
A Retrospective Cohort Study on the Clinical Characteristics of Patients with Surgical Blunt Bowel and/or Mesenteric Injuries among Motorcyclists and Car Occupants



Abstract
:1. Introduction
2. Materials and Methods
2.1. Ethical Approval
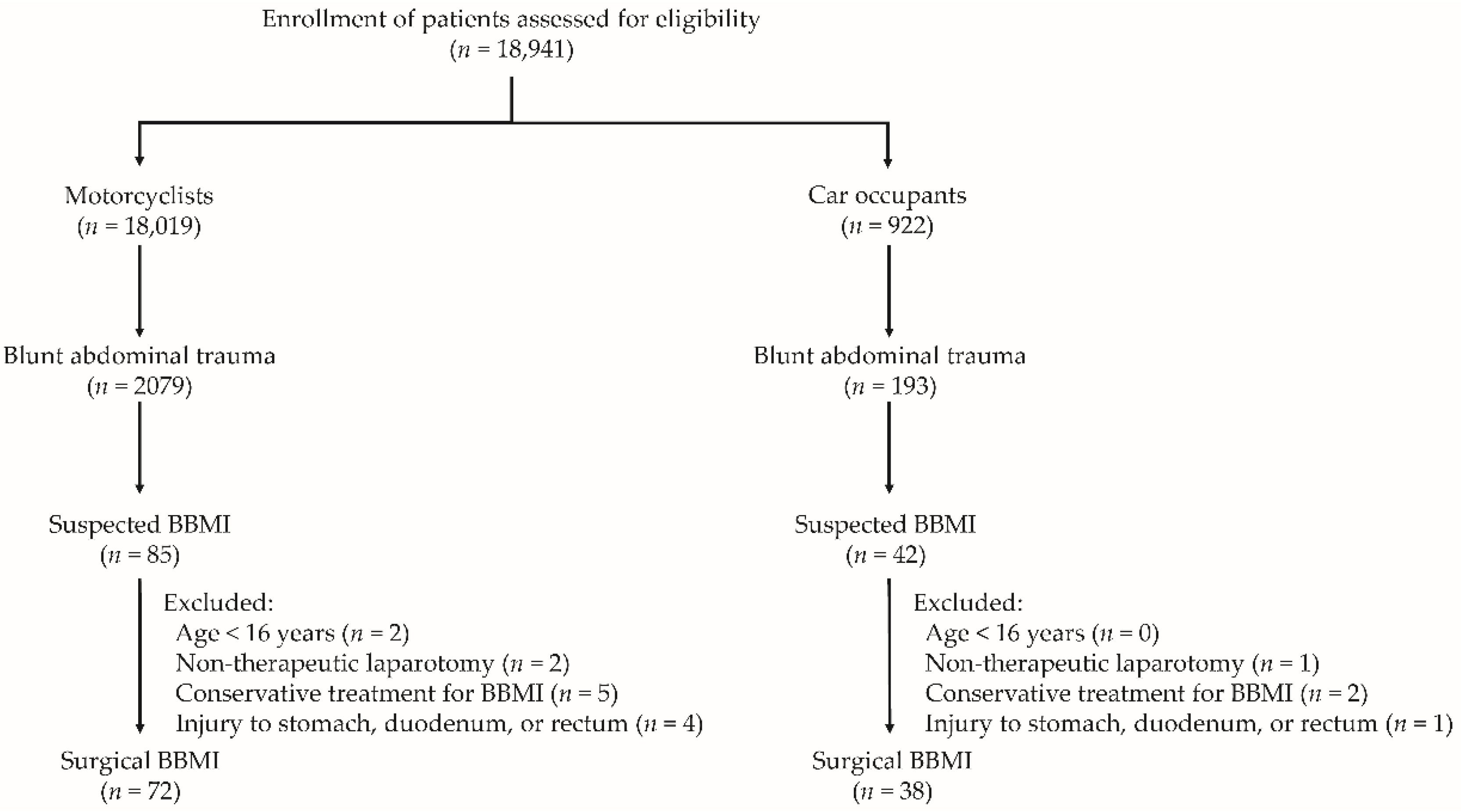
2.2. Study Population
2.3. Study Parameters
2.4. Definitions
2.5. Statistical Analysis
3. Results
3.1. Clinical Characteristics and Outcomes of Motorcyclists and Car Occupants with Surgical BBMI
3.2. Injury Severity of Body Region of Motorcyclists and Car Occupants with Surgical BBMI
3.3. Associated Injuries to Motorcyclists and Car Occupants with Surgical BBMI
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Malinoski, D.J.; Patel, M.S.; Yakar, D.O.; Green, D.; Qureshi, F.; Inaba, K.; Brown, C.V.; Salim, A. A diagnostic delay of 5 hours increases the risk of death after blunt hollow viscus injury. J. Trauma 2010, 69, 84–87. [Google Scholar] [CrossRef]
- Liao, C.H.; Hsieh, F.J.; Chen, C.C.; Cheng, C.T.; Ooyang, C.H.; Hsieh, C.H.; Yang, S.J.; Fu, C.Y. The Prognosis of Blunt Bowel and Mesenteric Injury-the Pitfall in the Contemporary Image Survey. J. Clin. Med. 2019, 8, 1300. [Google Scholar] [CrossRef] [Green Version]
- Watts, D.D.; Fakhry, S.M. Incidence of hollow viscus injury in blunt trauma: An analysis from 275,557 trauma admissions from the East multi-institutional trial. J. Trauma 2003, 54, 289–294. [Google Scholar] [CrossRef] [Green Version]
- Hsieh, T.M.; Cheng Tsai, T.; Liang, J.L.; Che Lin, C. Non-operative management attempted for selective high grade blunt hepatosplenic trauma is a feasible strategy. World J. Emerg. Surg. WJES 2014, 9, 51. [Google Scholar] [CrossRef] [Green Version]
- Cherniawsky, H.; Bratu, I.; Rankin, T.; Sevcik, W.B. Serious impact of handlebar injuries. Clin. Pediatrics 2014, 53, 672–676. [Google Scholar] [CrossRef]
- Fouda Mbarga, N.; Abubakari, A.R.; Aminde, L.N.; Morgan, A.R. Seatbelt use and risk of major injuries sustained by vehicle occupants during motor-vehicle crashes: A systematic review and meta-analysis of cohort studies. BMC Public Health 2018, 18, 1413. [Google Scholar] [CrossRef]
- Huang, C.Y.; Rau, C.S.; Chuang, J.F.; Kuo, P.J.; Hsu, S.Y.; Chen, Y.C.; Hsieh, H.Y.; Hsieh, C.H. Characteristics and Outcomes of Patients Injured in Road Traffic Crashes and Transported by Emergency Medical Services. Int. J. Environ. Res. Public Health 2016, 13, 236. [Google Scholar] [CrossRef] [Green Version]
- Hsieh, C.H.; Hsu, S.Y.; Hsieh, H.Y.; Chen, Y.C. Differences between the sexes in motorcycle-related injuries and fatalities at a Taiwanese level I trauma center. Biomed. J. 2017, 40, 113–120. [Google Scholar] [CrossRef]
- Hsieh, C.H.; Liu, H.T.; Hsu, S.Y.; Hsieh, H.Y.; Chen, Y.C. Motorcycle-related hospitalizations of the elderly. Biomed. J. 2017, 40, 121–128. [Google Scholar] [CrossRef]
- Liang, C.C.; Liu, H.T.; Rau, C.S.; Hsu, S.Y.; Hsieh, H.Y.; Hsieh, C.H. Motorcycle-related hospitalization of adolescents in a Level I trauma center in southern Taiwan: A cross-sectional study. BMC Pediatrics 2015, 15, 105. [Google Scholar] [CrossRef] [Green Version]
- Fakhry, S.M.; Brownstein, M.; Watts, D.D.; Baker, C.C.; Oller, D. Relatively short diagnostic delays (<8 hours) produce morbidity and mortality in blunt small bowel injury: An analysis of time to operative intervention in 198 patients from a multicenter experience. J. Trauma 2000, 48, 408–414; discussion 405–414. [Google Scholar] [CrossRef] [PubMed]
- Matsushima, K.; Mangel, P.S.; Schaefer, E.W.; Frankel, H.L. Blunt hollow viscus and mesenteric injury: Still underrecognized. World J. Surg. 2013, 37, 759–765. [Google Scholar] [CrossRef] [PubMed]
- Raharimanantsoa, M.; Zingg, T.; Thiery, A.; Brigand, C.; Delhorme, J.B.; Romain, B. Proposal of a new preliminary scoring tool for early identification of significant blunt bowel and mesenteric injuries in patients at risk after road traffic crashes. Eur. J. Trauma Emerg. Surg. Off. Publ. Eur. Trauma Soc. 2018, 44, 779–785. [Google Scholar] [CrossRef] [PubMed]
- Bège, T.; Chaumoître, K.; Léone, M.; Mancini, J.; Berdah, S.V.; Brunet, C. Blunt bowel and mesenteric injuries detected on CT scan: Who is really eligible for surgery? Eur. J. Trauma Emerg. Surg. Off. Publ. Eur. Trauma Soc. 2014, 40, 75–81. [Google Scholar] [CrossRef]
- Malhotra, A.K.; Fabian, T.C.; Katsis, S.B.; Gavant, M.L.; Croce, M.A. Blunt bowel and mesenteric injuries: The role of screening computed tomography. J. Trauma 2000, 48, 991–998; discussion 998–1000. [Google Scholar] [CrossRef] [PubMed]
- Abdel-Aziz, H.; Dunham, C.M. Effectiveness of computed tomography scanning to detect blunt bowel and mesenteric injuries requiring surgical intervention: A systematic literature review. Am. J. Surg. 2019, 218, 201–210. [Google Scholar] [CrossRef]
- Okishio, Y.; Ueda, K.; Nasu, T.; Kawashima, S.; Kunitatsu, K.; Kato, S. Surgical intervention for blunt bowel and mesenteric injury: Indications and time intervals. Eur. J. Trauma Emerg. Surg. 2021, 47, 1739–1744. [Google Scholar] [CrossRef]
- Menegaux, F.; Trésallet, C.; Gosgnach, M.; Nguyen-Thanh, Q.; Langeron, O.; Riou, B. Diagnosis of bowel and mesenteric injuries in blunt abdominal trauma: A prospective study. Am. J. Emerg. Med. 2006, 24, 19–24. [Google Scholar] [CrossRef]
- Al-Hassani, A.; Tuma, M.; Mahmood, I.; Afifi, I.; Almadani, A.; El-Menyar, A.; Zarour, A.; Mollazehi, M.; Latifi, R.; Al-Thani, H. Dilemma of blunt bowel injury: What are the factors affecting early diagnosis and outcomes. Am. Surg. 2013, 79, 922–927. [Google Scholar] [CrossRef]
- Hsieh, C.H.; Chen, Y.C.; Hsu, S.Y.; Hsieh, H.Y.; Chien, P.C. Defining polytrauma by abbreviated injury scale ≥3 for a least two body regions is insufficient in terms of short-term outcome: A cross-sectional study at a level I trauma center. Biomed. J. 2018, 41, 321–327. [Google Scholar] [CrossRef]
- Marshall, J.C.; Cook, D.J.; Christou, N.V.; Bernard, G.R.; Sprung, C.L.; Sibbald, W.J. Multiple organ dysfunction score: A reliable descriptor of a complex clinical outcome. Crit. Care Med. 1995, 23, 1638–1652. [Google Scholar] [CrossRef]
- Hsieh, T.M.; Tsai, T.C.; Liu, Y.W.; Hsieh, C.H. How Does the Severity of Injury Vary between Motorcycle and Automobile Accident Victims Who Sustain High-Grade Blunt Hepatic and/or Splenic Injuries? Results of a Retrospective Analysis. Int. J. Environ. Res. Public Health 2016, 13, 739. [Google Scholar] [CrossRef] [Green Version]
- Fadl, S.A.; Sandstrom, C.K. Pattern Recognition: A Mechanism-based Approach to Injury Detection after Motor Vehicle Collisions. RadioGraphics 2019, 39, 857–876. [Google Scholar] [CrossRef] [PubMed]
- Tan Chor Lip, H.; Tan, J.H.; Mohamad, Y.; Ariffin, A.C.; Imran, R.; Azmah Tuan Mat, T.N. Clinical characteristics of 1653 injured motorcyclists and factors that predict mortality from motorcycle crashes in Malaysia. Chin. J. Traumatol. Zhonghua Chuang Shang Za Zhi 2019, 22, 69–74. [Google Scholar] [CrossRef]
- Wang, C.S.; Chou, P. An analysis of unnatural deaths between 1990 and 1994 in A-Lein, Taiwan. Injury 1997, 28, 203–208. [Google Scholar] [CrossRef]
- Tsai, Y.C.; Wu, S.C.; Huang, J.F.; Kuo, S.C.H.; Rau, C.S.; Chien, P.C.; Hsieh, H.Y.; Hsieh, C.H. The effect of lowering the legal blood alcohol concentration limit on driving under the influence (DUI) in southern Taiwan: A cross-sectional retrospective analysis. BMJ Open 2019, 9, e026481. [Google Scholar] [CrossRef] [PubMed]
- Kuo, C.Y.; Chiou, H.Y.; Lin, J.W.; Tsai, S.H.; Chiang, Y.H.; Lin, C.M.; Chiu, W.T. Seatbelt Use Trauma. Brain Inj. Taiwan: A 16-Year Study. Iran. J. Public Health 2015, 44, 470–478. [Google Scholar] [PubMed]
- Granieri, S.S.; Reitano, E.E.; Bindi, F.F.; Renzi, F.F.; Sammartano, F.F.; Cimbanassi, S.S.; Gupta, S.S.; Chiara, O.O. Motorcycle-related trauma:effects of age and site of injuries on mortality. A single-center, retrospective study. World J. Emerg. Surg. 2020, 15, 18. [Google Scholar] [CrossRef]
- Küper, M.A.; Bachmann, R.; Wenig, G.F.; Ziegler, P.; Trulson, A.; Trulson, I.M.; Minarski, C.; Ladurner, R.; Stöckle, U.; Höch, A.; et al. Associated abdominal injuries do not influence quality of care in pelvic fractures-a multicenter cohort study from the German Pelvic Registry. World J. Emerg. Surg. WJES 2020, 15, 8. [Google Scholar] [CrossRef] [Green Version]
- Johnson, M.C.; Eastridge, B.J. Redefining the abdominal seatbelt sign: Enhanced CT imaging metrics improve injury prediction. Am. J. Surg. 2017, 214, 1175–1179. [Google Scholar] [CrossRef]
- Loftus, T.J.; Morrow, M.L.; Lottenberg, L.; Rosenthal, M.D.; Croft, C.A.; Smith, R.S.; Moore, F.A.; Brakenridge, S.C.; Borrego, R.; Efron, P.A.; et al. The Impact of Prior Laparotomy and Intra-abdominal Adhesions on Bowel and Mesenteric Injury Following Blunt Abdominal Trauma. World J. Surg. 2019, 43, 457–465. [Google Scholar] [CrossRef]
- Bonomi, A.M.; Granieri, S.; Gupta, S.; Altomare, M.; Cioffi, S.P.B.; Sammartano, F.; Cimbanassi, S.; Chiara, O. Traumatic hollow viscus and mesenteric injury: Role of CT and potential diagnostic-therapeutic algorithm. Updates Surg. 2021, 73, 703–710. [Google Scholar] [CrossRef]

{kind=link}
| Overall n = 110 | Motorcyclists n = 72 | Car Occupants n = 38 | p-Value | |
|---|---|---|---|---|
| Age, age | 43 (28–57) | 42.5 (24–61) | 46 (38–55) | 0.544 |
| Male, n (%) | 89 (80.9%) | 55 (76.4%) | 34 (89.5%) | 0.097 |
| ISS | 17 (9–25) | 18 (9–27) | 16 (9–18) | 0.044 |
| RTS | 7.84 (7.02–7.84) | 7.84 (6.90–7.84) | 7.84 (7.11–7.84) | 0.686 |
| TRISS | 0.97 (0.92–0.99) | 0.97 (0.90–0.99) | 0.98 (0.93–0.99) | 0.175 |
| ED vital signs and conscious | ||||
| SBP (mm/Hg) | 116 (87–137) | 118 (94–139) | 113 (86–130) | 0.352 |
| HR (beats/min) | 100 (83–119) | 101 (80–120) | 99 (85–113) | 0.952 |
| RR (times/min) | 20 (18–20) | 20 (18–20) | 20 (19–21) | 0.325 |
| GCS | 15 (14–15) | 15 (11–15) | 15 (15–15) | 0.034 |
| Intubation at ED, n (%) | 24 (21.8%) | 19 (26.4%) | 5 (13.2%) | 0.110 |
| Chest tube insertion, n (%) | 25 (22.7%) | 21 (29.2%) | 4 (10.5%) | 0.027 |
| Unplanned intubation, n (%) | 10 (9.1%) | 6 (8.3%) | 4 (10.5%) | 0.735 |
| Operative findings | ||||
| Isolated small bowel injury, n (%) | 27 (24.5%) | 18 (25%) | 9 (23.7%) | 0.879 |
| Isolated colon injury, n (%) | 10 (9.1%) | 8 (11.1%) | 2 (5.3%) | 0.489 |
| Isolated mesentery injury, n (%) | 34 (30.9%) | 26 (36.1%) | 8 (21.1%) | 0.104 |
| Combined injury, n (%) | 40 (36.4%) | 20 (27.8%) | 20 (52.6%) | 0.010 |
| Outcomes | ||||
| Morbidity, n (%) | 77 (70%) | 51 (70.8%) | 26 (68.4%) | 0.793 |
| MODS, n (%) | 59 (53.6%) | 39 (54.2%) | 20 (52.6%) | 0.878 |
| Mortality, n (%) | 15 (13.6%) | 9 (12.5%) | 6 (15.8%) | 0.633 |
| 24 h mortality, n (%) | 5 (4.5%) | 3 (4.2%) | 2 (5.3%) | 1.000 |
| Bowel-related mortality, n (%) | 3 (2.7%) | 1 (1.4%) | 2 (5.3%) | 0.274 |
| Exsanguination mortality, n (%) | 8 (7.3%) | 5 (6.9%) | 3 (7.9%) | 1.000 |
| Use of ventilator (days) | 0 (0–1) | 0 (0–2) | 0 (0–0) | 0.234 |
| ICU LOS (days) | 3 (2–8) | 3 (2–11) | 3 (2–7) | 0.934 |
| Hospitalization LOS (days) | 17 (11–31) | 21 (12–35) | 16 (11–29) | 0.248 |
| Overall n = 110 | Motorcyclists n = 72 | Car Occupants n = 38 | p-Value | |
|---|---|---|---|---|
| AIS head/neck ≥ 3 | 11 (10.0%) | 11 (15.3%) | 0 (0.0%) | 0.015 |
| AIS face ≥ 3 | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | |
| AIS chest ≥ 3 | 28 (25.5%) | 22 (30.6%) | 6 (15.8%) | 0.091 |
| AIS abdomen ≥ 3 | 101 (91.8%) | 64 (88.9%) | 37 (97.4%) | 0.159 |
| AIS extremity ≥ 3 | 24 (21.8%) | 20 (27.8%) | 4 (10.5%) | 0.037 |
| Overall n = 110 | Motorcyclists n = 72 | Car Occupants n = 38 | p-Value | |
|---|---|---|---|---|
| Intracerebral hemorrhage | 14 (12.7%) | 11 (15.3%) | 3 (7.9%) | 0.372 |
| Skull fracture | 4 (3.6%) | 4 (5.6%) | 0 (0.0%) | 0.296 |
| Facial bone fracture | 14 (12.7%) | 12 (16.7%) | 2 (5.3%) | 0.132 |
| Cervical spine fracture | 2 (1.8%) | 2 (2.8%) | 0 (0.0%) | 0.544 |
| Clavicle fracture | 7 (6.4%) | 5 (6.9%) | 2 (5.3%) | 1.000 |
| Scapula fracture | 2 (1.8%) | 1 (1.4%) | 1 (2.6%) | 1.000 |
| Rib fracture | 22 (20%) | 14 (19.4%) | 8 (21.1%) | 0.841 |
| Lung contusion | 15 (13.6%) | 9 (12.5%) | 6 (15.8%) | 0.633 |
| Hemopneumothorax | 22 (20.0%) | 17 (23.6%) | 5 (13.2%) | 0.192 |
| Spleen injury | 8 (7.3%) | 6 (8.3%) | 2 (5.3%) | 0.712 |
| Liver injury | 21 (19.1%) | 12 (16.7%) | 9 (23.7%) | 0.373 |
| Pancreas injury | 6 (5.5%) | 3 (4.2%) | 3 (7.9%) | 0.414 |
| Kidney injury | 7 (6.4%) | 6 (8.3%) | 1 (2.6%) | 0.418 |
| Diaphragm injury | 3 (2.7%) | 3 (4.2%) | 0 (0.0%) | 0.550 |
| Great vessel injury | 13 (11.8%) | 9 (12.5%) | 4 (10.5%) | 1.000 |
| Thoracic spine fracture | 1 (0.9%) | 1 (1.4%) | 0 (0.0%) | 1.000 |
| Lumbar spine fracture | 4 (3.6%) | 2 (2.8%) | 2 (5.3%) | 0.607 |
| Pelvic fracture | 14 (12.7%) | 13 (18.1%) | 1 (2.6%) | 0.032 |
| Upper limb fracture | 20 (18.2%) | 17 (23.6%) | 3 (7.9%) | 0.042 |
| Lower limb fracture | 22 (20%) | 16 (22.2%) | 6 (15.8%) | 0.423 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hsieh, T.-M.; Chuang, P.-C.; Liu, C.-T.; Wu, B.-Y.; Hsieh, C.-H. A Retrospective Cohort Study on the Clinical Characteristics of Patients with Surgical Blunt Bowel and/or Mesenteric Injuries among Motorcyclists and Car Occupants. Healthcare 2022, 10, 1323. https://doi.org/10.3390/healthcare10071323
Hsieh T-M, Chuang P-C, Liu C-T, Wu B-Y, Hsieh C-H. A Retrospective Cohort Study on the Clinical Characteristics of Patients with Surgical Blunt Bowel and/or Mesenteric Injuries among Motorcyclists and Car Occupants. Healthcare. 2022; 10(7):1323. https://doi.org/10.3390/healthcare10071323
Chicago/Turabian StyleHsieh, Ting-Min, Po-Chun Chuang, Chun-Ting Liu, Bei-Yu Wu, and Ching-Hua Hsieh. 2022. "A Retrospective Cohort Study on the Clinical Characteristics of Patients with Surgical Blunt Bowel and/or Mesenteric Injuries among Motorcyclists and Car Occupants" Healthcare 10, no. 7: 1323. https://doi.org/10.3390/healthcare10071323
APA StyleHsieh, T.-M., Chuang, P.-C., Liu, C.-T., Wu, B.-Y., & Hsieh, C.-H. (2022). A Retrospective Cohort Study on the Clinical Characteristics of Patients with Surgical Blunt Bowel and/or Mesenteric Injuries among Motorcyclists and Car Occupants. Healthcare, 10(7), 1323. https://doi.org/10.3390/healthcare10071323