
A Transfer Learning Approach with a Convolutional Neural Network for the Classification of Lung Carcinoma




Abstract
:1. Introduction
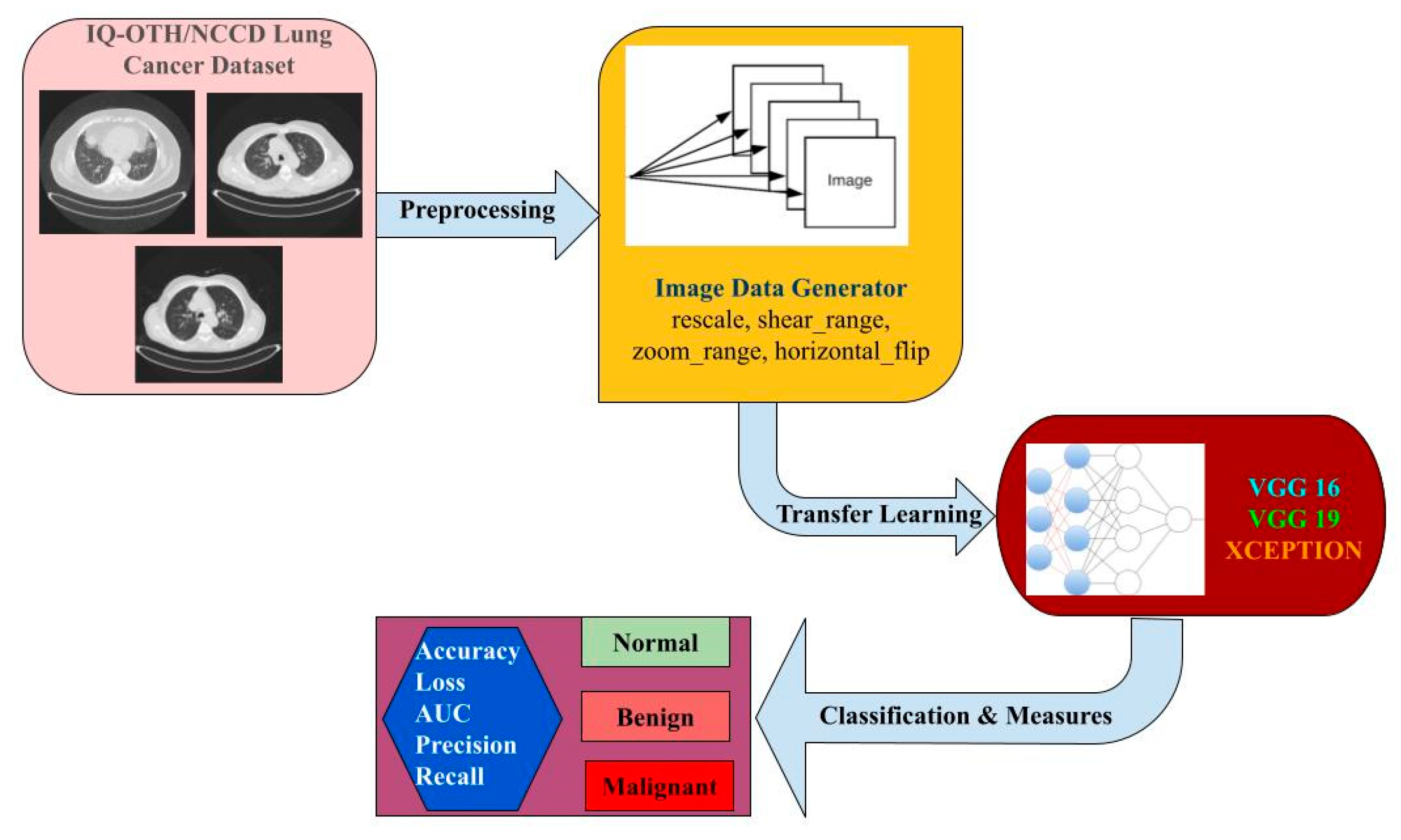
- We have designed a model which can classify the patients’ level of lung carcinoma by applying the TL process, and it is the first of the type to be carried out with this dataset [4].
- Using CT images as the system’s input, it can predict the level and helps to take contour action at the earliest time.
- We have applied three TL approaches here, namely VGG16, VGG19, and Xception, with 20 epochs in the Google Colab platform, and it was shown to be a better model to use for future prediction.
- Based on the experimental performance for lung carcinoma, VGG16 gives maximum accuracy of 98.83%, whereas Xception shows an accuracy rate of 97.4%.
2. Related Work
3. Workflow Architecture
3.1. Dataset Description
3.2. Image Data Generator
3.3. TL
3.4. Fine-Tuned Hyperparameters
3.4.1. Accuracy
| ACTUAL VALUES | ||||
| Normal | Benign | Malignant | ||
| PREDICTED VALUES | Normal | +ve 1 | −ve 2 | −ve 3 |
| Benign | −ve 4 | +ve 5 | −ve 6 | |
| Malignant | −ve 7 | −ve 8 | +ve 9 | |
- TP = Cell1
- FP = Cell2 + Cell3
- TN = Cell5 + Cell6 + Cell8 + Cell9
- FN = Cell4 + Cell7
- TP = Cell5
- FP = Cell4 + Cell6
- TN = Cell1 + Cell3 + Cell7 + Cell9
- FN = Cell2 + Cell8
- TP = Cell9
- FP = Cell7 + Cell8
- TN = Cell1 + Cell2 + Cell4 + Cell5
- FN = Cell3 + Cell6
- TP—True Positive—predict yes and have lung carcinoma
- TN—True Negative—correctly predict that they have no lung carcinoma
- FP—False Positive—incorrectly predict having lung carcinoma but no lung carcinoma (type 1 error)
- FN—False Negative—predict no lung carcinoma but have lung carcinoma (type 2 error)
3.4.2. Loss
3.4.3. AUC
3.4.4. Precision
3.4.5. Recall
3.4.6. F1 Score
4. Experimental Discussion and Analysis
4.1. VGG 16
4.2. VGG 19
4.3. Xception
5. Conclusions and Future Work
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Nall, R. What to Know about Lung Cancer. Medical News Today. 2018. Available online: https://www.medicalnewstoday.com/articles/323701 (accessed on 2 April 2022).
- Saeed, S.; Jhanjhi, N.Z.; Naqvi, M.; Humyun, M.; Ahmad, M.; Gaur, L. Optimized Breast Cancer Premature Detection Method with Computational Segmentation: A Systematic Review Mapping. In Approaches and Applications of Deep Learning in Virtual Medical Care; IGI Global: Harrisburg, PA, USA, 2022; pp. 24–51. [Google Scholar]
- Facts About Lung Cancer. Available online: https://www.lungcancerresearchfoundation.org/lung-cancer-facts/ (accessed on 27 March 2022).
- Shukla, D. New Test May Quickly Detect Early-Stage Lung Cancer. Medical News Today. 2022. Available online: https://www.medicalnewstoday.com/articles/new-test-may-quickly-detect-early-stage-lung-cancer (accessed on 28 March 2022).
- Zhou, Y.; Lu, Y.; Pei, Z. Accurate diagnosis of early lung cancer based on the convolutional neural network model of the embedded medical system. Microprocess. Microsyst. 2021, 81, 103754. [Google Scholar] [CrossRef]
- Nanglia, P.; Kumar, S.; Mahajan, A.N.; Singh, P.; Rathee, D. A hybrid algorithm for lung cancer classification using SVM and Neural Networks. ICT Express 2021, 7, 335–341. [Google Scholar] [CrossRef]
- Bai, Y.; Li, D.; Duan, Q.; Chen, X. Analysis of high-resolution reconstruction of medical images based on deep convolutional neural networks in lung cancer diagnostics. Comput. Methods Programs Biomed. 2022, 217, 106592. [Google Scholar] [CrossRef]
- Ahmad, A.S.; Mayya, A.M. A new tool to predict lung cancer based on risk factors. Heliyon 2020, 6, e03402. [Google Scholar] [CrossRef]
- Ahn, B.-C.; So, J.-W.; Synn, C.-B.; Kim, T.H.; Kim, J.H.; Byeon, Y.; Kim, Y.S.; Heo, S.G.; Yang, S.D.; Yun, M.R.; et al. Clinical decision support algorithm based on machine learning to assess the clinical response to anti–programmed death-1 therapy in patients with non–small-cell lung cancer. Eur. J. Cancer 2021, 153, 179–189. [Google Scholar] [CrossRef]
- Agarwal, S.; Yadav, A.S.; Dinesh, V.; Vatsav, K.S.S.; Prakash, K.S.S.; Jaiswal, S. By artificial intelligence algorithms and machine learning models to diagnosis cancer. Mater. Today Proc. 2021. [Google Scholar] [CrossRef]
- Huang, X.; Lei, Q.; Xie, T.; Zhang, Y.; Hu, Z.; Zhou, Q. Deep transfer convolutional neural network and extreme learning machine for lung nodule diagnosis on CT images. Knowl.-Based Syst. 2020, 204, 106230. [Google Scholar] [CrossRef]
- Doppalapudi, S.; Qiu, R.G.; Badr, Y. Lung cancer survival period prediction and understanding: Deep learning approaches. Int. J. Med. Inform. 2021, 148, 104371. [Google Scholar] [CrossRef]
- Ashraf, S.F.; Yin, K.; Meng, C.X.; Wang, Q.; Wang, Q.; Pu, J.; Dhupar, R. Predicting benign, preinvasive, and invasive lung nodules on computed tomography scans using machine learning. J. Thorac. Cardiovasc. Surg. 2022, 163, 1496–1505. [Google Scholar] [CrossRef]
- Shakeel, P.M.; Burhanuddin, M.A.; Desa, M.I. Lung cancer detection from CT image using improved profuse clustering and deep learning instantaneously trained neural networks. Measurement 2019, 145, 702–712. [Google Scholar] [CrossRef]
- ALzubi, J.A.; Bharathikannan, B.; Tanwar, S.; Manikandan, R.; Khanna, A.; Thaventhiran, C. Boosted neural network ensemble classification for lung cancer disease diagnosis. Appl. Soft Comput. 2019, 80, 579–591. [Google Scholar] [CrossRef]
- Alyasriy, H. The IQ-OTHNCCD Lung Cancer Dataset. Mendeley Data, Version 1. 2020. Available online: https://data.mendeley.com/datasets/bhmdr45bh2/1 (accessed on 28 March 2022).
- Szegedy, C.; Toshev, A.; Erhan, D. Deep neural networks for object detection. In Advances in Neural Information Processing Systems, Proceedings of the 26th International Conference on Neural Information Processing Systems, Nevada City, CA, USA, 5–10 December 2013; Morgan Kaufmann Publishers: San Francisco, CA, USA, 2013; Volume 26. [Google Scholar]
- Yu, X.; Wang, J.; Hong, Q.Q.; Teku, R.; Wang, S.H.; Zhang, Y.D. Transfer learning for medical images analyses: A survey. Neurocomputing 2022, 489, 230–254. [Google Scholar] [CrossRef]
- Hand, D.J.; Till, R.J. A simple generalisation of the area under the ROC curve for multiple class classification problems. Mach. Learn. 2001, 45, 171–186. [Google Scholar] [CrossRef]
- Ferri, C.; Hernández-Orallo, J.; Modroiu, R. An experimental comparison of performance measures for classification. Pattern Recognit. Lett. 2009, 30, 27–38. [Google Scholar] [CrossRef]
- Humayun, M.; Alsayat, A. Prediction Model for Coronavirus Pandemic Using Deep Learning. Comput. Syst. Sci. Eng. 2022, 40, 947–961. [Google Scholar] [CrossRef]
- Khalil, M.I.; Humayun, M.; Jhanjhi, N.; Talib, M.; Tabbakh, T.A. Multi-class Segmentation of Organ at Risk from Abdominal CT Images: A Deep Learning Approach. In Intelligent Computing and Innovation on Data Science; Peng, S.L., Hsieh, S.Y., Gopalakrishnan, S., Duraisamy, B., Eds.; Springer: Berlin, Germany, 2021; pp. 425–434. [Google Scholar]
- Gouda, W.; Almurafeh, M.; Humayun, M.; Jhanjhi, N.Z. Detection of COVID-19 Based on Chest X-rays Using Deep Learning. Healthcare 2022, 10, 343. [Google Scholar] [CrossRef]
- Khalil, M.I.; Tehsin, S.; Humayun, M.; Jhanjhi, N.; AlZain, M.A. Multi-Scale Network for Thoracic Organs Segmentation. CMC-Comput. Mater. Contin. 2022, 70, 3251–3265. [Google Scholar] [CrossRef]
- Cheng, S.; Zhou, G. Facial expression recognition method based on improved VGG convolutional neural network. Int. J. Pattern Recognit. Artif. Intell. 2020, 34, 2056003. [Google Scholar] [CrossRef]
- Tammina, S. Transfer learning using VGG-16 with deep convolutional neural network for classifying images. Int. J. Sci. Res. Publ. IJSRP 2019, 9, 143–150. [Google Scholar] [CrossRef]
- VGG-16: CNN Model. Available online: https://www.geeksforgeeks.org/vgg-16-cnn-model/ (accessed on 27 March 2022).
- Simonyan, K.; Zisserman, A. Very deep convolutional networks for large-scale image recognition. arXiv 2014, arXiv:1409.1556. [Google Scholar]
- Chollet, F. Xception: Deep learning with depthwise separable convolutions. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, Honolulu, HI, USA, 21–26 July 2017; pp. 1251–1258. [Google Scholar]
- Kareem, H.F.; AL-Husieny, M.S.; Mohsen, F.Y.; Khalil, E.A.; Hassan, Z.S. Evaluation of SVM Performance in the Detection of Lung Cancer in Marked CT Scan Dataset. Indones. J. Electr. Eng. Comput. Sci. 2021, 21, 1731–1738. [Google Scholar] [CrossRef]
- Amiripallia, S.S.; Rao, G.N.; Beharaa, J.; Sanjay, K. Mineral Rock Classification Using Convolutional Neural Network. In Recent Trends in Intensive Computing; IOS Press: Amsterdam, The Netherlands, 2021. [Google Scholar]

















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Epochs | Loss | Accuracy | AUC | Precision | Recall | F1 Score |
|---|---|---|---|---|---|---|
| 1 | 1.1475 | 0.6641 | 0.8333 | 0.6711 | 0.6562 | 0.6636 |
| 5 | 0.1522 | 0.9531 | 0.996 | 0.9601 | 0.9401 | 0.9500 |
| 10 | 0.0826 | 0.9831 | 0.9993 | 0.9831 | 0.9831 | 0.9831 |
| 15 | 0.0625 | 0.9844 | 0.9995 | 0.9856 | 0.9831 | 0.9843 |
| 20 | 0.0508 | 0.9883 | 0.9994 | 0.9883 | 0.9857 | 0.9870 |
| Epochs | Loss | Accuracy | AUC | Precision | Recall | F1 Score |
|---|---|---|---|---|---|---|
| 1 | 0.4963 | 0.8645 | 0.9409 | 0.882 | 0.8435 | 0.8623 |
| 5 | 0.4626 | 0.8274 | 0.9454 | 0.8394 | 0.8177 | 0.8284 |
| 10 | 0.4851 | 0.8645 | 0.9472 | 0.8695 | 0.8597 | 0.8646 |
| 15 | 0.6248 | 0.8145 | 0.923 | 0.8139 | 0.8113 | 0.8126 |
| 20 | 0.5997 | 0.8339 | 0.939 | 0.8363 | 0.8323 | 0.8343 |
| Epochs | Loss | Accuracy | AUC | Precision | Recall | F1 Score |
|---|---|---|---|---|---|---|
| 1 | 1.0643 | 0.681 | 0.8486 | 0.7093 | 0.6641 | 0.6860 |
| 5 | 0.2821 | 0.8984 | 0.9783 | 0.913 | 0.888 | 0.9003 |
| 10 | 0.115 | 0.9648 | 0.9978 | 0.9737 | 0.9635 | 0.9686 |
| 15 | 0.0785 | 0.9857 | 0.9992 | 0.9857 | 0.9857 | 0.9857 |
| 20 | 0.0658 | 0.9805 | 0.9992 | 0.9804 | 0.9766 | 0.9785 |
| Epochs | Loss | Accuracy | AUC | Precision | Recall | F1 Score |
|---|---|---|---|---|---|---|
| 1 | 1.5413 | 0.3032 | 0.5908 | 0.289 | 0.2661 | 0.2771 |
| 5 | 0.4545 | 0.8903 | 0.9494 | 0.8988 | 0.8742 | 0.8863 |
| 10 | 0.5633 | 0.8129 | 0.9296 | 0.823 | 0.8097 | 0.8163 |
| 15 | 0.6081 | 0.7968 | 0.9319 | 0.798 | 0.7839 | 0.7909 |
| 20 | 0.6524 | 0.8097 | 0.9262 | 0.811 | 0.8097 | 0.8103 |
| Epochs | Loss | Accuracy | AUC | Precision | Recall | F1 Score |
|---|---|---|---|---|---|---|
| 1 | 0.4247 | 0.9583 | 0.9805 | 0.9583 | 0.9583 | 0.9583 |
| 5 | 0.1418 | 0.9792 | 0.9928 | 0.9792 | 0.9792 | 0.9792 |
| 10 | 0.2022 | 0.9753 | 0.9897 | 0.9753 | 0.9753 | 0.9753 |
| 15 | 0.1218 | 0.9779 | 0.9946 | 0.9779 | 0.9779 | 0.9779 |
| 20 | 0.1238 | 0.974 | 0.9927 | 0.974 | 0.974 | 0.974 |
| Epochs | Loss | Accuracy | AUC | Precision | Recall | F1 Score |
|---|---|---|---|---|---|---|
| 1 | 3.5571 | 0.7935 | 0.8709 | 0.7935 | 0.7935 | 0.7935 |
| 5 | 2.7582 | 0.8597 | 0.9236 | 0.8597 | 0.8597 | 0.8597 |
| 10 | 4.0757 | 0.8129 | 0.8893 | 0.8129 | 0.8129 | 0.8129 |
| 15 | 3.2605 | 0.8645 | 0.9207 | 0.8643 | 0.8643 | 0.8643 |
| 20 | 3.5682 | 0.8968 | 0.9338 | 0.8968 | 0.8968 | 0.8968 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Humayun, M.; Sujatha, R.; Almuayqil, S.N.; Jhanjhi, N.Z. A Transfer Learning Approach with a Convolutional Neural Network for the Classification of Lung Carcinoma. Healthcare 2022, 10, 1058. https://doi.org/10.3390/healthcare10061058
Humayun M, Sujatha R, Almuayqil SN, Jhanjhi NZ. A Transfer Learning Approach with a Convolutional Neural Network for the Classification of Lung Carcinoma. Healthcare. 2022; 10(6):1058. https://doi.org/10.3390/healthcare10061058
Chicago/Turabian StyleHumayun, Mamoona, R. Sujatha, Saleh Naif Almuayqil, and N. Z. Jhanjhi. 2022. "A Transfer Learning Approach with a Convolutional Neural Network for the Classification of Lung Carcinoma" Healthcare 10, no. 6: 1058. https://doi.org/10.3390/healthcare10061058
APA StyleHumayun, M., Sujatha, R., Almuayqil, S. N., & Jhanjhi, N. Z. (2022). A Transfer Learning Approach with a Convolutional Neural Network for the Classification of Lung Carcinoma. Healthcare, 10(6), 1058. https://doi.org/10.3390/healthcare10061058