
A Design Approach to Optimise Secure Remote Three-Dimensional (3D) Printing: A Proof-of-Concept Study towards Advancement in Telemedicine


Abstract
:1. Introduction
2. Materials and Methods
2.1. Materials
2.2. Methods
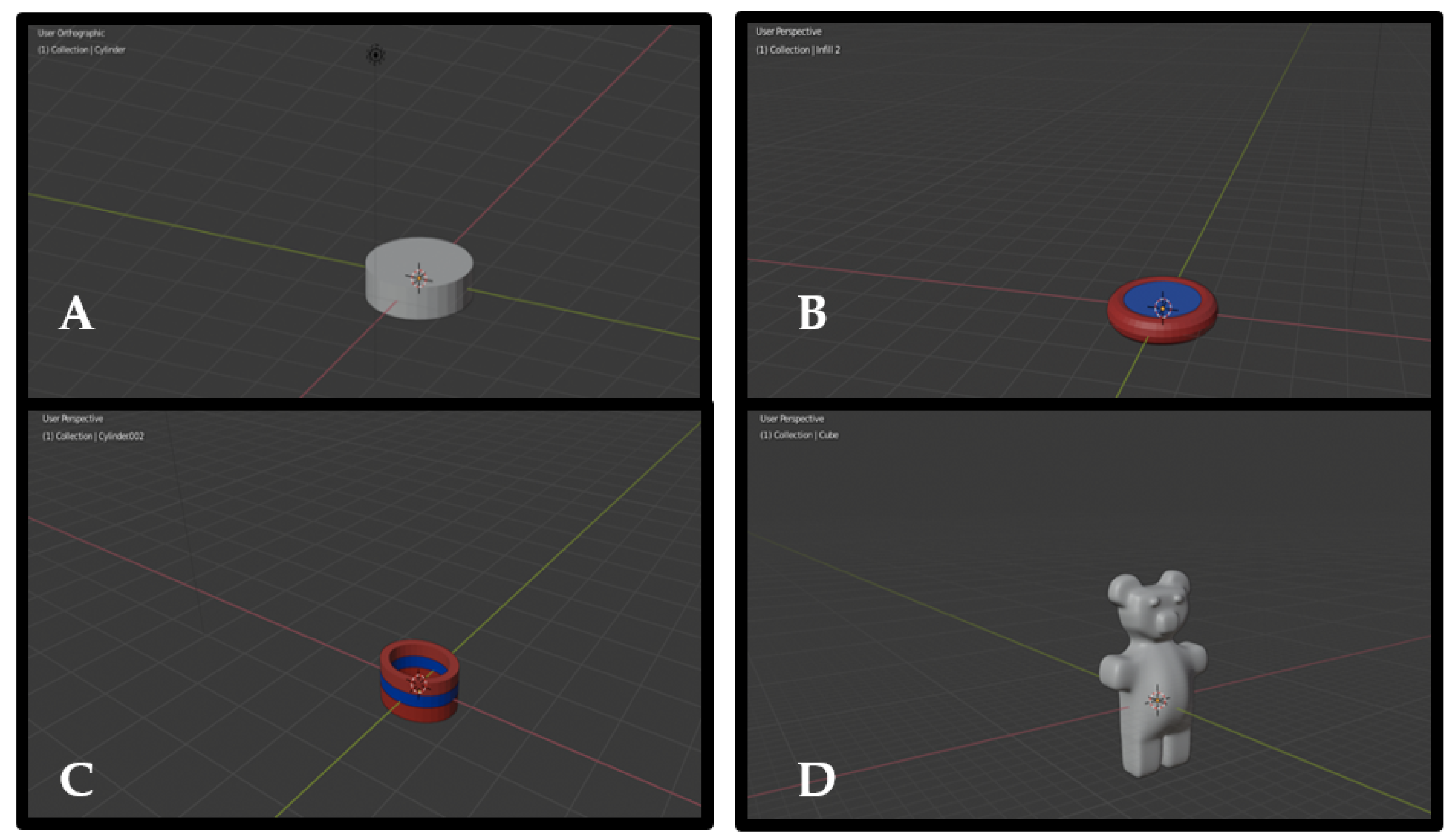
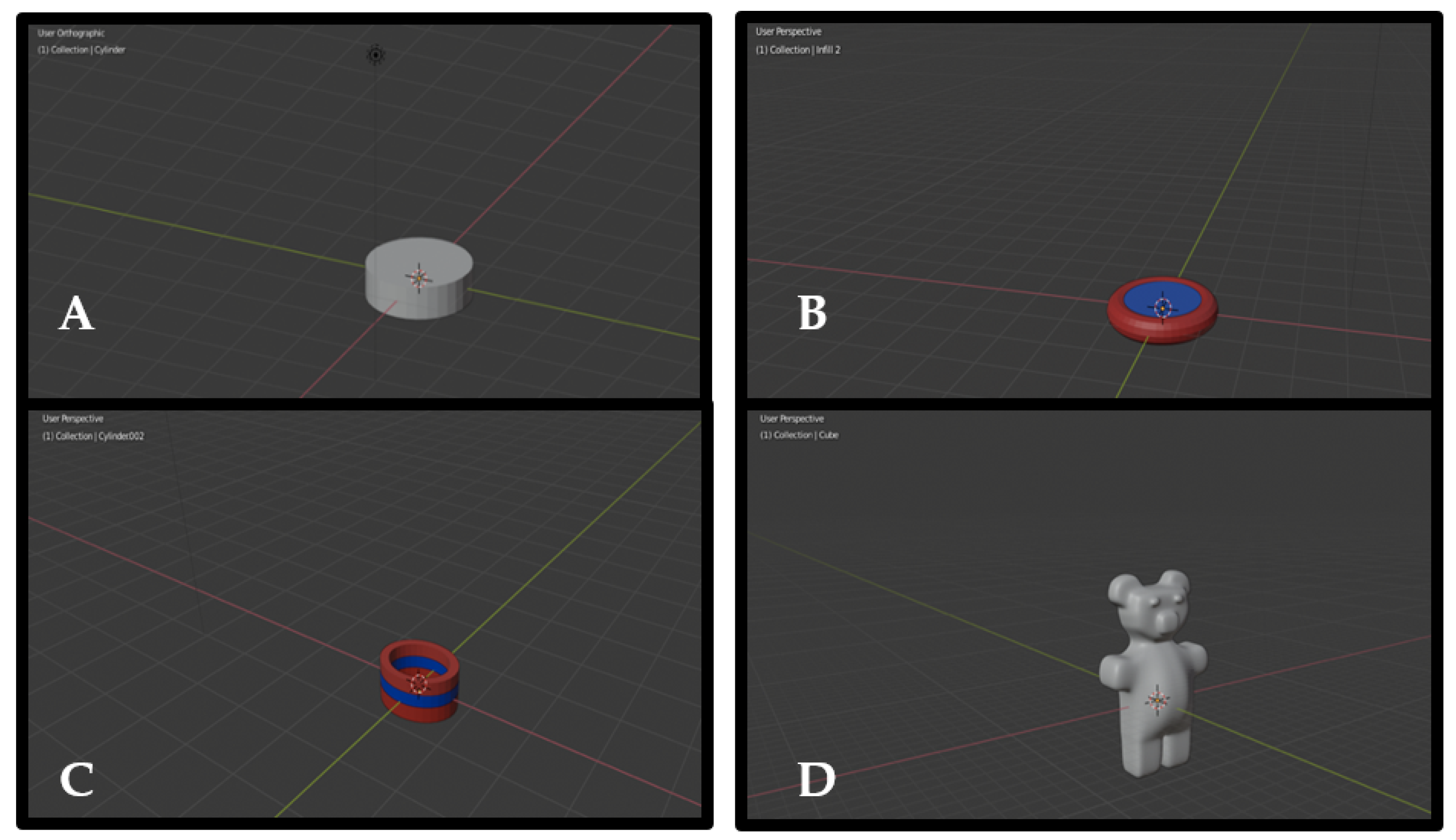
2.2.1. Computer-Aided Design(s) (CAD)
2.2.2. Remote-Fused Deposition Modelling (FDM) 3D Printing
2.2.3. Determination of Physical Properties
3. Results
3.1. Remote Printability
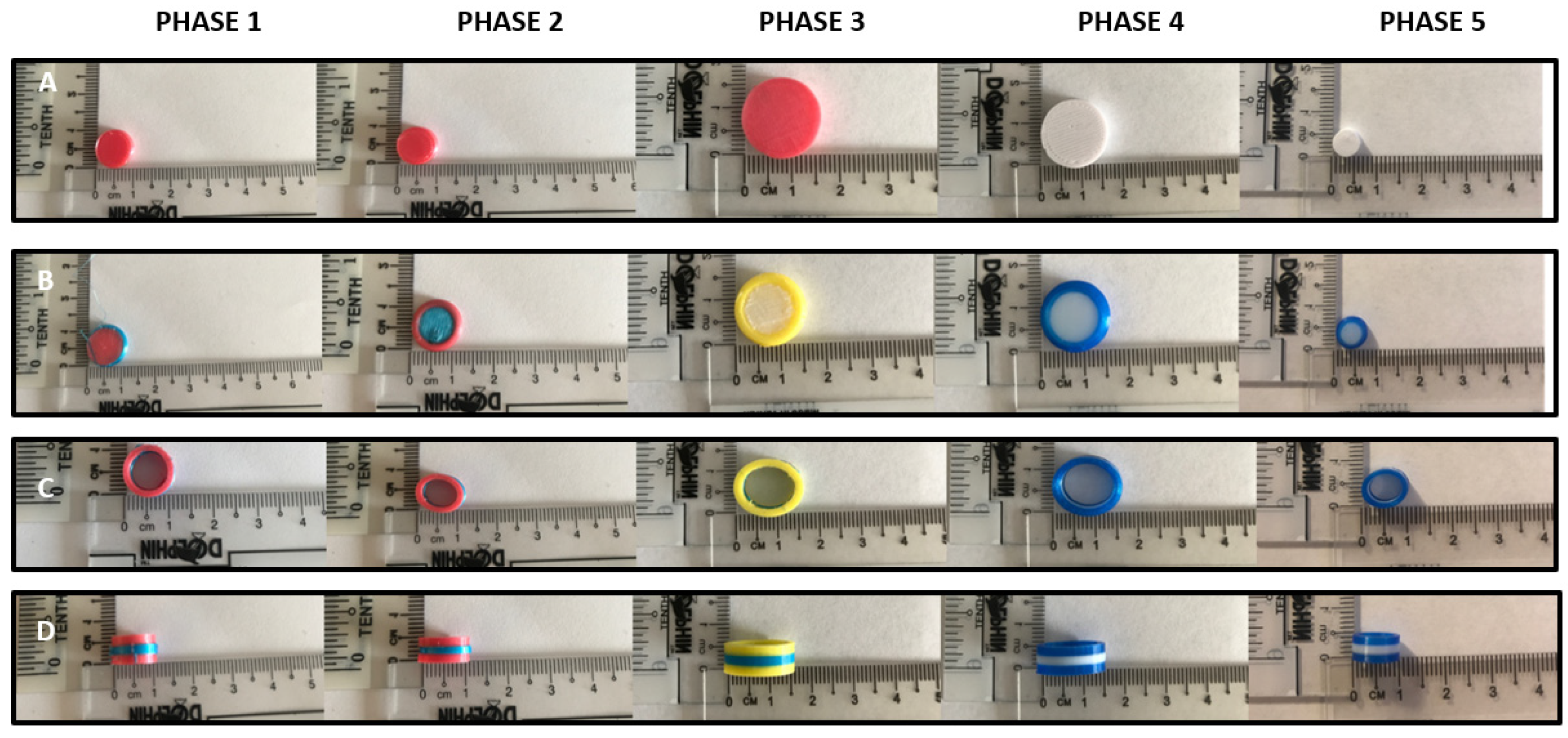
3.2. Visual Observations and Physical Properties of Remotely-Printed Products for Designs 1 to 3
3.3. Design 4—Gummy Bear Shape
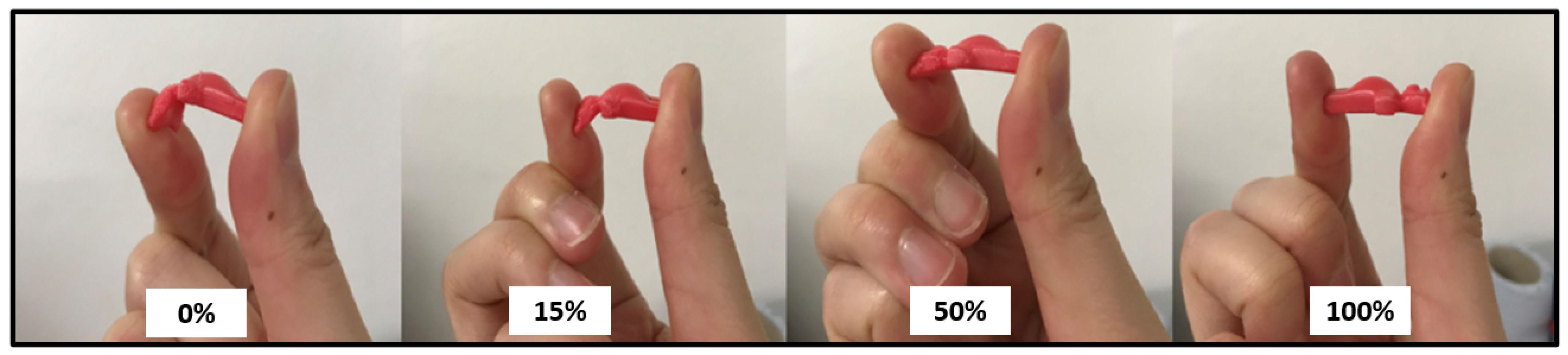
3.4. Design 4—Different Infill Densities
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Tan, D.K.; Maniruzzaman, M.; Nokhodchi, A. Advanced Pharmaceutical Applications of Hot-Melt Extrusion Coupled with Fused Deposition Modelling (FDM) 3D Printing for Personalised Drug Delivery. Pharmaceutics 2018, 10, 203. [Google Scholar] [CrossRef] [Green Version]
- Araújo, M.R.P.; Sa-Barreto, L.L.; Gratieri, T.; Gelfuso, G.M.; Cunha-Filho, M. The Digital Pharmacies Era: How 3D Printing Technology Using Fused Deposition Modeling Can Become a Reality. Pharmaceutics 2019, 11, 128. [Google Scholar] [CrossRef] [Green Version]
- Long, J.; Gholizadeh, H.; Lu, J.; Bunt, C.; Seyfoddin, A. Application of Fused Deposition Modelling (FDM) Method of 3D Printing in Drug Delivery. Curr. Pharm. Des. 2017, 23, 433–439. [Google Scholar] [CrossRef]
- Lim, S.H.; Kathuria, H.; Tan, J.J.Y.; Kang, L. 3D printed drug delivery and testing systems—A passing fad or the future? Adv. Drug Deliv. Rev. 2018, 132, 139–168. [Google Scholar] [CrossRef]
- Madla, C.M.; Trenfield, S.J.; Goyanes, A.; Gaisford, S.; Basit, A.W. 3D Printing technologies, implementation and regulation: An overview. In 3D Printing of Pharmaceuticals, 1st ed.; Basit, A., Gaisford, S., Eds.; Springer: London, UK, 2018; Volume 31, pp. 21–40. [Google Scholar]
- U.S. Department of Health and Human Services; Food and Drug Administration; Center for Devices and Radiological Health; Center for Biologics Evaluation and Research. Technical Considerations for Additive Manufactured Medical Devices: Guidance for Industry and Food and Drug Administration Staff; Center for Biologics Evaluation and Research: Silver Spring, MD, USA, 2017.
- Mirza, M.A.; Iqbal, Z. 3D Printing in Pharmaceuticals: Regulatory Perspective. Curr. Pharm. Des. 2018, 24, 5081–5083. [Google Scholar] [CrossRef]
- Doarn, C.R.; Merrell, R.C. Accessibility and Vulnerabilty: Ensuring Security of Data in Telemedicine. Telemed. e-Health 2015, 21, 143–144. [Google Scholar] [CrossRef]
- Ahmed, S.; Sanghvi, K.; Yeo, D. Telemedicine takes centre stage during COVID-19 pandemic. BMJ Innov. 2020, 6, 252–254. [Google Scholar] [CrossRef]
- Jalali, M.S.; Landman, A.; Gordon, W.J. Telemedicine, privacy, and information security in the age of COVID-19. J. Am. Med. Inform. Assoc. 2021, 28, 671–672. [Google Scholar] [CrossRef]
- Montelongo, A.; Becker, J.L.; Roman, R.; de Oliveira, E.B.; Umpierre, R.N.; Gonçalves, M.R.; Silva, R.; Doniec, K.; Yetisen, A.K. The management of COVID-19 cases through telemedicine in Brazil. PLoS ONE 2021, 16, e02543399. [Google Scholar] [CrossRef]
- DEFEND3D Official Website. Available online: https://www.defend3d.com/#about (accessed on 1 December 2021).
- Trenfield, S.J.; Madla, C.M.; Basit, A.W.; Gaisford, S. The shape of things to come: Emerging applications of 3D printing in healthcare. In 3D Printing of Pharmaceuticals, 1st ed.; Basit, A., Gaisford, S., Eds.; Springer: London, UK, 2018; Volume 31, pp. 1–19. [Google Scholar]
- Fastø, M.M.; Genina, N.; Kaae, S.; Kälvemark Sporrong, S. Perceptions, preferences and acceptability of patient designed 3D printed medicine by polypharmacy patients: A pilot study. Int. J. Clin. Pharm. 2019, 41, 1290–1298. [Google Scholar] [CrossRef]
- Ranmal, S.R.; Cram, A.; Tuleu, C. Age-appropriate and acceptable paediatric dosage forms: Insights into end-user perceptions, preferences and practices from the Children′s Acceptability of Oral Formulations (CALF) Study. Int. J. Pharm. 2016, 514, 296–307. [Google Scholar] [CrossRef] [PubMed]
- Jain, A.; Bansal, K.K.; Tiwari, A.; Rosling, A.; Rosenholm, J.M. Role of Polymers in 3D Printing Technology for Drug Delivery—An Overview. Curr. Pharm. Des. 2018, 24, 4979–4990. [Google Scholar] [CrossRef] [PubMed]
- Baran, E.H.; Erbil, H.Y. Surface Modification of 3D Printed PLA Objects by Fused Deposition Modeling: A Review. Colloids Interfaces 2019, 3, 43. [Google Scholar] [CrossRef] [Green Version]
- Van den Eynde, M.; van Puyvelde, P. 3D Printing of Poly(lactic acid), in Industrial Applications of Poly(lactic acid); di Lorenzo, M.L., Androsch, R., Eds.; Springer International Publishing: Cham, Switzerland, 2018; pp. 139–158. [Google Scholar]
- Mazzanti, V.; Malagutti, L.; Mollica, F. FDM 3D Printing of Polymers Containing Natural Fillers: A Review of their Mechanical Properties. Polymers 2019, 11, 1094. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goyanes, A.; Scarpa, M.; Kamlow, M.; Gaisford, S.; Basit, A.W.; Orlu, M. Patient acceptability of 3D printed medicines. Int. J. Pharm. 2017, 530, 71–78. [Google Scholar] [CrossRef]
- Guideline on Clinical Development of Fixed Combination Medicinal Products. 2017. Available online: https://www.ema.europa.eu/en/clinical-development-fixed-combination-medicinal-products (accessed on 14 December 2021).
- Chew, S.L.; de Mohac, L.M.; Raimi-Abraham, B.T. 3D-Printed Solid Dispersion Drug Products. Pharmaceutics 2019, 11, 672. [Google Scholar] [CrossRef] [Green Version]
- Gerrard, S.E.; Walsh, J.; Bowers, N.; Salunke, S.; Hershenson, S. Innovations in Pediatric Drug Formulations and Administration Technologies for Low Resource Settings. Pharmaceutics 2019, 11, 518. [Google Scholar] [CrossRef] [Green Version]
- Pravin, S.; Sudhir, A. Integration of 3D printing with dosage forms: A new perspective for modern healthcare. Biomed. Pharmacother. 2018, 107, 146–154. [Google Scholar] [CrossRef]
- Chung, M.; Radacsi, N.; Robert, C.; McCarthy, E.D.; Callanan, A.; Conlisk, N.; Hoskins, P.R.; Koutsos, V. On the optimization of low-cost FDM 3D printers for accurate replication of patient-specific abdominal aortic aneurysm geometry. 3D Print. Med. 2018, 4, 2. [Google Scholar] [CrossRef] [Green Version]
- Arnold, C.; Monsees, D.; Hey, J.; Schweyen, R. Surface Quality of 3D-Printed Models as a Function of Various Printing Parameters. Materials 2019, 12, 1970. [Google Scholar] [CrossRef] [Green Version]
- Liu, F.; Ranmal, S.; Batchelor, H.K.; Orlu-Gul, M.; Ernest, T.B.; Thomas, I.W.; Flanagan, T.; Tuleu, C. Patient-centred pharmaceutical design to improve acceptability of medicines: Similarities and differences in paediatric and geriatric populations. Drugs 2014, 74, 1871–1889. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kuznetsov, V.E.; Solonin, A.N.; Urzhumtsev, O.D.; Schilling, R.; Tavitov, A.G. Strength of PLA Components Fabricated with Fused Deposition Technology Using a Desktop 3D Printer as a Function of Geometrical Parameters of the Process. Polymers 2018, 10, 313. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mogan, Y.P. Thermoplastic Elastomer Infill Pattern Impact on Mechanical Properties 3D Printed Customized Orthotic Insole. 2015. Available online: https://www.semanticscholar.org/paper/THERMOPLASTIC-ELASTOMER-INFILL-PATTERN-IMPACT-ON-3D-mogan/09914aeb177ebeebe9c1d13aa990f394d2b3bccc (accessed on 14 December 2021).
- 3D Printing and Intellectual Property Futures. I.P. Office. Available online: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/757767/3D-printing.pdf (accessed on 14 December 2021).
- Cunha-Filho, M.; Araújo, M.R.; Gelfuso, G.M.; Gratieri, T. FDM 3D printing of modified drug-delivery systems using hot melt extrusion: A new approach for individualized therapy. Ther. Deliv. 2017, 8, 957–966. [Google Scholar] [CrossRef] [PubMed]
- Azad, M.A.; Olawuni, D.; Kimbell, G.; Badruddoza, A.; Hossain, M.S.; Sultana, T. Polymers for Extrusion-Based 3D Printing of Pharmaceuticals: A Holistic Materials-Process Perspective. Pharmaceutics 2020, 12, 124. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Polymer | Printer Type i.e., Single/Dual Extruder | Printing Parameters | ||||
|---|---|---|---|---|---|---|
| Nozzle Extrusion Temperature °C | Base Speed mm/s | Layer Height mm | Infill Density % | |||
| Phase 1 | TPU | Single extruder | 220 | 40 | 0.2 60 | 60 |
| Phase 2 | 210 | 35 | 30 | |||
| Phase 3 | 20 | 0.1 | 0, 15, 50, 100 | |||
| Phase 4 | PLA | Dual extruder | 50 | 15 | ||
| Phase 5 | ||||||
| Equation | Equation Number |
|---|---|
| (1) | |
| (2) | |
| (3) | |
| (4) | |
| (5) | |
| (6) | |
| (7) | |
| (8) |
| Diameter ± SD (mm) | Length ± SD (mm) | Thickness ± SD (mm) | Weight (g) | 2D Surface Area (mm2) | Theoretical Surface Area (mm2) | Theoretical Volume (mm3) | |
|---|---|---|---|---|---|---|---|
| Design 1 | |||||||
| Phase 1 | 10.00 ± 0.71 | 10.00 ± 0.71 | 4.50 ± 0.00 | 0.28 | 1.38 | 298.45 | 353.43 |
| Phase 2 | 10.00 ± 0.00 | 10.00 ± 0.00 | 4.50 ± 0.07 | 0.26 | 1.35 | 298.45 | 353.43 |
| Phase 3 | 16.00 ± 0.00 | 16.00 ± 0.71 | 6.00 ± 0.71 | 0.67 | 5.53 | 703.72 | 1206.37 |
| Phase 4 | 15.00 ± 0.00 | 15.00 ± 0.00 | 6.00 ± 0.00 | 0.85 | 4.11 | 636.17 | 1060.29 |
| Phase 5 | 6.00 ± 0.00 | 6.00 ± 0.00 | 3.00 ± 0.00 | 0.09 | 0.68 | 113.10 | 84.82 |
| Design 2 | |||||||
| Phase 1 | 12.00 ± 0.71 | 12.00 ± 0.71 | 3.00 ± 1.41 | 0.37 | 1.33 | 339.29 | 339.29 |
| Phase 2 | 12.00 ± 0.71 | 12.00 ± 0.71 | 3.00 ± 1.41 | 0.43 | 2.27 | 339.39 | 339.39 |
| Phase 3 | 15.00 ± 0.71 | 15.00 ± 0.71 | 6.00 ± 1.41 | 0.89 | 4.37 | 636.17 | 1060.29 |
| Phase 4 | 14.00 ± 0.00 | 14.00 ± 0.00 | 5.00 ± 0.71 | 0.81 | 4.49 | 527.79 | 769.69 |
| Phase 5 | 8.00 ± 2.12 | 8.00 ± 2.12 | 3.00 ± 0.71 | 0.11 | 0.77 | 175.93 | 150.80 |
| Design 3 | |||||||
| Phase 1 | 11.00 ± 0.00 | 11.00 ± 0.00 | 6.00 ± 0.71 | 0.26 | 2.21 | 1.40 | 146.08 |
| Phase 2 | 11.00 ± 0.00 | 11.00 ± 0.00 | 5.00 ± 0.00 | 0.33 | 1.62 | 1.37 | 175.93 |
| Phase 3 | 13.00 ± 1.41 | 16.00 ± 0.71 | 6.00 ± 0.71 | 0.49 | 3.31 | 2.56 | 164.93 |
| Phase 4 | 13.00 ± 0.71 | 16.00 ± 0.00 | 5.00 ± 0.71 | 0.43 | 3.52 | 2.19 | 155.50 |
| Phase 5 | 8.00 ± 0.00 | 10.00 ± 0.00 | 5.00 ± 0.71 | 0.14 | 1.61 | 1.41 | 75.40 |
| DESIGN 4 | Diameter (mm) | Length (mm) | Thickness (mm) | Weight (g) | 2D Surface Area (mm2) | Theoretical Surface Area (mm2) | Theoretical Volume (mm3) |
|---|---|---|---|---|---|---|---|
| Phase 1 | 15.00 ± 0.00 | 25.00 ± 0.71 | 2.00 ± 0.71 | 0.67 | 3.16 | 910.00 | 750.00 |
| Phase 2 | 15.00 ± 0.00 | 26.00 ± 0.00 | 4.00 ± 0.00 | 0.60 | 4.27 | 1168.00 | 1664.00 |
| Phase 3 | 14.00 ± 0.71 | 24.00 ± 0.00 | 3.00 ± 0.35 | 0.58 | 3.92 | 900.00 | 1008.00 |
| Phase 4 | 15.00 ± 0.71 | 24.00 ± 0.00 | 3.00 ± 0.35 | 0.97 | 4.25 | 954.00 | 1080.00 |
| Phase 5 | 10.00 ± 0.35 | 15.00 ± 0.00 | 3.00 ± 0.71 | 0.21 | 1.84 | 450.00 | 450.00 |
| Infill Densities | Diameter (mm) | Length (mm) | Thickness (mm) | Weight (g) | 2D Surface Area (mm2) | Theoretical Surface Area (mm2) | Theoretical Volume (mm3) |
|---|---|---|---|---|---|---|---|
| 0% | 14.00 ± 0.71 | 24.00 ± 0.00 | 3.00 ± 0.35 | 0.58 | 3.92 | 900.00 | 1008.00 |
| 15% | 14.00 ± 0.71 | 24.00 ± 0.71 | 3.00 ± 0.00 | 0.62 | 2.69 | 900.00 | 1008.00 |
| 50% | 13.00 ± 0.00 | 24.00 ± 0.00 | 3.00 ± 0.00 | 0.67 | 3.20 | 846.00 | 936.00 |
| 100% | 14.00 ± 0.00 | 25.00 ± 0.71 | 3.00 ± 0.35 | 1.16 | 3.65 | 934.00 | 1050.00 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kok, X.W.; Singh, A.; Raimi-Abraham, B.T. A Design Approach to Optimise Secure Remote Three-Dimensional (3D) Printing: A Proof-of-Concept Study towards Advancement in Telemedicine. Healthcare 2022, 10, 1114. https://doi.org/10.3390/healthcare10061114
Kok XW, Singh A, Raimi-Abraham BT. A Design Approach to Optimise Secure Remote Three-Dimensional (3D) Printing: A Proof-of-Concept Study towards Advancement in Telemedicine. Healthcare. 2022; 10(6):1114. https://doi.org/10.3390/healthcare10061114
Chicago/Turabian StyleKok, Xiao Wen, Anisha Singh, and Bahijja Tolulope Raimi-Abraham. 2022. "A Design Approach to Optimise Secure Remote Three-Dimensional (3D) Printing: A Proof-of-Concept Study towards Advancement in Telemedicine" Healthcare 10, no. 6: 1114. https://doi.org/10.3390/healthcare10061114
APA StyleKok, X. W., Singh, A., & Raimi-Abraham, B. T. (2022). A Design Approach to Optimise Secure Remote Three-Dimensional (3D) Printing: A Proof-of-Concept Study towards Advancement in Telemedicine. Healthcare, 10(6), 1114. https://doi.org/10.3390/healthcare10061114