
Hope Aspects of the Women’s Experience after Confirmation of a High-Risk Pregnancy Condition: A Systematic Scoping Review



Abstract
:1. Introduction
2. Materials and Methods
2.1. Review Questions
2.2. Inclusion Criteria
2.2.1. Participants
2.2.2. Concept
2.2.3. Context
2.2.4. Types of Sources
2.3. Search Strategy
2.4. Study/Source of Evidence Selection
2.5. Assessment of Methodological Quality
2.6. Data Extraction
2.7. Data Synthesis
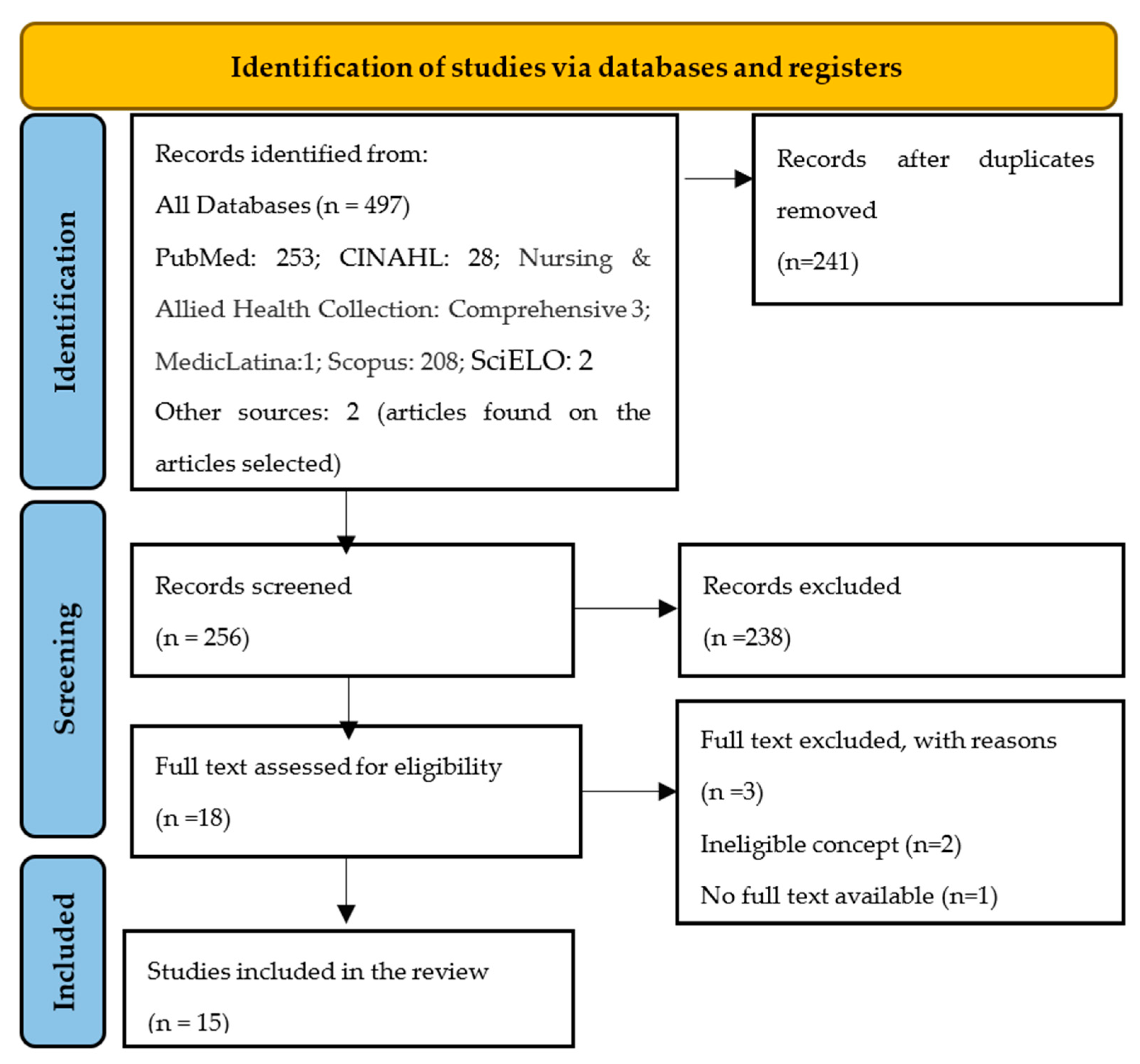
3. Results
3.1. Characteristics of Sources of Evidence
3.2. Critical Appraisal within Sources of Evidence
3.3. Results of Sources of Evidence
4. Discussion
5. Conclusions and Implications for Practice
6. Limitations
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

{kind=link}
| Scheme | Pubmed Search Equation | Results |
|---|---|---|
| #1 | pregnant women OR maternal OR expectant mother | 482,511 |
| #2 | high-risk pregnancy OR pregnancy complications OR obstetric complications OR medical condition OR obstetric health care | 2,526,150 |
| #3 | hope OR hopelessness | 89,314 |
| #4 | Qualitative Studies OR qualitative research OR phenomenological research OR Experiences OR Perceptions OR Attitudes OR Feelings OR meaning OR need | 3,843,920 |
| #5 | 1 AND 2 AND 3 AND 4 | 253 |
Appendix B
| Author(s) Year Publication Country | Hope and Hopeless Experiences or/and Expectations | Aims | Study Design | Study Population/Sample | Context | Population Characteristics and Typology | Main Results |
|---|---|---|---|---|---|---|---|
| The lived experience of women with a high-risk pregnancy: A phenomenology investigation Badakhsh, Hastings-Tolsma, Firouzkohi, Amirshahi & Hashemi (2020) Iran [18] | Hopelessness experiences are implicit with pregnancy concerns, worries about the child, future pregnancy, relations and support with others and increase cost Hope is implicit on adaptation to the challenges, believing that the condition would improve and being hopeful about the future. Spirituality, resorting to the God and Imans. | To describe the lived experience of women during HRP | Phenomenological study | Pregnant women | Public health centre in a large urban city in south-east Iran |
| Four thematic categories were extracted:
|
| Recasting Hope: A process of adaptation following fetal anomaly diagnosis Lalor, Begley & Galavan (2009) Ireland (United Kingdom) [28] | Hopelessness implicit on sense of incredulity, stress, the dually of the fight. Fear of developing a bond with the baby that could die. Initially some women hoped they would hear that the initial diagnosis was a mistake. Finally, in the rebuilding phase it would appear that the emergence of a positive vision of the future (whatever that might be), as the woman works through her experience in ways that permit her to reconstruct the future and adapt her previously held beliefs about pregnancy in particular and the world in general. | To provide a theorical framework of the process of adaptation following fetal anomaly diagnosis based on women’s experiences of carrying a baby with a fetal abnormality up to the end and beyond the birth | Grounded theory study | Pregnant women carrying a baby with fetal abnormality | Fetal medicine unit of a major Dublin maternity hospital | All Irish women. Forty-one women, eleven primigravidae and 30 multigravidae. Thirthy-one women continued the pregnancy and ten travelled to UK to access termination of pregnancy services not available within the state. Forty women were married or partnered and although not all pregnancies were planned, all were wanted. | Recasting Hope, the process of adaptation following diagnosis is represented temporally as four phases: ‘Assume Normal’, ‘Shock’, ‘Gaining Meaning’ and ‘Rebuilding’. Some mothers expressed a sense of incredulity when informed of the anomaly and the ‘Assume Normal’ phase provides an improved understanding as to why women remain unprepared for an adverse diagnosis. Transition to phase 2, ‘Shock,’ is characterised by receiving the diagnosis and makes explicit women’s initial reactions. Once the diagnosis is confirmed, a process of ‘Gaining Meaning’ commences, whereby an attempt to make sense of this ostensibly negative event begins. ‘Rebuilding’, the final stage in the process, is concerned with the extent to which women recover from the loss and resolve the inconsistency between their experience and their previous expectations. |
| When fetal hydronephrosis is suspected antenatally—a qualitative study Oscarsson, Gottvall & Swahnberg (2015) Sweden [19] | Hopelessness experiences of anxiety and fears about the unknown, worry and stress. Experiences of hope are based on going through crisis by knowing that you are doing the right thing, told themselves that they would deal with it after delivery and that everything would be all right at the end | To explore women’s reactions to the discovery of fetal hydronephrosis in the context of uncertainty regarding the prognosis | Qualitative study | Pregnant women | University clinic of Sweden | Ten women with antenatal diagnosis were invited to the interview 6-12 months after delivery. Mean age were 30.6 years. Six nulliparous and four parous. | The core category, ‘Going through crisis by knowing that you are doing the right thing’ illustrates the meaning of women’s reactions and feelings. It illuminates the four categories: ‘When the unexpected happens’—on the one hand, women had positive views that the suspicious malformation could be discovered; however, on the other hand, women questioned the screening. ‘To live in suspense during pregnancy’—the suspicious malformation caused anxiety and was a stressful situation. ‘Difficulties in understanding information’—the women thought they had limited knowledge and had difficulties in understanding the information. ‘Suppress feelings and hope for the best’—the women tried to postpone the problem and thought they should deal with it after delivery |
| Pregnancy through the Lens of Iranian Women with HIV: A Qualitative Study Zahra Behboodi-Moghadam, Khalajinia, Nasrabadi, Mohraz & Gharacheh (2015) Iran [20] | Hopelessness experiences implicit on the concerns about transmitting the virus to the baby, effects on their health. Becoming a mother after a HIV diagnosis was a source of hope, value and esteem, children seen as a “divine gift”, a chance to correct past mistakes. By participating in spiritual practices, women believed that God would respond to their needs, God would take care of their children. | To explore the experience of pregnancy among Iranian women with HIV | Qualitative study | Pregnant women | Counseling Center for Behavioral Diseases in Imam Khomeini Hospital in Tehran, Iran. | The study participants’ age ranged from 22 to 39 years. Five of them had completed primary school and 7 had finished high school. Length of time since HIV diagnosis was 1 to 5 years. A total of 7 participants had children and 5 of them reported being pregnant for the first time. Nine of the women (75%) had been infected with HIV by their husbands and 3 of them (25%) through unknown route. | Four main themes emerged from the data: fear and hope, stigma and discrimination, marital life stability, and trust in God. Despite concerns about mother-to-child transmission of HIV, and uncertain life span, HIV-infected women tended to continue their pregnancy, and having children was viewed as a window of hope for them. |
| Perspectives on pregnancy in women with Chronic Kidney Disease (CKD): A Semistructured Interview Study Tong, Brown, Winkelmayer, Craig & Jesudason (2015) Australia [21] | Hopelessness showed by conscious of fragility, noxious self, denied motherhood, social jealousy, fear of genetic transmission. Hope implicit on the opportunity of getting pregnant, found that the baby didn’t have the same disease, valuing life, gratitude in hindsight and focus on what is good. | To describe the beliefs, values, and experiences of pregnancy in women with CKD to inform prepregnancy counseling and pregnancy care. | Qualitative study | Pregnant women | Two renal units in Australia | 41 women (95% response rate) aged 22 to 56 years with CKD stages 3 to 5 (n 5 5), receiving dialysis (n 5 5), or received a kidney transplant (n 5 31) from 2 renal units in Australia. | Six themes were identified: bodily failure (conscious of fragility, noxious self, critical timing, and suspended in limbo), devastating loss (denied motherhood, disempowered by medical catastrophizing, resolving grief, barriers to parenthood alternatives, and social jealousy), intransigent guilt (disappointing part- ners, fear of genetic transmission, respecting donor sacrifice, and medical judgment), rationalizing conse- quential risks (choosing survival, avoiding fetal harm, responding to family protectiveness, compromising health, decisional ownership, and unjustifiable gamble), strengthening resolve (hope and opportunity, medical assurance, resolute determination, and reticent hope), and reorientating focus (valuing life and gratitude in hindsight). |
| Lived experiences of women with maternal near miss: qualitative research Sabzevari, Yazdi,& Rad (2021) Iran [22] | Hopelessness implicit on fears and concerns. Unable to get pregnant again, fear of raising their child without siblings, concerns about their child without a mother, re-marriage of the spouse if the spouse wanted more children, fear of getting pregnant again and experiencing postpartum complications, failure to adjust to complications and prolonged mourning, feeling guilty, not tolerating pain, irritability, and postpartum depression. The only hope seemed to be believing in God’s will and their survival and ability to support their children. | To understand experiences and perceptions of women with higher risk pregnancy relating to problems/needs of health and care practices. | Descriptive and qualitative | Pregnant women | The interviews were conducted at the office of the educational supervisor of Sabzevar Mobini Hospital or any other place that was conveni- ent to the mothers (e.g. their home). | The mothers were selected based on their ability to express their near-miss experience and willingness to be interviewed. The age range of the selected mothers was 19–36 years. | Five main categories were extracted, including fears and concerns, failure to accept and adapt, tolerating physical and psychological pain and hardships, death experience, and medical team mismanagement. Regret and fear of raising the child with siblings, fear of the re- marriage of the spouse, and fear of complications and costs were among the subcategories of fears and concerns. Lack of adaptation to the complications and prolonged mourning were the subcategories of failure to accept and adapt, and the subcategories of tolerating physical and psychological pain and hardships were a sense of guilt, tolerating physical pain, hopelessness, irritability, hatred toward the medical team, and postpartum depression. In addition, returning to normal life, and seeing/actually feeling death were the subcategories of the death experience. The subcategories of the medical team mismanagement included medical errors, lack of sup- port/negligence, |
| Emotional and cognitive experiences of pregnant women following prenatal diagnosis of fetal anomalies: A qualitative study in Iran Irani, Khadivzadeh, Nekah, Ebrahimipour & Tara (2019) Iran [29] | Hopelessness is defined by disbelief, distress, panic and shock during the time of diagnosis. When their pregnancy was terminated, women experienced perinatal loss such as guilt and shame during pregnancy termination, loss of their expected child, suffering and emotional distress process, and fear of recurrence in future pregnancies. Women that decided to continue their pregnancy had a dilemma between hope and worries. In general, women carrying babies tried to keep a positive attitude towards the birth, as a way to cope with the situation. They were hopeful about the best possible outcome or return of normality. Some women hope that the problem for the health of their unborn child in the case of abnormal findings will be resolved or is miner anomaly. | To explore the emotional and cognitive experiences of pregnant women following prenatal diagnosis of fetal anomalies in Mashhad, Iran. | Qualitative study | Pregnant women | Two tertiary referral centers for fetal anomaly at Mashhad University Hospitals, Omolbanin Hospital and Imam Reza Hospital in Mashhad, Iran. | The sample studied consisted of Persian speaking parents with prenatal diagnosis of fetal anomalies at the gestational week of 12–27. All the pregnant women with a suspected or definitive diagnosis of fetal anomaly as per the ultrasound or the combined test (NT, free β-hCG and PAPP-A) were eligible for participation. | Four categories and 10 subcategories emerged. Category one, grief reactions during the time of diagnosis, contained two subcategories: shocked and panicked, and distressed and disbelieved. Category two, perinatal loss through a pregnancy termination, contained four subcategories: guilt and shame during pregnancy termination, loss of their expected child, suffering and emotional distress process, and unmet needs by health professionals. Category three, fears of recurrence in future pregnancies, had two subcategories: worried about inadequate prenatal care in the future pregnancies and worried about abnormal fetus in next pregnancies. Finally, Category four, a dilemma between hope and worries contained two subcategories: hope for normality and worried about future. |
| Complexity of consenting for medical termination of pregnancy: Prospective and longitudinal study in Paris Tayeh, Jouannic, Mansour, Kesrouani &Attieh (2018) Paris [30] | Hope implicit in religious beliefs and convictions and believed that their child could exceptionally survive after birth. | To analyze the patients’ perception of prenatal diagnosis of fetal cardiac pathology, and the reasons for choosing to continue with pregnancy despite being eligible to receive a medical termination of pregnancy. | Descriptive, prospective and longitudinal study | Pregnant women | Hôpital Necker—Enfants Malades in Paris, France | Eligible participants were pregnant women who decided to continue their pregnancy despite an unfavorable medical advice because they were carrying fetuses with incurable cardiac pathologies. Age between 23 and 44 years old. | Patient informed consent should be sought before any decision in neonatology, even if conflicting with the medical team’s knowledge and the pregnant mother’s benefits. Decisions to accept or decline pregnancy termination depend on the patients’ psychological character, ideologies, convictions, and mistrust in the diagnosis/prognosis, or hope in the fetus survival. |
| Women’s Voices: The Lived Experience of Pregnancy and Motherhood After Diagnosis With HIV Sanders (2008) New York (USA) [23] | Hopelessness characterized by periods of emotional distress, ambivalence in relation to pregnancy and mother- hood, and stigma. Hope in protecting children from contracting HIV and from HIV related stigma and hoped to rectify mistakes made with children born previously and to be a good, loving mother. | The study aimed to explore the meaning of pregnancy after diagnosis with HIV | Qualitative study | Pregnant women | Interviews conducted in two academic health centers in metropolitan New York. | Participants were a purposive sampling of 9 women, 34 to 53 years old, who had been diagnosed with HIV and were currently pregnant or who had become mothers postdiagnosis. | The result of the study included themes of extreme emotional distress after HIV diagnosis, feeling stigmatized, emotions related to the pregnancy and baby, experiences with health care providers, and as positive and supporting. |
| The lived experiences of rural women diagnosed with the human Immunodeficiency virus in the antenatal period Fords, Crowley & Merwe (2017) South Africa [25] | Hopelessness implicit in a negative self-image, loneliness, feelings of isolation, fear from loved ones, women experienced blame, fear, the cruelties of stigma, stereotyping and judging an avoided any romantic relationship. Fear of being ill, being in a hospital or dying. Women felt hope to live and see the future of their children, hope on their spiritual beliefs. The initiation of ART gave them hope as they were confident that the treatment would improve their health, extend their life, protect their unborn children and even cure HIV. The most important hope that they had for the future was that their unborn child would be HIV free | To explore the lived experiences of women diagnosed with HIV in the antenatal period in a rural area in the Eastern Cape province of South Africa. | Phenomenological study | Pregnant women | Pregnant women residing in the Maluti local service area in the Eastern Cape who attended one the local clinics. | Ten women over the age of 18, diagnosed with HIV for the first time in the antenatal period of pregnancy. | Women diagnosed with HIV during pregnancy are ultimately concerned with the wellbeing of their unborn children, and this concern motivates their adherence to ART. Women’s lived experiences are situated in their unique sociocultural context, and although some known challenges remain, counselling and support strategies need to be informed by exploring context-specific issues and involving the local community. |
| The Lived Experiences of HIV-Positive, Pregnant Women in Thailand Ross, Sawatphanit, Wilaiphan; Burke & Suwansujarid (2007) Thailand [24] | Hopelessness: Women perceived their lives as a struggle. Struggling alone and experiences of shock, fear, anxiety and depression; Sharing one’s struggling, with fears of stigmatization and discrimination; struggling for the baby, most postpartum Thai mothers indicated that their babies were central to their determination in helping them to move on with their lives; Struggling through ups and downs Hope: Women found hope through the taking of antiretroviral medicines and, subsequently, showed a desire to fight the virus as long as possible for their children. For health care professionals, when a seropositive pregnant woman who has her baby as her hope is feeling “down,” gently reminding her of her unborn baby could be a help in lifting her hope and spirit | The purpose of our study was to examine the lived experiences of 10 pregnant women in Thailand following their HIV diagnosis | Phenomenological study | Pregnant women newly diagnose with HIV | Prenatal clinic at a government hospital in Thailand | All participants were Buddhist. They ranged in age from 18 to 29 years. Five were graduates of primary school, 3 had completed junior high school, and 2 had finished high school. Nine had a monthly low family income. Only one participant had a middle-class family. Eight were married or lived with a partner, and 2 were divorced. | All participants in these study decided not to end their pregnancies. This might be explained in the fact that all women were Buddhist, with Buddhists usually believing that terminating one’s life or ending a pregnancy is a big sin. From a health care perspective, identifying helpful resources such as a peer/support group can be critical for a woman when she is ready to share her struggle with others. Peer support was found to be helpful for 7 women in our study and has been found to be effective across cultures and countries in reducing seropositive women’s fears, depression, and attempts at suicide. In general, support from health care professionals to assist the HIV-positive mother’s efforts to promote her baby’s health will be of great value, regardless of the ultimate diagnosis of the baby’s HIV status. |
| The experiences of women with maternal near miss and their perception of quality of care in Kelantan, Malaysia: a qualitative study Norhayati, Hazlina, Nik Hussain; Asrenee & Sulaiman (2017) Malaysia [26] | Hopelessness: several forms of negative emotions such as fear, anxiety, alarm, incomplete self, discouragement and numbness. Fear on their own lives and lives of their babies, fear for the prenatal outcomes and of undergoing surgery, fear of recurrence similar incidents and inability to conceive in the future, sense of death; incomplete self, because being a woman without a uterus and without a baby; sadness for not being able to have more children Hope: The women adapted to most of negative emotions and to difficult life events, like traumatic childbirth by anchoring their reasoning to religiosity and faith and appeared to have accepted the situation calmly. They responded to their situations positively, delegating the resolution to God and regarding what had happened as what God had planned for them. They were very grateful that God gave them a second chance. Other forms of adaptation included natural maternal disposition in which their attention were distracted and focused on their children and that was a motivator to seek treatment and as a source of strength to continue living. The competency of the healthcare providers in the form of adequate knowledge and skills in providing optimal care had gained trust from the women. Emotion and social support and improved relationship quality were associated with better mental health and well-being, reduced stress and protection from postpartum depression. In the current study, social support appeared to play a role in protecting the women from ill health. Despite their experiences, the women were relieved at having survived their acute, severe complications and looked forward to resuming their lives normally. | This study aimed to explore the experiences of women with maternal near miss and their perception of the quality of care in Kelantan, Malaysia | Qualitative phenomenological approach | All women screened for the presence of any vital organ dysfunction or failure based on the World Health Organization criteria for maternal near miss. | All women admitted to labour room, obstetrics and gynaecology wards and intensive care units in 2014 | Thirty women who had experienced maternal near miss events were included in the analysis. All were Malays between the ages of 22 and 45. Almost all women (93.3%) had secondary and tertiary education and 63.3% were employed. | In appraising the maternal near miss events, the study found that the women viewed their experiences as frightening and that they experienced other negative emotions and a sense of imminent death. Their perceptions of the quality of their care were influenced by the competency and promptness in the provision of care, interpersonal communication, information-sharing and the quality of physical resources. These factors should be of concern to those seeking to improve services at healthcare facilities. The predisposition to seek healthcare was influenced by costs, self-attitude and beliefs. |
| The lived experience of pregnancy while carrying a child with a known, nonlethal congenital abnormality Hedrick (2004) USA [32] | Hopelessness is define by the loss of the perfect baby with feelings of grief, shock, anger and guilt. Hope defined with good sources of information, time to prepare, support from family and friends, spiritual beliefs and staying busy with work and other activities and empathizing with the baby | To gain an understanding of the experience of pregnancy while carrying a child with a known, nonlethal congenital abnormality | Phenomenological study | Pregnant women | Outpatient perinatal center at a large Midwestern hospital | Ages between 18 and 44 years. Gestacional age at the time of the diagnosis 17 to 26 weeks. Interviewed between 24 and 36 weeks. Fetal diagnosis of neural tube defect, cleft lip, congenital heart defect, renal anomaly, cystic malformation of the long and down syndrome | The pregnancy experience was of a paradoxical nature. Knowledge of fetal diagnosis with positive and negative consequences. Time is good but also the enemy; you grieve but you do not grieve; my baby’s not perfect, but he’s still mine |
| Feelings and expectations of pregnant women living with HIV: A phenomenological study Arcoverde, Conter, Silva & Santos (2015) Brazil [27] | Hopelessness:
| The objective of this research was to identify the feelings and expectations of such pregnant women about the disease and pregnancy | Phenomenological qualitative research based on Maurice Merleau-Ponty’s philosophy of perception | Pregnant women with HIV diagnosis | Outpatient unit of the SAE of Foz do Iguaçu, in the state of Parana | Five pregnant women diagnosed with HIV monitored in SAE of Foz do Iguaçu, in the state of Paraná, participated in the study. They were married, aged between 20 and 35 years old, and had been diagnosed from one month to ten years before research began | The interviews conveyed the experiences of the women with HIV, their acceptance of the limitations imposed by the disease and showed how they dealt with the stigma surrounding HIV. Despite the prejudice, such pregnant women did not lose faith and hope. Pregnant women believe in the treatment and the possibility of their children being born healthy. The desire of motherhood increases their expectations about the care, which prevents complications from the infection. The study participants accepted the pregnancy, mainly because the desire to become a mother was stronger than anything else they could feel. The treatment was then accepted, as the only way to protect their children from a HIV infection. The researchers identified feelings of strength, will, and determination to overcome the problems which transcend the difficulties encountered throughout pregnancy. The fear of harming the child—symbol of perseverance, wishes and hopes—is faced and reignites their desire to carry on living in order to care for their children and to protect them. Communication and education for the construction of new concepts and ideas related to the phenomenon can indicate new ways to learn about change processes. Social movements, cultural changes, as well as social equality and inequality; action and intervention based on fair policies can also be one of the responses to the problem. |
| ‘We did everything we could’—a qualitative study exploring the acceptability of maternal-fetal surgery for spina bifida to parents Crombag, Sacco, Stocks, Vloo, Merwe, Gallagher, David, Marlow & Deprest (2021) Belgium and United Kingdom [31] | Hopelessness:
| To explore the concepts and strategies parents employ when considering maternal-fetal surgery (MFS) as an option for the management of spina bifida (SB) in their fetus, and how this determines the acceptability of the intervention | Qualitative study | Parents | Two MFS partner centres with specialist assessment (University Hospitals Leuven, Belgium; University College London Hospital, United Kingdom) | Parents whose fetuses with SB were eligible for MFS, Age above 18 years old. | MFS for SB remains highly acceptable from diagnosis until 3–6 months postnatally. For those opting for MFS, expectations seemed to be realistic yet were driven by hope and expectation of the best outcome. For parents opting for termination of pregnancy, the potential benefit of MFS seems to play a minimal role in their final decision |
Appendix C
| Article | Abstract and Title | Introduction and Aims | Method and Data | Sampling | Data Analysis | Ethics and Bias | Results | Transferability or Generalizability | Implications and Usefulness | TOTAL |
| Badakhsh, Hastings-Tolsma, Firouzkohi, Amirshahi & Hashemi (2020) [18] | 4 | 4 | 4 | 4 | 4 | 4 | 4 | 4 | 4 | 36 |
| Lalor, Begley & Galavan (2009) [28] | 4 | 4 | 4 | 4 | 4 | 4 | 4 | 4 | 4 | 36 |
| Oscarsson, Gottvall & Swahnberg (2015) [19] | 4 | 4 | 4 | 4 | 4 | 4 | 4 | 4 | 4 | 36 |
| Behboodi-Moghadam, Khalajinia, Nasrabadi, Mohraz & Gharacheh (2015) [20] | 4 | 4 | 4 | 4 | 4 | 4 | 4 | 3 | 3 | 34 |
| Tong, Brown, Winkelmayer, Craig & Jesudason (2015) [21] | 4 | 4 | 4 | 4 | 4 | 4 | 4 | 4 | 4 | 36 |
| Sabzevari, Yazdi, & Rad (2021) [22] | 4 | 4 | 4 | 4 | 4 | 3 | 4 | 3 | 3 | 33 |
| Irani, Khadivzadeh, Nekah, Ebrahimipour & Tara (2019) [29] | 4 | 4 | 4 | 4 | 4 | 4 | 4 | 4 | 4 | 36 |
| Tayeh, Jouannic, Mansour, Kesrouani &Attieh (2018) [30] | 4 | 4 | 4 | 4 | 4 | 3 | 4 | 4 | 4 | 35 |
| Sanders (2008) [23] | 3 | 4 | 4 | 4 | 4 | 4 | 4 | 4 | 4 | 35 |
| Fords, Crowley & Merwe (2017) [25] | 4 | 4 | 4 | 4 | 4 | 4 | 4 | 4 | 4 | 36 |
| Ross, Sawatphanit, Wilaiphan; Burke & Suwansujarid (2007) [24] | 4 | 4 | 4 | 3 | 4 | 4 | 4 | 3 | 3 | 33 |
| Norhayati, Hazlina, Nik Hussain; Asrenee & Sulaiman (2017) [26] | 4 | 4 | 3 | 4 | 3 | 3 | 4 | 3 | 4 | 32 |
| Hedrick (2004) [32] | 4 | 4 | 3 | 4 | 3 | 3 | 4 | 4 | 3 | 32 |
| Arcoverde, Conter, Silva & Santos (2015) [27] | 4 | 4 | 4 | 4 | 3 | 4 | 3 | 3 | 3 | 32 |
| Crombag, Sacco, Stocks, Vloo, Merwe, Gallagher, David, Marlow & Deprest (2021) [31] | 4 | 4 | 4 | 4 | 4 | 4 | 4 | 4 | 4 | 36 |
References
- WHO. Maternal Mortality. World Heal Organ. 2019. Available online: https://www.who.int/news-room/fact-sheets/detail/m (accessed on 24 May 2022).
- Alkema, L.; Chou, D.; Hogan, D.; Zhang, S.; Moller, A.B.; Gemmill, A.; Fat, D.M.; Boerma, T.; Temmerman, M.; Mathers, C.; et al. National, regional and global levels and trend in MMR between 1990 and 2015 with scenario-based projections to 2030; a systematic analysis by the United Nations Maternal Mortality. Lancet 2016, 387, 462–474. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- James, D.K.; Steer, J.P. High-Risk Pregnancy: Management Options. 5th Edition. 2018, pp. 227–248. Available online: https://www.cambridge.org/us/academic/subjects/medicine/obstetrics-and-gynecology-reproductive-medicine/high-risk-pregnancy-management-options-5th-edition-1 (accessed on 6 June 2022).
- Bonanno, L.; Bennett, M.; Pitt, A. The experience of parents of newborns diagnosed with a congenital anomaly at birth: A systematic review protocol. JBI Database Syst. Rev. Implement Rep. 2013, 11, 100–111. [Google Scholar] [CrossRef]
- Leichtentritt, R.D.; Blumenthal, N.; Elyassi, A.; Rotmensch, S. High-Risk Pregnancy and Hospitalization: The Women’s Voices. Health Soc. Work. 2005, 30, 39–47. [Google Scholar] [CrossRef] [PubMed]
- WHO. Congenital Anomalies. 2017, pp. 1–2. Available online: https://www.who.int/news-room/fact-sheets/detail/c (accessed on 22 June 2022).
- Atienza-Carrasco, J.; Linares-Abad, M.; Padilla-Ruiz, M.; Morales-Gil, I.M. Experiences and outcomes following diagnosis of congenital foetal anomaly and medical termination of pregnancy: A phenomenological study. J. Clin. Nurs. 2020, 29, 1220–1237. [Google Scholar] [CrossRef]
- Sara Manuela Airosa da Silva Vinculação Materna durante e após a Gravidez: Ansiedade, Depressão, Stress e Suporte Social Universidade Fernando Pessoa Faculdade de Ciências Humanas e Sociais Mestrado Psicologia Clínica e da Saúde. Available online: https://bdigital.ufp.pt/bitstream/10284/3259/3/DM_16833.pdf (accessed on 20 September 2022).
- Georgsson Öhman, S.; Saltvedt, S.; Grunewald, C.; Waldenström, U. Does fetal screening affect women’s worries about the health of their baby? Acta Obstet. Gynecol. Scand. 2004, 83, 634–640. [Google Scholar] [CrossRef] [Green Version]
- De Araújo, W.S.; Romero, W.G.; Zandonade, E.; Amorim, M.H.C. Efeitos do relaxamento sobre os níveis de depressão em mulheres com gravidez de alto risco: Ensaio clínico randomizado. Rev. Lat. Am. Enferm. 2016, 24. [Google Scholar] [CrossRef]
- Oliveira, D.d.C.; Mandú, E.N.T. Women with high-risk pregnancy: Experiences and perceptions of needs and care. Esc Anna Nery—Rev. Enferm. 2015, 19, 93–101. [Google Scholar] [CrossRef]
- Bailey, T.C.; Snyder, C.R. Satisfaction with life and hope: A look at age and marital status. Psychol. Rec. 2007, 57, 233–240. [Google Scholar] [CrossRef] [Green Version]
- International Council of Nurses. CIPE® Versão 2019. Classificação Internacional Para a Prática de Enfermagem. Lisboa. Ordem dos Enfermeiros. 2019. Available online: https://www.icn.ch/what-we-do/projects/ehealth-icn (accessed on 6 June 2022).
- Jones, A.C. Relevant Hope to Promote Therapeutic Change. Linkedin. 2019. Available online: https://www.linkedin.com/pulse/relevant-hope-promote-therapeutic-change-alun-charles-jones (accessed on 6 June 2022).
- Martocchio, D.K.C. Hope: Its spheres and dimensions. Nurs. Clin. N. Am. 1985, 20, 382–389. [Google Scholar]
- Institute, J.B. The Joanna Briggs Institute Reviewer’s Manual 2020. Methodology for JBI Reviewers. 2020. Available online: https://jbi-global-wiki.refined.site/space/MANUAL/. (accessed on 20 March 2022).
- Ricco, A.C.; Lillie, E.; Zarin, W.O.K. PRISMA extension for scoping reviews (PRISMA-ScR): Checklist and explanation. Ann. Intern. Med. 2018, 169, 467–473. [Google Scholar]
- Badakhsh, M.; Hastings-Tolsma, M.; Firouzkohi, M.; Amirshahi, M.; Hashemi, Z.S. The lived experience of women with a high-risk pregnancy: A phenomenology investigation. Midwifery 2020, 82. [Google Scholar] [CrossRef]
- Oscarsson, M.; Gottvall, T.; Swahnberg, K. When fetal hydronephrosis is suspected antenatally-a qualitative study. BMC Pregnancy Childbirth 2015, 15, 349. [Google Scholar] [CrossRef]
- Behboodi-Moghadam, Z.; Khalajinia, Z.; Nasrabadi, A.R.N.; Mohraz, M.; Gharacheh, M. Pregnancy through the Lens of Iranian Women with H.I.V. J. Int. Assoc. Provid. AIDS Care 2016, 15, 148–152. [Google Scholar] [CrossRef] [Green Version]
- Tong, A.; Brown, M.A.; Winkelmayer, W.C.; Craig, J.C.; Jesudason, S. Perspectives on pregnancy in women with CKD: A semistructured interview study. Am. J. Kidney Dis. 2015, 66, 951–961. [Google Scholar] [CrossRef]
- Sabzevari, M.; Eftekhari Yazdi, M.; Rad, M. Lived experiences of women with maternal near miss: A qualitative research. J. Matern. Neonatal Med. 2021, 35, 7158–7165. [Google Scholar] [CrossRef]
- Sanders, L.B. Women’s Voices: The Lived Experience of Pregnancy and Motherhood After Diagnosis With HIV. J. Assoc. Nurses AIDS Care 2008, 19, 47–57. [Google Scholar] [CrossRef] [PubMed]
- Ross, R.; Sawatphanit, W.; Draucker, C.B.; Suwansujarid, T. The lived experiences of HIV-positive, pregnant women in Thailand. Health Care Women Int. 2007, 28, 731–744. [Google Scholar] [CrossRef] [PubMed]
- Fords, G.; Crowley, T.; Merwe, M. The Lived Experiences of Rural Women Diagnosed with the Human Immunodeficiency Virus in the Antenatal Period. 2017. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5639609/pdf/rsah-14-1379430.pdf (accessed on 25 May 2022).
- Norhayati, M.N.; Hazlina, N.H.N.; Asrenee, A.R.; Sulaiman, Z. The experiences of women with maternal near miss and their perception of quality of care in Kelantan, Malaysia: A qualitative study. BMC Pregnancy Childbirth 2017, 17, 189. [Google Scholar] [CrossRef] [Green Version]
- Arcoverde, M.A.M.; Conter, R.S.; da Silva, R.M.M.; dos Santos, M.F. Feelings and Expectations of Pregnant Women Living With Hiv: A Phenomenological Study. REME Rev. Min. Enferm. 2015, 19, 561–566. [Google Scholar] [CrossRef] [Green Version]
- Lalor, J.; Begley, C.M.; Galavan, E. Recasting Hope: A process of adaptation following fetal anomaly diagnosis. Soc. Sci. Med. 2009, 68, 462–472. [Google Scholar] [CrossRef]
- Irani, M.; Khadivzadeh, T.; Nekah, S.M.A.; Ebrahimipour, H.; Tara, F. Emotional and cognitive experiences of pregnant women following prenatal diagnosis of fetal anomalies: A qualitative study in Iran. Int. J. Community Based Nurs. Midwifery 2019, 7, 22–31. [Google Scholar] [PubMed]
- Tayeh, G.; Jouannic, J.M.; Mansour, F.; Kesrouani, A.; Attieh, E. Complexity of consenting for medical termination of pregnancy: Prospective and longitudinal study in Paris. BMC Med. Ethics 2018, 19, 33. [Google Scholar]
- Crombag, N.; Sacco, A.; Stocks, B.; De Vloo, P.; Van Der Merwe, J.; Gallagher, K.; David, A.; Marlow, N.; Deprest, J. ‘We did everything we could’—A qualitative study exploring the acceptability of maternal-fetal surgery for spina bifida to parents. Prenat. Diagn. 2021, 41, 910–921. [Google Scholar] [CrossRef] [PubMed]
- Hedrick, J. The lived experience of pregnancy while carrying a child with a known, nonlethal congenital abnormality. JOGNN J. Obstet. Gynecol. Neonatal Nurs. 2005, 34, 732–740. [Google Scholar] [CrossRef]

| Hopelessness Experiences | Hope Experiences |
|---|---|
|
| Hopelessness Experiences | Hope Experiences |
|---|---|
|
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Antunes, M.; Viana, C.R.; Charepe, Z. Hope Aspects of the Women’s Experience after Confirmation of a High-Risk Pregnancy Condition: A Systematic Scoping Review. Healthcare 2022, 10, 2477. https://doi.org/10.3390/healthcare10122477
Antunes M, Viana CR, Charepe Z. Hope Aspects of the Women’s Experience after Confirmation of a High-Risk Pregnancy Condition: A Systematic Scoping Review. Healthcare. 2022; 10(12):2477. https://doi.org/10.3390/healthcare10122477
Chicago/Turabian StyleAntunes, Mónica, Clara Roquette Viana, and Zaida Charepe. 2022. "Hope Aspects of the Women’s Experience after Confirmation of a High-Risk Pregnancy Condition: A Systematic Scoping Review" Healthcare 10, no. 12: 2477. https://doi.org/10.3390/healthcare10122477
APA StyleAntunes, M., Viana, C. R., & Charepe, Z. (2022). Hope Aspects of the Women’s Experience after Confirmation of a High-Risk Pregnancy Condition: A Systematic Scoping Review. Healthcare, 10(12), 2477. https://doi.org/10.3390/healthcare10122477