
The Complexities of Prescribing Assistive Equipment at the End of Life—Patient and Caregivers’ Perspectives

 , ,
, ,
Abstract
:1. Introduction
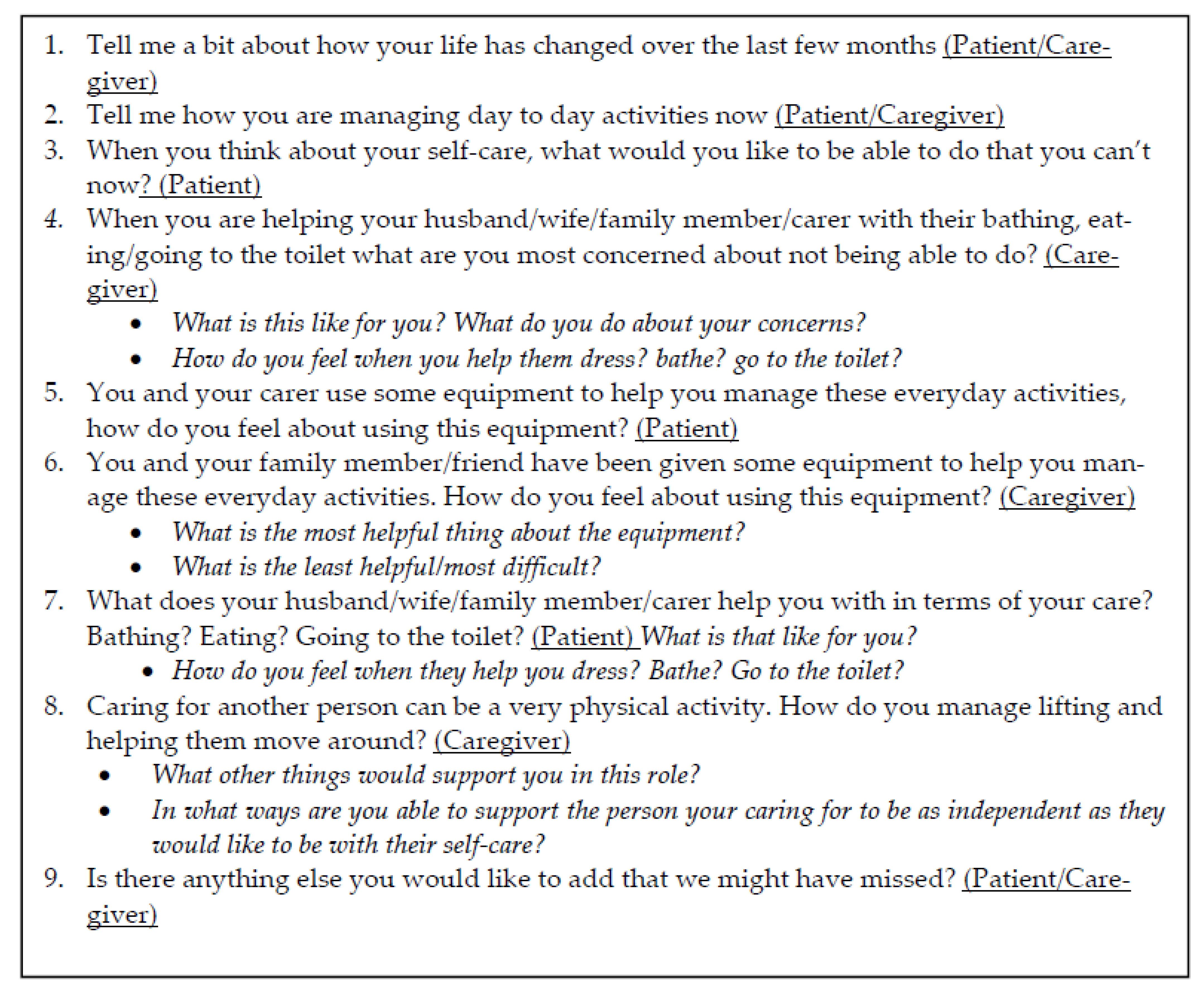
2. Methods
3. Results
3.1. Enabling Engagement in Everyday Activities
3.1.1. It’s Been Brilliant. I Can Get Out!
Kerry: I use the wheelchair every Thursday when we go shopping because it’s too difficult for me to do every aisle in the shopping centre, not only with the cancer but I also have a chronic back… if I was walking… I’d have to stop for ten minutes and then walk for five, stop for ten. But in the wheelchair, we can do everything we want plus the other shops that I normally couldn’t.
Anne: If it is a nice day we will go and get a coffee and sit by the lake … and Dave (husband) will push me around if the weather is nice yeah or we just sit in the car but it’s fantastic.
Adam: Yeah, what I used to do was grab the sink on the vanity—grab the taps on the vanity and just give myself a bit of a pull… They also gave me a metal frame that goes around the toilet bowl with an arm rest…So when I sit on the toilet, my back’s straight, my knees are at 90 degrees, and I have got an arm rest and can get up and back on it and it’s very helpful.
Christine: I stand up, stick my head under, wash my hair and then I sit on the seat and wash the rest of myself… I will make sure someone is home and that Carl (husband) is home to help me if need be. He usually sets the chair up for me in the shower and then I have another chair that I sit on to dry myself.
Gillian—Husband: Caroline would sleep a fair bit in the bed and I felt that if she had her bed out here at then if people came over—she can still hear because she’s got very good hearing—she doesn’t miss a thing, do you darling?
Gillian: Yeah.
Gillian—Husband: So then at least she is part of it and that I think was the important thing for me to have her within the lounge…being part of the whole family when they come.
Paula: …They made another step, the lower step, to go out through those back doors which has been really helpful, and I just have the little things over the sliding door tracks have been good so there’s nothing that we really haven’t used, have we?
3.1.2. I Feel More Secure and Confident
Interviewer: So, what is the most useful thing about the shower seat for you?
Jane: Just the fact that it is there when I need it or when I am not doing the best and I am feeling a little bit wobbly then—I have good days and bad days as well.
Mark: If I didn’t have the handrails, I would probably be just sitting in a chair instead of standing up in the shower; washing and do all that.
Christine: [I was] getting stuck on the toilet… because the seat’s low. I’ve got no strength in my arms or my legs much so I couldn’t sort of lever myself up and get up
Mark—Wife: But one of his favourite things is the toilet seat
Mark: Oh yeah! The raised toilet seat… Just like a donut, yeah, it’s brilliant…You’re just higher so when you want to stand up your legs aren’t bent. I reckon they should have them in every household. They should be built with them because when you go to stand up you don’t really have to lift your whole weight because your legs are up there.
Kerry: If it’s a full day out or a full shop, I will take the wheelchair because it just drags it out of you. … If I’m feeling really alert and know that I’ve got a little bit more energy, I will go without [stick], but if I haven’t and I feel blah, I will use the stick and just take a little bit more time, but either way it still drags it out of me… I can still do a lot of things, it’s just the fatigue and no strength is what stops me at the moment.
Derek: It gives you a little bit of... not satisfaction it gives you, it gives you a bit of protection been though it might not you feel as though it does.
Interviewer: Protection?
Derek: Against a fall.
Frank-Daughter: We had to hire one like for taking him out at night and it’s simply the transport for me of wheeling, you know, oxygen bottles and stuff like that. But we have a pride issue with wheelchairs, which I get…
Frank: …but it’s like Maree (daughter) said she’s got to hook the bottle on the cart there dragging the golf buggy around.
3.2. Dependency: A Two-Way Street
3.2.1. Minimising Dependency on Caregivers
Anne: That’s the only thing that worries you is what happens when his (husband) health doesn’t get—if anything happens to him or if he hurts his back or something but at the moment, he’s good… We have got a wheelchair in the garage that belonged to Dave’s mum but it’s got big wheels and it is quite bulky and it’s a bit heavier to move and we used to have that before we got the other but the other one’s much lighter to move.
Paula—Husband: I mean if the house was a bit bigger it would be easier to move—I put a few hits on the wall. I came around with a wheelchair and I smashed a plug that was in [it]…I smashed that to smithereens.
Paula—Husband: Once I put her on the commode then I could put her over the toilet or put her in the shower… It had the wheels on the bottom and Dom Care also provided ramps into the shower and ramps into the house, you know what I mean… so I didn’t have to carry her.
Kerry: Well, that’s due to relationship problems, mental fatigue, but yeah it also depends on what mood my husband’s in too, as whether we can get in and out within five minutes, or he’s in a good mood and we can be 15/20 min.
Margaret—Daughter: When we go out in the wheelchair, yeah. I think it’s easier for mum-no let me rephrase it, it was more comfortable for mum to be in the wheelchair rather than trying to walk, but somebody else steering, driving, pushing, stopping, starting with mum not in control… and you were worried about crossing roads.
Margaret: Yes, it seemed as if, it seemed as if they’ve (daughter) pushed me in front of a car, and [okay], and then waited, you know I was the one who was going to get cleaned up with the car. In a wheelchair so that you’re sitting sort of radiator height of the car coming to you. And, it is, I’ll say a bit of a concern.
3.2.2. Ways That Caregivers Manage Dependency
Frank—Daughter: I’m not physically big. It’s getting him in and out the car and I know how hard that was when he wasn’t well…. If he goes down, I’m going down…I don’t want to deprive him of going out just because I’m not physically capable of getting him in and out of the car, whereas if I’ve got a wheelchair … at least I know that he can still enjoy the things that he enjoys without putting a physical strain on me.
Gillian—Husband: I was worried that—I am pleased we have got the stool and the shower the way we did because before I was trying to do it on my own … we were struggling, fear of a fall, and… with a stool it’s great because I could actually move in the shower as well if I needed to. I don’t like to lift her or anything like that just in case I do it wrong and I don’t want to hurt myself too...’No, no good to anybody—I’ve gotta be careful.
Paula—Husband: That’s great, that’s great because you can lift her up—I can move the bed forward, move the bed up, move the bed. Before … [it] was very difficult for her because as I lifted her up, I was putting pressure on her so, now she stays in bed, she’s not moving so it’s better for her.
Margaret—Daughter: And somebody said “Don’t do that, this is how you walk up the steps with a walker.” And she just went, see there… lift it up, take a step forward, move it up the step. God, I wish somebody had told us that when we first got it…. We were trying to work out the steps into the house and the steps out of the house… I was struggling.
Anne: The only experience I have had with a walker was my husband’s mother, she had one, and she got-she used to let it get away from her and she looked so bent over and we always used to say to her stand up straight. —You see so many people with walkers and they don’t know how to use them properly and I was so grateful that the physio came out here and showed me how to use it.
3.3. The Pragmatics of Choosing, Using or Declining AE
3.3.1. If You Need It, You Need It
Adam: there might have been a time where I might have thought—walking frame, I don’t need the toilet raised, I don’t need a frame around the toilet but I am realistic, I do need it and I am grateful that I’ve got it…It serves it purpose, it does what it is intended to do and it is very helpful.
Christine: That’s going to help me so much… so that didn’t bother me at all. All I could see was all the help that you know you people were going to give me… I don’t care, as long as it helps me and I can still get around.
Anne: It has changed dramatically in the last few months. When the equipment came—wheelchair, walker, shower chair and got the toilet seat—I thought I won’t need this walker. I’ve lost all the power in my legs so this has been invaluable—if I hadn’t had that I wouldn’t be able to get around.
Christine: I don’t sort of want anybody—I don’t want to be relying on anybody sort of thing… I would like to stay as independent as I can for as long as I can.
Adam: I was given advice that if domiciliary care offer you any equipment, take it, because if you don’t take it and a few months down track you find you could have done with it, you might have trouble getting it. So, I took it—it was there on offer, I said ‘okay. we’ll have it’…It’s quite possible because I am not getting any stronger so there might be a time when I do need it but at the moment, I don’t feel that I need it but it’s there if I do.
Derek: So, what we do then is put the wheelchair in behind that, put your [gear] on the trailer, and with the walker, that goes in behind the wheelchair with the fishing rods on it … and you got one bloke (son) pushing all the stuff there.
3.3.2. If I am Not That Old Yet… Maybe One Day
Interviewer: And you are not keen on the walker? Can you talk about why?
Gillian: I am not that old yet.
Margaret: Karen (daughter) told me that they put a pole in I thought ‘Oh god!” …Because I’m not old and I didn’t want a stick to get out of bed with you know.
Kerry—Patient: Sometimes it’s more of a burden to actually have it. It’s easier just to hold onto a shopping trolley and walk behind a shopping trolley than actually physically have to use the stick.
Frank—Daughter: We got the bottle because we thought it would be a good idea and Dad was always conscious that…he was knocking it over or the stream [sprayed out]. So he actually reverted to peeing in the rubbish bin, because it was easier to place it, wasn’t it? But then he’d get wee on his pyjama pants… So we tried a multitude of things prior to actually getting the commode…It’s been brilliant for him.
Kerry: I just have to have someone to help me get a—because our bathroom is falling apart and we’re waiting to get a new one. I have to have someone there who I can hang on to because there’s nothing to hang on to…. It’s been like that for three and a half years… and she’s [real estate agent] fighting with him to get everything fixed and he won’t do it.
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Lala, A.P.; Kinsella, E.A. A Phenomenological Inquiry into the Embodied Nature of Occupation at End of Life. Can. J. Occup. Ther. 2011, 78, 246–254. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Morgan, D.D.; Taylor, R.R.; Ivy, M.; George, S.; Farrow, C.; Lee, V. Contemporary occupational priorities at the end of life mapped against Model of Human Occupation constructs: A scoping review. Aust. Occup. Ther. J. 2022. [Google Scholar] [CrossRef] [PubMed]
- Peoples, H.; Nissen, N.; Brandt, Å.; la Cour, K. Perceptions of quality of life by people with advanced cancer who live at home. Br. J. Occup. Ther. 2020, 84, 723–730. [Google Scholar] [CrossRef]
- Von Post, H.; Wagman, P. What is important to patients in palliative care? A scoping review of the patient’s perspective. Scand. J. Occup. Ther. 2019, 26, 1–8. [Google Scholar] [CrossRef]
- Morgan, D.D.; Currow, D.C.; Denehy, L.; Aranda, S.A. Living actively in the face of impending death: Constantly adjusting to bodily decline at the end-of-life. BMJ Support. Palliat. Care 2015, 7, 179–188. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- la Cour, K.; Johannessen, H.; Josephsson, S. Activity and meaning making in the everyday lives of people with advanced cancer. Palliat. Support. Care 2009, 7, 469–479. [Google Scholar] [CrossRef]
- Svidén, G.A.; Tham, K.; Borell, L. Involvement in everyday life for people with a life threatening illness. Palliat. Support. Care 2010, 8, 345–352. [Google Scholar] [CrossRef] [Green Version]
- Health Canada. First Annual Report on Medical Assistance in Dying in Canada, 2019. Government of Canada, 2020. Available online: https://www.canada.ca/en/health-canada/services/medical-assistance-dying-annual-report-2019.html (accessed on 25 July 2021).
- Montagnini, M.; Javier, N.M.; Mitchinson, A. The role of rehabilitation in patients receiving hospice and palliative care. Rehabil. Oncol. 2020, 38, 9–21. [Google Scholar] [CrossRef]
- World Health Organization. Health Services and Palliative Care: Practical Approaches and Resources to Support Policy, Strategy and Practice; World Health Organization: Geneva, Switzerland, 2021; pp. 1–58. [Google Scholar]
- Dietz, J.H., Jr. Adaptive rehabilitation in cancer. Postgrad. Med. 1980, 68, 145–153. [Google Scholar] [CrossRef]
- Häggblom-Kronlöf, G.; Sonn, U. Use of assistive devices—A reality full of contradictions in elderly persons’ everyday life. Disabil. Rehabil. Assist. Technol. 2007, 2, 335–345. [Google Scholar] [CrossRef]
- Blackler, A.; Brophy, C.; O’Reilly, M.; Chamorro-Koc, M. Seating in aged care: Physical fit, independence and comfort. SAGE Open Med. 2018, 6, 2050312117744925. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mann, W.C.; Llanes, C.; Justiss, M.D.; Tomita, M. Frail Older Adults’ Self-Report of Their Most Important Assistive Device. OTJR Occup. Particip. Health 2004, 24, 4–12. [Google Scholar] [CrossRef]
- Burns, C.M.; Abernethy, A.P.; Leblanc, T.W.; Currow, D.C. What is the role of friends when contributing care at the end of life? Findings from an Australian population study. Psycho-Oncology 2011, 20, 203–212. [Google Scholar] [CrossRef] [PubMed]
- Paganoni, S.; Karam, C.; Joyce, N.; Bedlack, R.; Carter, G.T. Comprehensive rehabilitative care across the spectrum of amyotrophic lateral sclerosis. NeuroRehabilitation 2015, 37, 53–68. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cecatto, R.B.; Battistella, L.R. Rehabilitation and Palliative Care in Neurocritical Patients. In Neurocritical Care for Neurosurgeons: Principles and Applications; Figueiredo, E.G., Welling, L.C., Rabelo, N.N., Eds.; Springer International Publishing: Cham, Switzerland, 2021; pp. 667–675. [Google Scholar]
- Choi, S.; Seo, J. Analysis of caregiver burden in palliative care: An integrated review. Nurs. Forum 2019, 54, 280–290. [Google Scholar] [CrossRef] [PubMed]
- Morgan, D.D.; Tieman, J.; Allingham, S.F.; Ekström, M.P.; Connolly, A.; Currow, D.C. The trajectory of functional decline over the last 4 months of life in a palliative care population: A prospective, consecutive cohort study. Palliat. Med. 2019, 33, 693–703. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dumont, S.; Jacobs, P.; Turcotte, V.; Anderson, D.; Harel, F. The trajectory of palliative care costs over the last 5 months of life: A Canadian longitudinal study. Palliat. Med. 2010, 24, 630–640. [Google Scholar] [CrossRef]
- Foley, G. The supportive relationship between palliative patients and family caregivers. BMJ Support. Palliat. Care 2018, 8, 184–186. [Google Scholar] [CrossRef]
- Morgan, D.L. Pragmatism as a Paradigm for Social Research. Qual. Inq. 2014, 20, 1045–1053. [Google Scholar] [CrossRef]
- Morgan, D.L. Integrating Qualitative and Quantitative Methods: A Pragmatic Approach; SAGE: Thousand Oaks, CA, USA, 2014. [Google Scholar] [CrossRef]
- Patton, M. Variety of qualitative inquiry frameworks: Paradigmatic, philosophical, and theoretical orientations. In Qualitative Research & Evaluation Methods, 4th ed.; SAGE: Thousand Oaks, CA, USA, 2015; pp. 85–168. [Google Scholar]
- Hennink, M.; Kaiser, B.N. Sample sizes for saturation in qualitative research: A systematic review of empirical tests. Soc. Sci. Med. 2022, 292, 114523. [Google Scholar] [CrossRef]
- Kiger, M.E.; Varpio, L. Thematic analysis of qualitative data: AMEE Guide No. 131. Med Teach. 2020, 42, 846–854. [Google Scholar] [CrossRef] [PubMed]
- Tong, A.; Sainsbury, P.; Craig, J. Consolidated criteria for reporting qualitative research (COREQ): A 32-item checklist for interviews and focus groups. Int. J. Qual. Health Care 2007, 19, 349–357. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brooks, F.A.; Keeney, T.; Ritchie, C.; Tolchin, D.W. Rehabilitation for Symptom Management for Patients with Cancer at the End of Life: Current Evidence and Barriers to Care. Curr. Phys. Med. Rehabil. Rep. 2021, 9, 215–223. [Google Scholar] [CrossRef]
- Cheville, A.L.; Morrow, M.; Smith, S.R.; Basford, J.R. Integrating Function-Directed Treatments into Palliative Care. PM&R 2017, 9, S335–S346. [Google Scholar] [CrossRef] [Green Version]
- Yamada, T.; Taylor, R.; Kielhofner, G.E. Person-specific concepts of human occupation. In Kielhofner’s Model of Human Occupation, 5th ed.; Wolters Kluwer: Philadelphia, PA, USA, 2017; pp. 38–56. [Google Scholar]
- Dahler, A.M.; Rasmussen, D.M.; Andersen, P.T. Meanings and experiences of assistive technologies in everyday lives of older citizens: A meta-interpretive review. Disabil. Rehabil. Assist. Technol. 2016, 11, 619–629. [Google Scholar] [CrossRef]
- Gramstad, A.; Storli, S.L.; Hamran, T. Exploring the meaning of a new assistive technology device for older individuals. Disabil. Rehabil. Assist. Technol. 2014, 9, 493–498. [Google Scholar] [CrossRef] [Green Version]
- Skymne, C.; Dahlin-Ivanoff, S.; Claesson, L.; Eklund, K. Getting used to assistive devices: Ambivalent experiences by frail elderly persons. Scand. J. Occup. Ther. 2012, 19, 194–203. [Google Scholar] [CrossRef]
- Marasinghe, K.M. Assistive technologies in reducing caregiver burden among informal caregivers of older adults: A systematic review. Disabil. Rehabil. Assist. Technol. 2016, 11, 353–360. [Google Scholar] [CrossRef]
- Gramstad, A.; Storli, S.L.; Hamran, T. “Do I need it? Do I really need it?” Elderly peoples experiences of unmet assistive technology device needs. Disabil. Rehabil. Assist. Technol. 2013, 8, 287–293. [Google Scholar] [CrossRef] [Green Version]
- Hoffmann, T.; McKenna, K. A Survey of Assistive Equipment Use by Older People following Hospital Discharge. Br. J. Occup. Ther. 2004, 67, 75–82. [Google Scholar] [CrossRef] [Green Version]
- Henson, L.A.; Maddocks, M.; Evans, C.; Davidson, M.; Hicks, S.; Higginson, I.J. Palliative Care and the Management of Common Distressing Symptoms in Advanced Cancer: Pain, Breathlessness, Nausea and Vomiting, and Fatigue. J. Clin. Oncol. 2020, 38, 905–914. [Google Scholar] [CrossRef]
- Runacres, F.; Gregory, H.; Ugalde, A. ‘The horse has bolted I suspect’: A qualitative study of clinicians’ attitudes and perceptions regarding palliative rehabilitation. Palliat. Med. 2017, 31, 642–650. [Google Scholar] [CrossRef] [PubMed]
- Wilson, C. Rehabilitation services and palliative care: An oxymoron or best practice? Home. Healthc. Now. 2019, 37, 174–175. [Google Scholar] [CrossRef] [PubMed]
- Martin, E.; Herkt, J. The reality and potential of occupational therapy within hospice care. N. Z. J. Occup. Ther. 2018, 65, 23–29. [Google Scholar] [CrossRef]
- McLeod, K.E.; Norman, K.E. “I’ve found it’s very meaningful work”: Perspectives of physiotherapists providing palliative care in Ontario. Physiother. Res. Int. 2020, 25, e1802. [Google Scholar] [CrossRef]
- Wittry, S.A.; Lam, N.-Y.; McNalley, T. The Value of Rehabilitation Medicine for Patients Receiving Palliative Care. Am. J. Hosp. Palliat. Med. 2018, 35, 889–896. [Google Scholar] [CrossRef]
- Fettes, L.; Bone, A.E.; Etkind, S.N.; Ashford, S.; Higginson, I.J.; Maddocks, M. Disability in Basic Activities of Daily Living Is Associated With Symptom Burden in Older People With Advanced Cancer or Chronic Obstructive Pulmonary Disease: A Secondary Data Analysis. J. Pain Symptom Manag. 2021, 61, 1205–1214. [Google Scholar] [CrossRef]
- Pilegaard, M.S.; la Cour, K.; Baldursdóttir, F.; Morgan, D.; Oestergaard, L.G.; Brandt, Å. Assistive devices among people living at home with advanced cancer: Use, non-use and who have unmet needs for assistive devices? Eur. J. Cancer Care 2022. [Google Scholar] [CrossRef]
- Philip, J.; Gold, M.; Brand, C.; Miller, B.; Douglass, J.; Sundararajan, V. Facilitating Change and Adaptation: The Experiences of Current and Bereaved Carers of Patients with Severe Chronic Obstructive Pulmonary Disease. J. Palliat. Med. 2014, 17, 421–427. [Google Scholar] [CrossRef]
- Ewing, G.; Penfold, C.; Benson, J.A.; Mahadeva, R.; Howson, S.; Burkin, J.; Booth, S.; Lovick, R.; Gilligan, D.; Todd, C.; et al. Clinicians’ Views of Educational Interventions for Carers of Patients With Breathlessness Due to Advanced Disease: Findings From an Online Survey. J. Pain Symptom Manag. 2016, 53, 265–271. [Google Scholar] [CrossRef] [Green Version]
- Bartley, C.; Webb, J.-A.; Bayly, J. Multidisciplinary approaches to moving and handling for formal and informal carers in community palliative care. Int. J. Palliat. Nurs. 2015, 21, 17–23. [Google Scholar] [CrossRef] [PubMed]
- Pousada, T.; Garabal-Barbeira, J.; Martínez, C.; Groba, B.; Nieto-Riveiro, L.; Pereira, J. How Loan Bank of Assistive Technology Impacts on Life of Persons with Amyotrophic Lateral Sclerosis and Neuromuscular Diseases: A Collaborative Initiative. Int. J. Environ. Res. Public Health 2021, 18, 763. [Google Scholar] [CrossRef] [PubMed]
- Funke, A.; Spittel, S.; Grehl, T.; Grosskreutz, J.; Kettemann, D.; Petri, S.; Weyen, U.; Weydt, P.; Dorst, J.; Ludolph, A.C.; et al. Provision of assistive technology devices among people with ALS in Germany: A platform-case management approach. Amyotroph. Lateral Scler. Front. Degener. 2018, 19, 342–350. [Google Scholar] [CrossRef] [PubMed]
- Mortenson, W.B.; Pysklywec, A.; Fuhrer, M.J.; Jutai, J.W.; Plante, M.; Demers, L. Caregivers’ experiences with the selection and use of assistive technology. Disabil. Rehabil. Assist. Technol. 2018, 13, 562–567. [Google Scholar] [CrossRef] [PubMed]
- Foley, G.; Timonen, V.; Hardiman, O. “I hate being a burden”: The patient perspective on carer burden in amyotrophic lateral sclerosis. Amyotroph. Lateral Scler. Front. Degener. 2016, 17, 351–357. [Google Scholar] [CrossRef]
- Independent Living Centre of Western Australia. Family Carers and the Physical Impact of Caring—Injury and Prevention; Research Report, Executive Summary; Independent Living Centre of Western Australia: Nedlands, Australia, 2006; pp. 1–10. [Google Scholar]
- Leroy, T.; Fournier, E.; Penel, N.; Christophe, V. Crossed views of burden and emotional distress of cancer patients and family caregivers during palliative care. Psycho-Oncology 2015, 25, 1278–1285. [Google Scholar] [CrossRef]
- Ullrich, A.; Ascherfeld, L.; Marx, G.; Bokemeyer, C.; Bergelt, C.; Oechsle, K. Quality of life, psychological burden, needs, and satisfaction during specialized inpatient palliative care in family caregivers of advanced cancer patients. BMC Palliat. Care 2017, 16, 31. [Google Scholar] [CrossRef]
- Aoun, S.M.; Connors, S.L.; Priddis, L.; Breen, L.J.; Colyer, S. Motor Neurone Disease family carers’ experiences of caring, palliative care and bereavement: An exploratory qualitative study. Palliat. Med. 2012, 26, 842–850. [Google Scholar] [CrossRef]
- James, C.L.; Rusli, N.; Broady, T.R. Carers and manual handling: Survey results. Int. J. Ther. Rehabil. 2017, 24, 146–154. [Google Scholar] [CrossRef]
- McCauley, R.; McQuillan, R.; Ryan, K.; Foley, G. Mutual support between patients and family caregivers in palliative care: A systematic review and narrative synthesis. Palliat. Med. 2021, 35, 875–885. [Google Scholar] [CrossRef]
- Larsen, S.M.; Mortensen, R.F.; Kristensen, H.K.; Hounsgaard, L. Older adults’ perspectives on the process of becoming users of assistive technology: A qualitative systematic review and meta-synthesis. Disabil. Rehabil. Assist. Technol. 2019, 14, 182–193. [Google Scholar] [CrossRef] [PubMed]
- Morgan, D.D.; Rawlings, D.; Moores, C.J.; Button, L.; Tieman, J.J. The Changing Nature of Palliative Care: Implications for Allied Health Professionals’ Educational and Training Needs. Healthcare 2019, 7, 112. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| Sex | Patients: Female (10), Male (4) |
| Caregivers: Female (2 *), Male (9) | |
| Ages | Range: 55–77 years |
| Living arrangements | Two participants lived alone, the remainder lived with one or more family members |
| Caregiver role | Husband (8), wife (1), daughter (1), son (1) |
| Patient diagnoses | Lung, CNS, breast, prostate, renal, colorectal and haematological cancers, COPD |
| Theme | Sub-Themes | |
|---|---|---|
| 3.1. Enabling engagement in everyday activities | 3.1.1. It’s been brilliant. I can get out! | 3.1.2. I feel more secure and confident. |
| 3.2. Dependency: A two-way street | 3.2.1. Minimising dependency on caregivers | 3.2.2. Ways that caregivers manage dependency |
| 3.3. The pragmatics of choosing, using or declining AE | 3.3.1. If you need it, you need it | 3.3.2. I’m not that old yet… maybe one day |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Morgan, D.D.; Willis, E.; Sweet, K.; Roe, P.; Rabaçal, J.; Currow, D.C. The Complexities of Prescribing Assistive Equipment at the End of Life—Patient and Caregivers’ Perspectives. Healthcare 2022, 10, 1005. https://doi.org/10.3390/healthcare10061005
Morgan DD, Willis E, Sweet K, Roe P, Rabaçal J, Currow DC. The Complexities of Prescribing Assistive Equipment at the End of Life—Patient and Caregivers’ Perspectives. Healthcare. 2022; 10(6):1005. https://doi.org/10.3390/healthcare10061005
Chicago/Turabian StyleMorgan, Deidre D., Eileen Willis, Kate Sweet, Pen Roe, Joana Rabaçal, and David C. Currow. 2022. "The Complexities of Prescribing Assistive Equipment at the End of Life—Patient and Caregivers’ Perspectives" Healthcare 10, no. 6: 1005. https://doi.org/10.3390/healthcare10061005
APA StyleMorgan, D. D., Willis, E., Sweet, K., Roe, P., Rabaçal, J., & Currow, D. C. (2022). The Complexities of Prescribing Assistive Equipment at the End of Life—Patient and Caregivers’ Perspectives. Healthcare, 10(6), 1005. https://doi.org/10.3390/healthcare10061005