
COVID-19 Pandemic-Revealed Consistencies and Inconsistencies in Healthcare: A Medical and Organizational View



{kind=link}
{kind=link}
Abstract
:1. Introduction
- -
- Recovery and transformation of national health systems through investment in the essential public health functions and the foundations of the health system, with a focus on the primary healthcare and the incorporation of health security.
- -
- All-hazards emergency risk management, to ensure and accelerate sustainable implementation of the International Health Regulations (2005).
- -
- Whole-of-government approach to ensure community engagement and whole-of-society involvement.
2. Materials and Methods
- The medical aspect.
- The healthcare organization aspect.
3. Results
3.1. Medical Aspect
3.1.1. Chronic Disease Burden
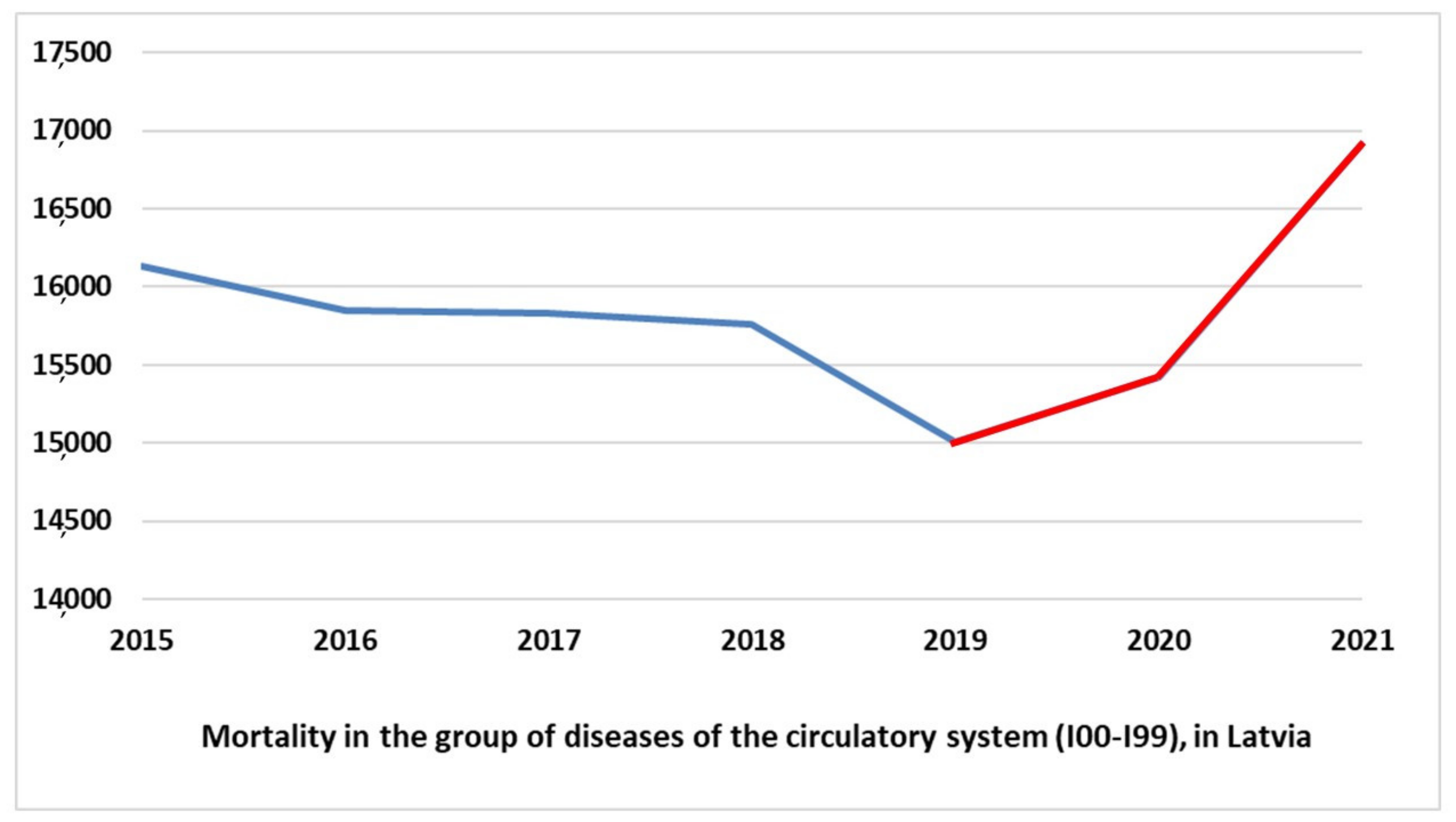
3.1.2. Mortality Rates in Indirect COVID-19-Related Diagnoses
- (1)
- Diseases of the circulatory system (I00-I99, ICD-10)
- (2)
- Neoplasms (C00-D48, ICD-10)
- (3)
- External causes of death (V00-Y98, ICD-10)
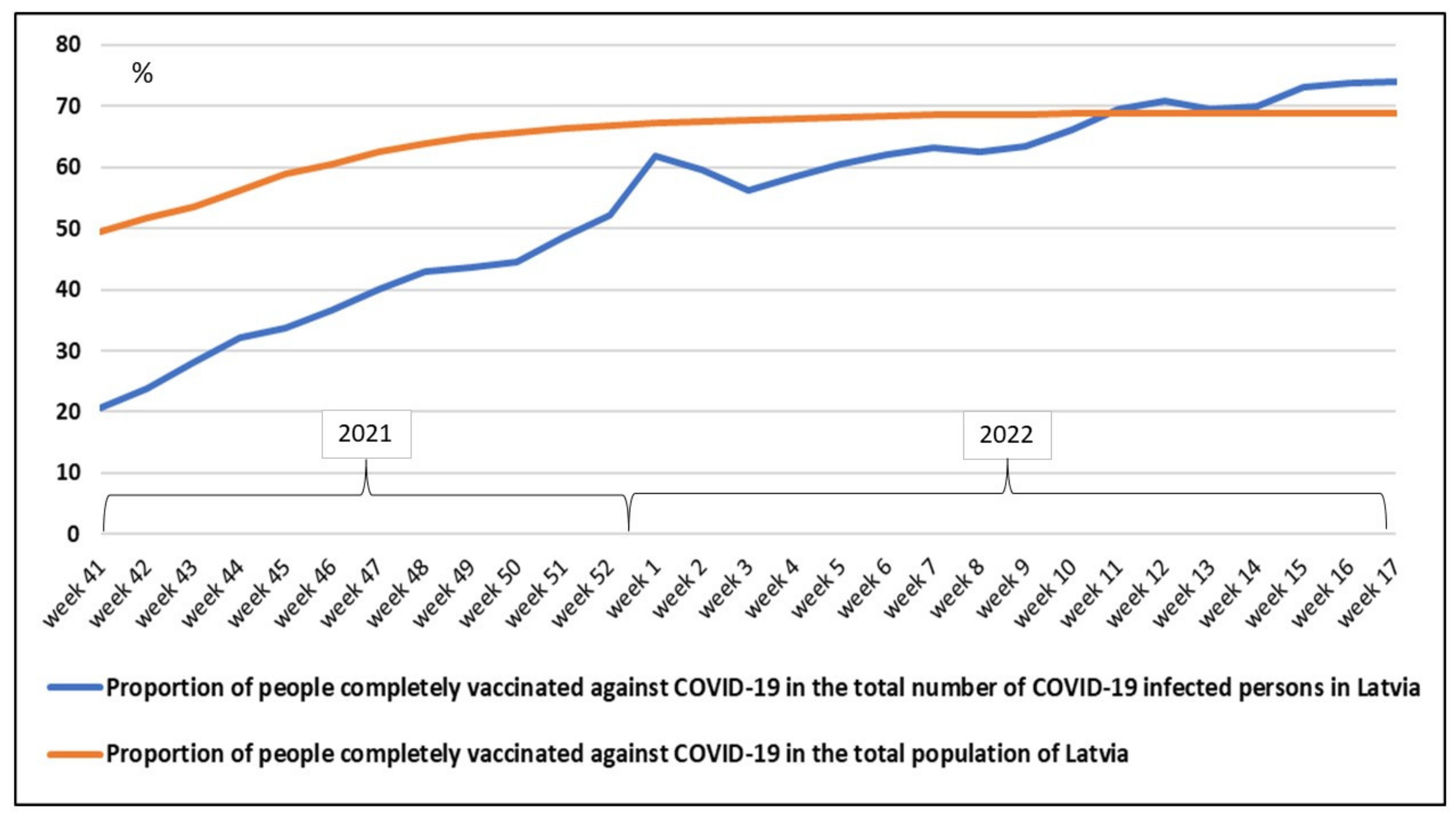
3.1.3. Immunization Tendencies
3.2. The Healthcare Organization Aspect
- Promoting high-value health systems for all
- Adapting health systems to new technologies and innovation
- Reorienting health systems to become more people-centered
- Encouraging dialogue and international co-operation
- Traditional organizational cultures that are hierarchical and controlling need to be challenged and reoriented towards collaborative, inclusive, and participative practices of engagement and involvement. Health systems’ processes must move from a top-down approach to integrative policy, planning, and implementation processes, increasingly adopting a people-centered approach [80,81,82].
- COVID-19 has brought upon us the opportunity to redesign health policy thinking and acting to stimulate new possibilities through critical debate, moving from fragmentation to adaptive self-organization, creating well-integrated, equitable, and prosperous societies resilient to sudden unexpected perturbations of any kind [83,84,85,86].
- A reimagined framework for global health that prioritizes health system integration across Universal Health Coverage and Global Health System holistic domains, innovative and unified health financing, cross-sector resilience indicators, and equity as core values offers a necessary path ahead [87,88,89].
- Resilience in health systems should not be seen as an apolitical outcome, synonymous with a strong health system or improved population health. The resilient healthcare systems should be assessed by considering how macro-level and meso-level structures support adaptive capacity at the micro-level [90,91,92].
- Leadership development must be an established and integrated component of organizations. The gaps were embedded among complex interactions between the health systems’ building blocks. Understanding the complexities in fostering whole-system strengthening through a holistic measure and applying system thinking is crucial [80,85,89],
- Democratic rights, human rights, equity, and ethics values have become prominent in national policy debates. Increased attention to an active community voice and the resources it requires can help practitioners to achieve improved health outcomes and researchers to understand the pathways to health improvement through collaboration [81,93]
- Democratic accountability and the rule of law cannot be completely suspended in any public health emergency. As humanity grapples with COVID-19, the way to combat one pandemic is not to create another, a pandemic of authoritarian rule. Reimagining a narrative should put the collective health and human rights at the center [88,94].
- Establishing the scope of public health is crucial to understanding its role within the larger health system and adds to the discourse around the relationship between public health, healthcare, and population health. Digital transformation must be further driven to ensure collaboration. Holistic, preventive policies must be adapted to local contexts and implemented through strong local health systems able to have the capacity to respond to emergencies [85,90,95,96].
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization. The International Health Regulations (2005), Adopted by the Fifth–Eighth World Health Assembly in May 2005, Entered into Force on 15 June 2007; WHO: Geneva, Switzerland, 2005. [Google Scholar]
- World Health Organization. The International Health Regulations (2005): Areas of Work for Implementation; World Health Organization: Geneva, Switzerland, 2007. [Google Scholar]
- United Nations. Resolution A/RES/67/81 Global Health and Foreign Policy, Adopted by the General Assembly on 12 December 2012. Sixty-Seventh Session Agenda Item 123; United Nations: New York, NY, USA, 2012. [Google Scholar]
- United Nations. Resolution A/RES/70/1 Transforming our World: The 2030 Agenda for Sustainable Development, Adopted by the General Assembly on 25 September 2015. Seventieth Session Agenda Items 15 and 116 15-16301 (E); United Nations: New York, NY, USA, 2015. [Google Scholar]
- Nomura, S.; Kayano, R.; Egawa, S.; Harada, N.; Koido, Y. Expected Scopes of Health Emergency and Disaster Risk Management (Health EDRM): Report on the Expert Workshop at the Annual Conference for the Japanese Association for Disaster Medicine 2020. Int. J. Environ. Res. Public Health 2021, 18, 4447. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Building Health Systems Resilience for Universal Health Coverage and Health Security during the COVID-19 Pandemic and Beyond: WHO Position Paper; World Health Organization: Geneva, Switzerland, 2021. [Google Scholar]
- U.S. Department of Health and Human Services; U.S. Food and Drug Administration. Paving the Way for Personalized Medicine: FDA’s Role in a New Era of Medical Product Development. FDA Report. 2013. Available online: https://www.fdanews.com/ext/resources/files/10/10-28-13-Personalized-Medicine.pdf (accessed on 12 February 2022).
- The Council of the European Union. Council Conclusions on Personalized Medicine for Patients (2015/C 421/03). 2015. Available online: https://eur-lex.europa.eu/legal-content/EN/TXT/PDF/?uri=CELEX:52015XG1217(01)&from=FR (accessed on 12 February 2022).
- Hoffman, S.L.; Rogers, W.O.; Carucci, D.J.; Venter, J.C. From Genomics to Vaccines: Malaria as a Model System. Nat. Med. 1998, 4, 1351–1353. [Google Scholar] [CrossRef] [PubMed]
- Poland, G.A.; Ovsyannikova, I.; Kennedy, R. Personalized Vaccinology: A Review. Vaccine 2018, 36, 5350–5357. [Google Scholar] [CrossRef] [PubMed]
- Whitaker, J.A.; Ovsyannikova, I.G.; Poland, G.A. Adversomics: A New Paradigm for Vaccine Safety and Design. Expert Rev. Vaccines 2015, 14, 935–947. [Google Scholar] [CrossRef] [Green Version]
- Poland, G.A.; Kennedy, R.B.; McKinney, B.A.; Ovsyannikova, I.G.; Lambert, N.D.; Jacobson, R.M.; Oberg, A.L. Vaccinomics, adversomics, and the immune response network theory: Individualized vaccinology in the 21st century. Semin. Immunol. 2013, 25, 89–103. [Google Scholar] [CrossRef] [Green Version]
- Omersel, J.; Karas Kuželički, N. Vaccinomics and Adversomics in the Era of Precision Medicine: A Review Based on HBV, MMR, HPV, and COVID-19 Vaccines. J. Clin. Med. 2020, 9, 3561. [Google Scholar] [CrossRef]
- Saltman, R.B.; Duran, A. Governance, government, and the search for new provider models. Int. J. Health Policy Manag. 2016, 5, 33–42. [Google Scholar] [CrossRef]
- Allocation of Resources to Reduce the Impact of COVID-19. Official Governmental Website of Latvia. Available online: https://covid19.gov.lv/atbalsts-sabiedribai/valsts-atbalsts/finansu-ieguldijums-krizes-parvaresanai/pieskirto-lidzeklu (accessed on 5 April 2022).
- Spending Review of Budget Allocation in Latvia. The Ministry of Finance, Republic of Latvia. Available online: https://www.fm.gov.lv/en/spending-review (accessed on 5 April 2022).
- Pheby, D.F.H.; Araja, D.; Berkis, U.; Brenna, E.; Cullinan, J.; de Korwin, J.-D.; Gitto, L.; Hughes, D.A.; Hunter, R.M.; Trepel, D.; et al. The development of a consistent Europe-wide approach to investigating the economic impact of myalgic encephalomyelitis (ME/CFS): A report from the European Network on ME/CFS (EUROMENE). Healthcare 2020, 8, 88. [Google Scholar] [CrossRef] [Green Version]
- Fernández-de-las-Peñas, C.; Palacios-Ceña, D.; Gómez-Mayordomo, V.; Cuadrado, M.L.; Florencio, L.L. Defining Post-COVID Symptoms (Post-Acute COVID, Long COVID, Persistent Post-COVID): An Integrative Classification. Int. J. Environ. Res. Public Health 2021, 18, 2621. [Google Scholar] [CrossRef]
- Oronsky, B.; Larson, C.; Hammond, T.C.; Oronsky, A.; Kesari, S.; Lybeck, M.; Reid, T.R. A Review of Persistent Post-COVID Syndrome (PPCS). Clinic. Rev. Allerg. Immunol. 2021, 20, 1–9. [Google Scholar] [CrossRef]
- Araja, D.; Berkis, U.; Lunga, A.; Murovska, M. Shadow Burden of Undiagnosed Myalgic Encephalomyelitis/Chronic Fatigue Syndrome (ME/CFS) on Society: Retrospective and Prospective—In Light of COVID-19. J. Clin. Med. 2021, 10, 3017. [Google Scholar] [CrossRef] [PubMed]
- Wong, T.L.; Weitzer, D.J. Long COVID and Myalgic Encephalomyelitis/Chronic Fatigue Syndrome (ME/CFS)—A Systemic Review and Comparison of Clinical Presentation and Symptomatology. Medicina 2021, 57, 418. [Google Scholar] [CrossRef] [PubMed]
- Poenaru, S.; Abdallah, S.J.; Corrales-Medina, V. COVID-19 and post-infectious myalgic encephalomyelitis/chronic fatigue syndrome: A narrative review. Ther. Adv. Infect. Dis. 2021, 8, 20499361211009385. [Google Scholar] [CrossRef] [PubMed]
- Paul, B.D.; Lemle, M.D.; Komaroff, A.L.; Snyder, S.H. Redox imbalance links COVID-19 and myalgic encephalomyelitis/chronic fatigue syndrome. Proc. Natl. Acad. Sci. USA 2021, 118, e2024358118. [Google Scholar] [CrossRef]
- Komaroff, A.L.; Lipkin, W.I. Review Insights from myalgic encephalomyelitis/chronic fatigue syndrome may help unravel the pathogenesis of postacute COVID-19 syndrome. Trends Mol. Med. 2021, 27, 895–906. [Google Scholar] [CrossRef]
- Deumer, U.-S.; Varesi, A.; Floris, V.; Savioli, G.; PACani, E.; López-Carrasco, P.; Rosati, G.M.; Prasad, S.; Ricevuti, G. Myalgic Encephalomyelitis/Chronic Fatigue Syndrome (ME/CFS): An Overview. J. Clin. Med. 2021, 10, 4786. [Google Scholar] [CrossRef]
- Ceban, F.; Ling, S.; Lui, L.M.W.; Lee, Y.; Gill, H.; Teopiz, K.M.; Rodrigues, N.B.; Subramaniapillai, M.; Di Vincenzo, J.D.; Cao, B.; et al. Fatigue and cognitive impairment in Post-COVID-19 Syndrome: A systematic review and meta-analysis. Brain Behav. Immun. 2022, 101, 93–135. [Google Scholar] [CrossRef]
- Rodríguez, P.S.; Espinosa, P.; Aguilar, A.M.; Muñoz, M.P.R.; Navarro, M.Á.R. Long COVID: Is it really myalgic encephalomyelitis? Bibliographic review and considerations. Med. Fam. Semer. 2022, 48, 63–69. (In Spanish) [Google Scholar] [CrossRef]
- González-Hermosillo, J.A.; Martínez-López, J.P.; Carrillo-Lampón, S.A.; Ruiz-Ojeda, D.; Herrera-Ramírez, S.; Amezcua-Guerra, L.M.; Martínez-Alvarado, M.d.R. Post-Acute COVID-19 Symptoms, a Potential Link with Myalgic Encephalomyelitis/Chronic Fatigue Syndrome: A 6-Month Survey in a Mexican Cohort. Brain Sci. 2021, 11, 760. [Google Scholar] [CrossRef]
- Vanichkachorn, G.; Newcomb, R.; Cowl, C.T.; Murad, H.; Breeher, L.; Miller, S.; Trenary, M.; Neveau, D.; Higgins, S. Post–COVID-19 Syndrome (Long Haul Syndrome): Description of a Multidisciplinary Clinic at Mayo Clinic and Characteristics of the Initial Patient Cohort. Mayo Clin. Proc. 2021, 96, 1782–1791. [Google Scholar] [CrossRef]
- Araja, D.; Berkis, U.; Lunga, A.; Murovska, M. Burden of COVID-19 Consequences: An Example of Post-viral Chronic Fatigue Syndrome. Value Health 2021, 24, S149–S150. [Google Scholar] [CrossRef]
- Aly, M.A.E.G.; Saber, H.G. Long COVID and chronic fatigue syndrome: A survey of elderly female survivors in Egypt. Int. J. Clin. Pract. 2021, 75, e14886. [Google Scholar] [CrossRef]
- Moncorps, F.; Jouet, E.; Bayen, S.; Fornasieri, I.; Renet, S.; Las-Vergnas, O.; Messaadi, N. Specifics of chronic fatigue syndrome co-ping strategies identified in a French flash survey during the COVID-19 containment. Health Soc. Care Community 2022, 30, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Petracek, L.S.; Suskauer, S.J.; Vickers, R.F.; Patel, N.R.; Violand, R.L.; Swope, R.L.; Rowe, P.C. Adolescent and Young Adult ME/CFS After Confirmed or Probable COVID-19. Front. Med. 2021, 29, 668944. [Google Scholar] [CrossRef] [PubMed]
- Jason, L.A.; Islam, M.F.; Conroy, K.; Cotler, J.; Torres, C.; Johnson, M.; Mabie, B. COVID-19 symptoms over time: Comparing long-haulers to ME/CFS. Fatigue Biomed. Health Behav. 2021, 9, 59–68. [Google Scholar] [CrossRef] [PubMed]
- Davis, H.E.; Assaf, G.S.; McCorkell, L.; Wei, H.; Low, R.J.; Re’em, Y.; Redfield, S.; Austin, J.P.; Akrami, A. Characterizing long COVID in an international cohort: 7 months of symptoms and their impact. EClinicalMedicine 2021, 38, 101019. [Google Scholar] [CrossRef]
- Murga, I.; Aranburu, L.; Gargiulo, P.A.; Gomez Esteban, J.C.; Lafuente, J.V. Clinical Heterogeneity in ME/CFS. A Way to Understand Long-COVID19 Fatigue. Front. Psychiatry 2021, 12, 735784. [Google Scholar] [CrossRef]
- Pavlia, A.; Theodoridoub, M.; Maltezou, H.C. Post-COVID Syndrome: Incidence, Clinical Spectrum, and Challenges for Primary Healthcare Professionals. Arch. Med. Res. 2021, 52, 575–581. [Google Scholar] [CrossRef]
- Jacobson, K.B.; Rao, M.; Bonilla, H.; Subramanian, A.; Hack, I.; Madrigal, M.; Singh, U.; Jagannathan, P.; Grant, G. Patients with Uncomplicated Coronavirus Disease 2019 (COVID-19) Have Long-Term Persistent Symptoms and Functional Impairment Similar to Patients with Severe COVID-19: A Cautionary Tale During a Global Pandemic. Clin. Infect. Dis. 2021, 73, e826–e829. [Google Scholar] [CrossRef]
- Mancini, D.M.; Brunjes, D.L.; Lala, A.; Trivieri, M.G.; Contreras, J.P.; Natelson, B.H. Use of Cardiopulmonary Stress Testing for Patients with Unexplained Dyspnea Post–Coronavirus Disease. JACC Heart Fail. 2021, 9, 927–937. [Google Scholar] [CrossRef]
- Hohberger, B.; Harrer, T.; Mardin, C.; Kruse, F.; Hoffmanns, J.; Rogge, L.; Heltmann, F.; Moritz, M.; Szewczykowski, C.; Schottenhamml, J.; et al. Case Report: Neutralization of Autoantibodies Targeting G-Protein-Coupled Receptors Improves Capillary Impairment and Fatigue Symptoms After COVID-19 Infection. Front. Med. 2021, 18, 754667. [Google Scholar] [CrossRef] [PubMed]
- Tleyjeh, I.M.; Saddik, B.; Ramakrishnan, R.K.; AlSwaidan, N.; AlAnazi, A.; Alhazmi, D.; Aloufi, A.; AlSumait, F.; Berbari, E.F.; Halwani, R. Long term predictors of breathlessness, exercise intolerance, chronic fatigue and well-being in hospitalized patients with COVID-19: A cohort study with 4 months median follow-up. J. Infect. Public Health 2022, 15, 21–28. [Google Scholar] [CrossRef] [PubMed]
- Tirelli, U.; Franzini, M.; Valdenassi, L.; Pisconti, S.; Taibi, R.; Torrisi, C.; Pandolfi, S.; Chirumbolo, S. Fatigue in post-acute sequelae of SARS-CoV2 (PASC) treated with oxygen-ozone autohemo-therapy—Preliminary results on 100 patients. Eur. Rev. Med. Pharmacol. Sci. 2021, 25, 5871–5875. [Google Scholar] [CrossRef] [PubMed]
- Pier, D. Persistent Neurologic Symptoms after Mild COVID-19 Infection in Pediatric Patients: A Case Series. Ann. Neurol. 2021, 90, S113. [Google Scholar]
- Harenwall, S.; Heywood-Everett, S.; Henderson, R.; Godsell, S.; Jordan, S.; Moore, A.; Philpot, U.; Shepherd, K.; Smith, J.; Bland, A.R. Post-Covid-19 Syndrome: Improvements in Health-Related Quality of Life Following Psychology-Led Interdisciplinary Virtual Rehabilitation. J. Prim. Care Community Health 2021, 12, 21501319211067674. [Google Scholar] [CrossRef]
- Shogenova, L.V.; Tuet, T.T.; Kryukova, N.O.; Yusupkhodzhaeva, K.A.; Pozdnyakova, D.D.; Kim, T.G.; Chernyak, A.V.; Kalmanova, E.N.; Medvedev, O.S.; Kuropatkina, T.A.; et al. KalHydrogen inhalation in rehabilitation program of the medical staff recovered from CO-VID-19. Cardiovasc. Ther. Prev. 2021, 20, 24–32. [Google Scholar] [CrossRef]
- Viele, A.; Addona, T.; Trivisonno, A.; Paolone, P.; Iorio, N.; Colavita, A. From a suspected myocarditis to a post-SARS CoV2 inflammatory. Eur. Heart J. Suppl. 2021, 23 (Suppl. C), C104. [Google Scholar]
- Yong, S.J. Long COVID or post-COVID-19 syndrome: Putative pathophysiology, risk factors, and treatments. Infect. Dis. 2021, 53, 737–754. [Google Scholar] [CrossRef]
- Alvan, N.A. The road to addressing Long Covid. Science 2021, 373, 491–493. [Google Scholar] [CrossRef]
- Mantovani, E.; Mariotto, S.; Gabbiani, D.; Dorelli, G.; Bozzetti, S.; Federico, A.; Zanzoni, S.; Girelli, D.; Crisafulli, E.; Ferrari, S.; et al. Chronic fatigue syndrome: An emerging sequela in COVID-19 survivors? J. Neurovirol. 2021, 27, 631–637. [Google Scholar] [CrossRef]
- World Health Organisation Coronavirus (COVID-19) Dashboard. Available online: https://covid19.who.int/ (accessed on 5 April 2022).
- MOR13. Mortality by Main Causes of Death by Month, Age Group and Vaccination Status. Latvian Centre for Disease Prevention and Control (CDPC), Health Statistic Database. Available online: https://statistika.spkc.gov.lv/pxweb/en/Health/Health__Mirstiba/MOR13_celoni_vecgrupas_COVID-vakcinacija.px/ (accessed on 5 April 2022).
- Wu, Z.; McGoogan, J.M. Characteristics of and Important Lessons from the Coronavirus Disease 2019 (COVID-19) Outbreak in China: Summary of a Report of 72,314 Cases from the Chinese Center for Disease Control and Prevention. JAMA 2020, 323, 1239–1242. [Google Scholar] [CrossRef]
- Li, G.; Saguner, A.M.; An, J.; Ning, Y.; Day, J.D.; Ding, L.; Waintraub, X.; Wang, J. Cardiovascular disease during the COVID-19 pandemic: Think ahead, protect hearts, reduce mortality. Cardiol. J. 2020, 27, 616–624. [Google Scholar] [CrossRef] [PubMed]
- Grasselli, G.; Zangrillo, A.; Zanella, A.; Antonelli, M.; Cabrini, L.; Castelli, A.; Cereda, D.; Coluccello, A.; Foti, G. Roberto Fumagalli COVID-19 Lombardy ICU Network. Baseline characteristics and outcomes of 1591 patients infected with SARS-CoV-2 admitted to Icus of the Lombardy region, Italy. JAMA 2020, 323, 1574–1581. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhou, F.; Yu, T.; Du, R.; Fan, G.; Liu, Y.; Liu, Z.; Xiang, J.; Wang, Y.; Song, B.; Gu, X. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: A retrospective cohort study. Lancet 2020, 395, 1054–1062. [Google Scholar] [CrossRef]
- Shi, S.; Qin, M.; Shen, B.; Cai, Y.; Liu, T.; Yang, F.; Gong, W.; Liu, X.; Liang, J.; Zhao, Q.; et al. Association of Cardiac Injury with Mortality in Hospitalized Patients with COVID-19 in Wuhan, China. JAMA Cardiol. 2020, 5, 802–810. [Google Scholar] [CrossRef] [Green Version]
- Robak, O.; Dudek, M.; Ladny, J.R.; Szarpak, L.; Gilis-Malinowska, N.; Frass, M. Cardiac tamponade as a cause of COVID-19. Cardiol. J. 2020, 27, 900–901. [Google Scholar] [CrossRef]
- Husby, A.; Hansen, J.V.; Fosbøl, E.; Thiesson, E.M.; Madsen, M.; Thomsen, R.W.; Sørensen, H.T.; Andersen, M.; Wohlfahrt, J.; Gislason, G.; et al. SARS-CoV-2 vaccination and myocarditis or myopericarditis: Population based cohort study. BMJ 2021, 16, 068665. [Google Scholar] [CrossRef]
- Oster, M.E.; Shay, D.K.; Su, J.R.; Gee, J.; Creech, C.B.; Broder, K.R.; Edwards, K.; Soslow, J.H.; Dendy, J.M.; Schlaudecker, E.; et al. Myocarditis Cases Reported After mRNA-Based COVID-19 Vaccination in the US from December 2020 to August 2021. JAMA 2022, 327, 331–340. [Google Scholar] [CrossRef]
- Patone, M.; Mei, X.W.; Handunnetthi, L.; Dixon, S.; Zaccardi, F.; Shankar-Hari, M.; Watkinson, P.; Khunti, K.; Harnden, A.; Coupland, C.A.C.; et al. Risks of myocarditis, pericarditis, and cardiac arrhythmias associated with COVID-19 vaccination or SARS-CoV-2 infection. Nat. Med. 2022, 28, 410–422. [Google Scholar] [CrossRef]
- Olagunju, A.; Moradi, A.; Johnson, B.; Lebaron, Z.; Johnson, R.; Mehdizadeh, A. Acute Myocarditis Following Vaccination with the First Dose of the mRNA-1273 Vaccine. J. Investig. Med. High Impact Case Rep. 2022, 10, 23247096221092291. [Google Scholar] [CrossRef]
- Mimouni, H.; Bahouh, C.; Amaqdouf, S.; Laaribi, I.; Baddi, M.; Berichi, S.; Bkiyar, H.; Ismaili, N.; EI Ouafi, N.; Housni, B. Cardiogenic shock revealing myocarditis after mRNA vaccination against covid-19: Case report and brief review for the first case in Morocco. Ann. Med. Surg. 2022, 74, 103210. [Google Scholar] [CrossRef] [PubMed]
- Fatima, M.; Cheema, H.A.; Khan, M.H.A.K.; Shahid, H.; Ali, M.S.; Hassan, U.; Murad, M.W.; Rehman, M.A.U.; Farooq, H. Development of myocarditis and pericarditis after COVID-19 vaccination in adult population: A systematic review. Ann. Med. Surg. 2022, 76, 103486. [Google Scholar] [CrossRef] [PubMed]
- Nef, H.M.; Albrecht, E.; Helge, M.; Abdel-Hadi, M.; Bauer, T.; Brück, M.; Eggebrecht, H.; Ehrlich, J.R.; Ferrari, M.W.; Fichtlscherer, S. Impact of the COVID-19 pandemic on cardiovascular mortality and catherization activity during the lockdown in central germany: An observational study. Clin. Res. Cardiol. 2021, 110, 292–301. [Google Scholar] [CrossRef]
- Melaika, K.; Sveikata, L.; Wisniewski, A.; Jaxybayeva, A.; Ekkert, A.; Jatužis, D.; Masiliunas, R. Changes in prehospital stroke care and stroke mimic patterns during the COVID-19 lockdown. Int. J. Environ. Res. Public Health 2021, 18, 2150. [Google Scholar] [CrossRef] [PubMed]
- Topriceanu, C.C.; Wong, A.; Moon, J.C.; Hughes, A.D.; Bann, D.; Chaturvedi, N.; Patalay, P.; Conti, G.; Captur, G. Evaluating access to health and care services during lockdown by the COVID-19 survey in five UK national longitudinal studies. BMJ Open 2021, 11, 045813. [Google Scholar] [CrossRef] [PubMed]
- Geelsa, M.J.; Thøgersena, R.L.; Guzmanb, C.S.; Hoc, M.M.; Verreckd, F.; Colline, N.; Robertsonc, J.S.; McConkeyf, S.J.; Kaufmanng, S.H.E.; Leroya, O. TRANSVAC research infrastructure—Results and lessons learned fromthe European network of vaccine research and development. Vaccine 2015, 33, 5481–5487. [Google Scholar] [CrossRef]
- The Council of the European Union. Recommendation (of 7 December 2018) on Strengthened Cooperation against Vaccine-Preventable Diseases (2018/C 466/01). Off. J. Eur. Union. 2018. Available online: https://eur-lex.europa.eu/legal-content/EN/TXT/PDF/?uri=CELEX:32018H1228(01) (accessed on 14 March 2022).
- World Health Organization. Immunization Agenda 2030: A Global Strategy to Leave No One Behind. Available online: https://www.who.int/teams/immunization-vaccines-and-biologicals/strategies/ia2030 (accessed on 14 March 2022).
- World Health Organization. European Immunization Agenda 2030. Available online: https://apps.who.int/iris/bitstream/handle/10665/348002/9789289056052-eng.pdf (accessed on 14 March 2022).
- European Union Vaccines Strategy, presented on 17 June 2020, by the European Commission of the European Union. Available online: https://ec.europa.eu/info/live-work-travel-eu/coronavirus-response/public-health/eu-vaccines-strategy_en (accessed on 16 March 2022).
- U.S. Department of Health and Human Services. Vaccines National Strategic Plan 2021–2025; U.S. Department of Health and Human Services: Washington, DC, USA, 2021.
- U.S. Centers for Disease Control and Prevention (CDCs). Strategy to Rein-force Confidence in COVID-19 Vaccines. 2021. Available online: https://www.cdc.gov/vaccines/covid-19/vaccinate-with-confidence/strategy.html (accessed on 22 March 2022).
- Population Number, Its Changes and Density. Official Statistic of Latvia. Available online: https://stat.gov.lv/en/statistics-themes/population/population-number/247-population-number-its-changes-and-density?themeCode=IR (accessed on 5 April 2022).
- Number of Persons Infected by COVID-19 and Number of Persons Vaccinated against COVID-19. Official Statistic of Latvia. Available online: https://covid19.gov.lv/covid-19/covid-19-statistika/covid-19-izplatiba-latvija (accessed on 5 April 2022).
- Wang, R.; Chen, J.; Hozumi, Y.; Yin, C.; Wei, G.W. Emerging Vaccine-Breakthrough SARS-CoV-2 Variants. ACS Infect. Dis. 2022, 8, 546–556. [Google Scholar] [CrossRef]
- World Health Organization. The World Health Report 2008: Primary Health Care—Now More than Ever. Available online: https://www.who.int/whr/2008/08_overview_en.pdf (accessed on 22 March 2022).
- OECD Health Ministerial Statement—The next generation of health reforms (17.01.2017). The Organization for Economic Co-operation and Development. Available online: https://www.oecd.org/newsroom/oecd-health-ministerial-statement-the-next-generation-of-health-reforms.htm (accessed on 22 March 2022).
- OECD Health Ministerial—Putting People at the Centre: The Future of Health. Available online: https://www.oecd.org/health/ministerial/ (accessed on 22 March 2022).
- Hølge-Hazelton, B.; Kjerholt, M.; Rosted, E.; Hansen, S.T.; Borre, L.Z.; McCormack, B. Improving Person-Centred Leadership: A Qualitative Study of Ward Managers’ Experiences during the COVID-19 Crisis. Risk Manag. Healthc. Policy 2021, 14, 1401–1411. [Google Scholar] [CrossRef]
- Bigdeli, M.; Rouffy, B.; Lane, B.D.; Schmets, G.; Soucat, A. Health systems governance: The missing links. BMJ Glob. Health 2020, 5, e002533. [Google Scholar] [CrossRef]
- Simões, J.; Magalhćes, J.P.M.; Biscaia, A.; da Luz Pereira, A. Organisation of the State, model of health system and COVID-19 health outcomes in six European countries, during the first months of the COVID-19 epidemic in 2020. Int. J. Health Plan. Manag. 2021, 36, 1874–1886. [Google Scholar] [CrossRef]
- Sturmberg, J.P.; Tsasis, P.; Hoemeke, L. COVID-19—An opportunity to redesign health policy thinking. Int. J. Health Policy Manag. 2020, 11, 409–413. [Google Scholar] [CrossRef] [PubMed]
- Vainieri, M.; Noto, G.; Ferre, F.; Rosella, L.C. A Performance Management System in Healthcare for All Seasons? Int. J. Environ. Res. Public Health 2020, 17, 5590. [Google Scholar] [CrossRef]
- Paul, E.; Brown, G.W.; Ridde, V. COVID-19: Time for paradigm shift in the nexus between local, national and global health. BMJ Glob. Health 2020, 5, e002622. [Google Scholar] [CrossRef]
- Hasan, H.F. Legal and Health Response to COVID-19 in the Arab Countries. Risk Manag. Healthc. Policy 2021, 14, 1141–1154. [Google Scholar] [CrossRef] [PubMed]
- Lal, A.; Erondu, N.A.; Heymann, D.L.; Gitahi, G.; Yates, R. Fragmented health systems in COVID-19: Rectifying the misalignment between global health security and universal health coverage. Health Policy 2021, 397, 61–67. [Google Scholar] [CrossRef]
- Khosla, R.; Allotey, P.; Gruskin, S. Global health and human rights for a postpandemic world. BMJ Glob. Health 2020, 5, e003548. [Google Scholar] [CrossRef]
- Balqis-Ali, N.Z.; Fun, W.H.; Ismail, M.; Ng, R.J.; Jaaffar, F.S.A.; Low, L.L. Addressing Gaps for Health Systems Strengthening: A Public Perspective on Health Systems’ Response towards COVID-19. Int. J. Environ. Res. Public Health 2021, 18, 9047. [Google Scholar] [CrossRef]
- Topp, S.M. Power and politics: The case for linking resilience to health system governance. BMJ Glob. Health 2020, 5, e002891. [Google Scholar] [CrossRef]
- Anderson, J.E.; Aase, K.; Bal, R.; Bourrier, M.; Braithwaite, J.; Nakajima, K.; Wiig, S.; Guise, V. Multilevel influences on resilient healthcare in six countries: An international comparative study protocol. BMJ Open 2020, 10, e039158. [Google Scholar] [CrossRef]
- Plagg, B.; Piccoliori, G.; Oschmann, J.; Engl, A.; Eisendle, K. Primary Health Care and Hospital Management During COVID-19: Lessons from Lombardy. Risk Manag. Healthc. Policy 2021, 14, 3987–3992. [Google Scholar] [CrossRef]
- Petiwala, A.; Lanford, D.; Landers, G.; Minyard, K. Community voice in cross-sector alignment: Concepts and strategies from a scoping review of the health collaboration literature. BMC Public Health 2021, 21, 712. [Google Scholar] [CrossRef] [PubMed]
- Thomson, S.; Ip, E.C. COVID-19 Emergency Measures Are Hurting Democracy Globally. Am. J. Public Health 2020, 110, 1356–1357. [Google Scholar] [CrossRef] [PubMed]
- Frick, N.R.J.; Möllmann, H.L.; Mirbabaie, M.; Stieglitz, S. Driving Digital Transformation During a Pandemic: Case Study of Virtual Collaboration in a German Hospital. JMIR Med. Inform. 2021, 9, 25183. [Google Scholar] [CrossRef] [PubMed]
- Lim, M.Y.H.; Lin, V. Governance in health workforce: How do we improve on the concept? A network-based, stakeholder-driven approach. Hum. Resour. Health 2021, 19, 1. [Google Scholar] [CrossRef]
- World Health Organization. Strategy to Achieve Global Covid-19 Vaccination by mid-2022. Available online: https://www.who.int/publications/m/item/strategy-to-achieve-global-covid-19-vaccination-by-mid-2022 (accessed on 6 October 2021).
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Araja, D.; Berkis, U.; Murovska, M. COVID-19 Pandemic-Revealed Consistencies and Inconsistencies in Healthcare: A Medical and Organizational View. Healthcare 2022, 10, 1018. https://doi.org/10.3390/healthcare10061018
Araja D, Berkis U, Murovska M. COVID-19 Pandemic-Revealed Consistencies and Inconsistencies in Healthcare: A Medical and Organizational View. Healthcare. 2022; 10(6):1018. https://doi.org/10.3390/healthcare10061018
Chicago/Turabian StyleAraja, Diana, Uldis Berkis, and Modra Murovska. 2022. "COVID-19 Pandemic-Revealed Consistencies and Inconsistencies in Healthcare: A Medical and Organizational View" Healthcare 10, no. 6: 1018. https://doi.org/10.3390/healthcare10061018
APA StyleAraja, D., Berkis, U., & Murovska, M. (2022). COVID-19 Pandemic-Revealed Consistencies and Inconsistencies in Healthcare: A Medical and Organizational View. Healthcare, 10(6), 1018. https://doi.org/10.3390/healthcare10061018