
Prevalence and Associated Factors of Erosive Tooth Wear among Preschool Children—A Systematic Review and Meta-Analysis



Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
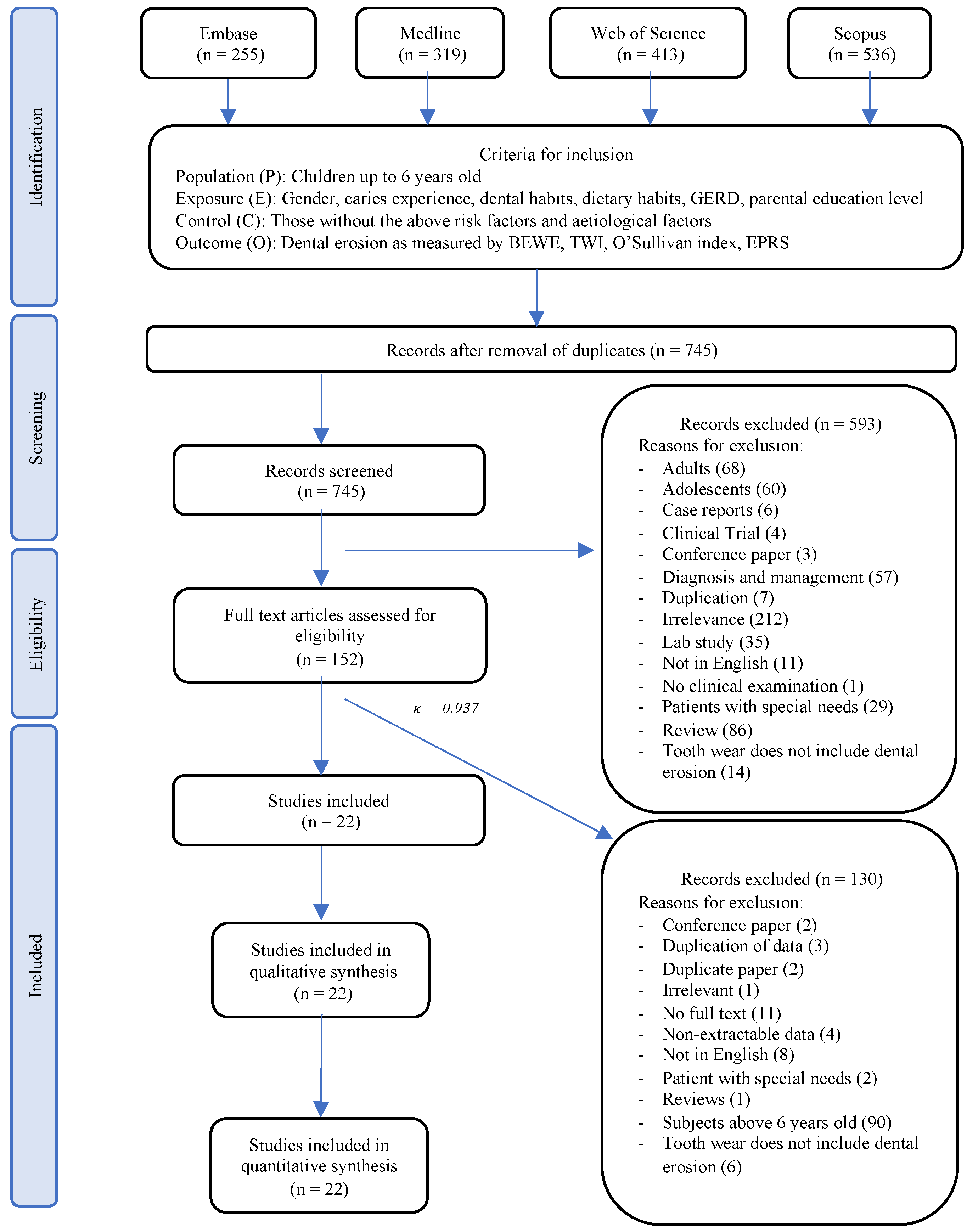
2.2. Eligibility Criteria
- Population (P): individuals with primary dentition up to age 6;
- Exposure (E) and Comparison (C) factors: gender, dental habits (such as frequency of brushing of teeth), dietary habits (such as frequency of consumption of fruit juice, soft drinks, and fruits), medical conditions (such as GERD and vomiting), and parental education level;
- Outcome (O): prevalence of erosive tooth wear, measured by different erosion indices such as Basic Erosive Wear Examination (BEWE), Tooth Wear Index (TWI), O’Sullivan’s Index, and Erosion Partial Recording System (EPRS); and
- Studies (S): observational studies, such as cohort, case–control, and cross-sectional studies on the prevalence and risk factors of erosive tooth wear in children up to 7 years of age with full texts written in English.
- Irrelevant studies;
- Studies on other types of tooth wear that were not erosive tooth wear;
- Studies on diagnosis and management of erosive tooth wear only;
- Studies reporting prevalence without conducting a clinical examination;
- Studies including individuals older than 7 years old or those with special needs;
- Case reports, clinical trials, laboratory studies, conference papers, and reviews; and
- Studies with non-extractable data, studies not in English, and duplicated studies.
2.3. Search Strategy
2.4. Selection of Studies
2.5. Data Extraction
2.6. Assessment of Risk of Bias
2.7. Data Synthesis
2.8. Assessment of Heterogeneity
2.9. Assessment of Publication Bias
2.10. Assessment of Quality of Evidence
3. Results
3.1. Study Selection
3.2. Study Characteristics
3.3. Risk of Bias
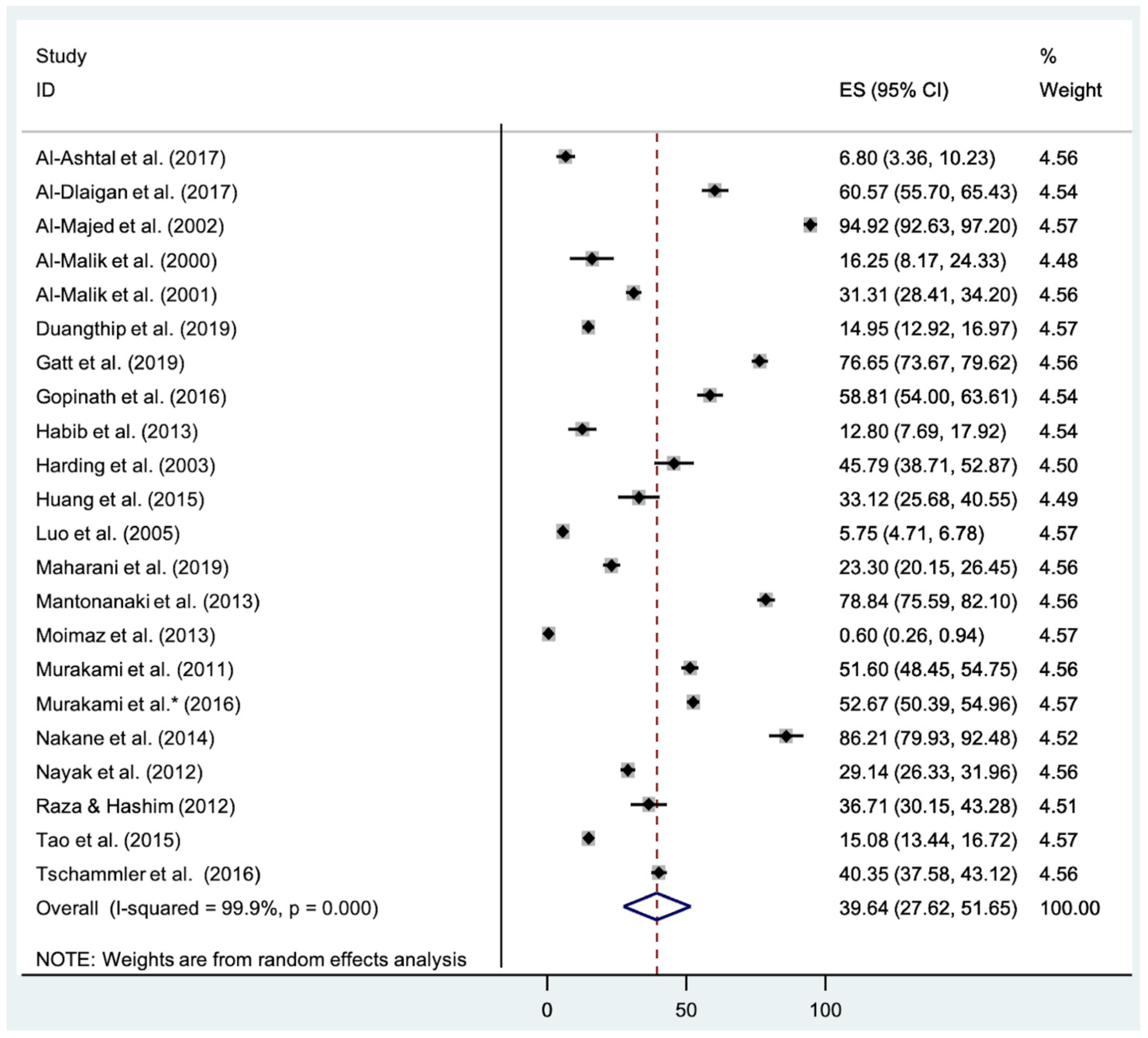
3.4. Prevalence of Erosive Tooth Wear
3.5. Meta-Analysis
3.5.1. Gender
3.5.2. Digestive Disorders
3.5.3. Birthplace
3.5.4. Caries Prevalence
3.5.5. Parental Education
3.5.6. Toothbrushing
3.6. Meta-Regression
3.6.1. Age
3.6.2. Erosion Indices
3.6.3. Sample Size
3.6.4. Human Development Index (HDI)
3.6.5. Year of Recruitment
3.7. Narrative Review
3.7.1. Fruit Juice Frequency
3.7.2. Soft Drinks Frequency
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Schlueter, N.; Amaechi, B.T.; Bartlett, D.; Buzalaf, M.A.R.; Carvalho, T.S.; Ganss, C.; Hara, A.T.; Huysmans, M.; Lussi, A.; Moazzez, R.; et al. Terminology of Erosive Tooth Wear: Consensus Report of a Workshop Organized by the ORCA and the Cariology Research Group of the IADR. Caries Res. 2020, 54, 2–6. [Google Scholar] [CrossRef] [PubMed]
- Sivasithamparam, K.; Harbrow, D.; Vinczer, E.; Young, W.G. Endodontic sequelae of dental erosion. Aust. Dent. J. 2003, 48, 97–101. [Google Scholar] [CrossRef] [PubMed]
- Johansson, A.K.; Sorvari, R.; Birkhed, D.; Meurman, J.H. Dental erosion in deciduous teeth—An in vivo and in vitro study. J. Dent. 2001, 29, 333–340. [Google Scholar] [CrossRef]
- Gillborg, S.; Åkerman, S.; Ekberg, E. Tooth wear in Swedish adults-A cross-sectional study. J. Oral Rehabil. 2020, 47, 235–245. [Google Scholar] [CrossRef]
- Marró, M.L.; Aránguiz, V.; Ramirez, V.; Lussi, A. Prevalence of erosive tooth wear in Chilean adults, 2016: A cross-sectional study. J. Oral Rehabil. 2020, 47, 467–472. [Google Scholar] [CrossRef]
- Zhang, S.; Chau, A.M.; Lo, E.C.; Chu, C.H. Dental caries and erosion status of 12-year-old Hong Kong children. BMC Public Health 2014, 14, 7. [Google Scholar] [CrossRef]
- Luo, Y.; Zeng, X.J.; Du, M.Q.; Bedi, R. The prevalence of dental erosion in preschool children in China. J. Dent. 2005, 33, 115–121. [Google Scholar] [CrossRef]
- Pace, F.; Pallotta, S.; Tonini, M.; Vakil, N.; Bianchi Porro, G. Systematic review: Gastro-oesophageal reflux disease and dental lesions. Aliment. Pharmacol. Ther. 2008, 27, 1179–1186. [Google Scholar] [CrossRef]
- Schlueter, N.; Luka, B. Erosive tooth wear-a review on global prevalence and on its prevalence in risk groups. Br. Dent. J. 2018, 224, 364–370. [Google Scholar] [CrossRef]
- Chan, A.S.; Tran, T.T.K.; Hsu, Y.H.; Liu, S.Y.S.; Kroon, J. A systematic review of dietary acids and habits on dental erosion in adolescents. Int. J. Paediatr. Dent. 2020, 30, 713–733. [Google Scholar] [CrossRef]
- Smits, K.P.J.; Listl, S.; Jevdjevic, M. Vegetarian diet and its possible influence on dental health: A systematic literature review. Community Dent. Oral Epidemiol. 2020, 48, 7–13. [Google Scholar] [CrossRef] [PubMed]
- Wiegand, A.; Müller, J.; Werner, C.; Attin, T. Prevalence of erosive tooth wear and associated risk factors in 2–7-year-old German kindergarten children. Oral Dis. 2006, 12, 117–124. [Google Scholar] [CrossRef] [PubMed]
- Nayak, S.S.; Ashokkumar, B.R.; Ankola, A.V.; Hebbal, M.I. Association of Erosion with Dietary Factors Among 5-year-old Children In India. J. Dent. Child. 2012, 79, 122–129. [Google Scholar]
- de Oliveira, P.A.D.; Paiva, S.M.; de Abreu, M.; Auad, S.M. Dental Erosion in Children with Gastroesophageal Reflux Disease. Pediatr. Dent. 2016, 38, 246–250. [Google Scholar] [CrossRef]
- Duangthip, D.; Chen, K.J.; Gao, S.S.; Lussi, A.; Lo, E.C.M.; Chu, C.H. Erosive tooth wear among preschool children in Hong Kong. Int. J. Paediatr. Dent. 2019, 29, 185–192. [Google Scholar] [CrossRef]
- Millwood, N.; Willie-Tyndale, D.; James, K.; Holder-Nevins, D. Factors associated with the decayed, missing, filled teeth (DMFT) rate: A comparison of rural and urban children ages three to five years old. West. Indian Med. J. 2016, 65 (Suppl. 6), 34. [Google Scholar]
- Moola, S.; Munn, Z.; Sears, K.; Sfetcu, R.; Currie, M.; Lisy, K.; Tufanaru, C.; Qureshi, R.; Mattis, P.; Mu, P. Conducting systematic reviews of association (etiology): The Joanna Briggs Institute’s approach. JBI Evid. Implement. 2015, 13, 163–169. [Google Scholar] [CrossRef]
- McKenzie, J.E.; Brennan, S.E.; Ryan, R.E.; Thomson, H.J.; Johnston, R.V.; Cochrane Statistical Methods Group. Summarizing study characteristics and preparing for synthesis. In Cochrane Handbook for Systematic Reviews of Interventions; Wiley-Blackwell: Hoboken, NJ, USA, 2019; pp. 229–240. [Google Scholar]
- Deeks, J.J.; Higgins, J.P.; Altman, D.G.; Cochrane Statistical Methods Group. Analysing data and undertaking meta-analyses. In Cochrane Handbook for Systematic Reviews of Interventions; Wiley-Blackwell: Hoboken, NJ, USA, 2019; pp. 241–284. [Google Scholar]
- Guyatt, G.; Rennie, D.; Meade, M.; Cook, D.; American Medical, A. Users’ Guides to the Medical Literature: A Manual for Evidence-Based Clinical Practice, 3rd ed.; McGraw-Hill Education: New York, NY, USA, 2015. [Google Scholar]
- Higgins, J.P.T.; Altman, D.G.; Gøtzsche, P.C.; Jüni, P.; Moher, D.; Oxman, A.D.; Savović, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A.C. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ 2011, 343, 889–893. [Google Scholar] [CrossRef]
- Atkins, D.; Best, D.; Briss, P.A.; Eccles, M.; Falck-Ytter, Y.; Flottorp, S.; Guyatt, G.H.; Harbour, R.T.; Haugh, M.C.; Henry, D.; et al. Grading quality of evidence and strength of recommendations. BMJ (Clin. Res. Ed.) 2004, 328, 1490. [Google Scholar] [CrossRef]
- Al-Ashtal, A.; Johansson, A.; Omar, R.; Johansson, A.K. Dental erosion in groups of Yemeni children and adolescents and the modification of an erosion partial recording system. Int. J. Paediatr. Dent. 2017, 27, 283–292. [Google Scholar] [CrossRef]
- Al-Dlaigan, Y.H.; Al-Meedania, L.A.; Anil, S. The influence of frequently consumed beverages and snacks on dental erosion among preschool children in Saudi Arabia. Nutr. J. 2017, 16, 80. [Google Scholar] [CrossRef] [PubMed]
- Al-Majed, I.; Maguire, A.; Murray, J.J. Risk factors for dental erosion in 5–6 year old and 12–14 year old boys in Saudi Arabia. Community Dent. Oral Epidemiol. 2002, 30, 38–46. [Google Scholar] [CrossRef] [PubMed]
- Al-Malik, M.; Holt, R.D. The prevalence of caries and of tooth tissue loss in a group of children living in a social welfare institute in Jeddah, Saudi Arabia. Int. Dent. J. 2000, 50, 289–292. [Google Scholar] [CrossRef] [PubMed]
- Al-Malik, M.I.; Holt, R.D.; Bedi, R. The relationship between erosion, caries and rampant caries and dietary habits in preschool children in Saudi Arabia. Int. J. Paediatr. Dent. 2001, 11, 430–439. [Google Scholar] [PubMed]
- Gatt, G.; Attard, N. Erosive wear of the primary dentition: Who is aware of it? Eur. Arch. Paediatr. Dent. Off. J. Eur. Acad. Paediatr. Dent. 2019, 20, 285–294. [Google Scholar] [CrossRef] [PubMed]
- Gopinath, V.K. The prevalence of dental erosion in 5-year-old preschoolers in Sharjah, United Arab Emirates. Eur. J. Dent. 2016, 10, 215–219. [Google Scholar] [CrossRef]
- Habib, M.; Hottel, T.L.; Hong, L. Prevalence and risk factors of dental erosion in American children. J. Clin. Pediatr. Dent. 2013, 38, 143–148. [Google Scholar] [CrossRef]
- Harding, M.A.; Whelton, H.; O’Mullane, D.M.; Cronin, M. Dental erosion in 5-year-old Irish school children and associated factors: A pilot study. Community Dent. Health 2003, 20, 165–170. [Google Scholar]
- Huang, L.L.; Leishman, S.; Newman, B.; Seow, W.K. Association of erosion with timing of detection and selected risk factors in primary dentition: A longitudinal study. Int. J. Paediatr. Dent. 2015, 25, 165–173. [Google Scholar] [CrossRef]
- Maharani, D.A.; Pratiwi, A.N.; Setiawati, F.; Zhang, S.; Gao, S.S.; Chu, C.H.; Rahardjo, A. Tooth wear among five-year-old children in Jakarta, Indonesia. BMC Oral Health 2019, 19, 192. [Google Scholar] [CrossRef]
- Mantonanaki, M.; Koletsi-Kounari, H.; Mamai-Homata, E.; Papaioannou, W. Dental erosion prevalence and associated risk indicators among preschool children in Athens, Greece. Clin. Oral Investig. 2013, 17, 585–593. [Google Scholar] [CrossRef] [PubMed]
- Moimaz, S.A.; Araujo, P.C.; Chiba, F.Y.; Garbin, C.A.; Saliba, N.A. Prevalence of deciduous tooth erosion in childhood. Int. J. Dent. Hyg. 2013, 11, 226–230. [Google Scholar] [CrossRef] [PubMed]
- Murakami, C.; Oliveira, L.B.; Sheiham, A.; Nahas Pires Correa, M.S.; Haddad, A.E.; Bonecker, M. Risk indicators for erosive tooth wear in Brazilian preschool children. Caries Res. 2011, 45, 121–129. [Google Scholar] [CrossRef] [PubMed]
- Murakami, C.; Tello, G.; Abanto, J.; Oliveira, L.B.; Bonini, G.C.; Bonecker, M. Trends in the prevalence of erosive tooth wear in Brazilian preschool children. Int. J. Paediatr. Dent. 2016, 26, 60–65. [Google Scholar] [CrossRef]
- Nakane, A.; Sasaki, Y.; Miwa, Z.; Kitasako, Y.; Tagami, J. Prevalence of dental erosion and related factors in the deciduous dentition of Japanese children. Pediatr. Dent. J. 2014, 24, 97–105. [Google Scholar] [CrossRef]
- Raza, M.; Hashim, R. Dental erosion in 5- and 6-year-old school children and associated factors: A pilot study. J. Int. Dent. Med. Res. 2012, 5, 36–40. [Google Scholar]
- Tao, D.Y.; Hao, G.; Lu, H.X.; Tian, Y.; Feng, X.P. Dental erosion among children aged 3–6 years and its associated indicators. J. Public Health Dent. 2015, 75, 291–297. [Google Scholar] [CrossRef]
- Tschammler, C.; Muller-Pflanz, C.; Attin, T.; Muller, J.; Wiegand, A. Prevalence and risk factors of erosive tooth wear in 3–6 year old German kindergarten children-A comparison between 2004/05 and 2014/15. J. Dent. 2016, 52, 45–49. [Google Scholar] [CrossRef]
- Corica, A.; Caprioglio, A. Meta-analysis of the prevalence of tooth wear in primary dentition. Eur. J. Paediatr. Dent. 2014, 15, 385–388. [Google Scholar]
- Salas, M.M.; Nascimento, G.G.; Huysmans, M.C.; Demarco, F.F. Estimated prevalence of erosive tooth wear in permanent teeth of children and adolescents: An epidemiological systematic review and meta-regression analysis. J. Dent. 2015, 43, 42–50. [Google Scholar] [CrossRef]
- Amaechi, B.T.; Higham, S.M.; Edgar, W.M. Factors influencing the development of dental erosion in vitro: Enamel type, temperature and exposure time. J. Oral Rehabil. 1999, 26, 624–630. [Google Scholar] [CrossRef]
- Dumith, S.C.; Gigante, D.P.; Domingues, M.R.; Hallal, P.C.; Menezes, A.M.; Kohl, H.W., 3rd. A longitudinal evaluation of physical activity in Brazilian adolescents: Tracking, change and predictors. Pediatr. Exerc. Sci. 2012, 24, 58–71. [Google Scholar] [CrossRef] [PubMed]
- Mulic, A.; Tveit, A.B.; Songe, D.; Sivertsen, H.; Skaare, A.B. Dental erosive wear and salivary flow rate in physically active young adults. BMC Oral Health 2012, 12, 8. [Google Scholar] [CrossRef] [PubMed]
- Amaechi, B.T.; Higham, S.M. Dental erosion: Possible approaches to prevention and control. J. Dent. 2005, 33, 243–252. [Google Scholar] [CrossRef] [PubMed]
- Kippe, K.O.; Lagestad, P.A. Kindergarten: Producer or Reducer of Inequality Regarding Physical Activity Levels of Preschool Children. Front. Public Health 2018, 6, 361. [Google Scholar] [CrossRef]
- Kreulen, C.M.; Van’t Spijker, A.; Rodriguez, J.M.; Bronkhorst, E.M.; Creugers, N.H.; Bartlett, D.W. Systematic review of the prevalence of tooth wear in children and adolescents. Caries Res. 2010, 44, 151–159. [Google Scholar] [CrossRef]
- Harris, R.; Gamboa, A.; Dailey, Y.; Ashcroft, A. One-to-one dietary interventions undertaken in a dental setting to change dietary behaviour. Cochrane Database Syst. Rev. 2012, 2012, Cd006540. [Google Scholar] [CrossRef]
- Nunn, J.H.; Ng, S.K.; Sharkey, I.; Coulthard, M. The dental implications of chronic use of acidic medicines in medically compromised children. Pharm. World Sci. 2001, 23, 118–119. [Google Scholar] [CrossRef]
- Zhao, D.; Tsoi, J.K.; Wong, H.M.; Chu, C.H.; Matinlinna, J.P. Paediatric Over-the-Counter (OTC) Oral Liquids Can Soften and Erode Enamel. Dent. J. 2017, 5, 17. [Google Scholar] [CrossRef]
- Scatena, C.; Galafassi, D.; Gomes-Silva, J.M.; Borsatto, M.C.; Serra, M.C. In vitro erosive effect of pediatric medicines on deciduous tooth enamel. Braz. Dent. J. 2014, 25, 22–27. [Google Scholar] [CrossRef]
- Grande, F.; Catapano, S. Developmental dental defects and tooth wear: Pathological processes relationship. In Human Teeth–Structure and Composition of Dental Hard Tissues and Developmental Dental Defects; IntechOpen: London, UK, 2021. [Google Scholar]



{kind=link}
{kind=link}
| No. | Author (Published Year, Country Where Study Was Conducted) | Study Design | Number of Subjects (% Males) | Age Range (Year) | Recruitment | Inclusion (I)/ Exclusion (E) Criteria | Factors Evaluated | Erosion Index Used |
|---|---|---|---|---|---|---|---|---|
| 1 | Al-Ashtal (2017, YE) | Cross-Sectional | 206 (NR) | 5–6 | University Dental Clinic | NR | nil | EPRS |
| 2 | Al-Dlaigan (2017, SB) | Cross-Sectional | 388 (47) | 3–5 | Kindergartens (2 public, 8 private) | NR | Diet | TWI |
| 3 | Al-Majed (2002, SB) | Cross-Sectional | 354 (100) | 5–6 | Elementary Schools | (E) Children without questionnaires (E) Children who were not examined | Diet OH | TWI |
| 4 | Al-Malik (2000, SB) | Cross-Sectional | 80 (64) | 4–5 | Home for Disadvantaged | (E) Children with significant medical history/learning difficulties (none) | Caries | TWI |
| 5 | Al-Malik (2001, SB) | Cross-Sectional | 987 (NR) | 2–5 | Schools (6 public, 11 private) | (E) Children without consent forms (E) Absent for examination (E) Uncooperative for examination | Diet OH Social Class | TWI |
| 6 | Duangthip (2019, HK) | Cross-Sectional | 1204 (46) | 3–5 | 7 non-profit kindergartens | (I) Healthy children (E) Children with chronic diseases (E) Children with special needs (E) Below 3 years old (E) Uncooperative for examination (E) Absent for examination | Gender Age SES Parental education level Diet OH Caries | BEWE |
| 7 | Gatt (2019, MT) | Cross-Sectional | 775 | 3–5 | Schools (state, church, independent) | (I) Resident on Islands all their lives 3–5 years old (E) Children with enamel defects exhibiting loss of tooth tissue | Gender Age SES Parental education level Diet OH Caries Asthma/respiratory disease GERD Medications BMI | BEWE |
| 8 | Gopinath (2016, AE) | Cross-Sectional | 403 (48.14) | 5 | Kindergartens | NR | Gender Diet Caries Nationality | TWI |
| 9 | Habib (2013, US) | Cross-Sectional | 164 | 2–4 | Daycare centre Preschool Grade school | (I) Consent given (I) Resident of Kansas City Metropolitan area | Gender EthnicitySES OH Diet | TWI |
| 10 | Harding (2003, IE) | Cross-Sectional | 202 | 5 | Schools | (E) Medical condition (E) Children on long term oral or inhaled corticosteroids | Gender SES Diet OH Fluoridation Vomiting | TWI |
| 11 | Huang (2015, AU) | Cohort | 154 (45) | 2–4 | Public birthing and community health clinics | (E) Those who did not attend all 3 reviews | Social Medical history Dental and dietary habits GERD | TWI |
| 12 | Luo (2005, CN) | Cross-Sectional | 1949 | 3–5 | Kindergartens | (I) No gastrointestinal problems | SES Parental Education Diet | TWI |
| 13 | Maharani (2019, ID) | Cross-Sectional | 691 (53.54) | 5 | Kindergartens | (E) Uncooperative for examination (E) No questionnaire (E) No consent | Gender SES Parental education SES Diet OH Digestive disorders | BEWE |
| 14 | Mantonanaki (2013, GR) | Cross-Sectional | 524 (examination and questionnaire done)605 (examination only) | 5 | Kindergartens | (E) No examination (E) Incomplete questionnaire (E) Immigrants (E) Above 5 years old | Parental education level SES OH Vomiting/regurgitation/heartburn Medication | BEWE |
| 15 | Moimaz (2013, BR) | Cross-Sectional | 1993 (49.42) | 4–6 | Preschools (public) | (E) No consent (E) Uncooperative for examination (E) Absent for examination | Gender Age OH | TWI |
| 16 | Murakami (2011, BR) | Cross-Sectional | 967 (47.88) | 3–4 | Children attending a statutory National Children’s Vaccination day | (E) Children living in same household as selected child (E) Children without parents present | Age Caries SES Diet Acid reflux | TWI |
| 17 | Murakami (2016, BR) (some repeat data from 2011, repeat data excluded in statistical analysis) | Cross-Sectional | 2801 | 3–4 | Children attending a statutory National Children’s Vaccination day in 2008, 2010, 2012 | (E) Children living in same household as selected child (E) Children without parents present | nil | TWI |
| 18 | Nakane (2014, JP) | Cross-Sectional | 116 (57.76) | 2–6 | University Hospital Paediatric Dental Clinic | NR | SES Diet Vomiting Medication OH Fluoride Medical history | O’Sullivan Index |
| 19 | Nayak (2012, IN) | Cross-Sectional | 1002 | 5 | Schools | (E) Special health care needs(E) Orofacial defects | Diet OH | SES Diet |
| 20 | Raza & Hashim (2012, AE) | Cross-Sectional | 207 (46.4) | 5–6 | Schools (private) | (I) Children who completed examination and questionnaire | Age Ethnicity Mother education level Diet Medications GERD Swimming | TWI |
| 21 | Tao (2015, CN) | Cross-Sectional | 1837 (51.55) | 3–6 | Kindergartens | (E) Children with orthodontics appliances | Age Gender Parental education Diet OH Medical health SES Swimming | O’Sullivan Index |
| 22 | Tschammler (2016, DE) | Cross-Sectional | 775 (52.26) | 3–6 | Kindergartens | (E) No consent Uncooperative during examination | Diet Chronic illness OH | BEWE |
| No. | Author | Year | Qs 1 | Qs 2 | Qs 3 | Qs 4 | Qs 5 | Qs 6 | Qs 7 | Qs 8 | Qs 9 | Total Score | Risk of Bias |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | Al-Ashtal et al. | 2017 | 2 | 1 | 1 | 2 | 3 | 1 | 1 | 1 | 3 | 5 out of 9 | Moderate |
| 2 | Al-Dlaigan et al. | 2017 | 1 | 1 | 1 | 2 | 2 | 1 | 1 | 1 | 3 | 6 out of 9 | Moderate |
| 3 | Al-Majed et al. | 2002 | 1 | 3 | 1 | 2 | 1 | 1 | 1 | 1 | 1 | 7 out of 9 | Low |
| 4 | Al-Malik et al. | 2000 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 0 | 9 out of 9 | Low |
| 5 | Al-Malik et al. | 2001 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 3 | 8 out of 9 | Low |
| 6 | Duangthip et al. | 2019 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 9 out of 9 | Low |
| 7 | Gatt et al. | 2019 | 1 | 1 | 1 | 2 | 1 | 1 | 1 | 1 | 2 | 7 out of 9 | Low |
| 8 | Gopinath et al. | 2016 | 1 | 2 | 3 | 2 | 1 | 1 | 1 | 1 | 1 | 6 out of 9 | Moderate |
| 9 | Habib et al. | 2013 | 1 | 1 | 1 | 1 | 3 | 1 | 1 | 1 | 3 | 7 out of 9 | Low |
| 10 | Harding et al. | 2003 | 1 | 3 | 3 | 1 | 1 | 1 | 1 | 1 | 3 | 6 out of 9 | Moderate |
| 11 | Huang et al. | 2015 | 1 | 1 | 3 | 2 | 3 | 1 | 1 | 1 | 3 | 5 out of 9 | Moderate |
| 12 | Luo et al. | 2005 | 1 | 1 | 3 | 1 | 3 | 1 | 1 | 1 | 3 | 6 out of 9 | Moderate |
| 13 | Maharani et al. | 2019 | 1 | 1 | 1 | 1 | 3 | 1 | 1 | 1 | 1 | 8 out of 9 | Low |
| 14 | Mantonanaki et al. | 2013 | 1 | 1 | 1 | 1 | 3 | 1 | 1 | 1 | 3 | 7 out of 9 | Low |
| 15 | Moimaz et al. | 2013 | 1 | 3 | 3 | 2 | 2 | 1 | 1 | 1 | 3 | 4 out of 9 | High |
| 16 | Murakami et al. | 2011 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 9 out of 9 | Low |
| 17 | Murakami et al. | 2016 | 1 | 1 | 1 | 2 | 3 | 1 | 1 | 1 | 1 | 7 out of 9 | Low |
| 18 | Nakane et al. | 2014 | 2 | 1 | 3 | 1 | 3 | 1 | 1 | 1 | 3 | 5 out of 9 | Moderate |
| 19 | Nayak et al. | 2012 | 1 | 1 | 1 | 1 | 3 | 1 | 1 | 1 | 1 | 8 out of 9 | Low |
| 20 | Raza & Hashim | 2012 | 1 | 1 | 3 | 1 | 3 | 1 | 3 | 1 | 3 | 5 out of 9 | Moderate |
| 21 | Tao et al. | 2015 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 3 | 8 out of 9 | Low |
| 22 | Tschammler et al. | 2016 | 1 | 1 | 1 | 2 | 1 | 1 | 1 | 1 | 1 | 8 out of 9 | Low |
| Outcome | No. of Studies | No. of Participants | Results | Risk of Bias † | Inconsistency ‡ | Indirectness § | Imprecision ¶ | Publication Bias †† | Quality of Evidence (GRADE) | |
|---|---|---|---|---|---|---|---|---|---|---|
| I2 Statistics | Heterogenicity χ2 Test (p Value) | |||||||||
| Dental Erosion Prevalence | 22 | 17,300 | Estimated overall prevalence: 38.38% p < 0.001 | Not serious | 99.9% * | p < 0.001 *** | Not serious | Not serious | Not serious | ⊕OOO very low due to observational data, substantial inconsistency |
| – | ↓ | – | – | – | ||||||
| Gender | 8 | 1106 | Likelihood of boys have dental erosion is significantly higher than girls (p < 0.001) | Not serious | 0.0% | p = 0.492 | Not serious | Not serious | N/A | ⊕⊕OO low due to observational data |
| – | – | – | – | |||||||
| GERD | 4 | 227 | Likelihood of children with GERD/frequent vomiting/digestive disorders having dental erosion is higher than children without the above disorders (p = 0.002) | Not serious | 0.0% | p = 0.413 | Not serious | Not serious | N/A | ⊕⊕OO low due to observational data |
| – | – | – | – | |||||||
| Birthplace | 3 | 243 | No significant difference | Not serious | 94.2% * | p < 0.001 *** | Not serious | Not serious | N/A | ⊕OOO very low due to observational data, substantial inconsistency |
| – | ↓ | – | – | |||||||
| Dmft > 0 /Caries Experience | 3 | 346 | No significant difference | Not serious | I2 = 82.2% * | p = 0.004 ** | Not serious | Not serious | N/A | ⊕OOO very low due to observational data, substantial inconsistency |
| – | ↓ | – | – | |||||||
| Parental Education (primary) | 3 | 114 | No significant difference | Not serious | I2 = 82.5% * | p = 0.003 ** | Not serious | Not serious | N/A | ⊕OOO very low due to observational data, substantial inconsistency |
| – | ↓ | – | – | |||||||
| Parental Education (Secondary) | 3 | 442 | No significant difference | Not serious | I2 = 91.9% * | p < 0.001 *** | Not serious | Not serious | N/A | ⊕OOO very low due to observational data, substantial inconsistency |
| – | ↓ | – | – | |||||||
| Toothbrushing | 3 | 231 | No significant difference | Not serious | I2 = 0.0% | p = 0.457 | Not serious | No serious | N/A | ⊕⊕OO low due to observational data |
| – | – | – | – | |||||||
| – | – | – | – | |||||||
| Variables | N (Studies) | Prevalence (%) | Meta-Regression |
|---|---|---|---|
| Age | |||
| 3 | 6 | 34.4 | 0.900 |
| 4 | 8 | 30.4 | 0.859 |
| 5 | 12 | 38.9 | 0.635 |
| 6 | 4 | 32.7 | Reference |
| Indices | |||
| BEWE | 5 | 46.81 | 0.197 |
| TWI | 14 | 37.87 | 0.289 |
| O’Sullivan | 2 | 50.58 | 0.208 |
| EPRS | 1 | 6.80 | Reference |
| Sample Size | |||
| 1–499 | 10 | 45.22 | 0.106 |
| 500–999 | 5 | 52.34 | 0.074 |
| 1000–1499 | 3 | 28.12 | 0.640 |
| 1500+ | 4 | 18.48 | Reference |
| Human Development Index (HDI) | |||
| Below 0.55 | 1 | 6.8 | 0.151 |
| 0.55–0.69 | 5 | 46.50 | 0.899 |
| 0.7–0.79 | 6 | 24.78 | 0.101 |
| 0.8–1.0 | 10 | 48.43 | Reference |
| Year of Recruitment | |||
| Before 2010 | 7 | 40.88 | 0.748 |
| 2010–2014 | 8 | 43.66 | 0.601 |
| 2015 and later | 8 | 36.12 | Reference |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yip, K.; Lam, P.P.Y.; Yiu, C.K.Y. Prevalence and Associated Factors of Erosive Tooth Wear among Preschool Children—A Systematic Review and Meta-Analysis. Healthcare 2022, 10, 491. https://doi.org/10.3390/healthcare10030491
Yip K, Lam PPY, Yiu CKY. Prevalence and Associated Factors of Erosive Tooth Wear among Preschool Children—A Systematic Review and Meta-Analysis. Healthcare. 2022; 10(3):491. https://doi.org/10.3390/healthcare10030491
Chicago/Turabian StyleYip, Kimberley, Phoebe Pui Ying Lam, and Cynthia Kar Yung Yiu. 2022. "Prevalence and Associated Factors of Erosive Tooth Wear among Preschool Children—A Systematic Review and Meta-Analysis" Healthcare 10, no. 3: 491. https://doi.org/10.3390/healthcare10030491
APA StyleYip, K., Lam, P. P. Y., & Yiu, C. K. Y. (2022). Prevalence and Associated Factors of Erosive Tooth Wear among Preschool Children—A Systematic Review and Meta-Analysis. Healthcare, 10(3), 491. https://doi.org/10.3390/healthcare10030491