef]
- Direção de Informação e Planeamento Estratégico. Infarmed Análise de Utilização de Benzodiazepinas e Análogos; Versão 1.2 (2017/06/02); Direção de Informação e Planeamento Estratégico (Infarmed): Lisbon, Portugal, 2017. [Google Scholar]
- Maree, R.D.; Marcum, Z.A.; Saghafi, E.; Weiner, D.K.; Karp, J.F. A Systematic Review of Opioid and Benzodiazepine Misuse in Older Adults. Am. J. Geriatr. Psychiatry 2016, 24, 949–963. [Google Scholar] [CrossRef] [Green Version]
- Serviços Partilhados do Ministério da Saúde (SPMS) System of Information and Monitoring of the Portuguese National Health System (SIM@SNS). Available online: https://bicsp.min-saude.pt/pt/investigacao/Paginas/medicamentoprescritor_publico.aspx?isdlg=1 (accessed on 12 November 2021).
- Infarmed–Autoridade Nacional do Medicamento e Produtos de Saúde, I.P. INFOMED. Available online: https://extranet.infarmed.pt/INFOMED-fo/ (accessed on 30 September 2021).
- Instituto Nacional de Estatística População Residente (N.o) Por Local de Residência, Sexo e Grupo Etário. Available online: https://www.ine.pt/xportal/xmain?xpid=INE&xpgid=ine_main (accessed on 4 March 2022).
- World Health Organization ATC/DDD Toolkit. Available online: https://www.who.int/tools/atc-ddd-toolkit (accessed on 5 March 2022).
- Estrela, M.; Silva, T.M.; Gomes, E.R.; Piñeiro, M.; Figueiras, A.; Roque, F.; Herdeiro, M.T. Prescription of Anxiolytics, Sedatives, Hypnotics and Antidepressants in Outpatient, Universal Care during the COVID-19 Pandemic in Portugal: A Nationwide, Interrupted Time-Series Approach. J. Epidemiol. Community Health 2022, 76, 1–6. [Google Scholar] [CrossRef]
- Andrade, G.; do Couto, F.S.; Câmara Pestana, L. Recommendations about the Use of Psychotropic Medications during the COVID-19 Pandemic. Acta Med. Port. 2020, 33, 693–702. [Google Scholar] [CrossRef]
- Luta, X.; Bagnoud, C.; Lambiris, M.; Decollogny, A.; Eggli, Y.; le Pogam, M.A.; Marques-Vidal, P.; Marti, J. Patterns of Benzodiazepine Prescription among Older Adults in Switzerland: A Cross-Sectional Analysis of Claims Data. BMJ Open 2020, 10, e031156. [Google Scholar] [CrossRef] [Green Version]
- Carr, M.J.; Steeg, S.; Webb, R.T.; Kapur, N.; Chew-Graham, C.A.; Abel, K.M.; Hope, H.; Pierce, M.; Ashcroft, D.M. Effects of the COVID-19 Pandemic on Primary Care-Recorded Mental Illness and Self-Harm Episodes in the UK: A Population-Based Cohort Study. Lancet Public Health 2021, 6, E124–E135. [Google Scholar] [CrossRef]
- Direção Geral de Saúde (DGS). Programas de Saúde Prioritários de Saúde 2020; Sistema Nacional de Saúde (SNS): Lisbon, Portugal, 2020. [Google Scholar]
- Organisation for Economic Co-operation and Development. Health at a Glance 2021: OECD Indicators; OECD: Paris, France, 2021. [Google Scholar]
- De Dios, C.; Fernandes, B.S.; Whalen, K.; Bandewar, S.; Suchting, R.; Weaver, M.F.; Selvaraj, S. Prescription Fill Patterns for Benzodiazepine and Opioid Drugs during the COVID-19 Pandemic in the United States. Drug Alcohol Depend. 2021, 229, 109176. [Google Scholar] [CrossRef]
- Instituto Nacional de Estatística Estatísticas Da Saúde: 2020. Available online: https://www.ine.pt/xurl/pub/436989156 (accessed on 26 April 2022).
- International Narcotics Control Board; United Nations. Report of the International Narcotics Control Board for 2021; International Narcotics Control Board: Vienna, Austria, 2022; ISSN 0257-3717. [Google Scholar]
- World Health Organization Collaborating Centre for Drug Statistics Methodology Anatomical Therapeutic Chemical (ATC) Classification Index. Available online: https://www.whocc.no/atc_ddd_index/ (accessed on 21 March 2022).
- Teixeira, I.; Furtado, C. Benzodiazepine’s Utilization in Continental Portugal: Medicine and Health Products Observatory/Medicine and Health Products Economics Department Institute of Pharmacy and Medicines. In Proceedings of the 22nd International Conference on Pharmacoepidemiology & Therapeutic Risk Management, Lisbon, Portugal, 24–27 August 2006. [Google Scholar]
- OECD OECD.Stat. Available online: https://stats.oecd.org/ (accessed on 13 April 2022).
- Sanabria, E.; Cuenca, R.E.; Esteso, M.Á.; Maldonado, M. Benzodiazepines: Their Use Either as Essential Medicines or as Toxics Substances. Toxics 2021, 9, 25. [Google Scholar] [CrossRef]
- Furtado, C.; Teixeira, I. Utilização de benzodiazepinas em Portugal continental (1999–2003) [Benzodiazepine’s utilization in continental Portugal (1999–2003)]. Acta Med. Port. 2006, 19, 239–246. [Google Scholar] [PubMed]
- de Sousa, R.D.; Rodrigues, A.M.; Gregório, M.J.; Branco, J.D.C.; Gouveia, M.J.; Canhão, H.; Dias, S.S. Anxiety and Depression in the Portuguese Older Adults: Prevalence and Associated Factors. Front. Med. 2017, 4, 196. [Google Scholar] [CrossRef] [Green Version]
- Estrela, M.; Herdeiro, M.T.; Ferreira, P.L.; Roque, F. The Use of Antidepressants, Anxiolytics, Sedatives and Hypnotics in Europe: Focusing on Mental Health Care in Portugal and Prescribing in Older Patients. Int. J. Environ. Res. Public Health 2020, 17, 8612. [Google Scholar] [CrossRef]
- Instituto Nacional de Estatística de Portugal; Instituto Nacional de Saúde Doutor Ricardo Jorge. Inquérito Nacional de Saúde; Instituto Nacional de Estatística de Portugal: Lisbon, Portugal, 2009. [Google Scholar]
- Programa Nacional para a Saúde Mental. PORTUGAL: Saúde Mental Em Números-2015; Direção-Geral da Saúde: Lisboa, Portugal, 2016. [Google Scholar]
- International Narcotics Control Board; United Nations. Report of the International Narcotics Control Board for 2004; International Narcotics Control Board: New York, NY, USA, 2005. [Google Scholar]
- International Narcotics Control Board; United Nations. Report of the International Narcotics Control Board for 2011; International Narcotics Control Board: New York, NY, USA, 2012. [Google Scholar]
- Antunes, A.; Frasquilho, D.; Azeredo-Lopes, S.; Neto, D.; Silva, M.; Cardoso, G.; Caldas-de-Almeida, J.M. Disability and Common Mental Disorders: Results from the World Mental Health Survey Initiative Portugal. Eur. Psychiatry 2018, 49, 56–61. [Google Scholar] [CrossRef]
- Paiva, D.; Silva, S.; Severo, M.; Moura-Ferreira, P.; Lunet, N.; Azevedo, A. Limited Health Literacy in Portugal Assessed with the Newest Vital Sign Prevalência de Literacia Em Saúde Inadequada Em Portugal Medida Com o Newest Vital Sign. Acta Med. Port. 2017, 30, 861–869. [Google Scholar] [CrossRef] [Green Version]
- Medical Doctors per 1000 Inhabitants by Place of Residence. [Internet]. 2021. Available online: https://www.ine.pt/xportal/xmain?xpid=INE&xpgid=ine_indicadores&contecto=pi&indOcorrCod=0008356&selTab=tab0&xlang=en (accessed on 15 July 2022).
- Sistema Nacional de Saúde (SNS). Relatório Anual Sobre o Acesso a Cuidados de Saúde Nos Estabelecimentos Do SNS e Entidades Convencionadas; Sistema Nacional de Saúde (SNS): Lisbon, Portugal, 2019. [Google Scholar]
- Social Security Pensions by Place of Residence and Type of Pension. [Internet]. 2021. Available online: https://www.ine.pt/xportal/xmain?xpid=INE&xpgid=ine_indicadores&indOcorrCod=0010277&contexto=bd&selTab=tab2&xlang=pt (accessed on 15 July 2022).
- Plácido, A.I.; Herdeiro, M.T.; Simões, J.L.; Amaral, O.; Figueiras, A.; Roque, F. Health Professionals Perception and Beliefs about Drug- Related Problems on Polymedicated Older Adults- a Focus Group Study. BMC Geriatr. 2021, 21, 27. [Google Scholar] [CrossRef]
- Ni, X.F.; Yang, C.S.; Bai, Y.M.; Hu, Z.X.; Zhang, L.L. Drug-Related Problems of Patients in Primary Health Care Institutions: A Systematic Review. Front. Pharmacol. 2021, 12, 698907. [Google Scholar] [CrossRef]
- Eurostat Eurostat Data Browser: Persons Reporting a Chronic Disease, by Disease, Sex, Age and Educational Attainment Level. Available online: https://ec.europa.eu/eurostat/databrowser/view/HLTH_EHIS_CD1E__custom_2494696/default/table?lang=en (accessed on 12 April 2022).
- McHugh, R.K.; Geyer, R.B.; Chase, A.R.; Griffin, M.L.; Bogunovic, O.; Weiss, R.D. Sex Differences in Benzodiazepine Misuse among Adults with Substance Use Disorders. Addict. Behav. 2021, 112, 106608. [Google Scholar] [CrossRef]
- Unsal, A.; Tozun, M.; Ayranci, U. Prevalence of Depression among Postmenopausal Women and Related Characteristics. Climacteric 2011, 14, 33–36. [Google Scholar] [CrossRef] [PubMed]
- European Monitoring Centre for Drugs and Drug Addiction. The Misuse of Benzodiazepines among High-Risk Opioid Users in Europe. Available online: www.emcdda.europa.eu/publications/manuals/tdi- (accessed on 17 July 2022).
- Vilaça, A.; Vieira, A.; Fernandes, A.; Ribeiro, D.; Esteves, I. Characterisation of Benzodiazepine Use in an Older Population Registered in Family Health Units in the Region of Minho, Portugal. Geriatrics 2019, 4, 27. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Delaš Aždajić, M.; Likić, R.; Gućanac, M.; Franceschi, N.; Tolušić Levak, M.; Štajduhar, A.; Šitum, M.; Štimac Grbić, D. Prescription Pattern and Prevalence of Benzodiazepine Use among Elderly Patients. Asian J. Psychiatry 2021, 55, 102514. [Google Scholar] [CrossRef]
- World Health Organization. Integrated Care for Older People Guidelines on Community-Level Interventions to Manage Declines in Intrinsic Capacity; World Health Organization: Geneva, Switzerland, 2017. [Google Scholar]


{kind=link}
{kind=link}
{kind=link}
| Alentejo | Algarve | Norte | Centro | LVT | National | |
|---|---|---|---|---|---|---|
| F/M | 3.0 | 2.6 | 2.4 | 2.7 | 2.8 | 2.7 |
| Benzodiazepine | 2019 (DID) | 2020 (DID) | 2021 (DID) | ∆ 2021–2019 (DID) | ∆ 2021–2019 (%) |
|---|---|---|---|---|---|
| ARSN | |||||
| Alprazolam (N05BA12) | 63.1 | 72.0 | 71.9 | 8.9 | 14.1% |
| Lorazepam (N05BA06) | 71.6 | 80.9 | 80.8 | 9.2 | 12.8% |
| Diazepam (N05BA01) | 18.1 | 20.2 | 19.4 | 1.3 | 7.2% |
| Ethyl loflazepate (N05BA18) | 16.9 | 13.4 | 18.2 | 1.3 | 7.4% |
| Bromazepam (N05BA08) | 11.6 | 12.8 | 12.4 | 0.8 | 6.8% |
| ARSC | |||||
| Alprazolam (N05BA12) | 78.8 | 79.5 | 75.4 | −3.4 | −4.4% |
| Lorazepam (N05BA06) | 65.1 | 65.9 | 63.6 | −1.5 | −2.2% |
| Diazepam (N05BA01) | 24.6 | 24.2 | 21.7 | −2.9 | −11.6% |
| Ethyl loflazepate (N05BA18) | 12.9 | 8.8 | 12.0 | −0.9 | 7.0% |
| Bromazepam (N05BA08) | 9.3 | 9.2 | 8.6 | −0.7 | −7.2% |
| ARSALE | |||||
| Alprazolam (N05BA12) | 52.9 | 55.8 | 54.7 | 1.7 | 3.3% |
| Lorazepam (N05BA06) | 34.2 | 36.9 | 36.2 | 2.1 | 6.0% |
| Diazepam (N05BA01) | 20.4 | 20.8 | 18.5 | −1.9 | −9.3% |
| Ethyl loflazepate (N05BA18) | 10.7 | 7.3 | 11.4 | 0.7 | 6.6% |
| Bromazepam (N05BA08) | 11.0 | 11.5 | 10.9 | −0.1 | −1.2% |
| ARSALG | |||||
| Alprazolam (N05BA12) | 37.5 | 40.3 | 36.8 | −0.7 | −1.8% |
| Lorazepam (N05BA06) | 25.6 | 26.5 | 1.5 | −0.3 | −1.0% |
| Diazepam (N05BA01) | 11.4 | 11.4 | 10.1 | −1.2 | −10.9% |
| Ethyl loflazepate (N05BA18) | 9.9 | 7.0 | 9.8 | −0.1 | −0.8% |
| Bromazepam (N05BA08) | 10.7 | 11.4 | 10.3 | −0.4 | −4.0% |
| ARSLVT | |||||
| Alprazolam (N05BA12) | 50.4 | 53.1 | 56.3 | 6.0 | 11.9% |
| Lorazepam (N05BA06) | 36.1 | 37.6 | 39.4 | 3.2 | 8.9% |
| Diazepam (N05BA01) | 19.6 | 19.6 | 19.4 | −0.2 | −0.8% |
| Ethyl loflazepate (N05BA18) | 13.9 | 10.2 | 15.9 | 2.0 | 14.2% |
| Bromazepam (N05BA08) | 11.9 | 12.2 | 12.7 | 0.8 | 6.8% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tavares, A.B.; Placido, A.I.; Rodrigues, D.A.; Morgado, M.; Figueiras, A.; Herdeiro, M.T.; Roque, F. Trends and Geographic Variabilities in Benzodiazepines Prescription in Primary Care to Older Adults: A 3-Year Population-Based Ecological Study in Portugal. Healthcare 2022, 10, 1342. https://doi.org/10.3390/healthcare10071342
Tavares AB, Placido AI, Rodrigues DA, Morgado M, Figueiras A, Herdeiro MT, Roque F. Trends and Geographic Variabilities in Benzodiazepines Prescription in Primary Care to Older Adults: A 3-Year Population-Based Ecological Study in Portugal. Healthcare. 2022; 10(7):1342. https://doi.org/10.3390/healthcare10071342
Chicago/Turabian StyleTavares, Ana Bárbara, Ana Isabel Placido, Daniela Almeida Rodrigues, Manuel Morgado, Adolfo Figueiras, Maria Teresa Herdeiro, and Fátima Roque. 2022. "Trends and Geographic Variabilities in Benzodiazepines Prescription in Primary Care to Older Adults: A 3-Year Population-Based Ecological Study in Portugal" Healthcare 10, no. 7: 1342. https://doi.org/10.3390/healthcare10071342
APA StyleTavares, A. B., Placido, A. I., Rodrigues, D. A., Morgado, M., Figueiras, A., Herdeiro, M. T., & Roque, F. (2022). Trends and Geographic Variabilities in Benzodiazepines Prescription in Primary Care to Older Adults: A 3-Year Population-Based Ecological Study in Portugal. Healthcare, 10(7), 1342. https://doi.org/10.3390/healthcare10071342