
Effectiveness of Fucoidan on Supplemental Therapy in Cancer Patients: A Systematic Review

 , ,
, ,
Abstract
:1. Introduction
2. Methods
2.1. Study Design and Search Strategy
2.2. Eligibility, Selection, and Data Extraction
2.3. Data Analysis
2.4. Quality Assessment
3. Results
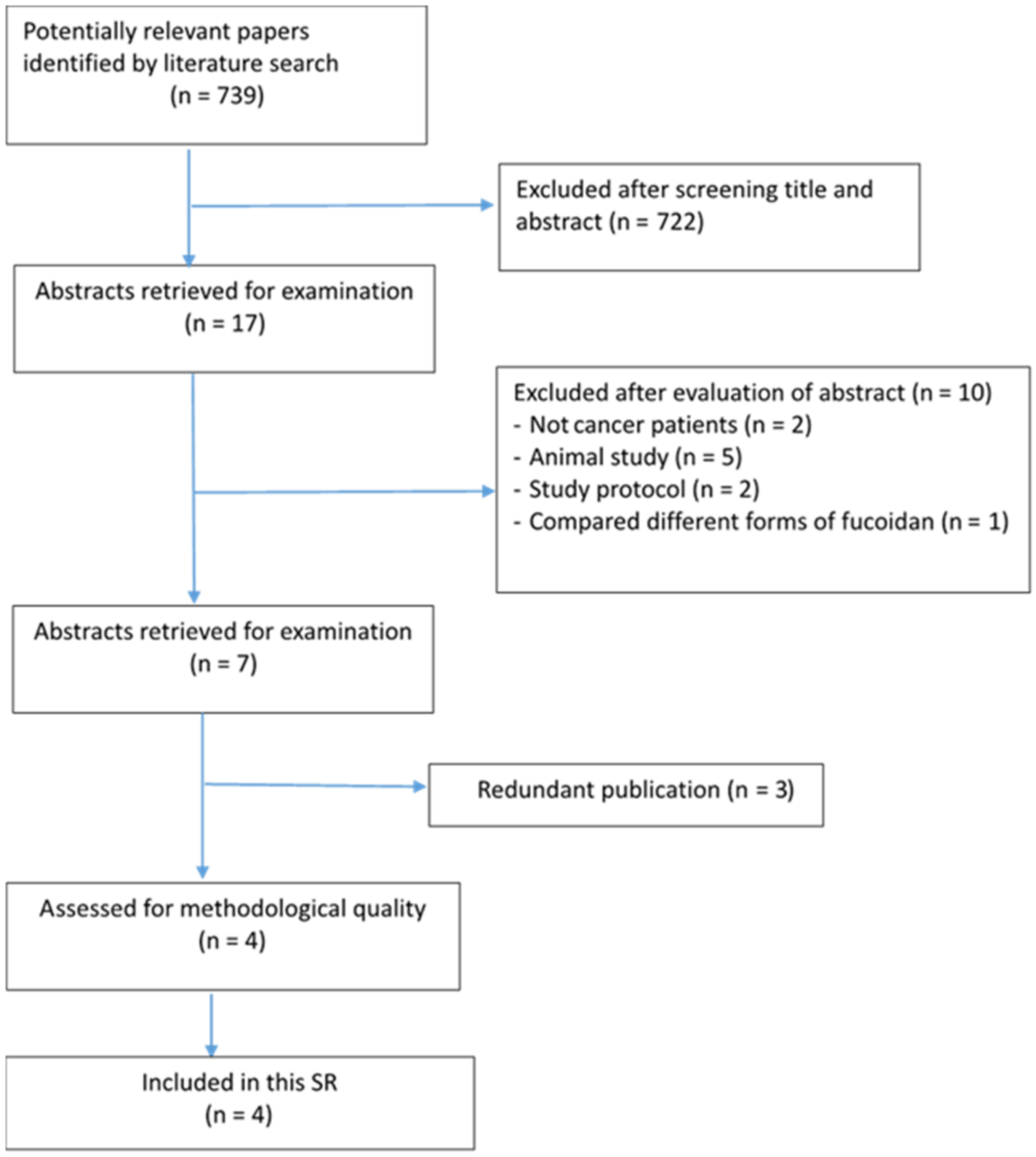
3.1. Study Selection
3.2. Characteristics of the Included Studies

{kind=link}
| Author (Year), Country | Participants | Fucoidan Source/Molecular Weight | Intervention vs. Control | Intervention Period | Outcome Measurements (also See Table 2) |
|---|---|---|---|---|---|
| Randomized controlled trials | |||||
| Tsai et al. [5] Taiwan | Metastatic Colorectal Cancer, n = 54 Median age: 57.46 ± 12.15(F) 62.38 ± 11.72(NF) | Sargassum hemiphyllum, LMF | 4 g of LMF powder vs. cellulose powder | 6 months | Clinical Patient reported |
| Quasi-experimental study | |||||
| Ikeguchi et al. [21] Japan | Advanced or recurrent colorectal cancer, n = 20 Mean age: 71.3 ± 7.5(F) 69.6 ± 8.8(NF) | Cladosiphon okamuranus, HMF | 150 ml/day liquid (total 4.05 g fucoidan) versus no fucoidan | 6 months | Clinical Patient reported |
| Ikeguchi et al. [22] Japan | Advanced gastric cancer, n = 24 Mean age: 61.2 ± 11(F) 63.3 ± 16.2(NF) | Cladosiphon okamuranus, HMF | 150 mL/day liquid (total 4.05 g fucoidan) versus no fucoidan | 6 months | |
| Takahashi et al. [13] Japan | Metastatic cancer n = 20 Mean age: 58.9 (Single group study) | Cladosiphon novae-caledoniae, LMF | 400 mL/day liquid fucoidan (total 4 g fucoidan) | 4 weeks | Clinical Patient reported |
| Variables | Reference | Results (Fucoidan Use Group vs. Control Group, or Fucoidan Only) |
|---|---|---|
| Clinical outcomes | ||
| Disease progression status | ||
| Survival time (ST) | ||
| Ikeguchi et al. [21] | 8 (80%) vs. 6 (60%) patients still survived at 27th months, p = 0.314 | |
| Tsai et al. [5] | 18.04 vs. 12.96 months, p = 0.092 | |
| Ikeguchi et al. [22] | Mean survival time; 12.0 vs. 8.0 months, p = 0.039 | |
| Takahashi et al. [13] | Median survival time; 13.0 (IL-1β level decreased) vs. 5.0 months (IL-1β level not decreased), p = 0.02 (Single group study) | |
| Progression-free survival (PFS) | ||
| Tsai et al. [5] | 15.93 vs. 10.80 months, p = 0.075 | |
| Overall response rate (ORR) | ||
| Tsai et al. [5] | 60.7% vs. 46.2%, p = 0.284 | |
| Disease control rate (DCR) | ||
| Tsai et al. [5] | 92.8% vs. 69.2%, p = 0.026 | |
| Chemotherapy treatment periods | ||
| Ikeguchi et al. [22] | 7.4 vs. 4.6 months, p = 0.004 | |
| Ikeguchi et al. [21] | 19.9 vs. 10.8 cycles, p = 0.016 | |
| Anti-inflammatory change over time | ||
| Takahashi et al. [13] (Single group study) | 1.IL-1B (358.2 → 189.9, p = 0.01) 2.IL-6 (2198.6 → 1522.8, p = 0.02) 3.TNF-a (4819.4 → 3257.2, p = 0.03) | |
| Prognostic nutritional indexes (PNIs) | ||
| Ikeguchi et al. [22] | 47.6 vs. 39.4, p = 0.028 | |
| Patient-reported outcomes Reference Results (fucoidan vs. control, or fucoidan change overtime) | ||
| Quality of life (QoL) | ||
| Takahashi et al. [13] | No significant difference over time (QoL score 58.3 ± 5.3 → 58.3 ± 4.8; p = 0.92) (Single group study) (QoL tool: EORTC QLQ-C30) | |
| Tsai et al. [5] | No significant difference (QoL tool: EORTC QLQ-CR29) | |
| Adverse effects (AEs) | ||
| Takahashi et al. [13] | Financial difficulty score reduced (QoL score 35.0 ± 7.0 → 20.0 ± 5.6; p < 0.01) (AEs tool: EORTC QLQ-C30) | |
| Ikeguchi et al. [21] | General fatigue (Incidence 10% vs. 60%, p = 0.019) (AEs tool: NCI CTCAE) | |
| Tsai et al. [5] | Oral mucositis (Incidence 50% vs. 65.4%, p = 0.253) Pruritus (Incidence 35.7% vs. 53.9%, p = 0.180) Vomiting (Incidence 35.7% vs. 53.9%, p = 0.180) Taste problem (Incidence 64.3% vs. 80.8%, p = 0.177) Bloody stool (Incidence 14.3% vs. 30.8%, p = 0.145) (AEs tool: NCI CTCAE and EORTC-QLQ-CR29) | |
| Ikeguchi et al. [22] | Fatigue (3 vs. 7 patients, p = 0.098) Diarrhea (0 vs. 3 patients, p = 0.064) (AEs tool: NCI CTCAE) | |
3.3. Methodological Quality of Included Studies
3.4. Clinical Outcomes
3.4.1. Disease Progression Status
3.4.2. Anti-Inflammatory Effects
3.4.3. Prognostic Nutritional Indexes (PNIs)
3.5. Patient-Reported Outcomes
3.5.1. Adverse Effects (AEs)
3.5.2. Quality of Life
4. Discussion
4.1. Disease Progression Status
4.1.1. Inflammatory Markers
4.1.2. Adverse Effects
4.1.3. Quality of Life
4.2. Strengths and Limitations
4.3. Implications for Clinical Practice
4.4. Suggestions for Future Research
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A
| Citation | Q1 | Q2 | Q3 | Q4 | Q5 | Q6 | Q7 | Q8 | Q9 | Score |
|---|---|---|---|---|---|---|---|---|---|---|
| Ikeguchi et al. [21] | Y | Y | N/A | Y | Y | Y | Y | Y | Y | 8 |
| Takahashi et al. [13] | Y | U | U | U | Y | Y | Y | Y | Y | 7 |
| Ikeguchi et al. [22] | Y | Y | N/A | Y | Y | Y | Y | Y | Y | 8 |
| Citation | Q1 | Q2 | Q3 | Q4 | Q5 | Q6 | Q7 | Q8 | Q9 | Q10 | Q11 | Q12 | Q13 | Score |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Tsai et al. [5] | Y | Y | Y | Y | Y | U | U | Y | Y | Y | Y | Y | U | 10 |
References
- Buckner, C.A.; Lafrenie, R.M.; Denommee, J.A.; Caswell, J.M.; Want, D.A. Complementary and alternative medicine use in patients before and after a cancer diagnosis. Curr. Oncol. 2018, 25, e275–e281. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- National Health Service (NHS). Complementary and Alternative Medicine. 2018. Available online: https://www.nhs.uk/conditions/complementary-and-alternative-medicine (accessed on 15 January 2021).
- Bahall, M. Prevalence, patterns, and perceived value of complementary and alternative medicine among cancer patients: A cross-sectional, descriptive study. BMC Complement. Altern. Med. 2017, 17, 345. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- John, G.M.; Hershman, D.L.; Falci, L.; Shi, Z.; Tsai, W.Y.; Greenlee, H. Complementary and alternative medicine use among US cancer survivors. J. Cancer Surviv. 2016, 10, 850–864. [Google Scholar] [CrossRef] [PubMed]
- Tsai, H.L.; Tai, C.J.; Huang, C.W.; Chang, F.R.; Wang, J.Y. Efficacy of Low-Molecular-Weight Fucoidan as a Supplemental Therapy in Metastatic Colorectal Cancer Patients: A Double-Blind Randomized Controlled Trial. Mar. Drugs 2017, 15, 122. [Google Scholar] [CrossRef] [Green Version]
- Senthilkumar, K.; Manivasagan, P.; Venkatesan, J.; Kim, S.K. Brown seaweed fucoidan: Biological activity and apoptosis, growth signaling mechanism in cancer. Int. J. Biol. Macromol. 2013, 60, 366–374. [Google Scholar] [CrossRef]
- Luthuli, S.; Wu, S.; Cheng, Y.; Zheng, X.; Wu, M.; Tong, H. Therapeutic Effects of Fucoidan: A Review on Recent Studies. Mar. Drugs 2019, 17, 487. [Google Scholar] [CrossRef] [Green Version]
- Wu, L.; Sun, J.; Su, X.; Yu, Q.; Yu, Q.; Zhang, P. A review about the development of fucoidan in antitumor activity: Progress and challenges. Carbohydr. Polym. 2016, 154, 96–111. [Google Scholar] [CrossRef]
- Jang, J.Y.; Moon, S.Y.; Joo, H.G. Differential effects of fucoidans with low and high molecular weight on the viability and function of spleen cells. Food Chem. Toxicol. 2014, 68, 234–238. [Google Scholar] [CrossRef]
- You, S.G.; Yang, C.; Lee, H.Y.; Lee, B.Y. Molecular characteristics of partially hydrolyzed fucoidans from sporophyll of Undaria pinnatifida and their in vitro anticancer activity. Food Chem. 2010, 119, 554–559. [Google Scholar] [CrossRef]
- Moussavou, G.; Kwak, D.H.; Obiang-Obonou, B.W.; Maranguy, C.A.; Dinzouna-Boutamba, S.D.; Lee, D.H.; Pissibanganga, O.G.; Ko, K.; Seo, J.I.; Choo, Y.K. Anticancer effects of different seaweeds on human colon and breast cancers. Mar. Drugs 2014, 12, 4898–4911. [Google Scholar] [CrossRef]
- Tocaciu, S.; Oliver, L.J.; Lowenthal, R.M.; Peterson, G.M.; Patel, R.; Shastri, M.; McGuinness, G.; Olesen, I.; Fitton, J.H. The Effect of Undaria pinnatifida Fucoidan on the Pharmacokinetics of Letrozole and Tamoxifen in Patients with Breast Cancer. Integr. Cancer Ther. 2018, 17, 99–105. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Takahashi, H.; Kawaguchi, M.; Kitamura, K.; Narumiya, S.; Kawamura, M.; Tengan, I.; Nishimoto, S.; Hanamure, Y.; Majima, Y.; Tsubura, S.; et al. An Exploratory Study on the Anti-inflammatory Effects of Fucoidan in Relation to Quality of Life in Advanced Cancer Patients. Integr. Cancer Ther. 2018, 17, 282–291. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wu, C.Y.; Chen, Q.C.; Syu, W.J.; Yih, K.H.; Wang, H.F. A Preliminary Study on the Application of Anti-Aging Cream with Small Molecular Fucoidan to Skin. HungKuang Acad. Rev. 2017, 79, 207–222. [Google Scholar] [CrossRef]
- Shih, P.H.; Shiue, S.J.; Chen, C.N.; Cheng, S.W.; Lin, H.Y.; Wu, L.W.; Wu, M.S. Fucoidan and Fucoxanthin Attenuate Hepatic Steatosis and Inflammation of NAFLD through Modulation of Leptin/Adiponectin Axis. Mar. Drugs 2021, 19, 148. [Google Scholar] [CrossRef] [PubMed]
- Hwang, P.A.; Hung, Y.L.; Chien, S.Y. Inhibitory activity of Sargassum hemiphyllum sulfated polysaccharide in arachidonic acid-induced animal models of inflammation. J. Food Drug Anal. 2015, 23, 49–56. [Google Scholar] [CrossRef] [Green Version]
- Lin, H.V.; Tsou, Y.C.; Chen, Y.T.; Lu, W.J.; Hwang, P.A. Effects of Low-Molecular-Weight Fucoidan and High Stability Fucoxanthin on Glucose Homeostasis, Lipid Metabolism, and Liver Function in a Mouse Model of Type II Diabetes. Mar. Drugs 2017, 15, 113. [Google Scholar] [CrossRef] [Green Version]
- Hsu, H.Y.; Hwang, P.A. Clinical applications of fucoidan in translational medicine for adjuvant cancer therapy. Clin. Transl. Med. 2019, 8, 15. [Google Scholar] [CrossRef] [Green Version]
- Wang, Y.; Xing, M.; Cao, Q.; Ji, A.; Liang, H.; Song, S. Biological Activities of Fucoidan and the Factors Mediating Its Therapeutic Effects: A Review of Recent Studies. Mar. Drugs 2019, 17, 183. [Google Scholar] [CrossRef] [Green Version]
- Tufanaru, C.; Munn, Z.; Aromataris, E.; Campbell, J.; Hopp, L. Chapter 3: Systematic reviews of effectiveness. In JBI Manual for Evidence Synthesis; Aromataris, E., Munn, Z., Eds.; JBI: Adelaide, Australia, 2020; Available online: https://synthesismanual.jbi.global (accessed on 15 December 2020).
- Ikeguchi, M.; Yamamoto, M.; Arai, Y.; Maeta, Y.; Ashida, K.; Katano, K.; Miki, Y.; Kimura, T. Fucoidan reduces the toxicities of chemotherapy for patients with unresectable advanced or recurrent colorectal cancer. Oncol. Lett. 2011, 2, 319–322. [Google Scholar] [CrossRef]
- Ikeguchi, M.; Saito, H.; Miki, Y.; Kimura, T. Effect of fucoidan dietary supplement on the chemotherapy treatment of patients with unresectable advanced gastric cancer. J. Cancer Ther. 2015, 6, 1020–1026. [Google Scholar] [CrossRef] [Green Version]
- Oncology Center of Excellence; Center for Drug Evaluation and Research (CDER); Center for Biologics Evaluation and Research (CBER) at the Food and Drug Administration; Food and Drug Administration. Clinical Trial Endpoints for the Approval of Cancer Drugs and Biologics Guidance for Industry. 2018. Available online: https://www.fda.gov/media/71195/download (accessed on 15 January 2021).
- Ben-Aharon, O.; Magnezi, R.; Leshno, M.; Goldstein, D.A. Median Survival or Mean Survival: Which Measure Is the Most Appropriate for Patients, Physicians, and Policymakers? Oncologist 2019, 24, 1469–1478. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, T.; Molassiotis, A.; Chung, B.P.M.; Tan, J.Y. Unmet care needs of advanced cancer patients and their informal caregivers: A systematic review. BMC Palliat. Care 2018, 17, 96. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Litiere, S.; Collette, S.; de Vries, E.G.; Seymour, L.; Bogaerts, J. RECIST—Learning from the past to build the future. Nat. Rev. Clin. Oncol. 2017, 14, 187–192. [Google Scholar] [CrossRef]
- Mushti, S.L.; Mulkey, F.; Sridhara, R. Evaluation of Overall Response Rate and Progression-Free Survival as Potential Surrogate Endpoints for Overall Survival in Immunotherapy Trials. Clin. Cancer Res. 2018, 24, 2268–2275. [Google Scholar] [CrossRef] [Green Version]
- Shi, Q.; Sargent, D.J. Meta-analysis for the evaluation of surrogate endpoints in cancer clinical trials. Int. J. Clin. Oncol. 2009, 14, 102–111. [Google Scholar] [CrossRef]
- Park, J.; Cha, J.D.; Choi, K.M.; Lee, K.Y.; Han, K.M.; Jang, Y.S. Fucoidan inhibits LPS-induced inflammation in vitro and during the acute response in vivo. Int. Immunopharmacol. 2017, 43, 91–98. [Google Scholar] [CrossRef] [PubMed]
- O’Higgins, C.M.; Brady, B.; O’Connor, B.; Walsh, D.; Reilly, R.B. The pathophysiology of cancer-related fatigue: Current controversies. Support. Care Cancer 2018, 26, 3353–3364. [Google Scholar] [CrossRef]
- Chui, P.L.; Abdullah, K.L.; Wong, L.P.; Taib, N.A. Quality of Life in CAM and Non-CAM Users among Breast Cancer Patients during Chemotherapy in Malaysia. PLoS ONE 2015, 10, e0139952. [Google Scholar] [CrossRef]
- Erku, D.A. Complementary and Alternative Medicine Use and Its Association with Quality of Life among Cancer Patients Receiving Chemotherapy in Ethiopia: A Cross-Sectional Study. Evid. Based Complement. Altern. Med. 2016, 2016, 2809875. [Google Scholar] [CrossRef] [Green Version]
- Jang, A.; Kang, D.H.; Kim, D.U. Complementary and Alternative Medicine Use and Its Association with Emotional Status and Quality of Life in Patients with a Solid Tumor: A Cross-Sectional Study. J. Altern. Complement. Med. 2017, 23, 362–369. [Google Scholar] [CrossRef] [Green Version]
- Paul, M.; Davey, B.; Senf, B.; Stoll, C.; Munstedt, K.; Mucke, R.; Micke, O.; Prott, F.J.; Buentzel, J.; Hubner, J. Patients with advanced cancer and their usage of complementary and alternative medicine. J. Cancer Res. Clin. Oncol. 2013, 139, 1515–1522. [Google Scholar] [CrossRef] [PubMed]
- Yildirim, Y. Patterns of the use of complementary and alternative medicine in women with metastatic cancer. Cancer Nurs. 2010, 33, 194–200. [Google Scholar] [CrossRef] [PubMed]
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wu, C.-J.; Yeh, T.-P.; Wang, Y.-J.; Hu, H.-F.; Tsay, S.-L.; Liu, L.-C. Effectiveness of Fucoidan on Supplemental Therapy in Cancer Patients: A Systematic Review. Healthcare 2022, 10, 923. https://doi.org/10.3390/healthcare10050923
Wu C-J, Yeh T-P, Wang Y-J, Hu H-F, Tsay S-L, Liu L-C. Effectiveness of Fucoidan on Supplemental Therapy in Cancer Patients: A Systematic Review. Healthcare. 2022; 10(5):923. https://doi.org/10.3390/healthcare10050923
Chicago/Turabian StyleWu, Chih-Jung, Tzu-Pei Yeh, Ya-Jung Wang, Hsiao-Fang Hu, Shiow-Luan Tsay, and Liang-Chih Liu. 2022. "Effectiveness of Fucoidan on Supplemental Therapy in Cancer Patients: A Systematic Review" Healthcare 10, no. 5: 923. https://doi.org/10.3390/healthcare10050923
APA StyleWu, C.-J., Yeh, T.-P., Wang, Y.-J., Hu, H.-F., Tsay, S.-L., & Liu, L.-C. (2022). Effectiveness of Fucoidan on Supplemental Therapy in Cancer Patients: A Systematic Review. Healthcare, 10(5), 923. https://doi.org/10.3390/healthcare10050923