
Evaluation of Ibuprofen Use on the Immune System Indicators and Force in Disabled Paralympic Powerlifters of Different Sport Levels

 ,
, 
 , , , ,
, , , ,  ,
,  ,
,  ,
,  , ,
, ,  ,
,  ,
,  ,
,  and
and 
Abstract
:1. Introduction
2. Materials and Methods
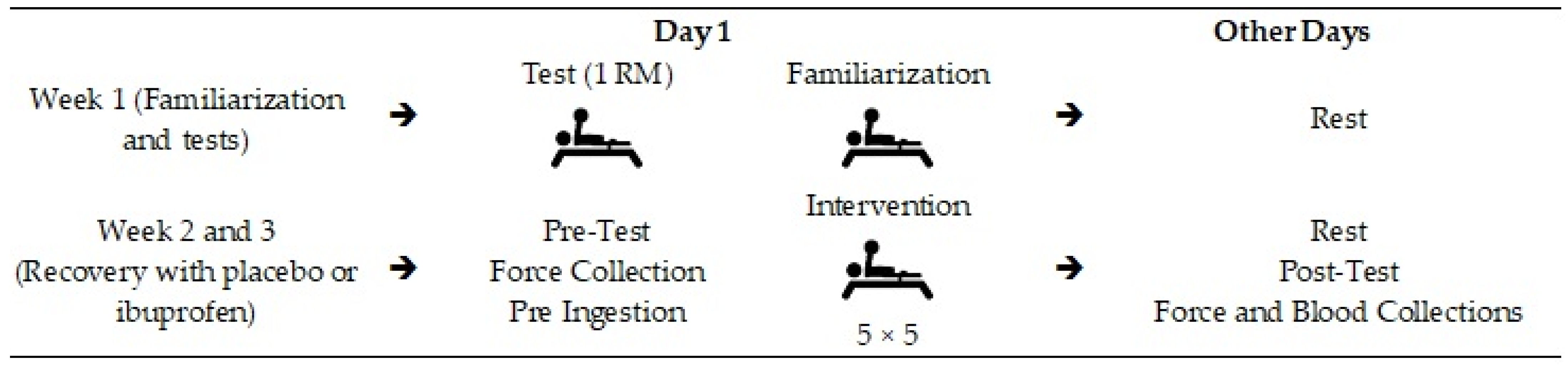
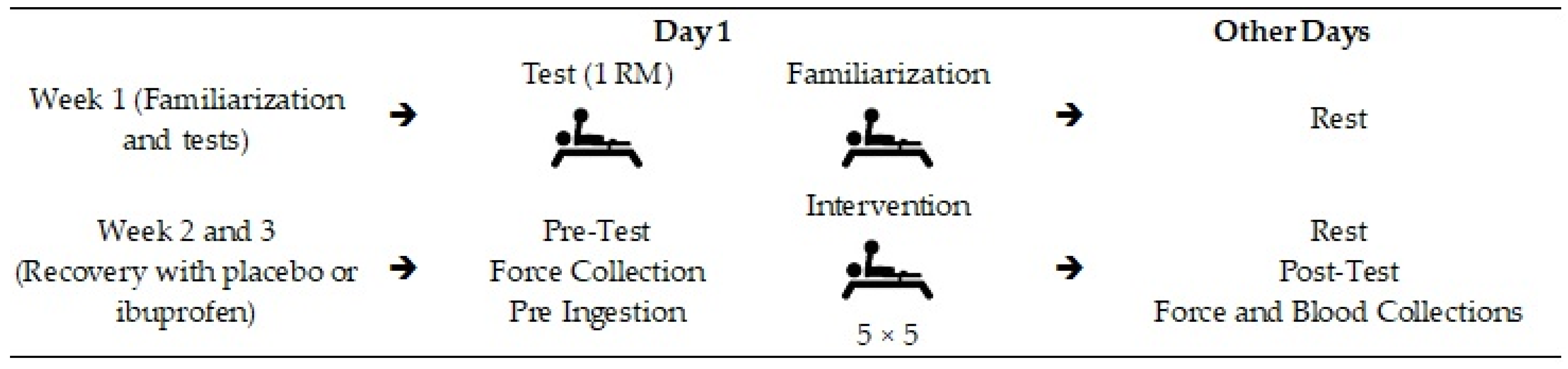
2.1. Study Design
2.2. Sample
2.3. Ethics
2.4. Body Mass Analysis
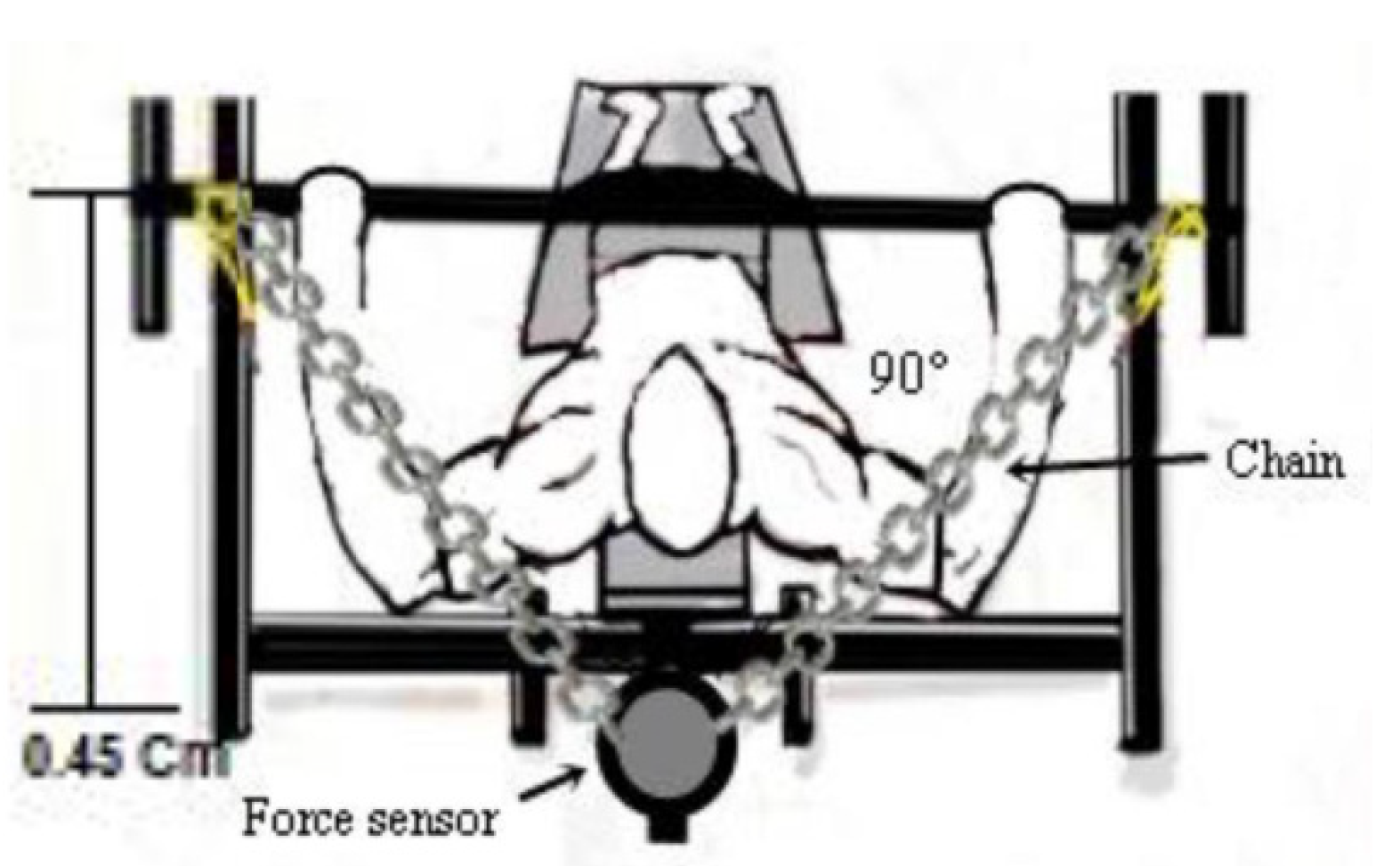
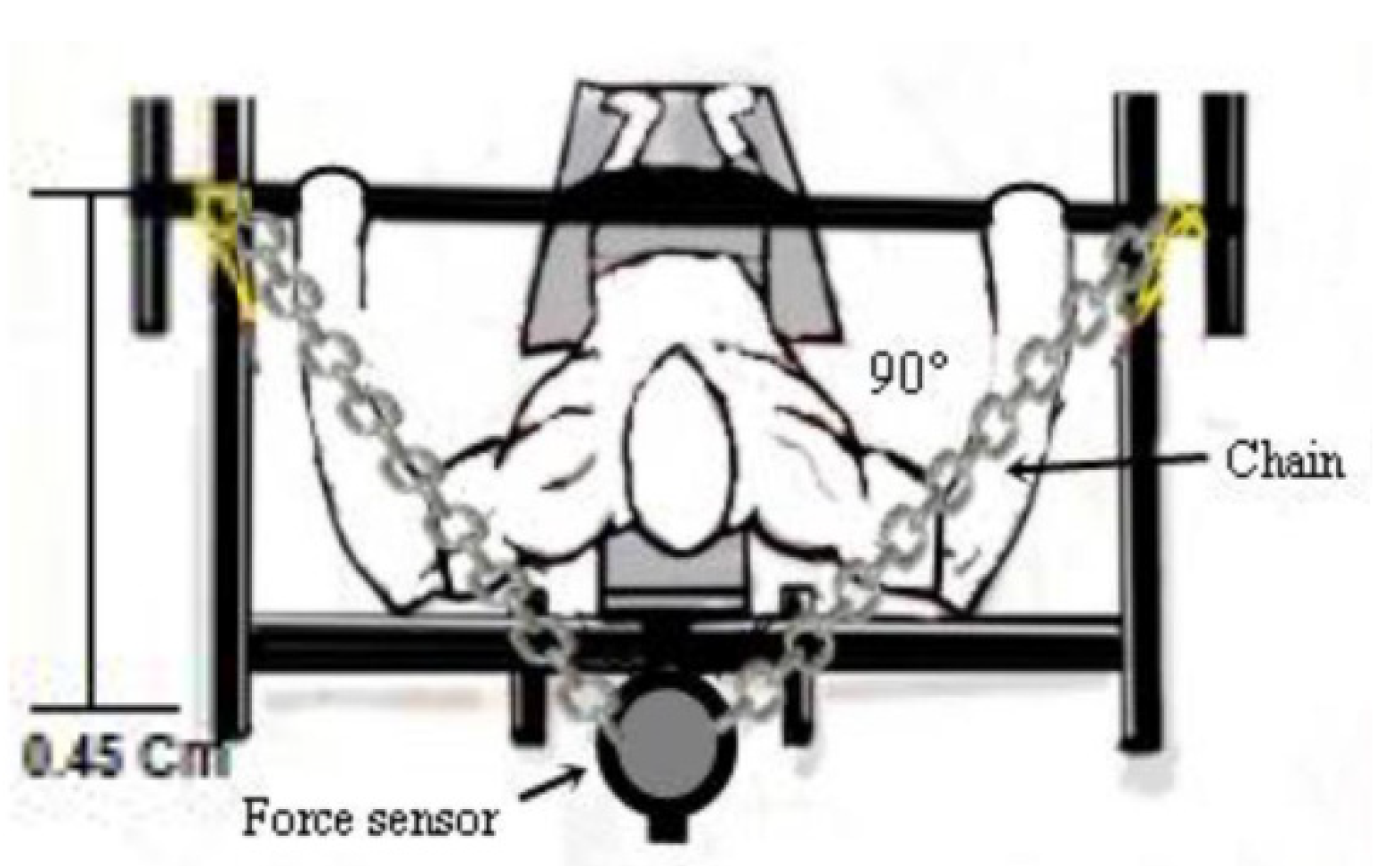
2.5. Maximum Training Load Analysis
2.6. Blood Sample Collection, Blood Cells, Leukocytes Count (HEMOGRAM), and Ammonia
2.7. Post-Workout Recovery Using a Placebo
2.8. Post-Workout Recovery Using Ibuprofen
2.9. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Fraga, G.S.; Aidar, F.J.; Matos, D.G.; Marçal, A.C.; Santos, J.L.; Souza, R.F.; Carneiro, A.L.; Vasconcelos, A.B.; Da Silva-Grigoletto, M.E.; Tillaar, R.V.D.; et al. Effects of Ibuprofen Intake in Muscle Damage, Body Temperature and Muscle Power in Paralympic Powerlifting Athletes. Int. J. Environ. Res. Public Health 2020, 17, 5157. [Google Scholar] [CrossRef]
- Hecksteden, A.; Skorski, S.; Schwindling, S.; Hammes, D.; Pfeiffer, M.; Kellmann, M.; Ferrauti, A.; Meyer, T. Blood-Borne Markers of Fatigue in Competitive Athletes—Results from Simulated Training Camps. PLoS ONE 2016, 11, e0148810. [Google Scholar] [CrossRef] [PubMed]
- Sampaio, C.R.S.F.; Aidar, F.J.; Ferreira, A.R.P.; Santos, J.L.D.; Marçal, A.C.; Matos, D.G.; Souza, R.F.; Moreira, O.C.; Guerra, I.; Fernandes Filho, J.; et al. Can Creatine Supplementation Interfere with Muscle Strength and Fatigue in Brazilian National Level Paralympic Powerlifting? Nutrientes 2020, 12, 2492. [Google Scholar] [CrossRef] [PubMed]
- Bessa, A.L.; Oliveira, V.N.; Agostini, G.G.; Oliveira, R.J.; Oliveira, A.C.; White, G.E.; Wells, G.D.; Teixeira, D.N.; Espindola, F.S. Exercise Intensity and Recovery. J. Strength Cond. Res. 2016, 30, 311–319. [Google Scholar] [CrossRef] [PubMed]
- Nunes-Silva, A.; Bernardes, P.T.T.; Rezende, B.M.; Lopes, F.; Gomes, E.C.; Marques, P.E.; Lima, P.M.A.; Coimbra, C.C.; Menezes, G.B.; Teixeira, M.M.; et al. Treadmill Exercise Induces Neutrophil Recruitment into Muscle Tissue in a Reactive Oxygen Species-Dependent Manner. An Intravital Microscopy Study. PLoS ONE 2014, 9, e96464. [Google Scholar] [CrossRef] [PubMed]
- Gonçalves, C.A.M.; Dantas, P.M.S.; Dos Santos, I.K.; Dantas, M.P.; Da Silva, D.C.P.; Cabral, B.G.D.A.T.; Guerra, R.O.; Júnior, G.B.C. Effect of Acute and Chronic Aerobic Exercise on Immunological Markers: A Systematic Review. Front. Physiol. 2020, 10, 1602. [Google Scholar] [CrossRef]
- Mishra, D.K.; Fridén, J.; Schmitz, M.C.; Lieber, R.L. Anti-inflammatory medication after muscle injury. A treatment resulting in short-term improvement but subsequent loss of muscle function. J. Bone Jt. Surg. Am. 1995, 77, 1510–1519. [Google Scholar] [CrossRef]
- Bondesen, B.A.; Mills, S.T.; Kegley, K.M.; Pavlath, G.K. The COX-2 pathway is essential during early stages of skeletal muscle re-generation. Am. J. Physiol. Cell Physiol. 2004, 56, C475–C483. [Google Scholar] [CrossRef]
- Bondesen, B.A.; Mills, S.T.; Pavlath, G.K. The COX-2 pathway regulates growth of atrophied muscle via multiple mechanisms. Am. J. Physiol. Physiol. 2006, 290, C1651–C1659. [Google Scholar] [CrossRef] [Green Version]
- Varamenti, E.; Nikolovski, Z.; Elgingo, M.I.; Jamurtas, A.Z.; Cardinale, M. Training-induced variations in haematological and bio-chemical variables in adolescent athletes of arab origin throughout an entire athletic season. J. Hum. Kinet. 2018, 64, 123–135. [Google Scholar] [CrossRef] [Green Version]
- Speer, H.; D’Cunha, N.M.; Alexopoulos, N.I.; McKune, A.J.; Naumovski, N. Anthocyanins and Human Health—A Focus on Oxidative Stress, Inflammation and Disease. Antioxidants 2020, 9, 366. [Google Scholar] [CrossRef]
- Aidar, F.J.; Fraga, G.S.; Getirana-Mota, M.; Marçal, A.C.; Santos, J.L.; de Souza, R.F.; Ferreira, A.R.P.; Neves, E.B.; Zanona, A.D.F.; Bulhões-Correia, A.; et al. Effects of Ibuprofen Use on Lymphocyte Count and Oxidative Stress in Elite Paralympic Powerlifting. Biology 2021, 10, 986. [Google Scholar] [CrossRef] [PubMed]
- Santos, W.; Aidar, F.; Matos, D.; Tillaar, R.V.D.; Marçal, A.; Lobo, L.; Marcucci-Barbosa, L.; Machado, S.; Almeida-Neto, P.; Garrido, N.; et al. Physiological and Biochemical Evaluation of Different Types of Recovery in National Level Paralympic Powerlifting. Int. J. Environ. Res. Public Health 2021, 18, 5155. [Google Scholar] [CrossRef] [PubMed]
- International Paralympic Committee (IPC). World Para Powerlifiting. Rules & Regulations. Available online: https://www.paralympic.org/sites/default/files/document/180215210800620_World%2BPara%2BPowerlifting%2BRules%2Band%2BRegulations_Feb%2B2018_0.pdf (accessed on 13 October 2021).
- Resende, M.; Resende, R.V.; Reis, G.; Barros, L.; Bezerra, M.; Matos, D.; Marçal, A.; Almeida-Neto, P.; Cabral, B.; Neiva, H.; et al. The Influence of Warm-Up on Body Temperature and Strength Performance in Brazilian National-Level Paralympic Powerlifting Athletes. Medicina 2020, 56, 538. [Google Scholar] [CrossRef] [PubMed]
- Ball, R.; Weidman, D. Analysis of USA Powerlifting Federation Data From January 1, 2012–June 11, 2016. J. Strength Cond. Res. 2018, 32, 1843–1851. [Google Scholar] [CrossRef]
- Souza, R.F.; Nogueira, A.C.; Ferreira, A.R.P.; Matos, D.G.; Oliveira, L.S.L.; Zanona, A.F.; Aidar, F.J. Analysis of muscle recovery time after acute stretching at peak torque of the hamstring muscles. Med. Dello Sport 2019, 72, 171–180. [Google Scholar] [CrossRef]
- Mendonça, T.P.; Aidar, F.J.; Matos, D.G.; Souza, R.F.; Marçal, A.C.; Almeida-Neto, P.F.; Cabral, B.G.; Garrido, N.D.; Neiva, H.P.; Marinho, D.A.; et al. Force production and muscle activation during partial vs. full range of motion in Paralympic Powerlifting. PLoS ONE 2021, 16, e0257810. [Google Scholar] [CrossRef]
- Teles, L.J.L.; Aidar, F.J.; Matos, D.G.; Marçal, A.C.; Almeida-Neto, P.F.; Neves, E.B.; Moreira, O.C.; Neto, F.R.; Garrido, N.D.; Vilaça-Alves, J.; et al. Static and Dynamic Strength Indicators in Paralympic Power-Lifters with and without Spinal Cord Injury. Int. J. Environ. Res. Public Health 2021, 18, 5907. [Google Scholar] [CrossRef]
- Cayres, S.U.; de Lira, F.S.; Kemper, H.C.G.; Codogno, J.S.; Barbosa, M.F.; Fernandes, R.A. Sport-based physical activity recommendations and modifications in C-reactive protein and arterial thickness. Eur. J. Pediatr. 2018, 177, 551–558. [Google Scholar] [CrossRef] [Green Version]
- Roberts, W.L.; Moulton, L.; Law, T.C.; Farrow, G.; Cooper-Anderson, M.; Savory, J.; Rifai, N. Evaluation of Nine Automated High-Sensitivity C-Reactive Protein Methods: Implications for Clinical and Epidemiological Applications. Part 2. Clin. Chem. 2001, 47, 418–425. [Google Scholar] [CrossRef] [Green Version]
- Prado, E.S.; Neto, J.M.D.R.; De Almeida, R.D.; De Melo, M.G.D.; Cameron, L.-C. Keto analogue and amino acid supplementation affects the ammonaemia response during exercise under ketogenic conditions. Br. J. Nutr. 2011, 105, 1729–1733. [Google Scholar] [CrossRef] [PubMed]
- de Souza, R.F.; de Matos, D.G.; Ferreira, A.R.P.; Chilibeck, P.; Barros, N.D.A.; Oliveira, A.S.; Cercato, L.M.; da Silva, D.S.; Aidar, F.J. Effect of Ibuprofen on Muscle, Hematological and Renal Function, Hydric Balance, Pain, and Performance During Intense Long-Distance Running. J. Strength Cond. Res. 2020, 34, 2076–2083. [Google Scholar] [CrossRef] [PubMed]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences, 2nd ed.; Lawrence Erlbaum Associates: Hillsdale, NJ, USA, 1988; ISBN 978-0-8058-0283-2. [Google Scholar]
- Cohen, J. Statistics a power primer. Psychol. Bull. 1992, 112, 155–159. [Google Scholar] [CrossRef] [PubMed]
- Lakens, D. Calculating and reporting effect sizes to facilitate cumulative science: A practical primer for t-tests and ANOVAs. Front. Psychol. 2013, 4, 863. [Google Scholar] [CrossRef] [Green Version]
- Elshafei, M.; Shihab, E. Towards Detecting Biceps Muscle Fatigue in Gym Activity Using Wearables. Sensors 2021, 21, 759. [Google Scholar] [CrossRef]
- Mushtaq, W.; Hamdani, N.; Noohu, M.M.; Raghavan, S. Effect of Modified Constrain Induced Movement Therapy on Fatigue and Motor Performance in Sub Acute Stroke. J. Stroke Cerebrovasc. Dis. 2020, 29, 105378. [Google Scholar] [CrossRef]
- Kerhervé, H.A.; Stewart, D.G.; McLellan, C.; Lovell, D. Fatigue Indices and Perceived Exertion Highlight Ergometer Specificity for Repeated Sprint Ability Testing. Front. Sports Act. Living 2020, 2, 45. [Google Scholar] [CrossRef]
- Chen, C.-Y.; Chou, W.-Y.; Ko, J.-Y.; Lee, M.S.; Wu, R.-W. Early Recovery of Exercise-Related Muscular Injury by HBOT. BioMed Res. Int. 2019, 2019, 6289380. [Google Scholar] [CrossRef] [Green Version]
- Trafimow, J.H.; Schipplein, O.D.; Novak, G.J.; Andersson, G.B.J. The Effects of Quadriceps Fatigue on the Technique of Lifting. Spine 1993, 18, 364–367. [Google Scholar] [CrossRef]
- Krzysztofik, M.; Zajac, A.; Żmijewski, P.; Wilk, M. Can the Cambered Bar Enhance Acute Performance in the Bench Press Exercise? Front. Physiol. 2020, 11, 577400. [Google Scholar] [CrossRef]
- Reno, A.M.; Green, M.; Killen, L.G.; O’Neal, E.K.; Pritchett, K.; Hanson, Z. Effects of Magnesium Supplementation on Muscle Soreness and Performance. J. Strength Cond. Res. 2020. Epub Ahead. [Google Scholar] [CrossRef] [PubMed]
- Stolk, R.F.; Van Der Pasch, E.; Naumann, F.; Schouwstra, J.; Bressers, S.; Van Herwaarden, A.E.; Gerretsen, J.; Schambergen, R.; Ruth, M.M.; Van Der Hoeven, J.G.; et al. Norepinephrine Dysregulates the Immune Response and Compromises Host Defense during Sepsis. Am. J. Respir. Crit. Care Med. 2020, 202, 830–842. [Google Scholar] [CrossRef] [PubMed]
- Basile, U.; Bruno, C.; Napodano, C.; Vergani, E.; Pocino, K.; Brunetti, A.; Gulli, F.; Santini, S.A.; Mancini, A. Plasmatic free light chains as inflammatory marker in insulin resistance: Comparison of metabolic syndrome with adult growth hormone deficiency. BioFactors 2018, 44, 480–484. [Google Scholar] [CrossRef]
- Moro, T.; Tinsley, G.; Longo, G.; Grigoletto, D.; Bianco, A.; Ferraris, C.; Guglielmetti, M.; Veneto, A.; Tagliabue, A.; Marcolin, G.; et al. Time-restricted eating effects on performance, immune function, and body composition in elite cyclists: A randomized controlled trial. J. Int. Soc. Sports Nutr. 2020, 17, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Bouzid, M.A.; Hammouda, O.; Matran, R.; Robin, S.; Fabre, C. Influence of physical fitness on antioxidant activity and malondialdehyde level in healthy older adults. Appl. Physiol. Nutr. Metab. 2015, 40, 582–589. [Google Scholar] [CrossRef]
- Nobari, H.; Nejad, H.; Kargarfard, M.; Mohseni, S.; Suzuki, K.; Adsuar, J.C.; Pérez-Gómez, J. The Effect of Acute Intense Exercise on Activity of Antioxidant Enzymes in Smokers and Non-Smokers. Biomolecules 2021, 11, 171. [Google Scholar] [CrossRef]
- Pingitore, A.; Lima, G.P.P.; Mastorci, F.; Quinones, A.; Iervasi, G.; Vassalle, C. Exercise and oxidative stress: Potential effects of an-ti-oxidant dietary strategies in sports. Nutrition 2015, 31, 916–922. [Google Scholar] [CrossRef]
- Bogdanis, G.; Stavrinou, P.; Fatouros, I.; Philippou, A.; Chatzinikolaou, A.; Draganidis, D.; Ermidis, G.; Maridaki, M. Short-term high-intensity interval exercise training attenuates oxidative stress responses and improves antioxidant status in healthy hu-mans. Food Chem. Toxicol. 2013, 61, 171–177. [Google Scholar] [CrossRef]
- Alves, N.F.; Porpino, S.K.; Monteiro, M.M.; Gomes, E.; Braga, V.A. Coconut oil supplementation and physical exercise improves baroreflex sensitivity and oxidative stress in hypertensive rats. Appl. Physiol. Nutr. Metab. 2015, 40, 393–400. [Google Scholar] [CrossRef] [Green Version]
- Lima, F.D.; Stamm, D.N.; Pace, I.D.D.; Ribeiro, L.R.; Rambo, L.M.; Bresciani, G.; Ferreira, J.; Rossato, M.F.; Silva, M.A.; Pereira, M.E.; et al. Ibuprofen intake increases exercise time to exhaustion: A possible role for pre-venting exercise-induced fa-tigue. Scand. J. Med. Sci. Sports 2016, 26, 1160–1170. [Google Scholar] [CrossRef]
- McAnulty, S.R.; Owens, J.T.; McAnulty, L.S.; Nieman, D.C.; Morrow, J.D.; Dumke, C.L.; Milne, G.L. Ibuprofen use during extreme exercise: Effects on oxidative stress and PGE2. Med. Sci. Sports Exerc. 2007, 39, 1075–1079. [Google Scholar] [CrossRef] [PubMed]
- López-Durán, J.L.; Frías-Iniesta, J. Drug synergism in analgesia treated with ibuprofen and codeine. SEMERGEN-Med. Fam. 2014, 38, 24–32. [Google Scholar] [CrossRef]
- Almqvist, P.M.; Ekström, B.; Kuenzig, M.; Haglund, U.; Schwartz, S.I. Increased survival of endotoxin-injected dogs treated with methylprednisolone, naloxone, and ibuprofen. Circ. Shock 1984, 14, 129–136. [Google Scholar] [PubMed]
- Ma, G.-D.; Chiu, C.-H.; Hsu, Y.-J.; Hou, C.-W.; Chen, Y.-M.; Huang, C.-C. Changbai Mountain Ginseng (Panax ginseng C.A. Mey) Extract Supplementation Improves Exercise Performance and Energy Utilization and Decreases Fatigue-Associated Parameters in Mice. Molecules 2017, 22, 237. [Google Scholar] [CrossRef] [PubMed]
- Febbraio, M.A.; Chiu, A.; Angus, D.J.; Arkinstall, M.J.; Hawley, J.A. Effects of carbohydrate ingestion before and during exercise on glucose kinetics and performance. J. Appl. Physiol. 2000, 89, 2220–2226. [Google Scholar] [CrossRef] [Green Version]
- Wang, J.J.; Shieh, M.J.; Kuo, S.L.; Lee, C.L.; Pan, T.M. Effect of red mold rice on antifatigue and exercise-related changes in lipid pe-roxidation in endurance exercise. Appl. Microbiol. Biotechnol. 2006, 70, 247–253. [Google Scholar] [CrossRef]
- Prakash, R.; Mullen, K.D. Mechanisms, diagnosis and management of hepatic encephalopathy. Nat. Rev. Gastroenterol. Hepatol. 2010, 7, 515–525. [Google Scholar] [CrossRef]
- Gutiérrez-De-Juan, V.; De Davalillo, S.L.; Fernández-Ramos, D.; Barbier-Torres, L.; Zubiete-Franco, I.; Fernández-Tussy, P.; Simón, J.; Lopitz-Otsoa, F.; Heras, J.D.L.; Iruzubieta, P.; et al. A morphological method for ammonia detection in liver. PLoS ONE 2017, 12, e0173914. [Google Scholar] [CrossRef] [Green Version]
- Zarrouk, N.; Mtibaa, K.; Hammouda, O.; Chtourou, H.; Chaabouni, K.; Ayadi-Makni, F.; Rebai, H. Assessment of acute neuromuscular fatigue manifestations and functional performances after heavy resistance exercise. J. Sports Med. Phys. Fit. 2021, 61, 1596–1604. [Google Scholar] [CrossRef]
- Kantanista, A.; Kusy, K.; Pospieszna, B.; Korman, P.; Wieliński, D.; Zieliński, J. Combined Analysis of Blood Ammonia and Lactate Levels as a Practical Tool to Assess the Metabolic Response to Training Sessions in Male and Female Sprinters. J. Strength Cond. Res. 2021, 35, 2591–2598. [Google Scholar] [CrossRef]
- Aamann, L.; Ochoa-Sanchez, R.; Oliveira, M.; Tremblay, M.; Bémeur, C.; Dam, G.; Vilstrup, H.; Aagaard, N.K.; Rose, C.F. Progressive resistance training prevents loss of muscle mass and strength in bile duct-ligated rats. Liver Int. 2018, 39, 676–683. [Google Scholar] [CrossRef]
- Chen, Y.-M.; Tsai, Y.-H.; Tsai, T.-Y.; Chiu, Y.-S.; Wei, L.; Chen, W.-C.; Huang, C.-C. Fucoidan Supplementation Improves Exercise Performance and Exhibits Anti-Fatigue Action in Mice. Nutrients 2014, 7, 239–252. [Google Scholar] [CrossRef] [Green Version]
- Khammassi, M.; Ouerghi, N.; Said, M.; Feki, M.; Khammassi, Y.; Pereira, B.; Thivel, D.; Bouassida, A. Continuous Moderate-Intensity but Not High-Intensity Interval Training Improves Immune Function Biomarkers in Healthy Young Men. J. Strength Cond. Res. 2020, 34, 249–256. [Google Scholar] [CrossRef]
- Fortunato, A.K.; Pontes, W.; De Souza, D.M.S.; Prazeres, J.S.F.; Marcucci-Barbosa, L.S.; Santos, J.M.M.; Veira, L.M.; Bearzoti, E.; Pinto, K.M.D.C.; Talvani, A.; et al. Strength Training Session Induces Important Changes on Physiological, Immunological, and Inflammatory Biomarkers. J. Immunol. Res. 2018, 2018, 9675216. [Google Scholar] [CrossRef]
- Ciampa, P.J.; White, R.O.; Perrin, E.M.; Yin, H.S.; Sanders, L.M.; Gayle, E.A.; Rothman, R.L. The Association of Acculturation and Health Literacy, Numeracy and Health-Related Skills in Spanish-speaking Caregivers of Young Children. J. Immigr. Minor. Health 2012, 15, 492–498. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Poonai, N.; Bhullar, G.; Lin, K.; Papini, A.; Mainprize, D.; Howard, J.; Teefy, J.; Bale, M.; Langford, C.; Lim, R.; et al. Oral administration of morphine versus ibuprofen to manage postfracture pain in children: A randomized trial. Can. Med. Assoc. J. 2014, 186, 1358–1363. [Google Scholar] [CrossRef] [Green Version]
- Vingren, J.L.; Boyett, J.C.; Lee, E.C.; Levitt, D.E.; Luk, H.Y.; McDermott, B.P.; Munoz, C.X.; Ganio, M.S.; Armstrong, L.E.; Hill, D.W. A Single Dose of Ibuprofen Impacts IL-10 Response to 164-km Road Cycling in the Heat. Res. Q. Exerc. Sport, 2022; 1–7, Epub Ahead. [Google Scholar] [CrossRef]
- Aidar, F.J.; Paz, D.A.; Gama, D.d.M.; de Souza, R.F.; Souza, L.M.V.; dos Santos, J.L.; Almeida-Neto, P.F.; Marçal, A.C.; Neves, E.B.; Moreira, O.C.; et al. Evaluation of the Post-Training Hypotensor Effect in Paralympic and Conventional Powerlifting. J. Funct. Morphol. Kinesiol. 2021, 6, 92. [Google Scholar] [CrossRef] [PubMed]
- Neves, E.B.; Vilaca-Alves, J.; Antunes, N.; Felisberto, I.M.; Rosa, C.; Reis, V.M. Different responses of the skin temperature to physical exercise: Systematic review. Annu. Int. Conf. IEEE Eng. Med. Biol. Soc. 2015, 2015, 1307–1310. [Google Scholar] [CrossRef] [PubMed]
- de Carvalho, G.; Girasol, C.E.; Gonçalves, L.G.C.; Guirro, E.C.O.; Guirro, R.R.D.J. Correlation between skin temperature in the lower limbs and biochemical marker, performance data, and clinical recovery scales. PLoS ONE 2021, 16, e0248653. [Google Scholar] [CrossRef] [PubMed]
- Sanchez-Jimenez, J.L.; Aparicio, I.; Romero-Avila, J.L.; Bellot-Arcís, C.; de Anda, R.M.C.O.; Priego-Quesada, J.I. Skin temperature measurement in individuals with spinal cord injury during and after exercise: Systematic review. J. Therm. Biol. 2021, 105, 103146. [Google Scholar] [CrossRef] [PubMed]
- Nieman, D.C. Marathon Training and Immune Function. Sports Med. 2007, 37, 412–415. [Google Scholar] [CrossRef] [PubMed]
- Clementi, E.; Cossu, M.V.; Cattaneo, D.; Fucile, S.; Baldelli, S.; Cozzi, V.; Capetti, A.F.; Pellegrino, P. Combined isosorbide dinitrate and ibuprofen as a novel therapy for muscular dystrophies: Evidence from Phase I studies in healthy volunteers. Drug Des. Dev. Ther. 2014, 8, 411–419. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alturki, M.; Beyer, I.; Mets, T.; Bautmans, I. Impact of drugs with anti-inflammatory effects on skeletal muscle and inflammation: A systematic literature review. Exp. Gerontol. 2018, 114, 33–49. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | National Level (X ± SD) | Regional Level (X ± SD) | p | t | Cohen’s d |
|---|---|---|---|---|---|
| n | 10 | 10 | |||
| Age (years) | 32.50 ± 3.00 | 30.75 ± 5.32 | 0.055 | 0.975 | 0.427 |
| Body mass (kg) | 84.00 ± 17.63 | 74.50 ± 33.88 | 0.305 | 0.963 | 0.352 |
| Experience (years) | 3.80 ± 0.68 | 3.18 ± 0.24 | 0.068 | 0.913 | 0.216 |
| 1-RM/Bench press (kg) | 153.75 ± 20.56 * | 123.00 ± 33.46 | 0.046 # | 2.930 | 1.061a |
| 1-RM/Body Weight | 1.86 ± 0.21 ** | 1.77 ± 0.41 ** | 0.038 # | 1.419 | 0.419b |
| National Level (NL) | Regional Level (RL) | ANOVA Effects | |||||
|---|---|---|---|---|---|---|---|
| PLA | IBU | PLA | IBU | Supplem | Level | Interact | |
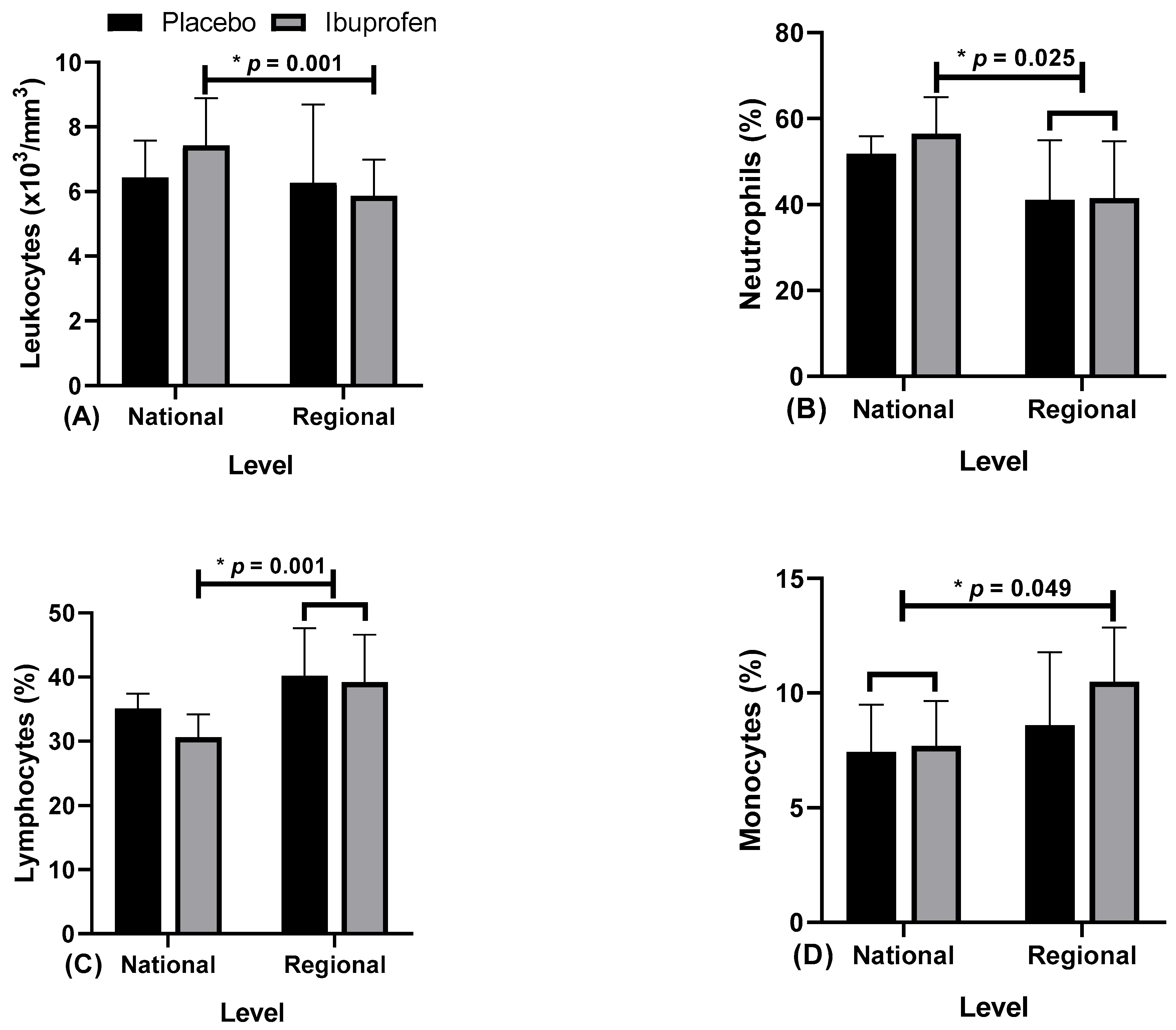
| Leukocytes (×103/mm3) | 6.44 ± 1.15 | 7.42 ± 1.47 * | 6.27 ± 2.43 | 5.87 ± 1.128 * | F = 0.350 η2p = 0.037 p = 0.569 | F = 4.405 η2p = 0.329b p = 0.001 * | F = 1.708 η2p = 0.160 p = 0.224 |
| Neutrophils (%) | 51.84 ± 4.08 | 56.46 ± 8.52 * | 41.07 ± 13.91 * | 41.50 ± 13.27 * | F = 1.038 η2p = 0.103 p = 0.335 | F = 7.187 η2p = 0.444b p = 0.025 * | F = 0.394 η2p = 0.042 p = 0.546 |
| Lymphocytes (%) | 35.12 ± 2.27 | 30.60 ± 3.58 * | 40.20 ± 7.39 * | 39.20 ± 7.41 * | F = 2.816 η2p = 0.128 p = 0.238 | F = 8.675 η2p = 0.491b p = 0.001 * | F = 1.000 η2p = 0.100 p = 0.343 |
| Monocytes (%) | 7.42 ± 2.08 * | 7.68 ± 1.98 * | 8.59 ± 3.19 | 10.49 ± 2.37 * | F = 2.853 η2p = 0.241 p = 0.125 | F = 4.712 η2p = 0.344b p = 0.049 * | F = 0.954 η2p = 0.096 p = 0.354 |
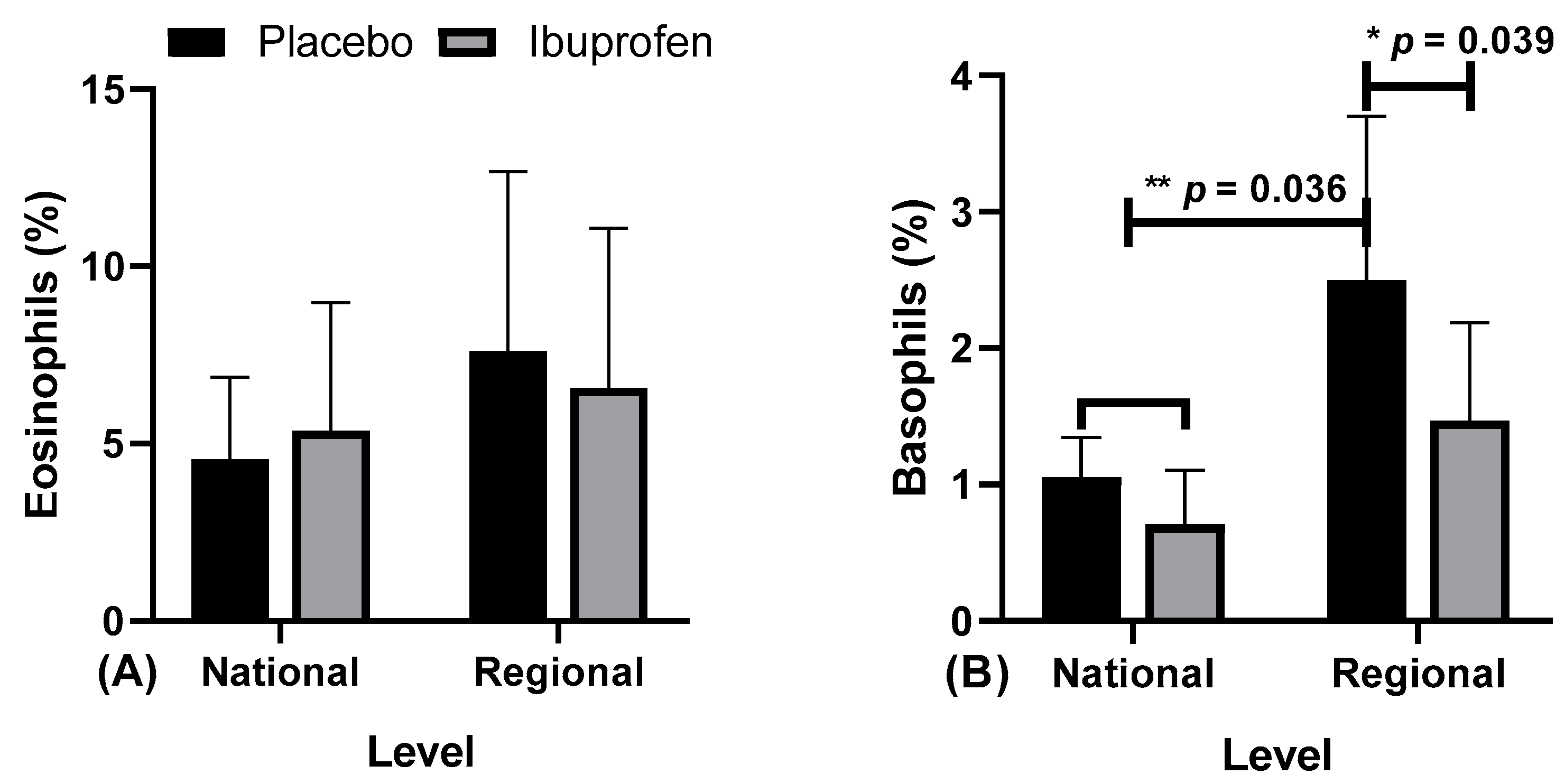
| Eosinophils (%) | 4.56 ± 2.31 | 5.36 ± 3.63 | 7.62 ± 5.05 | 6.57 ± 4.52 | F = 0.036 η2p = 0.004 p = 0.853 | F = 0.997 η2p = 0.100 p = 0.344 | F = 1.174 η2p = 0.115 p = 0.307 |
| Basophils (%) | 1.05 ± 0.29 * | 0.71 ± 0.39 * | 2.50 ± 1.21 *# | 1.47 ± 0.72 # | F = 14.240 η2p = 0.613a p = 0.036 * | F = 19.659 η2p = 0.686a p = 0.039 # | F = 1.627 η2p = 0.153 p = 0.234 |
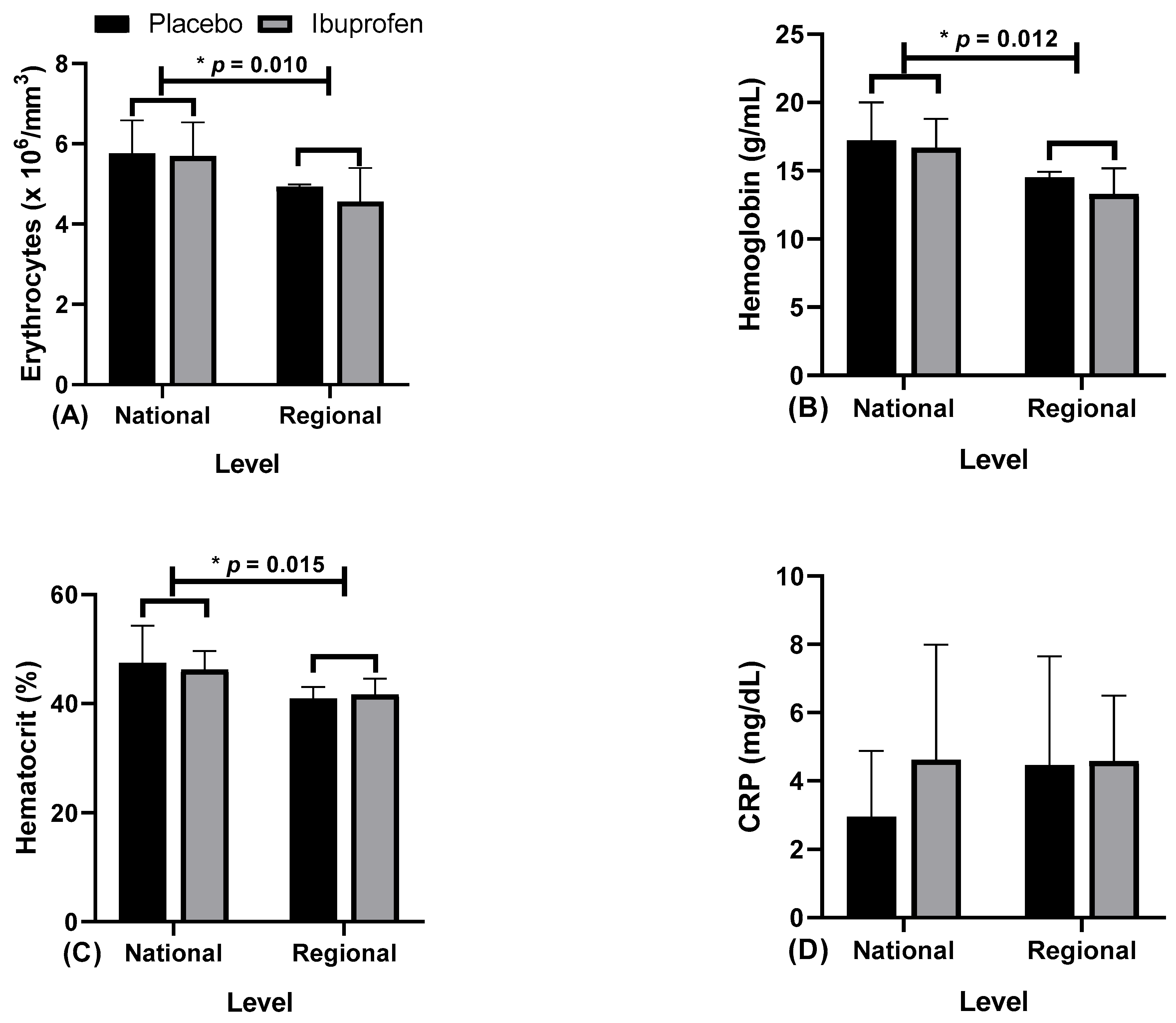
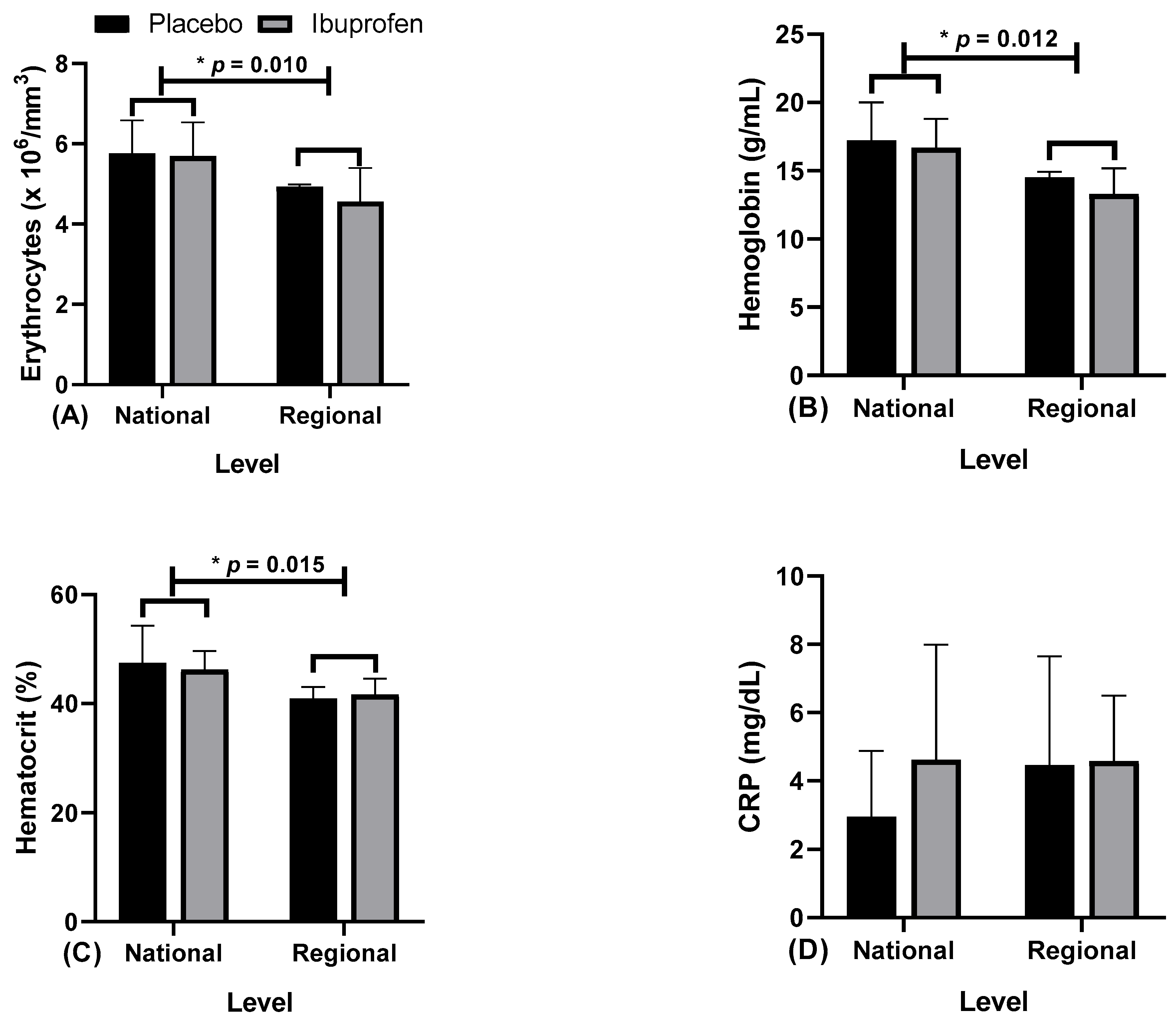
| Erythrocytes (×103/mm3) | 5.77 ± 0.82 * | 5.70 ± 0.84 * | 4.93 ± 0.05 * | 4.57 ± 0.83 * | F = 2.436 η2p = 0.213 p = 0.153 | F = 6.761 η2p = 0.429b p = 0.010 * | F = 1.282 η2p = 0.125 p = 0.287 |
| Hemoglobin (g/mL) | 17.22 ± 2.80 * | 16.70 ± 2.09 * | 14.50 ± 0.43 * | 13.30 ± 1.87 * | F = 3.280 η2p = 0.267 p = 0.104 | F = 8.998 η2p = 0.501a p = 0.012 * | F = 3.197 η2p = 0.262 p = 0.107 |
| Hematocrit (%) | 47.46 ± 6.84 | 46.21 ± 3.49 | 40.93 ± 2.07 | 41.69 ± 2.90 | F = 0.039 η2p = 0.004 p = 0.849 | F = 10.047 η2p = 0.527a p = 0.015 * | F = 1.161 η2p = 0.114 p = 0.309 |
| C-Reactive Protein (mg/dL) | 2.96 ± 1.92 | 4.62 ± 3.36 | 4.46 ± 3.20 | 4.58 ± 1.92 | F = 5.885 η2p = 0.195 p = 0.058 | F = 0.594 η2p = 0.062 p = 0.461 | F = 1.236 η2p = 0.121 p = 0.295 |
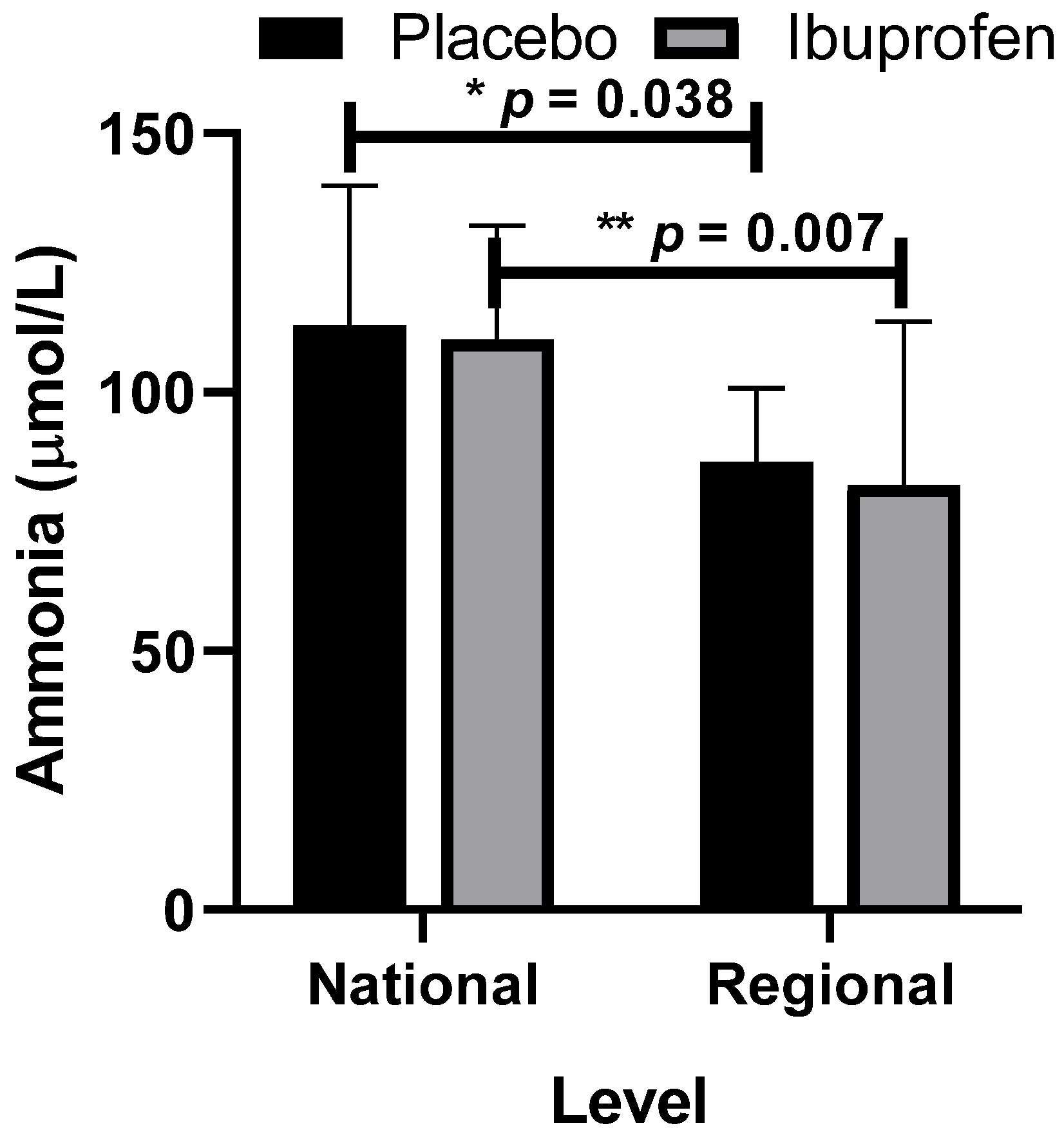
| Ammonia (μmol/L) | 112.90 ± 27.04 * | 110.23 ± 21.97 * | 86.57 ± 14.26 # | 82.05 ± 31.64 # | F = 0.132 η2p = 0.014 p = 0.725 | F = 11.937 η2p = 0.570a p = 0.038 * p = 0.007 # | F = 0.029 η2p = 0.003 p = 0.869 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Aidar, F.J.; Fraga, G.S.; Getirana-Mota, M.; Marçal, A.C.; Santos, J.L.; de Souza, R.F.; Vieira-Souza, L.M.; Ferreira, A.R.P.; de Matos, D.G.; de Almeida-Neto, P.F.; et al. Evaluation of Ibuprofen Use on the Immune System Indicators and Force in Disabled Paralympic Powerlifters of Different Sport Levels. Healthcare 2022, 10, 1331. https://doi.org/10.3390/healthcare10071331
Aidar FJ, Fraga GS, Getirana-Mota M, Marçal AC, Santos JL, de Souza RF, Vieira-Souza LM, Ferreira ARP, de Matos DG, de Almeida-Neto PF, et al. Evaluation of Ibuprofen Use on the Immune System Indicators and Force in Disabled Paralympic Powerlifters of Different Sport Levels. Healthcare. 2022; 10(7):1331. https://doi.org/10.3390/healthcare10071331
Chicago/Turabian StyleAidar, Felipe J., Guacira S. Fraga, Márcio Getirana-Mota, Anderson Carlos Marçal, Jymmys L. Santos, Raphael Fabricio de Souza, Lucio Marques Vieira-Souza, Alexandre Reis Pires Ferreira, Dihogo Gama de Matos, Paulo Francisco de Almeida-Neto, and et al. 2022. "Evaluation of Ibuprofen Use on the Immune System Indicators and Force in Disabled Paralympic Powerlifters of Different Sport Levels" Healthcare 10, no. 7: 1331. https://doi.org/10.3390/healthcare10071331
APA StyleAidar, F. J., Fraga, G. S., Getirana-Mota, M., Marçal, A. C., Santos, J. L., de Souza, R. F., Vieira-Souza, L. M., Ferreira, A. R. P., de Matos, D. G., de Almeida-Neto, P. F., Garrido, N. D., Díaz-de-Durana, A. L., Knechtle, B., de Araújo Tinoco Cabral, B. G., Murawska-Ciałowicz, E., Nobari, H., Silva, A. F., Clemente, F. M., & Badicu, G. (2022). Evaluation of Ibuprofen Use on the Immune System Indicators and Force in Disabled Paralympic Powerlifters of Different Sport Levels. Healthcare, 10(7), 1331. https://doi.org/10.3390/healthcare10071331