
Mixed-Method Evaluation of a Community Pharmacy Antimicrobial Stewardship Intervention (PAMSI)

 ,
,  ,
,  , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
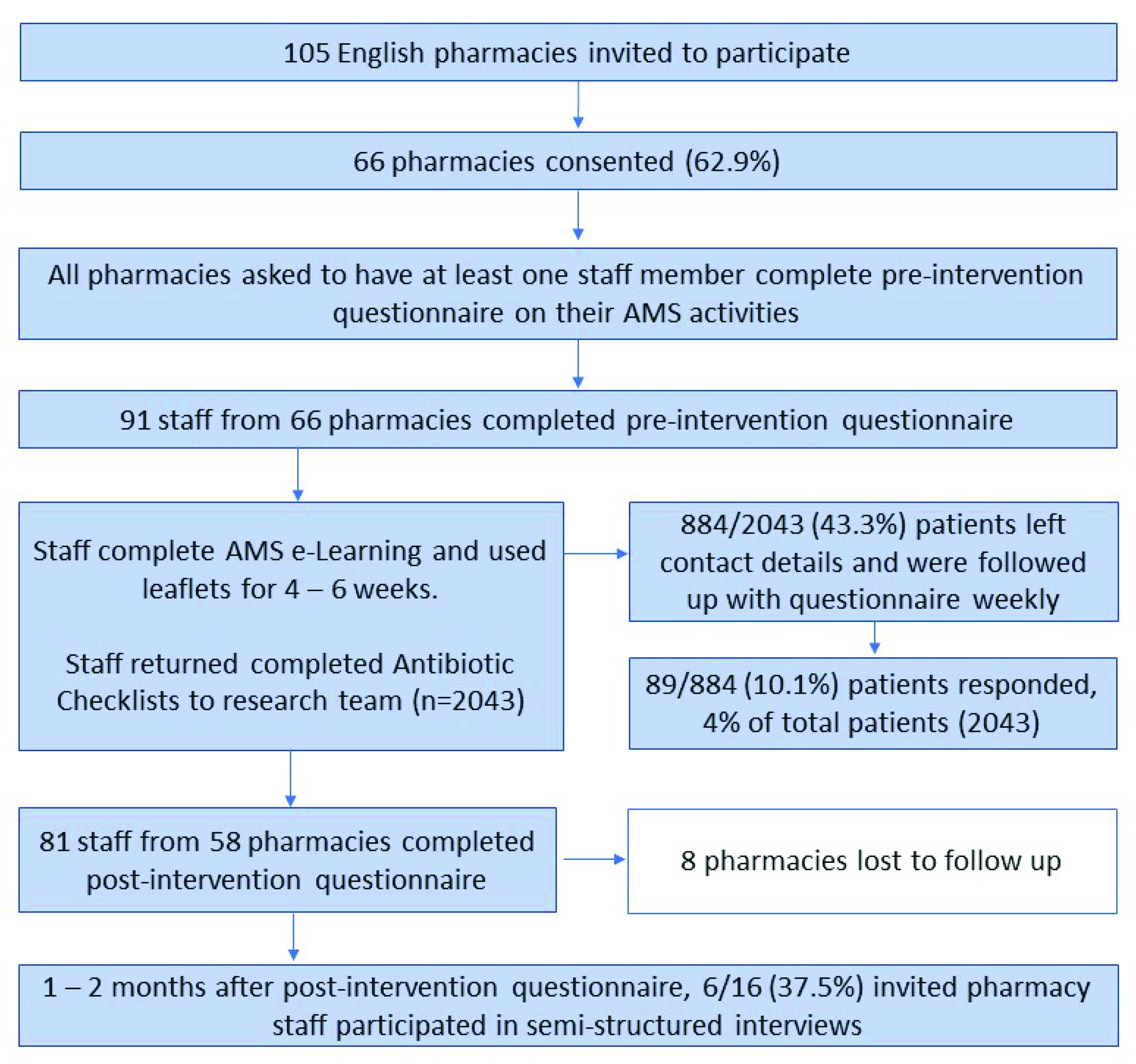
2.1. Study Design
2.2. Pilot Study
2.3. Setting and Participants
2.4. Data Collection
- (a)
- TARGET Antibiotic Checklists
- (b)
- Staff questionnaires
- (c)
- Staff interviews
- (d)
- Patient questionnaire
2.5. Data Analysis
2.6. Ethics
3. Results
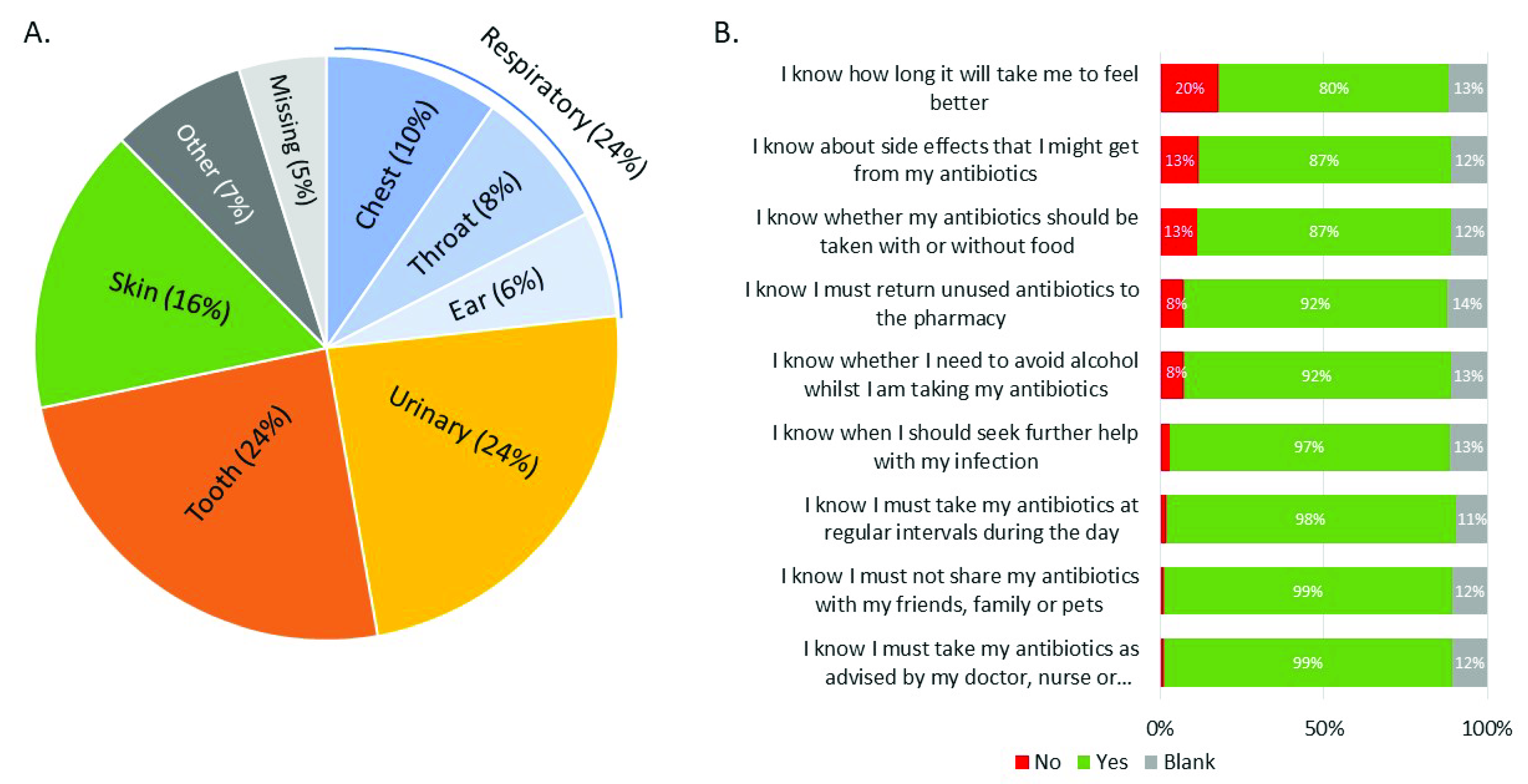
3.1. TARGET Antibiotic Checklist Results
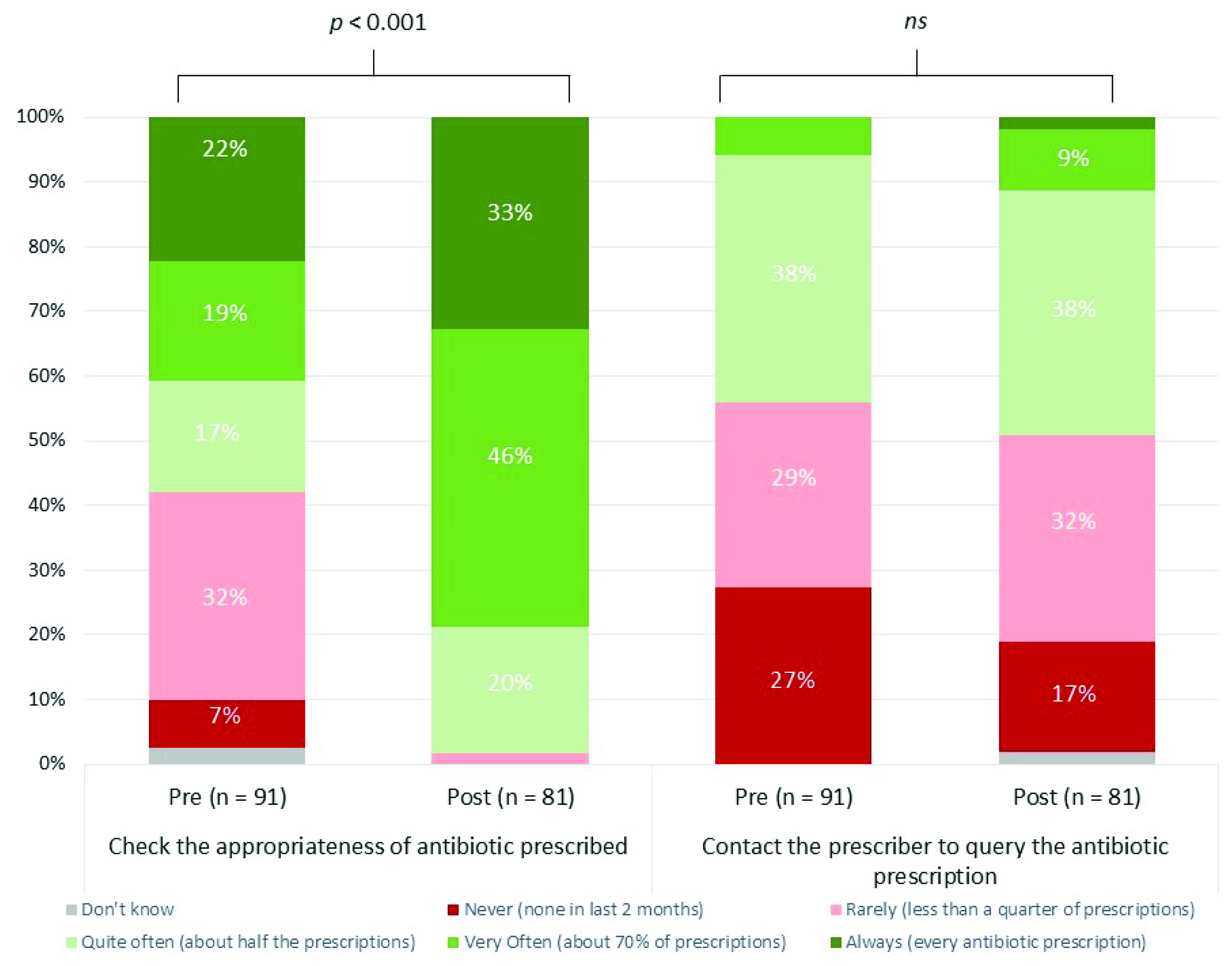
3.2. Pharmacy Staff Questionnaire Findings
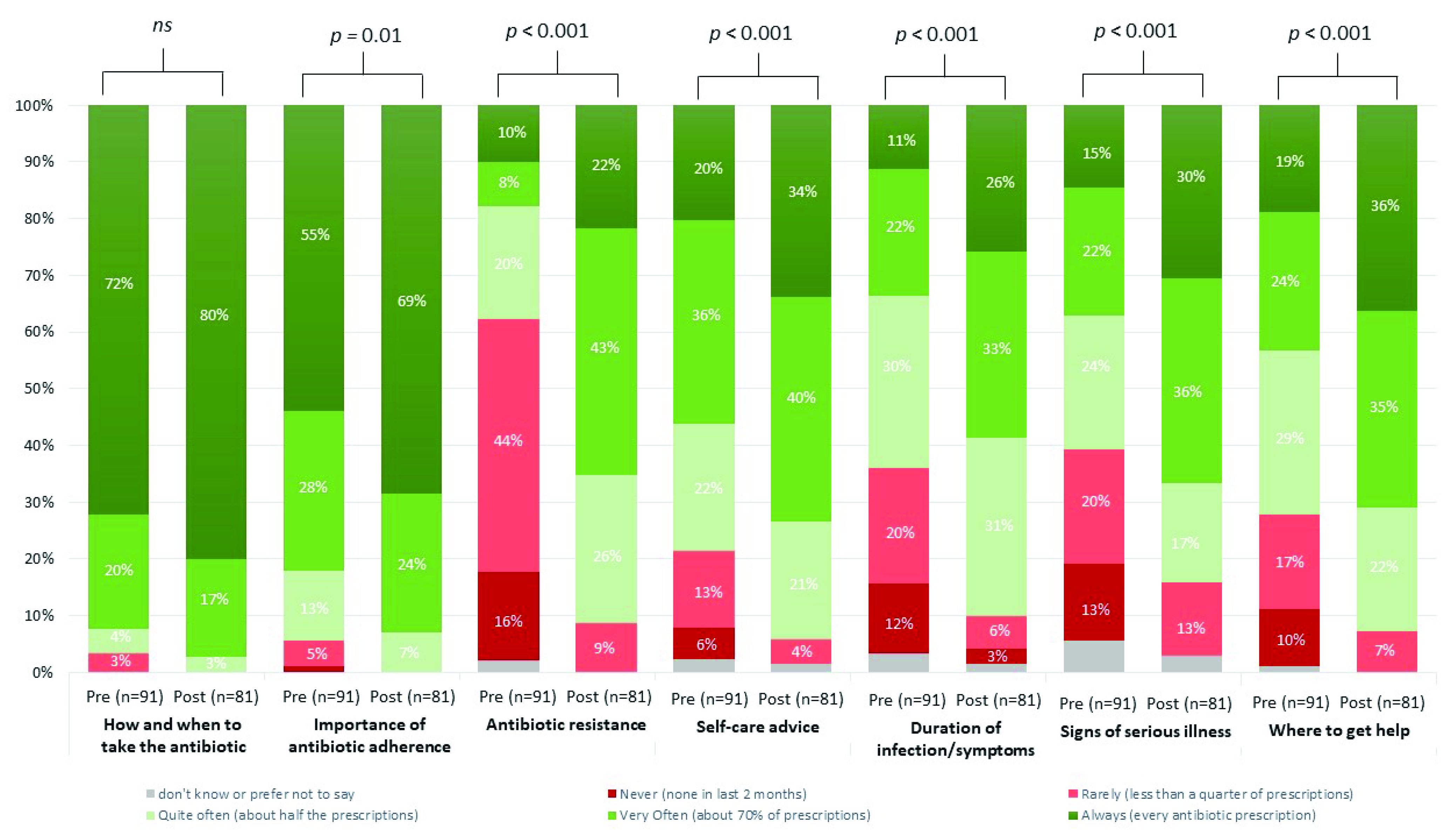
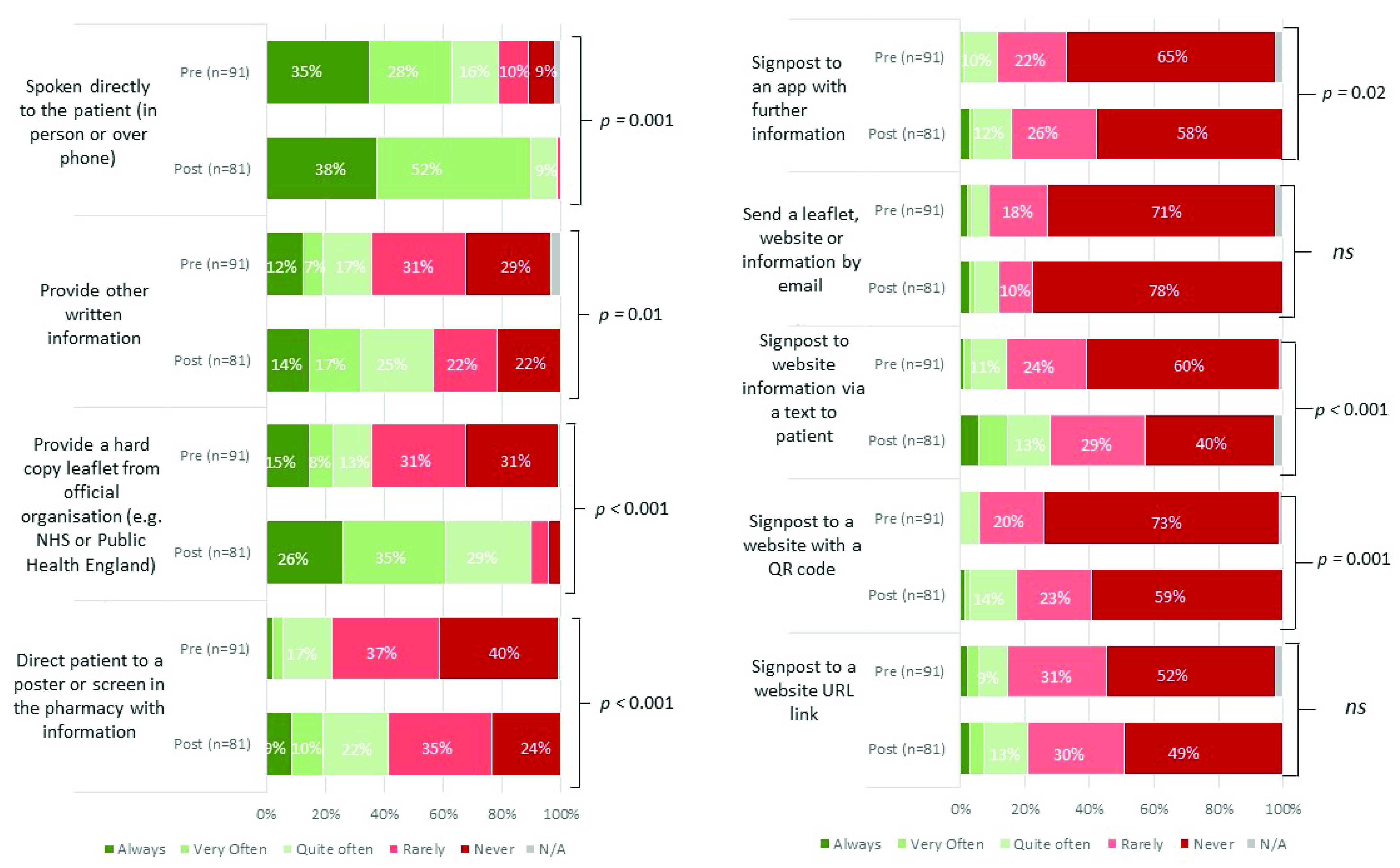
3.2.2. Providing Advice
3.3. Pharmacy Staff Interview Themes
3.3.1. Theme 1: Enablers for Embedding into Practice
3.3.2. Theme 2: Perceived Benefits
3.3.3. Theme 3: Barriers to Intervention Implementation
4. Discussion
5. Strengths and Limitations
6. Implications and Recommendations
7. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Department of Health and Social Care. The UK’s 20-Year Vision for Antimicrobial Resistance; Department of Health and Social Care: London, UK, 2019. [Google Scholar]
- Department of Health and Social Care. UK AMR 5 Year National Action Plan; Department of Health and Social Care: London, UK, 2019. [Google Scholar]
- UK Health Security Agency. English Surveillance Programme for Antimicrobial Utilisation and Resistance (ESPAUR): Report 2018–2019; UK Health Security Agency: London, UK, 2019. [Google Scholar]
- UK Health Security Agency. English Surveillance Programme for Antimicrobial Utilisation and Resistance (ESPAUR) Report 2020–2021; UK Health Security Agency: London, UK, 2021. [Google Scholar]
- Pharmaceutical Services Negotiating Committee. About Community Pharmacy. Available online: https://psnc.org.uk/psncs-work/about-community-pharmacy/ (accessed on 6 December 2021).
- Bishop, C.; Yacoob, Z.; Knobloch, M.J.; Safdar, N. Community pharmacy interventions to improve antibiotic stewardship and implications for pharmacy education: A narrative overview. Res. Soc. Adm. Pharm. 2019, 15, 627–631. [Google Scholar] [CrossRef] [PubMed]
- Department of Health and Social Care; NHS England and NHS Improvement; Pharmaceutical Services Negotiating Committee (PSNC). The Community Pharmacy Contractual Framework for 2019/20 to 2023/24: Supporting Delivery for the NHS Long Term Plan. Available online: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/819601/cpcf-2019-to-2024.pdf (accessed on 1 December 2021).
- Pharmaceutical Services Negotiating Committee. Pharmacy Quality Scheme 2021/22. Available online: https://psnc.org.uk/services-commissioning/pharmacy-quality-scheme/ (accessed on 6 December 2021).
- Fernandes, M.; Leite, A.; Basto, M.; Nobre, M.A.; Vieira, N.; Fernandes, R.; Nogueira, P.; Nicola, P.J. Non-adherence to antibiotic therapy in patients visiting community pharmacies. Int. J. Clin. Pharm. 2014, 36, 86–91. [Google Scholar] [CrossRef] [PubMed]
- Francis, N.A.; Gillespie, D.; Nuttall, J.; Hood, K.; Little, P.; Verheij, T.; Coenen, S.; Cals, J.W.; Goossens, H.; Butler, C.C.; et al. Antibiotics for acute cough: An international observational study of patient adherence in primary care. Br. J. Gen. Pract. 2012, 62, e429–e437. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kardas, P.; Devine, S.; Golembesky, A.; Roberts, C. A systematic review and meta-analysis of misuse of antibiotic therapies in the community. Int. J. Antimicrob. Agents 2005, 26, 106–113. [Google Scholar] [CrossRef] [PubMed]
- Llor, C.; Hernandez, S.; Bayona, C.; Moragas, A.; Sierra, N.; Hernandez, M.; Miravitlles, M. A study of adherence to antibiotic treatment in ambulatory respiratory infections. Int. J. Infect. Dis. 2013, 17, e168–e172. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McNulty, C.; Read, B.; Quigley, A.; Verlander, N.Q.; Lecky, D.M. What the public in England know about antibiotic use and resistance in 2020: A face-to-face questionnaire survey. BMJ Open 2022, 12, e055464. [Google Scholar] [CrossRef] [PubMed]
- UK Health Security Agency. Antibiotic-Resistant Infections Fell in 2020 for First Time Since 2016, but UKHSA Warns Drop Likely Temporary; UK Health Security Agency: London, UK, 2021. [Google Scholar]
- Ghiga, I.; Stålsby Lundborg, C. ‘Struggling to be a defender of health’ -a qualitative study on the pharmacists’ perceptions of their role in antibiotic consumption and antibiotic resistance in Romania. J. Pharm. Policy Pract. 2016, 9, 10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jones, L.F.; Owens, R.; Sallis, A.; Ashiru-Oredope, D.; Thornley, T.; Francis, N.A.; Butler, C.; McNulty, C.A.M. Qualitative study using interviews and focus groups to explore the current and potential for antimicrobial stewardship in community pharmacy informed by the Theoretical Domains Framework. BMJ Open 2018, 8, e025101. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tonna, A.P.; Weidmann, A.E.; Sneddon, J.; Stewart, D. Views and experiences of community pharmacy team members on antimicrobial stewardship activities in Scotland: A qualitative study. Int. J. Clin. Pharm. 2020, 42, 1261–1269. [Google Scholar] [CrossRef] [PubMed]
- Blanchette, L.; Gauthier, T.; Heil, E.; Klepser, M.; Kelly, K.M.; Nailor, M.; Wei, W.; Suda, K. Outpatient Stewardship Working, G. The essential role of pharmacists in antibiotic stewardship in outpatient care: An official position statement of the Society of Infectious Diseases Pharmacists. J. Am. Pharm. Assoc. 2018, 58, 481–484. [Google Scholar] [CrossRef]
- Royal College of General Practitioners. Target Antibiotics Toolkit Hub. Available online: https://elearning.rcgp.org.uk/course/view.php?id=553 (accessed on 26 May 2022).
- Allison, R.; Chapman, S.; Howard, P.; Thornley, T.; Ashiru-Oredope, D.; Walker, S.; Jones, L.F.; McNulty, C.A. Community pharmacy campaign to Keep Antibiotics Working (KAW): An innovative new approach to improve patients’ understanding of their antibiotics. JAC Antimicrob. Resist. 2020, 2, dlaa089. [Google Scholar] [CrossRef] [PubMed]
- Michie, S.; van Stralen, M.M.; West, R. The behaviour change wheel: A new method for characterising and designing behaviour change interventions. Implement. Sci. 2011, 6, 42. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Antimicrobial Stewardship for Community Pharmacy Staff E-Learning. Available online: https://www.e-lfh.org.uk/programmes/antimicrobial-resistance-and-infections/ (accessed on 7 December 2021).
- Antibiotic Research UK. Resources about Antibiotic Resistance. Available online: https://www.antibioticresearch.org.uk/resources/ (accessed on 7 December 2021).
- Braun, V.; Clarke, V. Using thematic analysis in psychology. Qual. Res. Psychol. 2006, 3, 77–101. [Google Scholar] [CrossRef] [Green Version]
- Hancock, L.J.; Mellor, C. An evaluation of antimicrobial stewardship in community pharmacy. Fields J. Hudders. Stud. Res. 2016, 2, e23. [Google Scholar]
- Ashiru-Oredope, D.; Doble, A.; Thornley, T.; Saei, A.; Gold, N.; Sallis, A.; McNulty, C.A.M.; Lecky, D.; Umoh, E.; Klinger, C. Improving Management of Respiratory Tract Infections in Community Pharmacies and Promoting Antimicrobial Stewardship: A Cluster Randomised Control Trial with a Self-Report Behavioural Questionnaire and Process Evaluation. Pharmacy 2020, 8, 44. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Res, R.; Hoti, K.; Charrois, T.L. Pharmacists’ perceptions regarding optimization of antibiotic prescribing in the community. J. Pharm. Pract. 2017, 30, 146–153. [Google Scholar] [CrossRef] [PubMed]
- Peiffer-Smadja, N.; Allison, R.A.-O.; Jones, L.A.-O.; Holmes, A.; Patel, P.; Lecky, D.A.-O.; Ahmad, R.; McNulty, C.A.-O. Preventing and Managing Urinary Tract Infections: Enhancing the Role of Community Pharmacists—A Mixed Methods Study. Antibiotics 2020, 9, 583. [Google Scholar] [CrossRef] [PubMed]
- Baqir, W.; Learoyd, T.; Sim, A.; Todd, A. Cost analysis of a community pharmacy ‘minor ailment scheme’across three primary care trusts in the North East of England. J. Public Health 2011, 33, 551–555. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hayes, C.V.; Mahon, B.; Sides, E.; Allison, R.; Lecky, D.M.; McNulty, C.A.M. Empowering Patients to Self-Manage Common Infections: Qualitative Study Informing the Development of an Evidence-Based Patient Information Leaflet. Antibiotics 2021, 10, 1113. [Google Scholar] [CrossRef] [PubMed]
- Fanuel, E.K. Exploring public awareness of community pharmacy services through the ‘ask your pharmacy team’ campaign. Med. Law 2016, 35, 5–24. [Google Scholar]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Pharmacy Staff Characteristics (n = 101) | Number (%) |
|---|---|
| Role | |
| Pharmacist | 60 (59%) |
| Dispensary team/dispenser | 18 (18%) |
| Pharmacy technician | 7 (7%) |
| Pharmacy manager | 11 (11%) |
| Pre-registration pharmacist | 4 (4%) |
| Trainee technician | 1 (1%) |
| Has participated in previous AMS/IPC intervention | |
| Yes | 10 (10%) |
| No | 75 (74%) |
| Do not know or missing | 16 (16%) |
| Has had previous training on AMS or IPC | |
| Yes | 21 (21%) |
| No | 54 (53%) |
| Do not know | 17 (17%) |
| Missing | 9 (9%) |
| Type of pharmacy they work in | |
| Town centre/high street | 31 (30%) |
| Edge of town | 7 (7%) |
| City Centre | 13 (13%) |
| Small London store | 7 (7%) |
| Health centre | 5 (5%) |
| Retail park/shopping centre | 8 (8%) |
| Train station pharmacy | 5 (5%) |
| Rural | 14 (14%) |
| Rural (small pharmacy) | 11 (11%) |
| Region of pharmacy they work in | |
| South West | 29 (28%) |
| East of England | 14 (14%) |
| Central England | 9 (9%) |
| London | 20 (20%) |
| West Midlands | 4 (4%) |
| South East | 21 (21%) |
| North West | 4 (4%) |
| Theme | Subtheme | COM | Quote |
|---|---|---|---|
| Enablers for embedding into practice | Extra time to implement resources is feasible and justified in everyday practice | O | “Yeah I think it should be part of your normal practice. If someone’s got something that needs explaining it needs explaining.” “…because some people say, no, that’s miles too much time. But, again, if care is at the forefront then what’s five minutes?” |
| Use of Antibiotic Checklist and leaflets became part of routine | O | “…when I’m doing a consultation and I give the leaflet out to people then, just because it’s part of our consultation routine already” “We have the wallet system on the counter so we put it in with the prescription in the wallet so that when the girls got the prescription out they could see that it needed to be part of the survey.” | |
| Whole team involvement to implement the resources | O M | “so it wasn’t just the pharmacists doing it, we had the whole team on it, doing the checklist and handing out, at the handing out process, because part of handing out process they do, do that… So they were confident doing the checklist.“ | |
| Leaflets and checklist worked in conjunction to facilitate conversations | O | “…the number of patients we saw that were coming in with minor infections and ailments…we could use the leaflets at that stage to talk to patients” “I think because we were having more of an active conversation about the antibiotics, and then you can make reference to the leaflet and it ties it all in together for the patient” | |
| Implementation fit with wider priorities | O M | “It [AMS e-Learning] was part of our Pharmacy Quality Payments Scheme, there’s a domain that we have to fulfil around antimicrobial resistance.” | |
| e-Learning helped understand justification | M | “So, I think, more than anything, the e-Learning was what made me evaluate my practice and try and promote antibiotic resistance as much, more than I did at the time.” | |
| Perceived benefits | Staff felt confident and encouraged to query prescriptions | C O M | “But the reverse part which checklist brought back to me was that like, do you actually need this [antibiotic] at this point, is what was very interesting.” “So from a team point of view, materials helped give them confidence that they had something to use as a resource to have the conversation [with a prescriber].” |
| Conversations with patients were more effective | C O M | “…that’s a conversation that wouldn’t have ever occurred had we not had the checklist.” “I think [completing antibiotic checklist] was really helpful actually. I think it draws the patient’s attention more to what they might not realise.” | |
| Beliefs about benefits to patients | M | “I was answering questions that I would not usually be asked by patients, so I think they were gaining a lot from the checklist, a lot more knowledge about their medications.” “…they’re [the patients] using their antibiotics more effectively and getting more optimal effects from them, and that’s what we want our patients to get at the end of the day” | |
| Barriers to intervention due to COVID-19 and other contextual factors | Change in prescribing habits and fluctuating patients | O | “No, we just, what had happened during COVID-19 is the dentists weren’t really seeing patients, so they were emailing us prescriptions for antibiotics.” “…there was definitely a reduction of the amount of checklists that we would have completed because we had a higher volume of patients coming in before the pandemic. And so, we would have had more prescriptions and people completing the checklist.” |
| Importance of continuity along patient pathway | O | “…maybe some highlighting or awareness to GP surgeries as well, but this is what they’re doing. And maybe that would get them to reflect on their practice too because I think, as much as we change our practice, it’s also really important for GPs and prescribers to have that awareness and that extra thought that we now have, is this really necessary or is it the correct duration, and things like that.” “…but I do feel that there’s more conversations to be had between the GPs and the pharmacists of the nominated pharmacy that it’s going to.” | |
| Patients did not want to interact with physical materials | O | “In terms of any other barriers, I would say the main barrier that I faced was a lot of people didn’t want to touch it [the Antibiotic Checklist] after I had touched it.” “There wasn’t really anything preventing them from giving the leaflets but, we had to be mindful of infection control when using pens and passing them back and forth.” | |
| Time barriers | O | “We couldn’t just ask them to sit down and do it. So yeah, it was a little bit more time consuming than I suppose it would have been in normal times but quite helpful.” | |
| Patients not physically present | O | “…sometimes I think you’re wanting to make sure the message landed once the prescription got back to the patient and there was no way of checking that.” “Maybe not so many for the delivery patients because it’s difficult to have a conversation with them and they’re not quite sure why they’re being given medication anyway.” “When a representative came in to collect a prescription on behalf of the patient, I would add to the conversation I had put some leaflets inside, please get [the patient] to give me a call if they have any questions...And I didn’t get anything.” | |
| Belief that not all patients engaged with checklist | O | “So I personally think and because it’s such a long questionnaire as well handing it over the patient, I don’t think we would get a realistic response, but I would definitely try it.” “…when you hand something over to patient to complete, I find, this is my personal experience, that they don’t read all the questions, they just skim read it and tick it off” “sometimes it makes it easier for the patients to understand and for you to tick for them.” | |
| Language barriers | O | “…but then again if you have a pharmacist who can speak that language it was well signposted to the pharmacist directly in the first place. So they saw a barrier, they overcome the barrier, but I wouldn’t say they overcame that 100% of the time.” |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hayes, C.V.; Lecky, D.M.; Pursey, F.; Thomas, A.; Ashiru-Oredope, D.; Saei, A.; Thornley, T.; Howard, P.; Dickinson, A.; Ingram, C.; et al. Mixed-Method Evaluation of a Community Pharmacy Antimicrobial Stewardship Intervention (PAMSI). Healthcare 2022, 10, 1288. https://doi.org/10.3390/healthcare10071288
Hayes CV, Lecky DM, Pursey F, Thomas A, Ashiru-Oredope D, Saei A, Thornley T, Howard P, Dickinson A, Ingram C, et al. Mixed-Method Evaluation of a Community Pharmacy Antimicrobial Stewardship Intervention (PAMSI). Healthcare. 2022; 10(7):1288. https://doi.org/10.3390/healthcare10071288
Chicago/Turabian StyleHayes, Catherine V., Donna M. Lecky, Fionna Pursey, Amy Thomas, Diane Ashiru-Oredope, Ayoub Saei, Tracey Thornley, Philip Howard, Aimi Dickinson, Clare Ingram, and et al. 2022. "Mixed-Method Evaluation of a Community Pharmacy Antimicrobial Stewardship Intervention (PAMSI)" Healthcare 10, no. 7: 1288. https://doi.org/10.3390/healthcare10071288
APA StyleHayes, C. V., Lecky, D. M., Pursey, F., Thomas, A., Ashiru-Oredope, D., Saei, A., Thornley, T., Howard, P., Dickinson, A., Ingram, C., Allison, R., & McNulty, C. A. M. (2022). Mixed-Method Evaluation of a Community Pharmacy Antimicrobial Stewardship Intervention (PAMSI). Healthcare, 10(7), 1288. https://doi.org/10.3390/healthcare10071288