
The Impact of Using mHealth Apps on Improving Public Health Satisfaction during the COVID-19 Pandemic: A Digital Content Value Chain Perspective




Abstract
:1. Introduction
2. Theoretical Background and Hypothesis Development
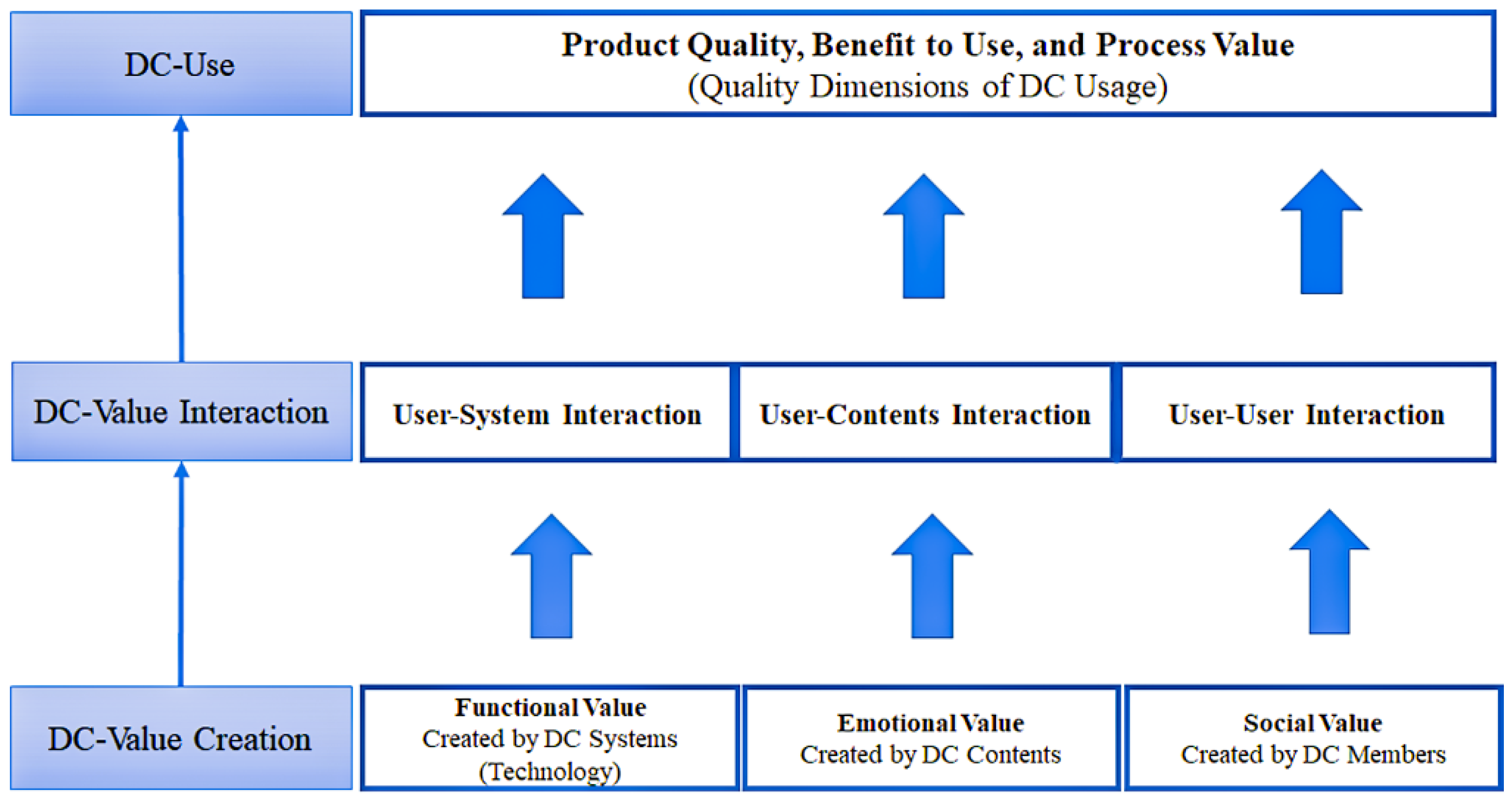
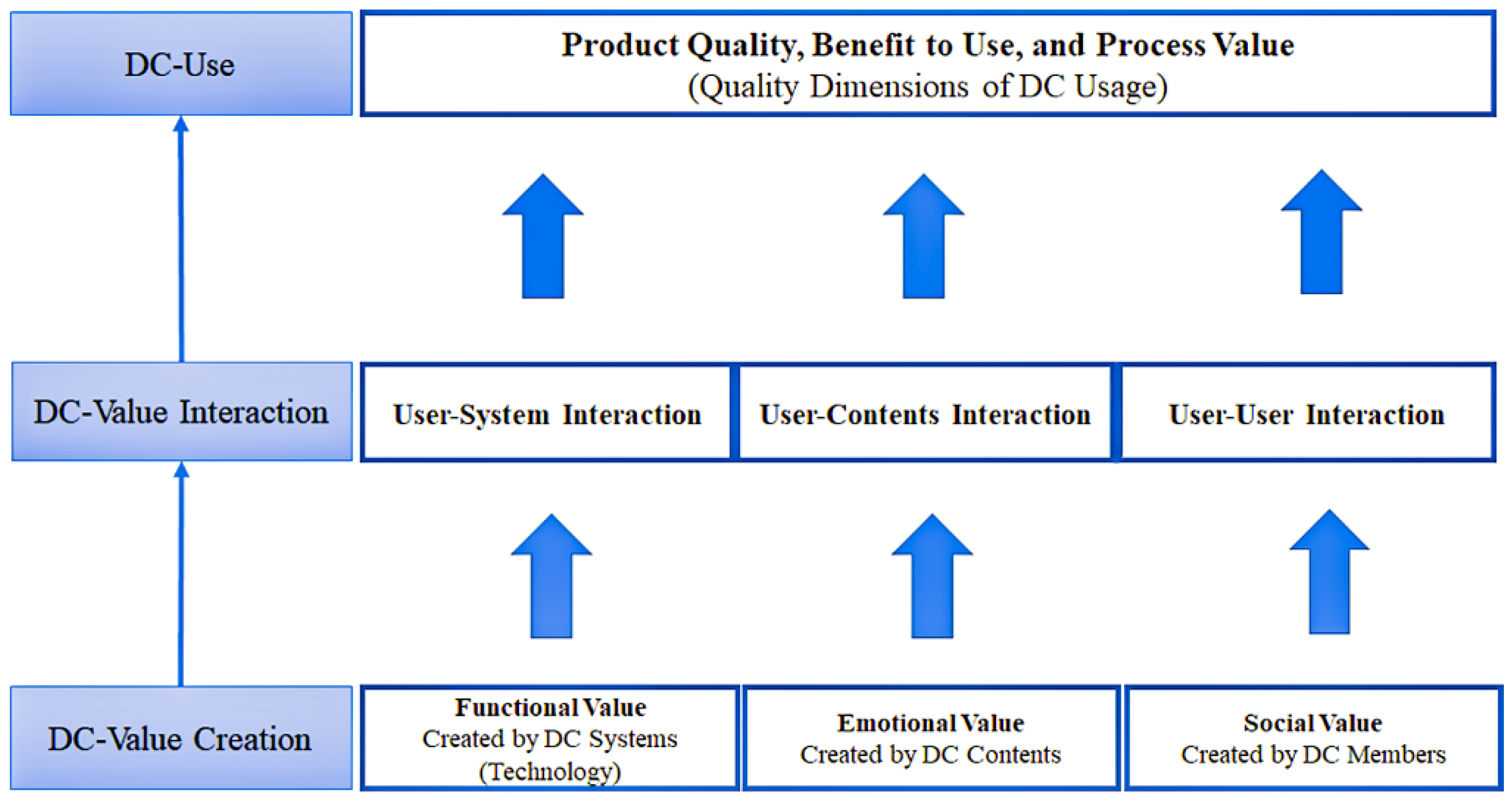
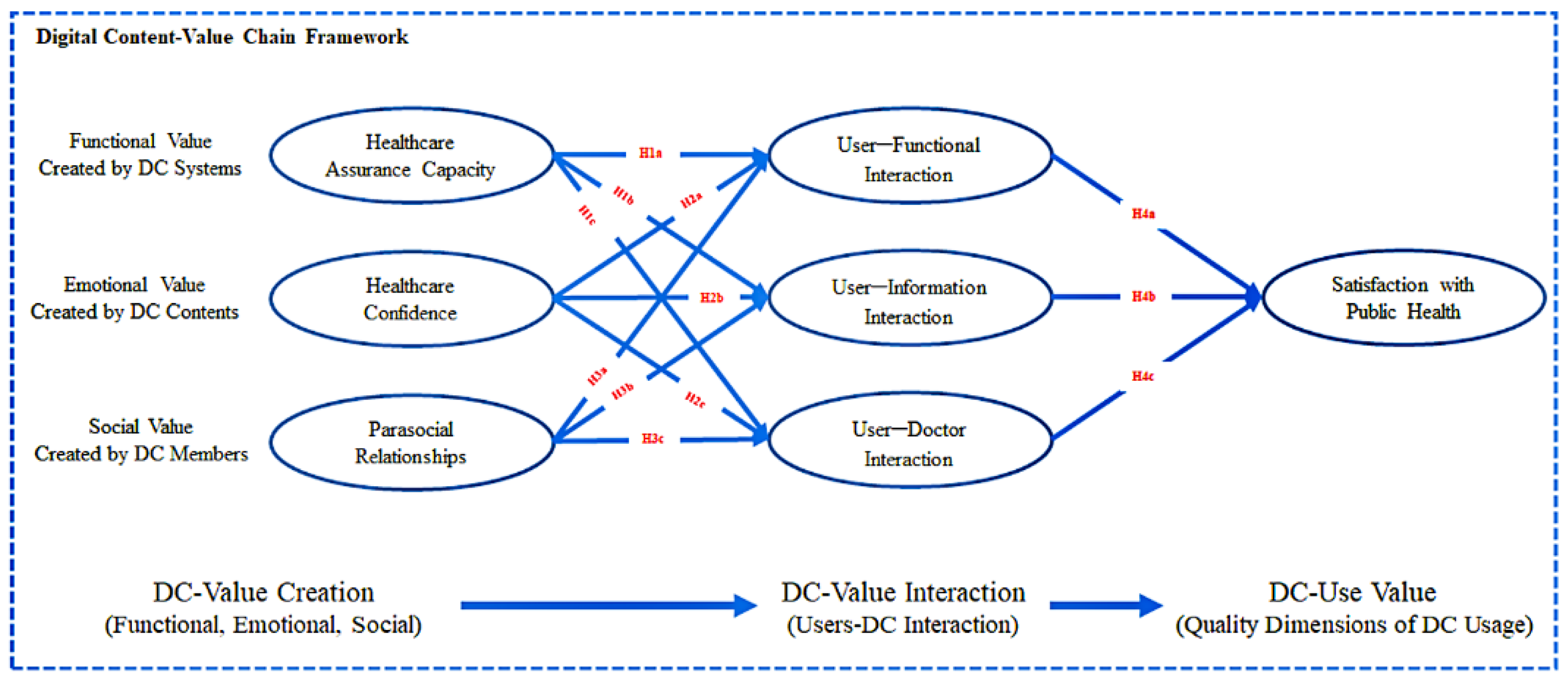
2.1. Digital Content Value Chain Framework
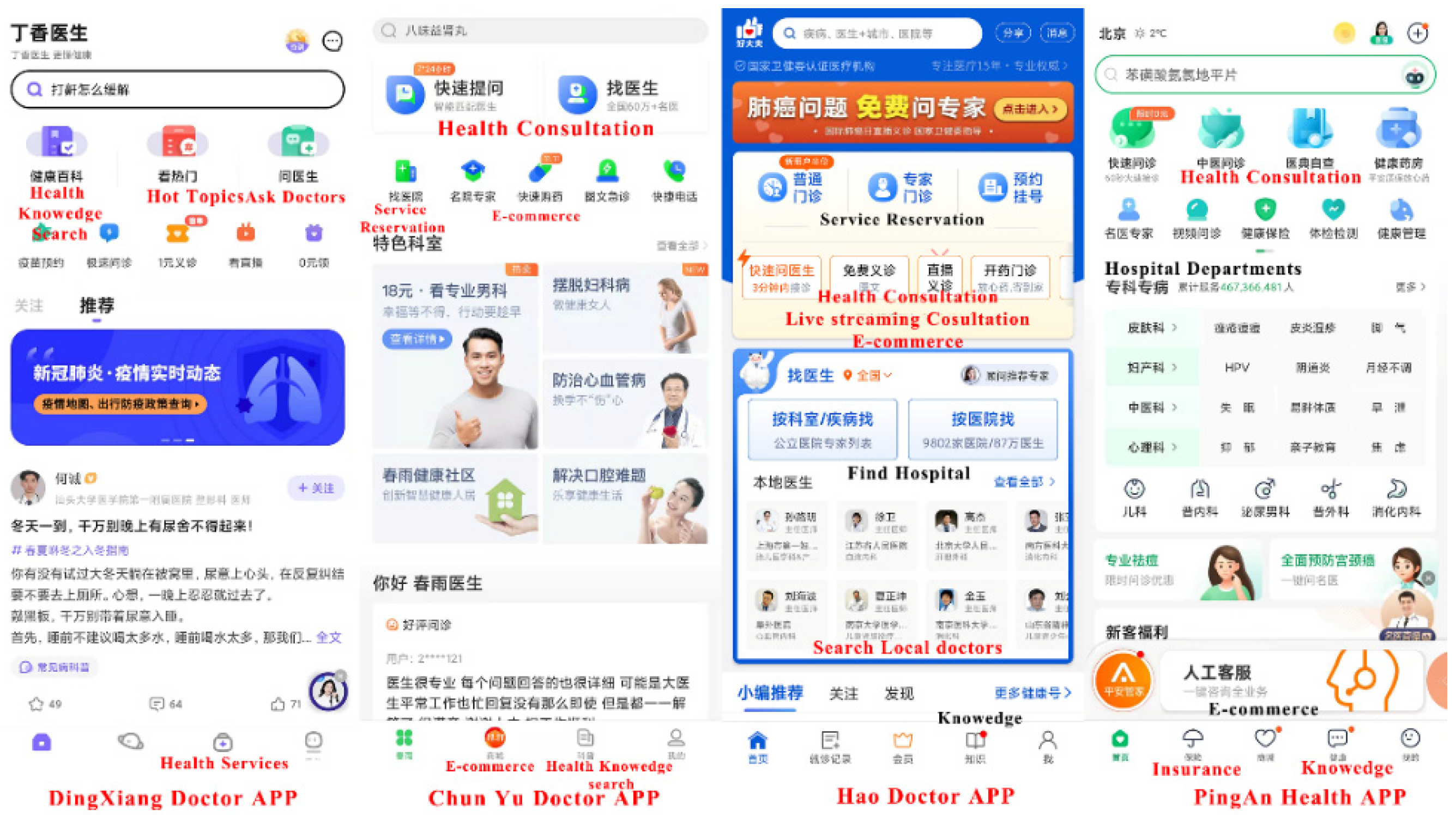
2.2. Main Values of mHealth App during the COVID-19 Pandemic
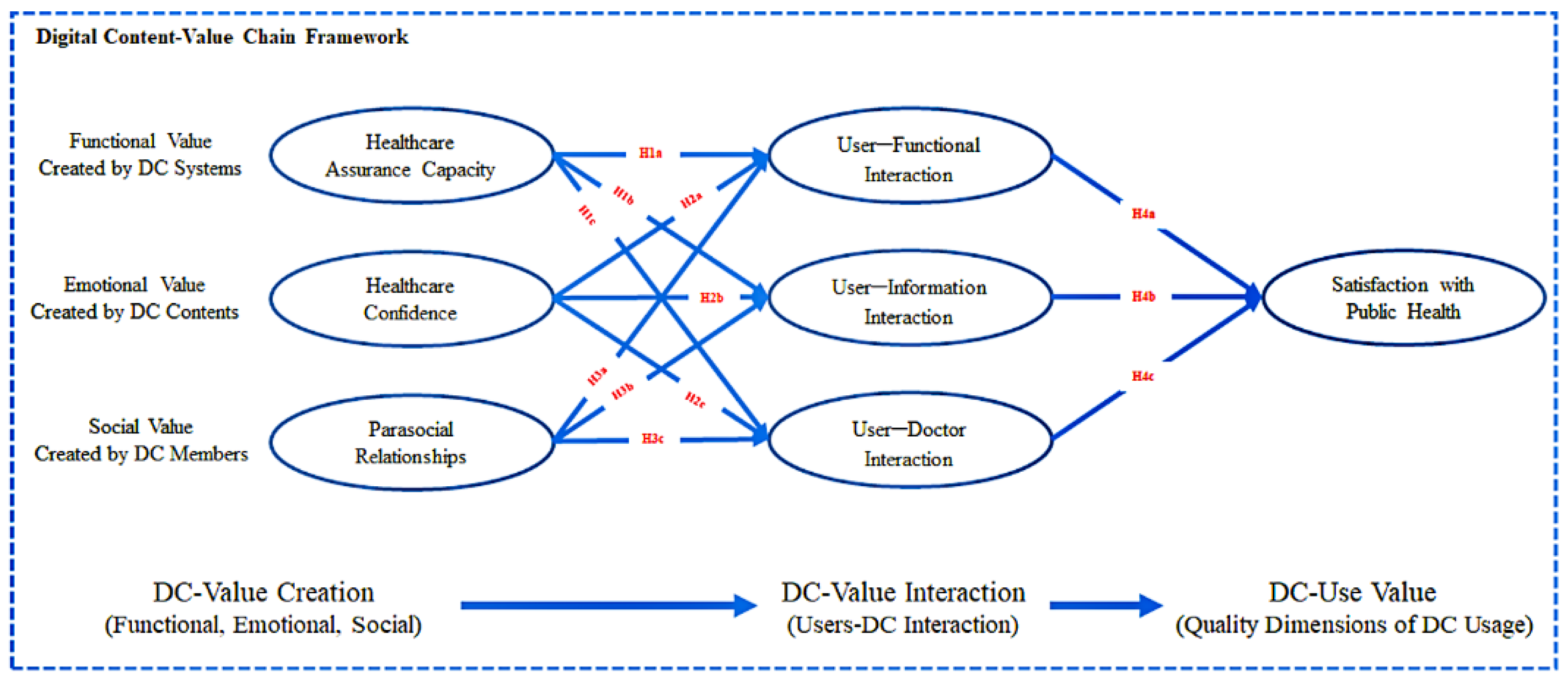
3. Research Model and Questionnaire Survey
3.1. Digital Content-Value Chain Framework
3.2. Questionnaire Survey
4. Methods
5. Results
5.1. Pretest Results
5.2. Common Method Bias Test Results
5.3. Measurement Model Results
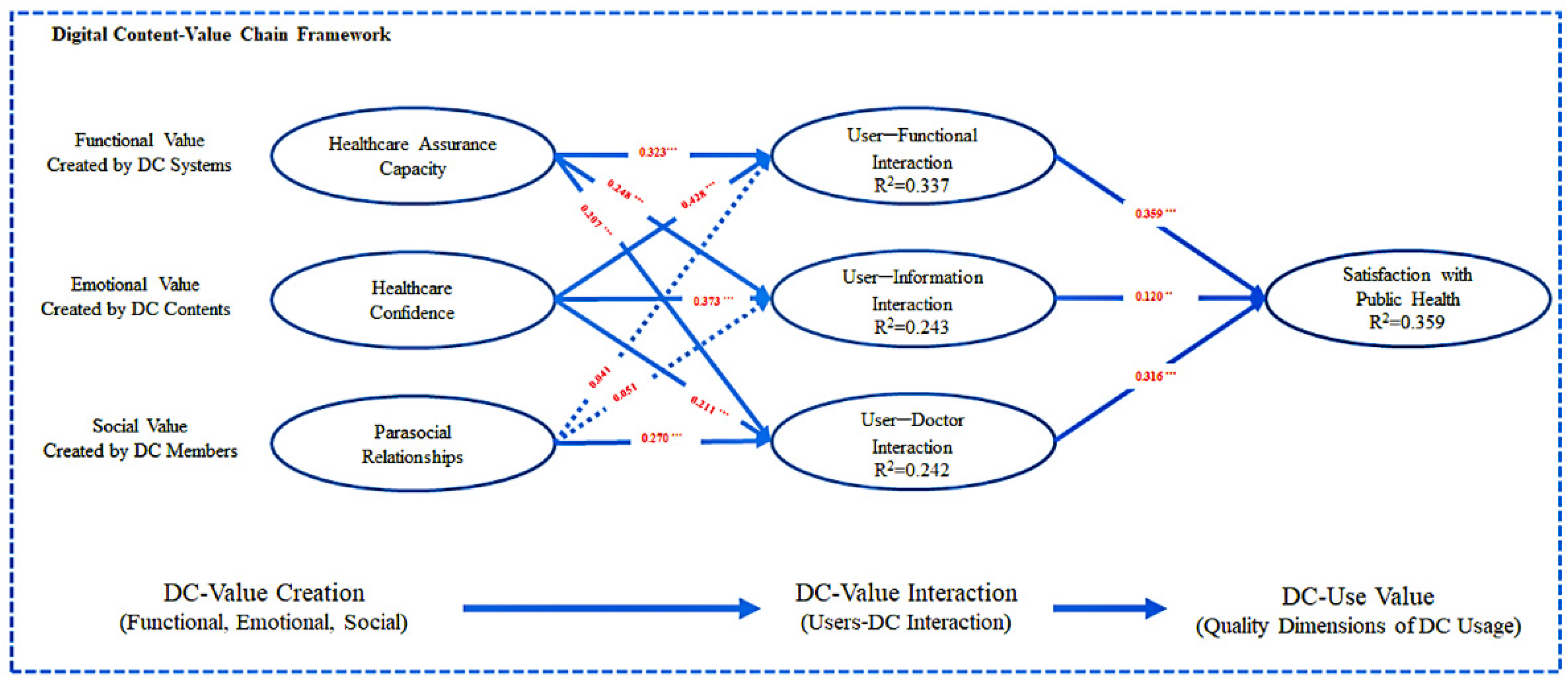
5.4. Structural Model Results
5.5. Mediation Effect Results
6. Discussion and Implications
6.1. Discussion of Key Findings
6.2. Theoretical Contribution
6.3. Practical Contribution
6.4. Limitations and Future Research
Author Contributions
Funding
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A
| Factor | Serial Num. | Item | Reference |
| Healthcare assurance capacity (HAC) | HAC1 | During the COVID-19 pandemic, the health management function in the mhealth app encouraged me. | Akter et al. [61] |
| HAC 2 | During the COVID-19 pandemic, because of the health management function in the mhealth app, I feel safe. | ||
| HAC 3 | During the COVID-19 pandemic, the health management function in the mhealth app can solve my health problems. | ||
| Healthcare confidence (ACO) | ACO1 | During the COVID-19 pandemic, the information provided by mhealth apps allows me to know enough about my health. | Benson et al. [67] |
| ACO2 | During the COVID-19 pandemic, the information provided by mhealth apps makes me feel that I can take care of my health. | ||
| ACO3 | During the COVID-19 pandemic, the information provided by mhealth apps helped me when I needed it. | ||
| ACO4 | During the COVID-19 pandemic, the information provided by mhealth apps helped me make decisions about health management. | ||
| Parasocial relationships (PSR) | PSR1 | When I use mhealth app during the COVID-19 pandemic, the doctor I chose to make me feel like a friend. | Sokolova and Perez [68] |
| PSR2 | When I use mhealth apps during the COVID-19 pandemic, my communication with the doctor is very comfortable. | Zafar et al. [69] | |
| PSR3 | When I use mhealth apps during the COVID-19 pandemic, I can rely on the doctor to provide me with a diagnosis. | ||
| PSR4 | When I use mhealth apps during the COVID-19 pandemic, there was a small error in the doctor’s diagnosis immediately, and I will forgive him. | ||
| User–function interaction (UFI) | UFI1 | The health management function in mhealth apps is safe and reliable. | Kim and Kim [22] |
| UFI2 | The health management function in mhealth apps is easy to use. | ||
| UFI3 | The steps of using health management in mhealth apps are easy to learn. | ||
| UFI4 | The health management function in mhealth apps meets individual needs. | ||
| User–information interaction (UII) | UII1 | The information and user interaction in mhealth apps are accurate. | Kim and Kim [22] |
| UII2 | Information and user interaction in mhealth apps are useful. | ||
| UII3 | The interaction between the information and the user in mhealth apps is effective. | ||
| UII4 | The information in mhealth apps can interact with the user quickly. | ||
| User–doctor interaction (UDI) | UDI1 | Mhealth apps improve the interaction between users and doctors. | Kim and Kim [22] |
| UDI2 | Mhealth apps improve communication between users and doctors. | ||
| UDI3 | Mhealth apps allow users and doctors to interact with various types of information. | ||
| UDI4 | Mhealth apps simplify the exchange of information between users and doctors. | ||
| Satisfaction with public health (SPH) | SPH1 | During the COVID-19 pandemic, the public medical resources available to me satisfy me. | Akter, Ambra and Ray [70] |
| SPH2 | During the COVID-19 pandemic, I can conveniently use public medical resources. | ||
| SPH3 | During the COVID-19 pandemic, I am very happy that I can use public medical resources. | ||
| SPH4 | During the COVID-19 pandemic, I can use public medical resources at any time. |
References
- Canty, J. Social work and public health—Logical collaborators. Aotearoa N. Z. Soc. Work 2021, 33, 94–98. [Google Scholar] [CrossRef]
- Wu, J.; Xie, X.; Yang, L.; Xu, X.; Cai, Y.; Wang, T.; Xie, X. Mobile health technology combats COVID-19 in China. J. Infect. 2020, 82, 159–198. [Google Scholar] [CrossRef] [PubMed]
- Kondylakis, H.; Katehakis, D.G.; Kouroubali, A.; Logothetidis, F.; Triantafyllidis, A.; Kalamaras, I.; Votis, K.; Tzovaras, D. COVID-19 Mobile Apps: A Systematic Review of the Literature. J. Med. Internet Res. 2020, 22, e23170. [Google Scholar] [CrossRef] [PubMed]
- Hilty, D.; Chan, S.; Torous, J.; Luo, J.; Boland, R. A Framework for Competencies for the Use of Mobile Technologies in Psychiatry and Medicine: Scoping Review. JMIR mHealth uHealth 2020, 8, e12229. [Google Scholar] [CrossRef] [PubMed]
- Tabi, K.; Randhawa, A.S.; Choi, F.; Mithani, Z.; Albers, F.; Schnieder, M.; Nikoo, M.; Vigo, D.; Jang, K.; Demlova, R.; et al. Mobile Apps for Medication Management: Review and Analysis. JMIR mHealth uHealth 2019, 7, e13608. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- WHO. mHealth: New Horizons for Health Through Mobile Technologies: Second Global Survey on eHealth; World Health Organization: Geneva, Switzerland, 2011. [Google Scholar]
- Scott, A.R.; Alore, E.A.; Naik, A.D.; Berger, D.H.; Suliburk, J.W. Mixed-Methods Analysis of Factors Impacting Use of a Postoperative mHealth App. JMIR mHealth uHealth 2017, 5, e11. [Google Scholar] [CrossRef]
- Powell, A.C.; Torous, J.; Chan, S.; Raynor, G.S.; Shwarts, E.; Shanahan, M.; Landman, A.B. Interrater Reliability of mHealth App Rating Measures: Analysis of Top Depression and Smoking Cessation Apps. JMIR mHealth uHealth 2016, 4, e15. [Google Scholar] [CrossRef]
- Zhou, L.; Bao, J.; Setiawan, I.M.A.; Saptono, A.; Parmanto, B. The mHealth App Usability Questionnaire (MAUQ): Development and Validation Study. JMIR mHealth uHealth 2019, 7, e11500. [Google Scholar] [CrossRef]
- Palmer, S. Swipe Right for Health Care: How the State May Decide the Future of the mHealth App Industry in the Wake of FDA Uncertainty. J. Legal Med. 2017, 37, 249–263. [Google Scholar] [CrossRef]
- Roth, V.J. The mHealth Conundrum: Smartphones & Mobile medical apps-How much FDA medical device regulation is required. North Carol. J. Law Technol. 2013, 15, 359. [Google Scholar]
- Ming, L.C.; Untong, N.; Aliudin, N.A.; Osili, N.; Kifli, N.; Tan, C.S.; Goh, K.W.; Ng, P.W.; Al-Worafi, Y.M.; Lee, K.S.; et al. Mobile Health Apps on COVID-19 Launched in the Early Days of the Pandemic: Content Analysis and Review. JMIR mHealth uHealth 2020, 8, e19796. [Google Scholar] [CrossRef] [PubMed]
- Akbar, S.; Coiera, E.; Magrabi, F. Safety concerns with consumer-facing mobile health applications and their consequences: A scoping review. J. Am. Med. Inform. Assoc. 2019, 27, 330–340. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Apidi, N.A.; Murugiah, M.K.; Muthuveloo, R.; Soh, Y.C.; Caruso, V.; Patel, R.; Ming, L.C. Mobile Medical Applications for Dosage Recommendation, Drug Adverse Reaction, and Drug Interaction: Review and Comparison. Ther. Innov. Regul. Sci. 2017, 51, 480–485. [Google Scholar] [CrossRef] [PubMed]
- Izahar, S.; Lean, Q.Y.; Hameed, M.A.; Murugiah, M.K.; Patel, R.P.; Al-Worafi, Y.M.; Wong, T.W.; Ming, L.C. Content Analysis of Mobile Health Applications on Diabetes Mellitus. Front. Endocrinol. 2017, 8, 318. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Timmers, T.; Janssen, L.; Stohr, J.; Murk, J.L.; Berrevoets, M.A.H. Using eHealth to Support COVID-19 Education, Self-Assessment, and Symptom Monitoring in the Netherlands: Observational Study. JMIR mHealth uHealth 2020, 8, e19822. [Google Scholar] [CrossRef]
- Ros, M.; Neuwirth, L.S. Increasing global awareness of timely COVID-19 healthcare guidelines through FPV training tutorials: Portable public health crises teaching method. Nurse Educ. Today 2020, 91, 104479. [Google Scholar] [CrossRef]
- Yamamoto, K.; Takahashi, T.; Urasaki, M.; Nagayasu, Y.; Shimamoto, T.; Tateyama, Y.; Matsuzaki, K.; Kobayashi, D.; Kubo, S.; Mito, S.; et al. Health Observation App for COVID-19 Symptom Tracking Integrated With Personal Health Records: Proof of Concept and Practical Use Study. JMIR mHealth uHealth 2020, 8, e19902. [Google Scholar] [CrossRef]
- Hense, S.; Kodali, P.; Kopparty, S.; Kalapala, G.; Haloi, B. How Indians responded to the Arogya Setu app? Indian J. Public Health 2020, 64, 228. [Google Scholar] [CrossRef]
- Zamberg, I.; Manzano, S.; Posfay-Barbe, K.; Windisch, O.; Agoritsas, T.; Schiffer, E. A Mobile Health Platform to Disseminate Validated Institutional Measurements During the COVID-19 Outbreak: Utilization-Focused Evaluation Study. JMIR Public Health Surveill. 2020, 6, e18668. [Google Scholar] [CrossRef]
- Ben Hassen, H.; Ayari, N.; Hamdi, B. A home hospitalization system based on the Internet of things, Fog computing and cloud computing. Inform. Med. Unlocked 2020, 20, 100368. [Google Scholar] [CrossRef]
- Kim, C.; Kim, D.J. Uncovering the value stream of digital content business from users’ viewpoint. Int. J. Inf. Manag. 2017, 37, 553–565. [Google Scholar] [CrossRef]
- Ben-Zeev, O. Mobile Health for All: Public-Private Partnerships Can Create a New Mental Health Landscape. JMIR Ment. Health 2016, 3, e26. [Google Scholar] [CrossRef] [PubMed]
- DeMuro, P.; Petersen, C. Legal and Regulatory Considerations Associated with Use of Patient-Generated Health Data from Social Media and Mobile Health (mHealth) Devices. Appl. Clin. Inform. 2015, 6, 16–26. [Google Scholar] [CrossRef] [PubMed]
- Similä, H.; Immonen, M.; Toska-Tervola, J.; Enwald, H.; Keränen, N.; Kangas, M.; Jämsä, T.; Korpelainen, R. Feasibility of mobile mental wellness training for older adults. Geriatr. Nurs. 2018, 39, 499–505. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mushquash, A.R.; Pearson, E.S.; Waddington, K.; MacIsaac, A.; Mohammed, S.; Grassia, E.; Smith, S.; Wekerle, C. User perspectives on the resilience-building JoyPop app: Qualitative study. JMIR mHealth uHealth 2021, 9, e28677. [Google Scholar] [CrossRef]
- Cao, J.; Lim, Y.; Sengoku, S.; Guo, X.; Kodama, K. Exploring the Shift in International Trends in Mobile Health Research From 2000 to 2020: Bibliometric Analysis. JMIR mHealth uHealth 2021, 9, e31097. [Google Scholar] [CrossRef]
- Sun, J.; Guo, Y.; Wang, X.; Zeng, Q. mHealth For Aging China: Opportunities and Challenges. Aging Dis. 2016, 7, 53–67. [Google Scholar] [CrossRef] [Green Version]
- Williams, K.; Chatterjee, S.; Rossi, M. Design of emerging digital services: A taxonomy. Eur. J. Inf. Syst. 2008, 17, 505–517. [Google Scholar] [CrossRef]
- Shi, Z.; Rui, H.; Whinston, A.B. Content Sharing in a Social Broadcasting Environment: Evidence from Twitter. MIS Q. 2014, 38, 123–142. [Google Scholar] [CrossRef] [Green Version]
- Springer, A.; Venkatakrishnan, A.; Mohan, S.; Nelson, L.; Silva, M.; Pirolli, P.; Acosta, M.; Bardus, M.; Bartlett, Y.; Nelson, L. Leveraging Self-Affirmation to Improve Behavior Change: A Mobile Health App Experiment. JMIR mHealth uHealth 2018, 6, e157. [Google Scholar] [CrossRef]
- Chang, H.; Hou, Y.; Yeh, F.; Lee, S. The impact of an mHealth app on knowledge, skills and anxiety about dressing changes: A randomized controlled trial. J. Adv. Nurs. 2019, 76, 1046–1056. [Google Scholar] [CrossRef] [PubMed]
- Wind, T.R.; Rijkeboer, M.; Andersson, G.; Riper, H. The COVID-19 pandemic: The ‘black swan’ for mental health care and a turning point for e-health. Internet Interv. 2020, 20, 100317. [Google Scholar] [CrossRef] [PubMed]
- Rawaf, S.; Allen, L.N.; Stigler, F.L.; Kringos, D.; Yamamoto, H.Q.; van Weel, C.; on behalf of the Global Forum on Universal Health Coverage and Primary Health Care. Lessons on the COVID-19 pandemic, for and by primary care professionals worldwide. Eur. J. Gen. Pract. 2020, 26, 129–133. [Google Scholar] [CrossRef] [PubMed]
- Fontelo, P.; Rossi, E.; Ackerman, M.; Marceglia, S. A Standards-Based Architecture Proposal for Integrating Patient mHealth Apps to Electronic Health Record Systems. Appl. Clin. Inform. 2015, 06, 488–505. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Salehan, M.; Kim, D.; Kim, C. Use of Online Social Networking Services from a Theoretical Perspective of the Motivation-Participation-Performance Framework. J. Assoc. Inf. Syst. 2017, 18, 141–172. [Google Scholar] [CrossRef]
- Qin, H.; Peak, D.A.; Prybutok, V. A virtual market in your pocket: How does mobile augmented reality (MAR) influence consumer decision making? J. Retail. Consum. Serv. 2020, 58, 102337. [Google Scholar] [CrossRef]
- Akter, S.; D’Ambra, J.; Ray, P.; Hani, U. Modelling the impact of mHealth service quality on satisfaction, continuance and quality of life. Behav. Inf. Technol. 2013, 32, 1225–1241. [Google Scholar] [CrossRef]
- Akter, S.; D’Ambra, J.; Ray, P. Development and validation of an instrument to measure user perceived service quality of mHealth. Inf. Manag. 2013, 50, 181–195. [Google Scholar] [CrossRef] [Green Version]
- Dawson, D.L.; Golijani-Moghaddam, N. COVID-19: Psychological flexibility, coping, mental health, and wellbeing in the UK during the pandemic. J. Context. Behav. Sci. 2020, 17, 126–134. [Google Scholar] [CrossRef]
- Kopelovich, S.L.; Monroe-DeVita, M.; Buck, B.E.; Brenner, C.; Moser, L.; Jarskog, L.F.; Harker, S.; Chwastiak, L.A. Community Mental Health Care Delivery During the COVID-19 Pandemic: Practical Strategies for Improving Care for People with Serious Mental Illness. Community Ment. Health J. 2020, 57, 405–415. [Google Scholar] [CrossRef]
- Singh, H.J.L.; Couch, D.; Yap, K. Mobile Health Apps That Help With COVID-19 Management: Scoping Review. JMIR Nurs. 2020, 3, e20596. [Google Scholar] [CrossRef] [PubMed]
- Handa, M.; Gupta, N. A Study of the Relationship between Shopping Orientation and Online Shopping Behavior among Indian Youth. J. Internet Commer. 2014, 13, 22–44. [Google Scholar] [CrossRef]
- Kirchberg, J.; Fritzmann, J.; Weitz, J.; Bork, U. eHealth Literacy of German Physicians in the Pre–COVID-19 Era: Questionnaire Study. JMIR mHealth uHealth 2020, 8, e20099. [Google Scholar] [CrossRef] [PubMed]
- Yellowlees, P.; Chan, S.R.; Parish, M.B. The hybrid doctor–patient relationship in the age of technology—Telepsychiatry consultations and the use of virtual space. Int. Rev. Psychiatry 2015, 27, 476–489. [Google Scholar] [CrossRef]
- Tran, G.A.; Yazdanparast, A.; Strutton, D. Investigating the marketing impact of consumers’ connectedness to celebrity endorsers. Psychol. Mark. 2019, 36, 923–935. [Google Scholar] [CrossRef]
- Hu, L.; Min, Q.; Han, S.; Liu, Z. Understanding followers’ stickiness to digital influencers: The effect of psychological responses. Int. J. Inf. Manag. 2020, 54, 102169. [Google Scholar] [CrossRef]
- Liebers, N.; Straub, R. Fantastic relationships and where to find them: Fantasy and its impact on romantic parasocial phenomena with media characters. Poetics 2020, 83, 101481. [Google Scholar] [CrossRef]
- Kim, K.; Lustria, M.L.A.; Burke, D.; Kwon, N. Predictors of cancer information overload: Findings from a national survey. Inf. Res. 2007, 12, 12–14. [Google Scholar]
- Jiang, S.; Beaudoin, C.E. Health literacy and the internet: An exploratory study on the 2013 HINTS survey. Comput. Hum. Behav. 2016, 58, 240–248. [Google Scholar] [CrossRef]
- Giveon, S.; Yaphe, J.; Hekselman, I.; Mahamid, S.; Hermoni, D. The e-patient: A survey of israeli primary care physi-cians’ responses to patients’ use of online information during the consultation. Isr. Med. Assoc. J. 2009, 11, 537–541. [Google Scholar]
- Delone, W.H.; McLean, E.R. Information Systems Success: The Quest for the Dependent Variable. Inf. Syst. Res. 1992, 3, 60–95. [Google Scholar] [CrossRef] [Green Version]
- Delone, W.H.; McLean, E.R. The DeLone and McLean Model of Information Systems Success: A Ten-Year Update. J. Manag. Inf. Syst. 2003, 19, 9–30. [Google Scholar] [CrossRef]
- Hoffman, D.L.; Novak, T.P. Marketing in Hypermedia Computer-Mediated Environments: Conceptual Foundations. J. Mark. 1996, 60, 50. [Google Scholar] [CrossRef]
- Hair, J.F.; Sarstedt, M.; Ringle, C.M.; Mena, J.A. An assessment of the use of partial least squares structural equation modeling in marketing research. J. Acad. Mark. Sci. 2012, 40, 414–433. [Google Scholar] [CrossRef]
- Hair, J.F., Jr.; Matthews, L.M.; Matthews, R.L.; Sarstedt, M. PLS-SEM or CB-SEM: Updated guidelines on which method to use. Int. J. Multivar. Data Anal. 2017, 1, 107. [Google Scholar] [CrossRef]
- Liu, F.; Park, K.; Whang, U. Organizational Capabilities, Export Growth and Job Creation: An Investigation of Korean SMEs. Sustainability 2019, 11, 3986. [Google Scholar] [CrossRef] [Green Version]
- Cao, J.; Liu, F.; Shang, M.; Zhou, X. Toward street vending in post COVID-19 China: Social networking services information overload and switching intention. Technol. Soc. 2021, 66, 101669. [Google Scholar] [CrossRef]
- Korkmaz, S.; Goksuluk, D.; Zararsiz, G. MVN: An R Package for Assessing Multivariate Normality. R J. 2014, 6, 151–162. [Google Scholar] [CrossRef] [Green Version]
- Sharma, A.; Dwivedi, Y.K.; Arya, V.; Siddiqui, M.Q. Does SMS advertising still have relevance to increase consumer purchase intention? A hybrid PLS-SEM-neural network modelling approach. Comput. Hum. Behav. 2021, 124, 106919. [Google Scholar] [CrossRef]
- Harman, H. Modern Factor Analysis; Amsterdam University Press: Amsterdam, The Netherlands, 1976. [Google Scholar]
- Podsakoff, P.M.; MacKenzie, S.B.; Lee, J.Y.; Podsakoff, N.P. Common method biases in behavioral research: A critical review of the literature and recommended remedies. J. Appl. Psychol. 2003, 88, 879–903. [Google Scholar] [CrossRef]
- Kock, N. Common Method Bias in PLS-SEM. Int. J. e-Collab. 2015, 11, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Hair, J.F.; Risher, J.J.; Sarstedt, M.; Ringle, C.M. When to use and how to report the results of PLS-SEM. Eur. Bus. Rev. 2019, 31, 2–24. [Google Scholar] [CrossRef]
- Tenenhaus, M.; Vinzi, V.E.; Chatelin, Y.M.; Lauro, C. PLS path modeling. Comput. Stat. Data Anal. 2005, 48, 159–205. [Google Scholar] [CrossRef]
- Cao, Y.; Li, J.; Qin, X.; Hu, B. Examining the Effect of Overload on the MHealth Application Resistance Behavior of Elderly Users: An SOR Perspective. Int. J. Environ. Res. Public Health 2020, 17, 6658. [Google Scholar] [CrossRef] [PubMed]
- Benson, T.; Potts, H.; Bark, P.; Bowman, C. Development and initial testing of a Health Confidence Score (HCS). BMJ Open Qual. 2019, 8, e000411. [Google Scholar] [CrossRef] [Green Version]
- Sokolova, K.; Perez, C. You follow fitness influencers on YouTube. But do you actually exercise? How parasocial relationships, and watching fitness influencers, relate to intentions to exercise. J. Retail. Consum. Serv. 2020, 58, 102276. [Google Scholar] [CrossRef]
- Zafar, A.U.; Qiu, J.; Shahzad, M. Do digital celebrities’ relationships and social climate matter? Impulse buying in f-commerce. Internet Res. 2020, 30, 1731–1762. [Google Scholar] [CrossRef]
- Akter, S.; D’Ambra, J.; Ray, P. Service quality of mHealth platforms: Development and validation of a hierarchical model using PLS. Electron. Mark. 2010, 20, 209–227. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Items | Options | Frequency (Total = 316) | Percentage (%) |
|---|---|---|---|
| Gender | Male | 128 | 40.5 |
| Female | 188 | 59.5 | |
| Age | 18–20 | 55 | 17.4 |
| 21–30 | 84 | 26.6 | |
| 31–40 | 87 | 27.5 | |
| 41–50 | 44 | 13.9 | |
| 51 years or above | 46 | 14.6 | |
| Income (Per month) | RMB 1000–2000 | 47 | 14.9 |
| RMB 2001–3000 | 80 | 25.3 | |
| RMB 3001–4000 | 71 | 22.5 | |
| RMB 4001–5000 | 68 | 21.5 | |
| More than RMB 5000 | 50 | 15.8 | |
| Education | High School | 140 | 44.3 |
| Bachelor’s Degree | 154 | 48.7 | |
| Master or PhD Degree | 22 | 7 | |
| mHealth app Brand | Pingan Health App | 74 | 23.4 |
| Chunyu Doctor App | 70 | 22.2 | |
| Dinxiang Doctor App | 66 | 20.9 | |
| Other | 106 | 33.5 |
| Group | N | Mean (SD) | t-Value | Df | p-Value |
|---|---|---|---|---|---|
| mhealth users | 316 | 3.063 (0.640) | 9.972 | 291.203 | 0.000 |
| Non-mhealth users | 172 | 2.356 (0.801) |
| Latent Variable | Item | Loading | Mean (SD) | Cronbach’s a | CR | AVE |
|---|---|---|---|---|---|---|
| HAC | HAC1 | 0.927 | 3.044 (1.136) | 0.856 | 0.913 | 0.777 |
| HAC2 | 0.846 | |||||
| HAC3 | 0.869 | |||||
| ACO | ACO1 | 0.922 | 3.300 (1.080) | 0.909 | 0.937 | 0.787 |
| ACO2 | 0.818 | |||||
| ACO3 | 0.848 | |||||
| ACO4 | 0.955 | |||||
| PSR | PSR1 | 0.857 | 2.726 (0.672) | 0.840 | 0.892 | 0.674 |
| PSR2 | 0.777 | |||||
| PSR3 | 0.734 | |||||
| PSR4 | 0.889 | |||||
| UFI | UFI1 | 0.832 | 3.258 (0.807) | 0.827 | 0.884 | 0.656 |
| UFI2 | 0.791 | |||||
| UFI3 | 0.810 | |||||
| UFI4 | 0.805 | |||||
| UII | UII1 | 0.908 | 3.407 (0.855) | 0.885 | 0.921 | 0.747 |
| UII2 | 0.798 | |||||
| UII3 | 0.798 | |||||
| UII4 | 0.942 | |||||
| UDI | UDI1 | 0.902 | 3.058 (0.769) | 0.817 | 0.880 | 0.648 |
| UDI2 | 0.719 | |||||
| UDI3 | 0.787 | |||||
| UDI4 | 0.801 | |||||
| SPH | SPH1 | 0.882 | 3.062 (0.640) | 0.837 | 0.891 | 0.673 |
| SPH2 | 0.785 | |||||
| SPH3 | 0.708 | |||||
| SPH4 | 0.892 |
| HAC | ACO | PSR | UFI | UII | UDI | SPH | |
|---|---|---|---|---|---|---|---|
| HAC | |||||||
| ACO | 0.12 | ||||||
| PSR | 0.434 | 0.284 | |||||
| UFI | 0.441 | 0.536 | 0.314 | ||||
| UII | 0.346 | 0.454 | 0.267 | 0.439 | |||
| UDI | 0.396 | 0.348 | 0.478 | 0.302 | 0.326 | ||
| SPH | 0.334 | 0.44 | 0.344 | 0.559 | 0.392 | 0.517 |
| HAC | ACO | PSR | UFI | UII | UDI | SPH | |
|---|---|---|---|---|---|---|---|
| HAC | 0.881 | ||||||
| ACO | 0.106 | 0.887 | |||||
| PSR | 0.377 | 0.265 | 0.821 | ||||
| UFI | 0.383 | 0.473 | 0.276 | 0.81 | |||
| UII | 0.307 | 0.413 | 0.243 | 0.385 | 0.864 | ||
| UDI | 0.331 | 0.305 | 0.404 | 0.272 | 0.279 | 0.805 | |
| SPH | 0.296 | 0.394 | 0.308 | 0.491 | 0.346 | 0.447 | 0.82 |
| Hypotheses | ß | STDEV | t-Statistics | p-Values | Result |
|---|---|---|---|---|---|
| H1a: HAC → UFI | 0.323 | 0.045 | 7.148 | 0.000 | Support |
| H1b: HAC → UII | 0.248 | 0.053 | 4.705 | 0.000 | Support |
| H1c: HAC →UDI | 0.207 | 0.054 | 3.817 | 0.000 | Support |
| H2a: ACO → UFI | 0.428 | 0.043 | 9.933 | 0.000 | Support |
| H2b: ACO → UII | 0.373 | 0.05 | 7.513 | 0.000 | Support |
| H2c: ACO → UDI | 0.211 | 0.057 | 3.705 | 0.000 | Support |
| H3a: PSR → UFI | 0.041 | 0.05 | 0.819 | 0.413 | Reject |
| H3b: PSR → UII | 0.051 | 0.055 | 0.931 | 0.352 | Reject |
| H3c: PSR → UDI | 0.270 | 0.056 | 4.814 | 0.000 | Support |
| H4a: UFI → SPH | 0.359 | 0.052 | 6.874 | 0.000 | Support |
| H4b: UII →SPH | 0.120 | 0.049 | 2.456 | 0.014 | Support |
| H4c: UDI → SPH | 0.316 | 0.052 | 6.051 | 0.000 | Support |
| Path | ß | STDEV | t-Statistics | p-Values |
|---|---|---|---|---|
| HAC → UFI → SPH | 0.116 | 0.024 | 4.749 | 0.000 |
| ACO → UFI → SPH | 0.154 | 0.026 | 5.877 | 0.000 |
| PSR → UFI → SPH | 0.015 | 0.018 | 0.812 | 0.417 |
| HAC → UII → SPH | 0.03 | 0.014 | 2.089 | 0.037 |
| ACO → UII → SPH | 0.045 | 0.02 | 2.253 | 0.024 |
| PSR → UII → SPH | 0.006 | 0.008 | 0.783 | 0.434 |
| HAC → UDI → SPH | 0.066 | 0.02 | 3.21 | 0.001 |
| ACO → UDI → SPH | 0.067 | 0.02 | 3.331 | 0.001 |
| PSR → UDI → SPH | 0.085 | 0.025 | 3.392 | 0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cao, J.; Zhang, G.; Liu, D. The Impact of Using mHealth Apps on Improving Public Health Satisfaction during the COVID-19 Pandemic: A Digital Content Value Chain Perspective. Healthcare 2022, 10, 479. https://doi.org/10.3390/healthcare10030479
Cao J, Zhang G, Liu D. The Impact of Using mHealth Apps on Improving Public Health Satisfaction during the COVID-19 Pandemic: A Digital Content Value Chain Perspective. Healthcare. 2022; 10(3):479. https://doi.org/10.3390/healthcare10030479
Chicago/Turabian StyleCao, Junwei, Guihua Zhang, and Dong Liu. 2022. "The Impact of Using mHealth Apps on Improving Public Health Satisfaction during the COVID-19 Pandemic: A Digital Content Value Chain Perspective" Healthcare 10, no. 3: 479. https://doi.org/10.3390/healthcare10030479
APA StyleCao, J., Zhang, G., & Liu, D. (2022). The Impact of Using mHealth Apps on Improving Public Health Satisfaction during the COVID-19 Pandemic: A Digital Content Value Chain Perspective. Healthcare, 10(3), 479. https://doi.org/10.3390/healthcare10030479