
Stabilization of the Distal Radioulnar Joint with or without Triangular Fibrocartilage Complex Tear by an External Wrist Band Brace: A Cadaveric Study


{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Specimens
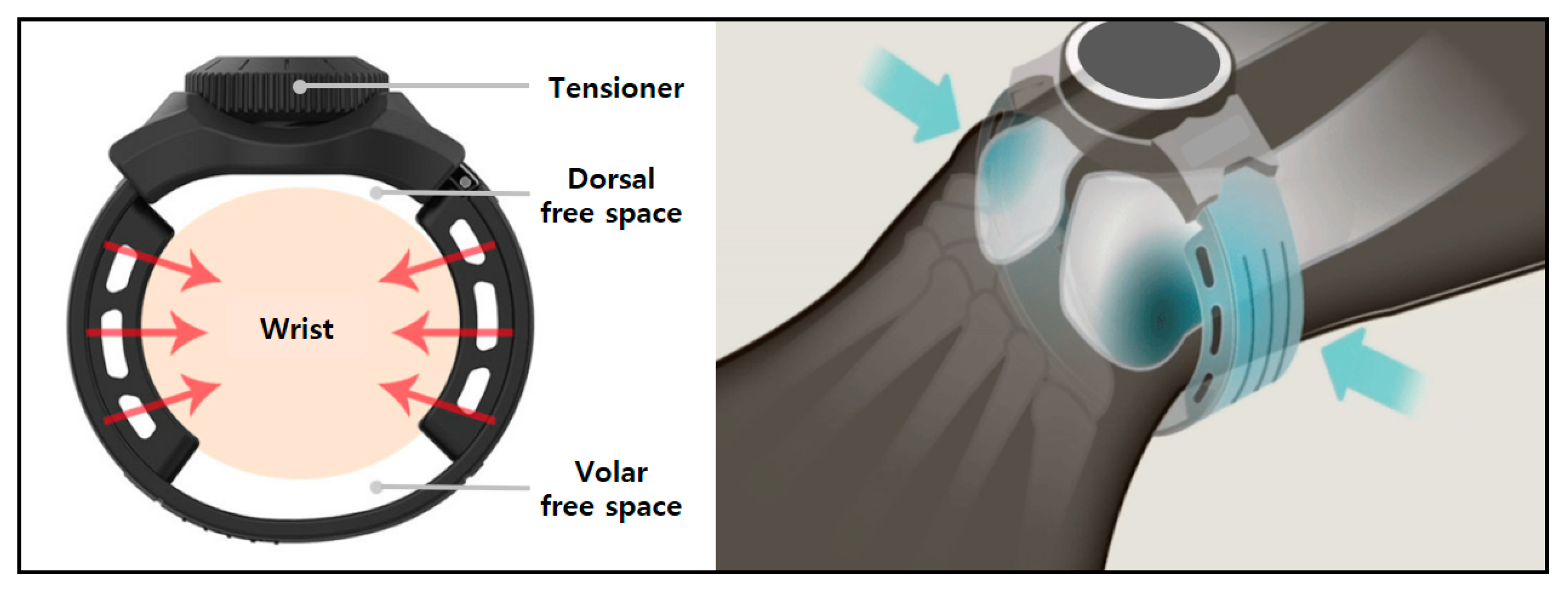
2.2. Concept of the Brace
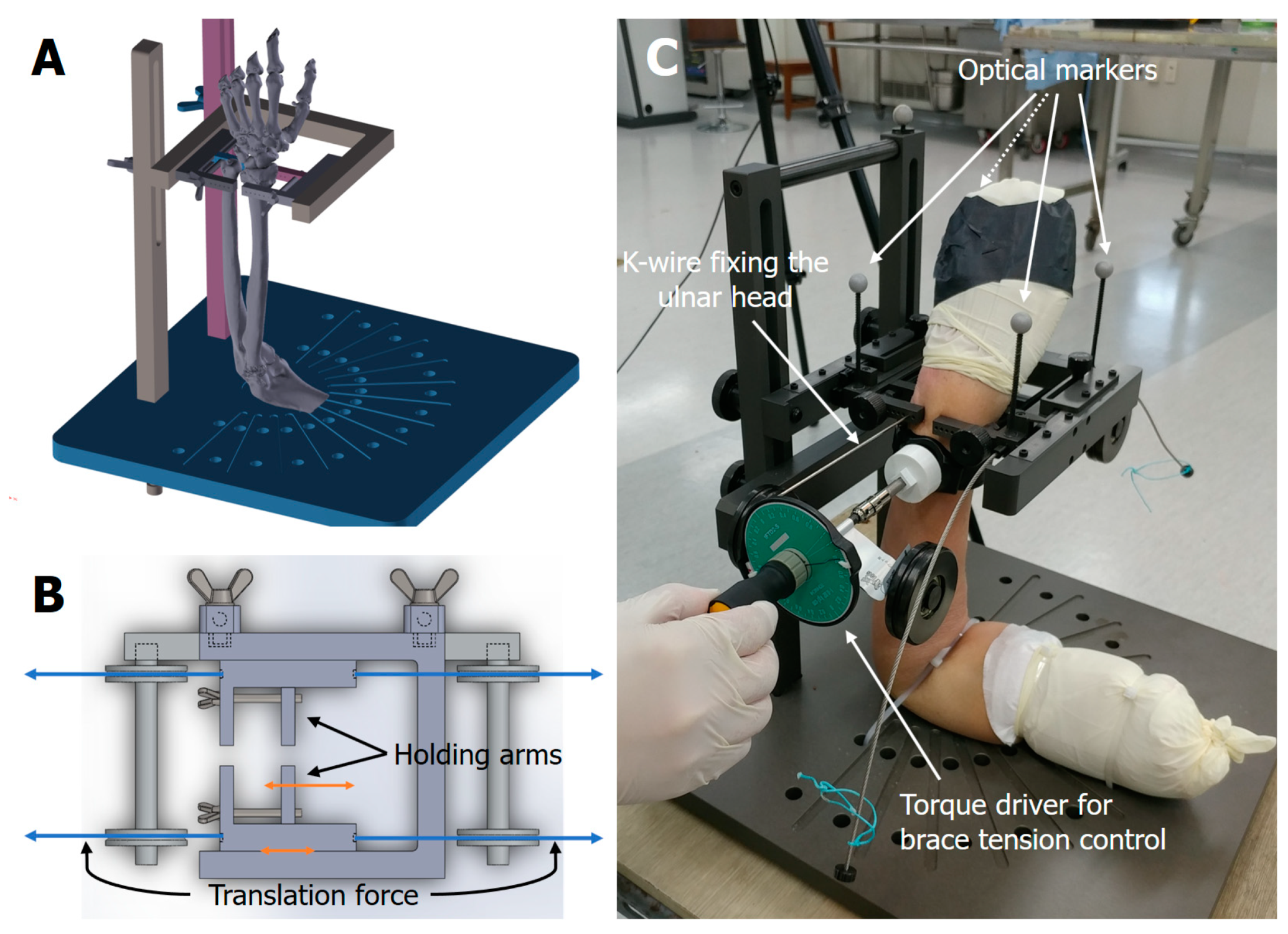
2.3. Biomechanical Testing
2.4. Test Setting and Translation Measurement
2.5. Statistical Analysis
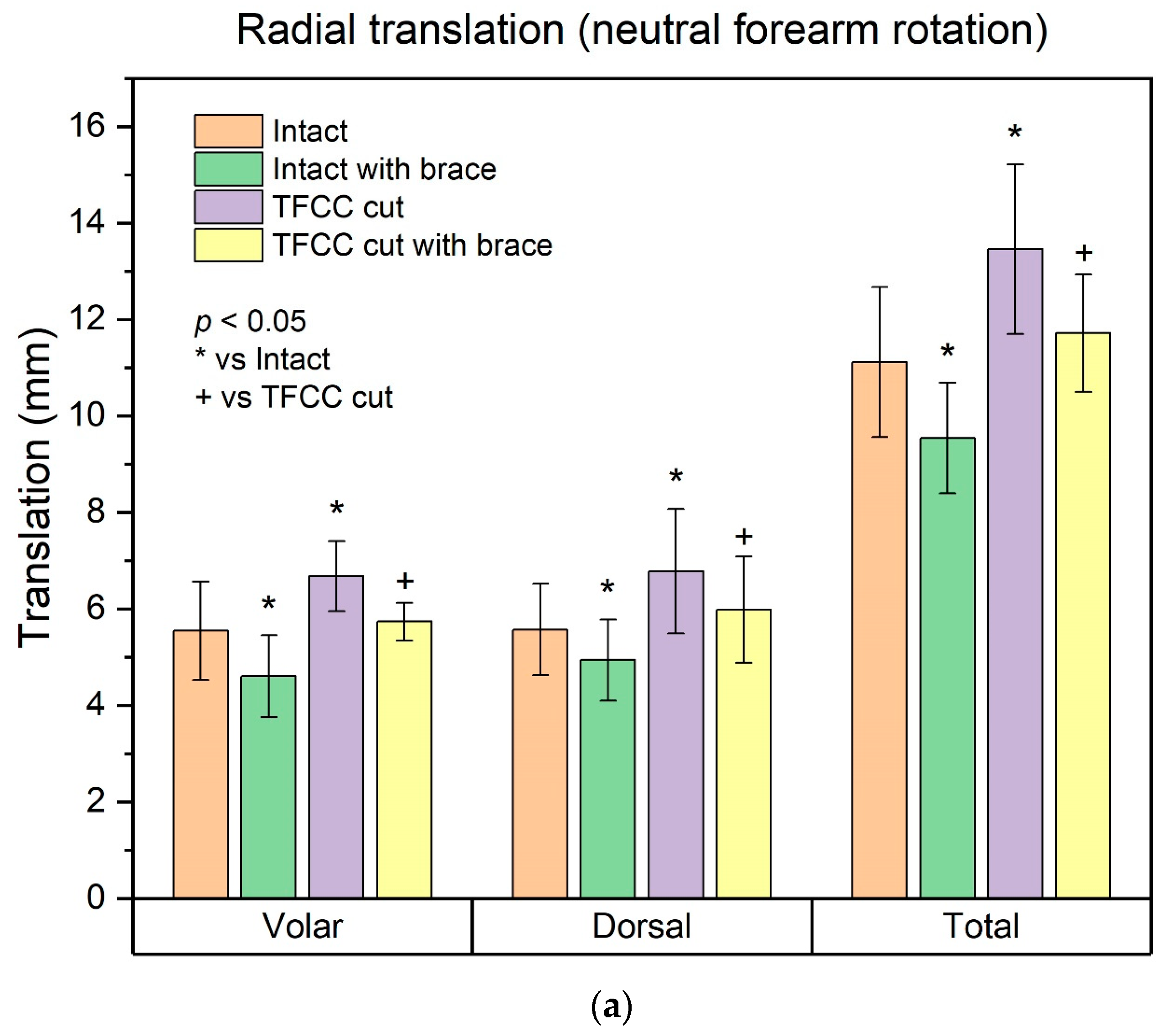
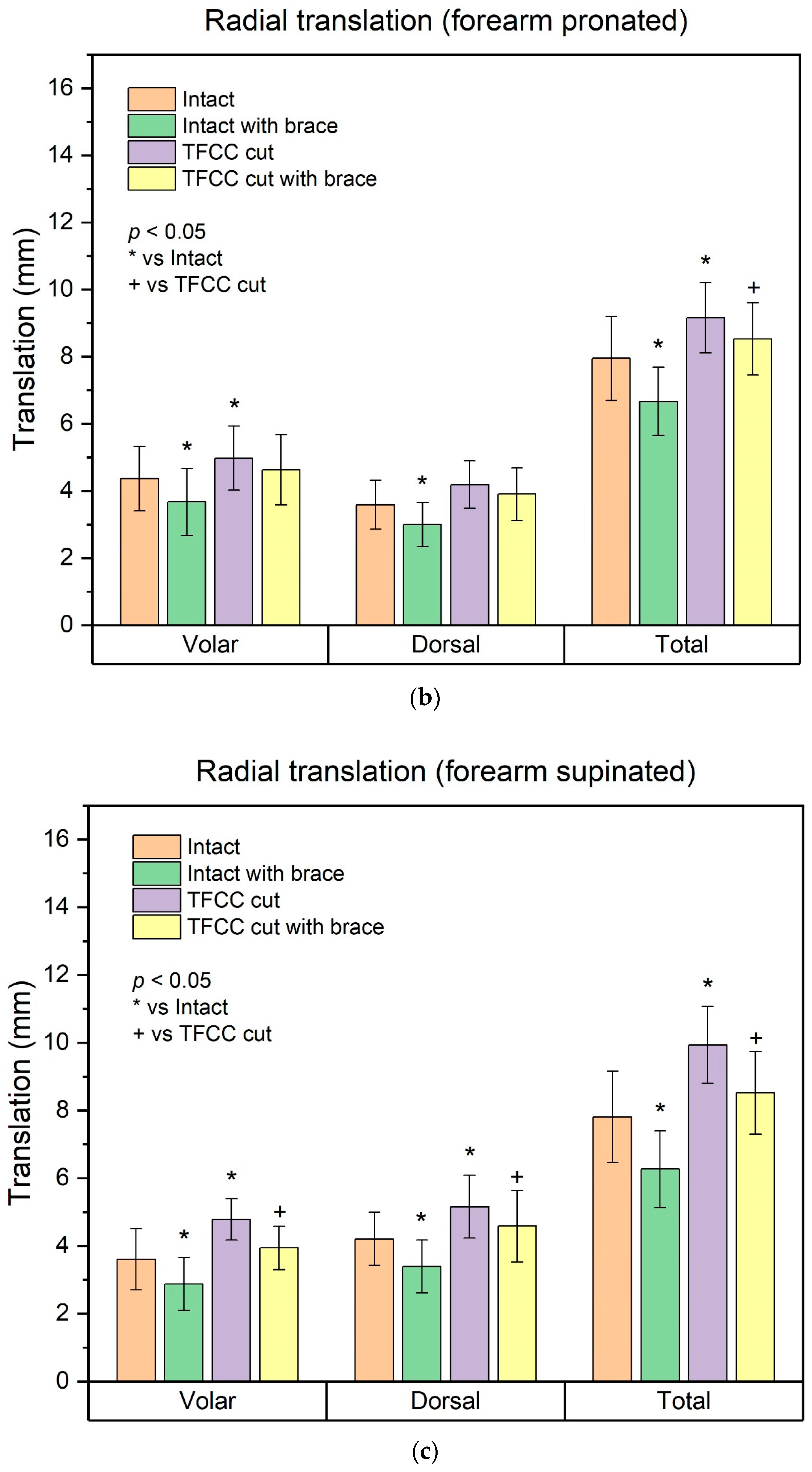
3. Results
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Szabo, R.M. Distal radioulnar joint instability. J. Bone Jt. Surg. Am. 2006, 88, 884–894. [Google Scholar] [CrossRef] [PubMed]
- Kleinman, W.B. Stability of the distal radioulna joint: Biomechanics, pathophysiology, physical diagnosis, and restoration of function what we have learned in 25 years. J. Hand Surg. Am. 2007, 32, 1086–1106. [Google Scholar] [CrossRef] [PubMed]
- Palmer, A.K.; Werner, F.W. The triangular fibrocartilage complex of the wrist--anatomy and function. J. Hand Surg. Am. 1981, 6, 153–162. [Google Scholar] [CrossRef]
- Spies, C.K.; Langer, M.; Muller, L.P.; Oppermann, J.; Unglaub, F. Distal radioulnar joint instability: Current concepts of treatment. Arch. Orthop. Trauma Surg. 2020, 140, 639–650. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lester, B.; Halbrecht, J.; Levy, I.M.; Gaudinez, R. “Press test” for office diagnosis of triangular fibrocartilage complex tears of the wrist. Ann. Plast. Surg. 1995, 35, 41–45. [Google Scholar] [CrossRef] [PubMed]
- Atzei, A. New trends in arthroscopic management of type 1-B TFCC injuries with DRUJ instability. J. Hand Surg. Eur. Vol. 2009, 34, 582–591. [Google Scholar] [CrossRef]
- Lee, S.K.; Kim, K.J.; Cha, Y.H.; Choy, W.S. Conservative Treatment Is Sufficient for Acute Distal Radioulnar Joint Instability with Distal Radius Fracture. Ann. Plast. Surg. 2016, 77, 297–304. [Google Scholar] [CrossRef]
- Xiao, A.X.; Graf, A.R.; Dawes, A.; Daley, C.; Wagner, E.R.; Gottschalk, M.B. Management of Acute Distal Radioulnar Joint Instability Following a Distal Radius Fracture: A Systematic Review and Meta-Analysis. J. Hand Surg. Glob. Online 2021, 3, 133–138. [Google Scholar] [CrossRef]
- Lee, J.K.; Hwang, J.Y.; Lee, S.Y.; Kwon, B.C. What is the Natural History of the Triangular Fibrocartilage Complex Tear without Distal Radioulnar Joint Instability? Clin. Orthop. Relat. Res. 2019, 477, 442–449. [Google Scholar] [CrossRef]
- Boynton, J.F.; Budoff, J.E.; Clifford, J.W. The effect of forearm bracing on radioulnar impingement. J. Hand Surg. Br. 2005, 30, 157–161. [Google Scholar] [CrossRef]
- Jaffe, R.; Chidgey, L.K.; LaStayo, P.C. The distal radioulnar joint: Anatomy and management of disorders. J. Hand Ther. 1996, 9, 129–138. [Google Scholar] [CrossRef]
- Slaughter, A.; Miles, L.; Fleming, J.; McPhail, S. A comparative study of splint effectiveness in limiting forearm rotation. J. Hand Ther. 2010, 23, 241–247; quiz 248. [Google Scholar] [CrossRef] [PubMed]
- Park, M.J.; Jagadish, A.; Yao, J. The rate of triangular fibrocartilage injuries requiring surgical intervention. Orthopedics 2010, 33, 806. [Google Scholar] [CrossRef] [PubMed]
- O’Brien, V.H.; Thurn, J. A simple distal radioulnar joint orthosis. J. Hand Ther. 2013, 26, 287–290. [Google Scholar] [CrossRef]
- Barlow, S.J. A Non-surgical Intervention for Triangular Fibrocartilage Complex Tears. Physiother. Res. Int. 2016, 21, 271–276. [Google Scholar] [CrossRef]
- Millard, G.M.; Budoff, J.E.; Paravic, V.; Noble, P.C. Functional bracing for distal radioulnar joint instability. J. Hand Surg. Am. 2002, 27, 972–977. [Google Scholar] [CrossRef]
- Onishi, T.; Omokawa, S.; Iida, A.; Nakanishi, Y.; Kira, T.; Moritomo, H.; Ruxasagluwang, S.; Kraisarin, J.; Shimizu, T.; Tanaka, Y. Biomechanical study of distal radioulnar joint ballottement test. J. Orthop. Res. 2017, 35, 1123–1127. [Google Scholar] [CrossRef]
- Pickering, G.T.; Nagata, H.; Giddins, G.E. In-vivo three-dimensional measurement of distal radioulnar joint translation in normal and clinically unstable populations. J. Hand Surg. Eur. Vol. 2016, 41, 521–526. [Google Scholar] [CrossRef]
- Watanabe, H.; Berger, R.A.; Berglund, L.J.; Zobitz, M.E.; An, K.N. Contribution of the interosseous membrane to distal radioulnar joint constraint. J. Hand Surg. Am. 2005, 30, 1164–1171. [Google Scholar] [CrossRef]
- Sander, A.L.; Sommer, K.; Kaiser, A.K.; Marzi, I.; Frank, J. Outcome of conservative treatment for triangular fibrocartilage complex lesions with stable distal radioulnar joint. Eur. J. Trauma Emerg. Surg. 2021, 47, 1621–1625. [Google Scholar] [CrossRef] [Green Version]
- Jawed, A.; Ansari, M.T.; Gupta, V. TFCC injuries: How we treat? J. Clin. Orthop. Trauma 2020, 11, 570–579. [Google Scholar] [CrossRef] [PubMed]
- Khuyagbaatar, B.; Lee, S.-J.; Cheon, M.; Batbayar, T.; Ganbat, D.; Kim, Y.H. Effect of wrist-wearing distal radioulnar joint stabilizer on distal radioulnar joint instability using a forearm finite element model. J. Mech. Sci. Technol. 2019, 33, 2503–2508. [Google Scholar] [CrossRef]
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shin, S.-H.; Park, T.; Hong, E.; Kwak, D.-S.; Chung, Y.-G. Stabilization of the Distal Radioulnar Joint with or without Triangular Fibrocartilage Complex Tear by an External Wrist Band Brace: A Cadaveric Study. Healthcare 2022, 10, 828. https://doi.org/10.3390/healthcare10050828
Shin S-H, Park T, Hong E, Kwak D-S, Chung Y-G. Stabilization of the Distal Radioulnar Joint with or without Triangular Fibrocartilage Complex Tear by an External Wrist Band Brace: A Cadaveric Study. Healthcare. 2022; 10(5):828. https://doi.org/10.3390/healthcare10050828
Chicago/Turabian StyleShin, Seung-Han, Taeyong Park, Eunah Hong, Dai-Soon Kwak, and Yang-Guk Chung. 2022. "Stabilization of the Distal Radioulnar Joint with or without Triangular Fibrocartilage Complex Tear by an External Wrist Band Brace: A Cadaveric Study" Healthcare 10, no. 5: 828. https://doi.org/10.3390/healthcare10050828
APA StyleShin, S.-H., Park, T., Hong, E., Kwak, D.-S., & Chung, Y.-G. (2022). Stabilization of the Distal Radioulnar Joint with or without Triangular Fibrocartilage Complex Tear by an External Wrist Band Brace: A Cadaveric Study. Healthcare, 10(5), 828. https://doi.org/10.3390/healthcare10050828