1. Public Interest Summary
Evidence-based measurements are becoming increasingly popular among policymakers and administrators in the healthcare sector to identify shortcomings in healthcare delivery. As a result, it is critical to characterize health inequalities as discrepancies in the quality of care provided. This has the potential to provide an effective framework for those who are involved in initiatives to identify health disparities. Furthermore, it is most successful in leveraging performance improvement when evidence-based measures are used. Therefore, studies focused on inequalities are extremely important for policymakers to consider. In order to address this issue, some researchers are advocating for introducing quality measures suitable for tracking healthcare quality discrepancies at the subpopulation level.
2. Background
Approximately 945,000 deaths are attributed to cardiovascular diseases annually in the United States, which accounts for about 41% of all mortalities in the country [
1]. Cardiovascular diseases also contribute to high morbidity in the country. Indeed, they account for about 6 million hospital admissions annually [
2,
3]. Diabetes mellitus refers to dysglycaemia that is accompanied by nephropathy, retinopathy, and cardiovascular diseases, among others. Some cardiovascular diseases associated with diabetes mellitus include congestive heart failure, stroke, cardiomyopathy, and coronary heart disease, among others. Cardiovascular disease and diabetes mellitus comorbidities are associated with early death. In 1999, a collective effort of the following organizations resulted in recognition of the need for collective cooperation in the prevention of cardiovascular disease in diabetes patients: the American Diabetes Association (A.D.A.), the National Institute of Diabetes and Digestive and Kidney Diseases, and National Heart, Lung, and Blood Institute (NHLBI), Juvenile Diabetes Foundation International, and the American Heart Association (A.H.A.) [
4]. The pathophysiology of cardiovascular disease involves the thickening of arterial walls, which occurs gradually.
Clinical detection of atherosclerosis is only possible at an advanced level, which has made clinical assessment impractical. However, imaging technology advancements have produced sophisticated and effective tools for detecting atherosclerosis at an early stage. These advancements have also made it possible to classify people based on their exposure to the risk of atherosclerosis symptoms. These advancements also provide the means for assessing the treatment results and improving the current understanding of atherosclerosis biology [
5]. The problem statement of the present study is as follows. The American College of Cardiology/American Heart Association (ACC/AHA) released new cholesterol management guidelines in 2019. Since then, the guidelines have been updated severally. Indeed, the guidelines are updated frequently to incorporate new evidence. However, in many cases, healthcare providers do not keep up with the frequency at which changes are made.
Consequently, they often fail to implement them in clinical practice. Based on the latest A.H.A. data, an appropriate statin regimen was prescribed to only about 46.4% and 30% of diabetes patients and patients with atherosclerotic cardiovascular disease (ASCVD). Charity care clinics can adopt various interventions for safe statin use. Such interventions include the following: educational programs, frequent reminders, support tools, and outcome evaluation [
6].
Healthcare providers also need to educate their patients on the right dose and side effects of statins. They should also regularly check the patient’s medication list to ensure safety and prevent drug–drug interaction. Nursing staff also need to verify medication compliance and conduct patient counseling on various issues, such as the recommended way to administer drugs and report any possible identified concerns to prescribers. Efforts should also be made to ensure equal access to the same information among members of interprofessional teams for informed decision-making and improved therapeutic outcomes. Consequently, we present a hypothesis that an approach that involves systematic identification of targeted interventions and barriers at the following levels presents high prospects of improving cholesterol management efforts: electronic medical records (E.M.R.), pharmacy levels, and providers.
Atherosclerotic cardiovascular disease accounts for most deaths and disabilities in North America. In response to this high burden, the American Heart Association launched an initiative in 1996 dubbed “Guide to the Primary Prevention of Cardiovascular Disease.” The guide was updated in 2002 [
7]. These guidelines, however, do not address the prevention of atherosclerosis in children. However, interventions targeting this group carry many prospects of success [
8].
3. Methodology
To achieve a 25% relative improvement by six months based on the baseline data of the appropriate intensity statin prescription for patients with ASCVD or D.M. by medical resident trainees in our single-center primary care clinic.
3.1. Family of Measures
In
Table 1, it’s the conceptual definition of our study measures.
3.2. Key Stakeholders
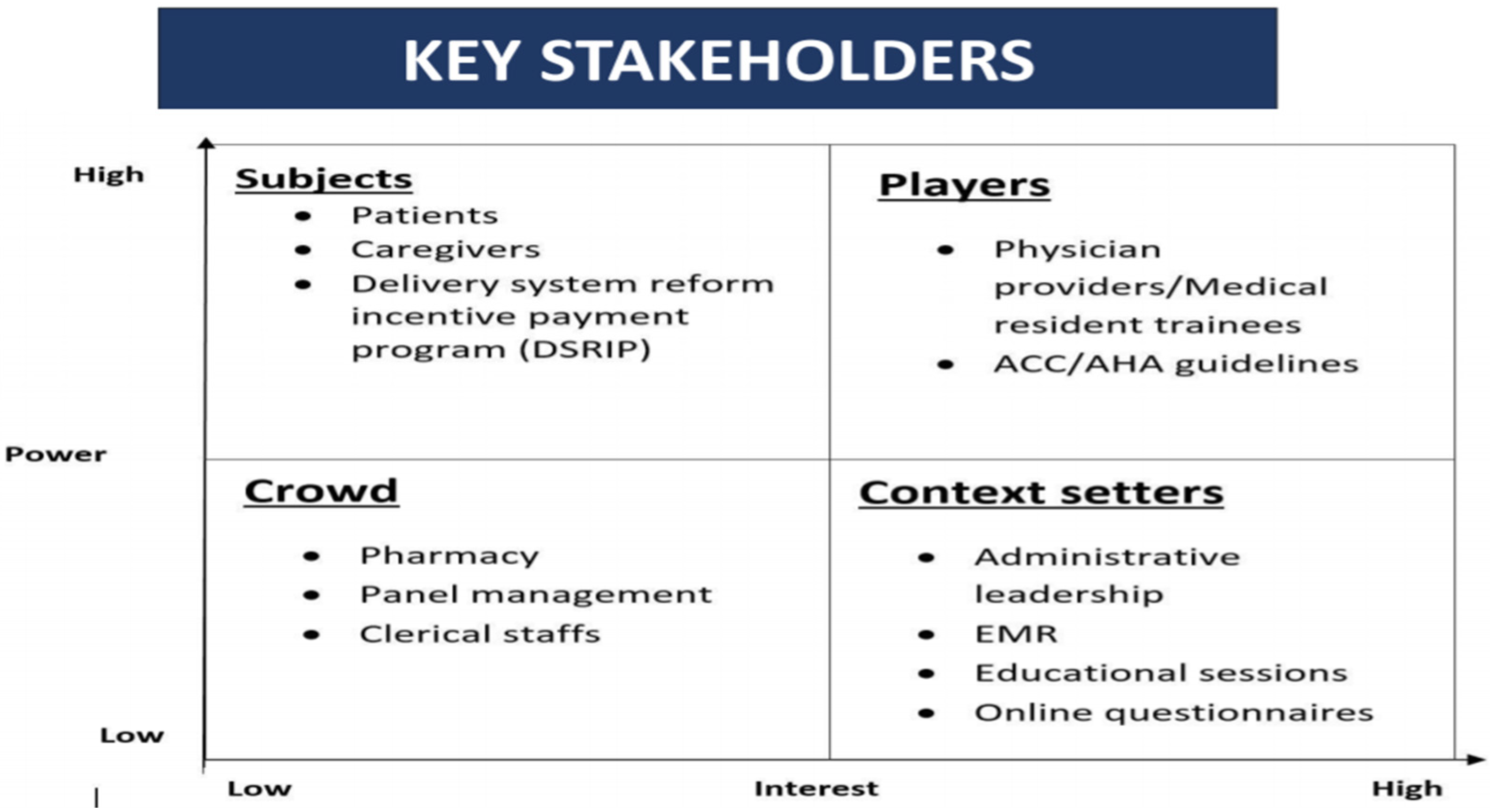
People involved in statin use in the charity care primary clinic are stakeholders. The following matrix explains the role of interest and power in the high and low context (
Figure 1). When interest and power are high, their players (physician providers/ Medical resident trainees, ACC/AHA guidelines) play a vitally important role in the matrix. When the role of interest and power is low, the crowd (pharmacy, panel management, clerical staff) in the matrix plays a vibrant role. When the role of interest is high and power is low, the context setters (Administrative leadership, E.M.R., Educational sessions, and online questionnaires) in the matrix play a dynamic role. When the role of interest is low and power is high, the subjects (Patients, caregivers, delivery system reform incentive payment program (DSRIP)) play a vicarious role.
At the beginning stage of the research, a questionnaire was circulated among 51 internal medicine residents to identify the barriers to appropriate statin prescriptions at the clinic. Ten items of the questionnaire were measured using the dichotomous scale (Yes/No) given in
Table 2. Items of the questionnaire were adopted from the poster by Khetan et al. in March 2017. The details of the participants were kept anonymous in order to avoid social desirability bias among the participants of the study.
4c PDSA cycles were run during the study’s observation for six months. The PDSA cycle is an iterative, four-step model for improving a process. The first step is developing a plan in which predictions of outcomes are clearly stated and tasks are assigned. The plan’s who, what, when, and where are decided in this phase. In the “do” phase, the plan is implemented. Data and results obtained are then analyzed in the “study” phase. Lastly, the plan is either adopted, adapted, or abandoned in the “act” phase based on the evaluation of the data in the prior step. Learning from one cycle should guide the cycles that follow. Here, the Interventions intensified during each subsequent cycle. The interventions were then incorporated into routine clinical practice.
The present study intended to improve the performance of our institutional practice. The study also constitutes a part of resident education. Consequently, it did not go through the I.R.B. review process. Additionally, the patient data were obtained from the data bank available for hospital quality metrics.
3.3. Data Analysis
3.3.1. Problem Characterization
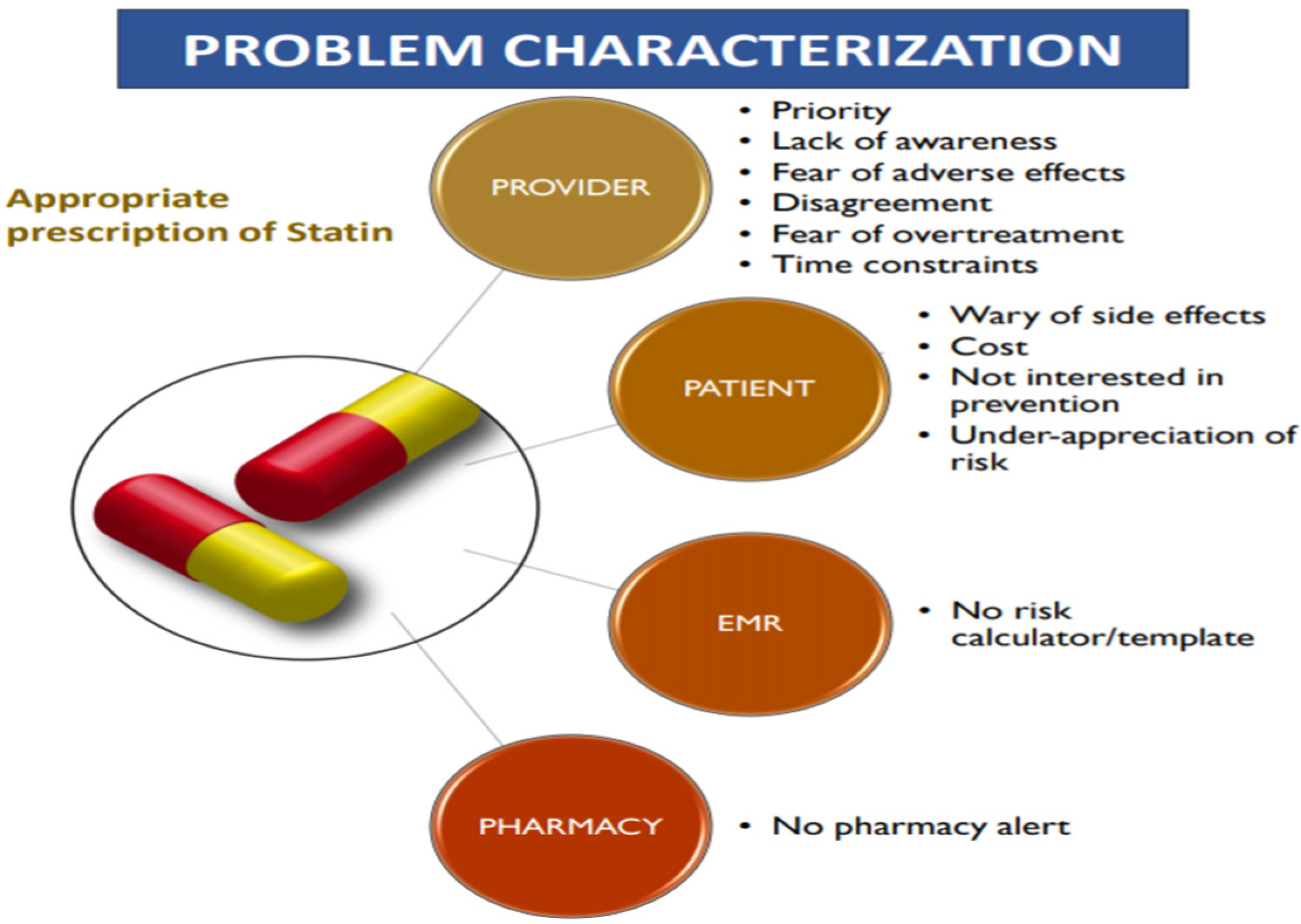
Characterization of the problem for an appropriate statin prescription could be broadly classified into four categories (see
Figure 2). They are (a) provider, (b) patient, (c) EMR, (d) Pharmacy. “Provider” barriers could be broadly classified into six major points: a priority, lack of awareness, fear of adverse effects, disagreement, fear of overtreatment, and time constraints. “Patient” barriers could be classified into four major points: the worry of side effects, costs, lack of interest in prevention, and under-appreciation of risk. THE “E.M.R.” barrier relies on no risk calculator/template. The “Pharmacy” barrier relies on no pharmacy chart.
3.3.2. Intervention
Medical resident trainees in the clinic were surveyed to understand the barriers to prescribing statins and are identified.
3.3.3. Implementation
In
Table 3, it shows the PDSA cycles that we implemented and the outcomes obtained.
4. Findings
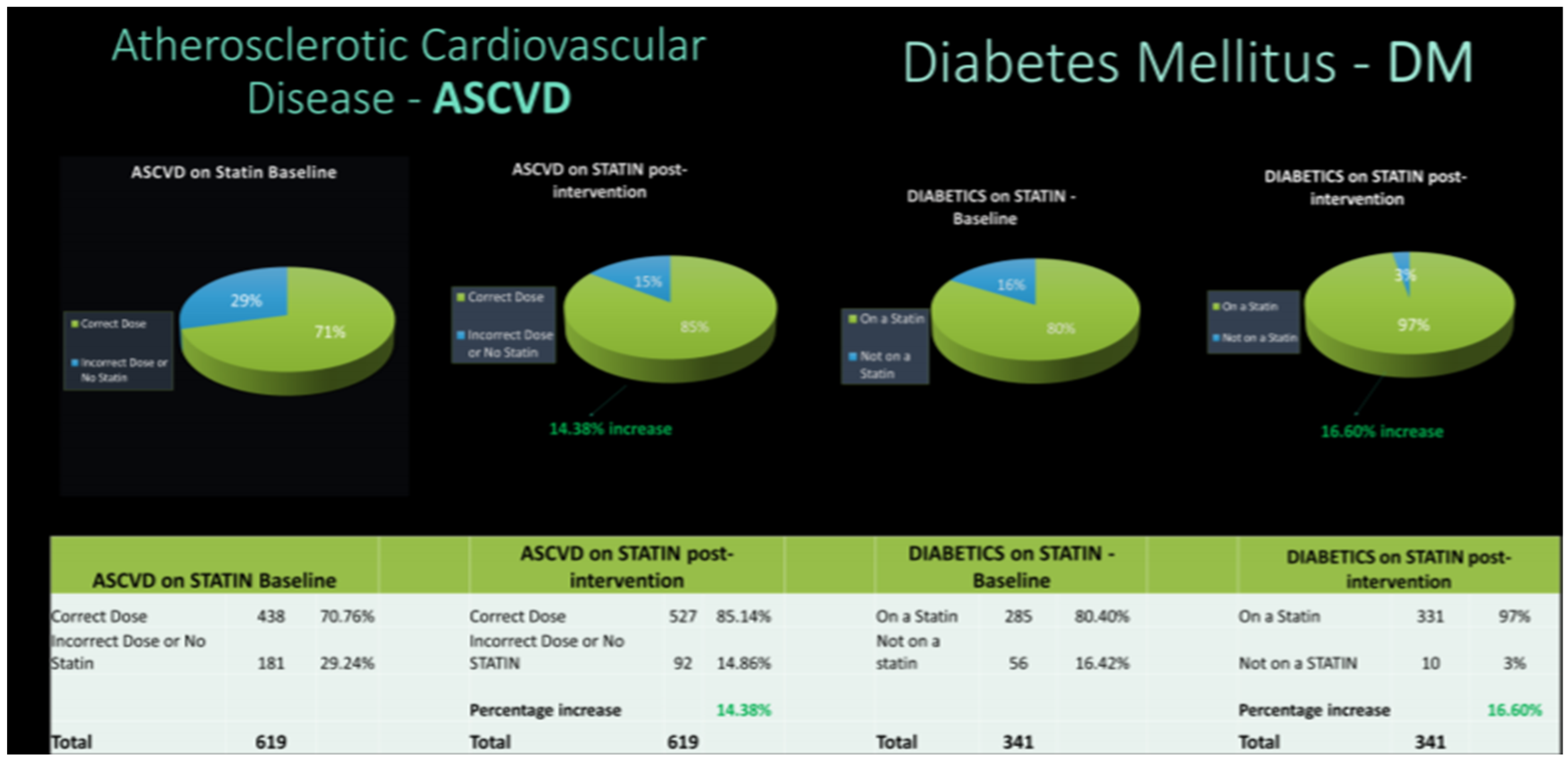
Seventy-point seven percent of cardiovascular disease patients were found to be on the appropriate statin dose at baseline. On the other hand, the proportion of patients with diabetes mellitus who were on proper dose statin was 80.4%. After one month, the proportion of patients with cardiovascular disease on the appropriate statin dose had increased by 8.4%. On the other hand, the proportion of patients with diabetes mellitus who were on appropriate statins increased by 4.2%.
Figure 3 shows the results after six months.
5. Limitations
A fair change in clinical practice was observed among the internal medicine resident community, though the aim was not achieved by 25% relative improvement. In addition, an attempt to compare the prescription of statin use among the attendings and residents was made but did not receive adequate responses to the survey among the attending population.
6. Discussion
In March 2019, a new guideline for the initiation of statin treatment targeting cardiovascular disease prevention was released by the American Heart Association (ACC/AHA) and the American College of Cardiology [
9]. Unlike the previous guidelines, these guidelines focused on the risk of total atherosclerotic cardiovascular disease (ASCVD) [
10,
11,
12]. In this case, the cardiovascular disease risk employed in these guidelines was based on deemphasizing low-density lipoprotein (LDL) cholesterol thresholds and new Pooled Cohort Equations. Four categories of statin treatment eligibility for adults aged 40–75 years were established by the ACC/AHA guidelines. The new cardiovascular disease risk threshold provides the basis for the use of statins in treating abnormal cholesterol in 8.2 million adults more in the United States [
13]. However, expanding the eligible age for starting statin treatment under the ACC/AHA guidelines has elicited controversy [
14]. Some critics have argued that the Pooled Cohort Equations are prone to overestimating risk. This exposes many adults to unnecessary statin use in the United States [
15,
16]. Optimal Medline
search strategies can be developed and tested by
retrieving sound clinical
studies on prevention or
treatment of health disorders [
17,
18,
19].
Statins are well tolerated. However, recent evidence suggests that it could lead to an increased risk of diabetes [
7,
20]. However, there is no consensus on this observation. Instead, other researchers suggest that statins should be used under ACC/AHA guidelines based on the conclusion that statins reduce the risk of LDL cholesterol [
7,
16,
21]. In previous studies, evidence shows that using a relatively lenient threshold could be cost-effective. This is the case even though statin use is associated with diabetes risk [
22]. Our studies seek to generate a hypothesis to aid in the analysis of cost-effectiveness based on the ACC/AHA guidelines. This effort stands to help in establishing optimal value for cardiovascular disease threshold for ten years [
13,
23,
24]. These healthcare use disparities are potentially attributed to factors linked to providers, patients, or systems [
25]. Alternatively, they could be attributed to social inequalities such as socioeconomic status. Consequently, there is a need for healthcare researchers to understand and examine possible ways in which the underlying factors (at the system, organizational, individual, and provider levels) impact health and disparities in healthcare status and access.
Policymakers and administrators in the healthcare sector are increasingly adopting the use of evidence-based measures to detect inadequacies in healthcare quality. The importance of clinical decision-making can be seen in the clinical reasoning which is based on complex and multifaceted cognitive processes, and the level of cognition is perhaps the most relevant factor that impacts the physician’s clinical reasoning [
26,
27,
28]. Therefore, it is vital to define health disparities as gaps in the quality of care. This offers a practical framework for efforts to detect health disparities. Furthermore, evidence-based measures are mainly effective in leveraging performance improvement [
29]. Consequently, studies focusing on disparities are highly necessary for policymakers. Therefore, some researchers push for developing quality measures to monitor healthcare quality disparities at the subpopulation level [
30].
This study further highlights the significance of the role played by the leadership of junior doctors in the Implementation and sustenance of the improvement programs. Junior doctors remain untapped as a potential talent pool for quality improvement measures. Therefore, there is a need to equip them with information on potential pitfalls, which can be instrumental in reducing system errors that commonly inflict healthcare organizations [
31]. There is a need for the e-learning platform to improve the performance outcome of these junior doctors [
32]. Through teamwork and effective communication, the consistency of the PDSA cycle was realized. Efforts to demonstrate concurrent maintenance of morale change implementation poses a challenge. However, it is necessary for success [
33].
7. Conclusions
In conclusion, this study finds that PDSA cycles pose significant prospects for increased rates of statin use. In addition, the study finds that PDSA could lead to quicker ACC/AHA guideline uptake.
8. Implications
Insights that have already been gathered show that doubts about the guidelines, overmedication of people at low risk, time limitations, and time limitations constitute some of the main barriers to increased use of prescriptions. Enhancing appropriate usage of statin can be improved through proactive panel management.
9. Key Highlights
The experiment takes place in a charity care clinic serving a large population in the northeastern United States, serving a huge population. There are 51 internal medicine residents at the facility. The facility has an electronic health record system used by the clinical staff.
In addition, clinicians use electronic drug prescribing to streamline the process (E-Scribe).
This quality improvement project hypothesizes that an education campaign on electronic pop-up reminders and evidence-based algorithms targeting prescribers will have the capacity to increase awareness of cardiovascular disease and diabetes mellitus recommendations in the future.
This study result was presented at the following conferences:
2021 Annual Research Day, Saint Peter’s University Hospital, New Brunswick, United States.
ACPNJ Scientific meeting 2020, Princeton, United States.
Resident 360 QI Challenge 2020.
Author Contributions
Conceptualization, H.D.M. and R.N.D.; Data curation, C.K.; Methodology, H.D.M.; Project administration, H.D.M.; Resources, H.D.M. and R.N.D.; Supervision, R.N.D.; Writing–original draft, H.D.M. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Conflicts of Interest
The authors declare no conflict of interest.
References
- U.S. Department of Justice. Annual Summary of Births, Marriages, Divorces, and Deaths: United States, 1993. Available online: https://www.ojp.gov/ncjrs/virtual-library/abstracts/annual-summary-births-marriages-divorces-and-deaths-united-states (accessed on 8 July 2022).
- Graves, E. National Hospital Discharge Survey: Annual summary, 1992. Vital Health Stat. 13 1994, 119, 1–63. [Google Scholar]
- Stafford, R.; Blumenthal, D.; Pasternak, R. Variations in Cholesterol Management Practices of U.S. Physicians. J. Am. Coll. Cardiol. 1997, 29, 139–146. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Buse, J.; Ginsberg, H.; Bakris, G.; Clark, N.; Costa, F.; Eckel, R.; Fonseca, V.; Gerstein, H.C.; Grundy, S.; Nesto, W.R.; et al. Primary Prevention of Cardiovascular Diseases in People with Diabetes Mellitus. Diabetes Care 2007, 30, 162–172. [Google Scholar] [CrossRef]
- Sanz, J.; Fayad, Z. Imaging of atherosclerotic cardiovascular disease. Nature 2008, 451, 953–957. [Google Scholar] [CrossRef] [PubMed]
- BSussman, J.; Holleman, R.; Youles, B.; Lowery, J. Quality Improvement and Personalization for Statins: The QUIPS Quality Improvement Randomized Trial of Veterans’ Primary Care Statin Use. J. Gen. Intern. Med. 2018, 33, 2132–2137. [Google Scholar] [CrossRef] [PubMed]
- Robinson, J. Accumulating Evidence for Statins in Primary Prevention. JAMA 2013, 310, 2405. [Google Scholar] [CrossRef] [PubMed]
- Kavey, R.; Daniels, S.; Lauer, R.; Atkins, D.; Hayman, L.; Taubert, K. American Heart Association Guidelines for Primary Prevention of Atherosclerotic Cardiovascular Disease Beginning in Childhood. Circulation 2003, 107, 1562–1566. [Google Scholar] [CrossRef]
- Arnett, D.; Blumenthal, R.; Albert, M.; Buroker, A.; Goldberger, Z.; Hahn, E.; Himmelfarb, C.D.; Khera, A.; Lloyd-Jones, D.; McEvoy, J.W.; et al. 2019 ACC/AHA Guideline on the Primary Prevention of Cardiovascular Disease: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Circulation 2019, 140, e596–e646. [Google Scholar] [CrossRef]
- Stone, N.; Robinson, J.; Lichtenstein, A.; Bairey Merz, C.; Blum, C.; Eckel, R.; Goldberg, A.C.; Gordon, D.; Levy, D.; Lloyd-Jones, D.M.; et al. 2013 ACC/AHA Guideline on the Treatment of Blood Cholesterol to Reduce Atherosclerotic Cardiovascular Risk in Adults. J. Am. Coll. Cardiol. 2014, 63, 2889–2934. [Google Scholar] [CrossRef]
- Bucholz, E.; Rodday, A.; Kolor, K.; Khoury, M.; de Ferranti, S. Prevalence and Predictors of Cholesterol Screening, Awareness, and Statin Treatment Among US Adults with Familial Hypercholesterolemia or Other Forms of Severe Dyslipidemia (1999–2014). Circulation 2018, 137, 2218–2230. [Google Scholar] [CrossRef]
- Psaty, B.; Weiss, N. 2013 ACC/AHA Guideline on the Treatment of Blood Cholesterol. JAMA 2014, 311, 461. [Google Scholar] [CrossRef] [PubMed]
- Pandya, A.; Sy, S.; Cho, S.; Weinstein, M.; Gaziano, T. Cost-effectiveness of 10-Year Risk Thresholds for Initiation of Statin Therapy for Primary Prevention of Cardiovascular Disease. JAMA 2015, 314, 142. [Google Scholar] [CrossRef] [PubMed]
- Guallar, E.; Laine, C. Controversy Over Clinical Guidelines: Listen to the Evidence, Not the Noise. Ann. Intern. Med. 2014, 160, 361–362. [Google Scholar] [CrossRef]
- Abramson, D.J.; Redberg, F.R. Don’t Give More Patients Statins. New York Times, 2013. Available online: https://hms.harvard.edu/news/dont-give-more-patients-statins (accessed on 8 July 2022).
- Ridker, P.; Cook, N. Statins: New American guidelines for prevention of cardiovascular disease. Lancet 2013, 382, 1762–1765. [Google Scholar] [CrossRef]
- Corrao, S.; Colomba, D.; Arnone, S.; Argano, C.; Chiara, T.D.; Scaglione, R.; Licata, G. Improving Efficacy of PubMed Clinical Queries for Retrieving Scientifically Strong Studies on Treatment. J. Am. Med. Inform. Assoc. 2006, 13, 485–487. [Google Scholar] [CrossRef] [PubMed]
- Corrao, S.; Colomba, D.; Argano, C.; Calvo, L.; Scaglione, R.; Licata, G. Optimized Search Strategy for Detecting Scientifically Strong Studies on Treatment through PubMed. Intern. Emerg. Med. 2012, 7, 283–287. [Google Scholar] [CrossRef] [PubMed]
- Haynes, R.B.; McKibbon, K.A.; Wilczynski, N.L.; Walter, S.D.; Werre, S.R. Optimal search strategies for retrieving scientifically strong studies of treatment from Medline: Analytical survey. BMJ 2005, 330, 1179. [Google Scholar] [CrossRef]
- Sattar, N.; Preiss, D.; Murray, H.; Welsh, P.; Buckley, B.; de Craen, A.; Seshasai, S.R.K.; McMurray, J.J.; Freeman, D.J.; Jukema, J.W.; et al. Statins and risk of incident diabetes: A collaborative meta-analysis of randomised statin trials. Lancet 2010, 375, 735–742. [Google Scholar] [CrossRef]
- Goff, D.; Lloyd-Jones, D.; Bennett, G.; Coady, S.; D’Agostino, R.; Gibbons, R.; Greenland, P.; Lackland, D.T.; Levy, D.; O’Donnell, J.C.; et al. 2013 ACC/AHA Guideline on the Assessment of Cardiovascular Risk. Circulation 2014, 129 (Suppl. 2), S49–S73. [Google Scholar] [CrossRef] [PubMed]
- Deaño, R.; Pandya, A.; Jones, E.; Borden, W. A Look at Statin Cost-Effectiveness in View of the 2013 ACC/AHA Cholesterol Management Guidelines. Curr. Atheroscler. Rep. 2014, 16, 438. [Google Scholar] [CrossRef] [PubMed]
- Krumholz, H. The New Cholesterol and Blood Pressure Guidelines. JAMA 2014, 311, 1403. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Pencina, M.; Navar-Boggan, A.; D’Agostino, R.; Williams, K.; Neely, B.; Sniderman, A.; Peterson, E.D. Application of New Cholesterol Guidelines to a Population-Based Sample. N. Engl. J. Med. 2014, 370, 1422–1431. [Google Scholar] [CrossRef]
- Hope, H.; Binkley, G.; Fenton, S.; Kitas, G.; Verstappen, S.; Symmons, D. Systematic review of the predictors of statin adherence for the primary prevention of cardiovascular disease. PLoS ONE 2019, 14, e0201196. [Google Scholar] [CrossRef]
- Lütgendorf-Caucig, C.; Kaiser, P.A.; Machacek, A.; Waldstein, C.; Pötter, R.; Löffler-Stastka, H. Vienna Summer School on Oncology: How to Teach Clinical Decision Making in a Multidisciplinary Environment. BMC Med. Educ. 2017, 17, 100. [Google Scholar] [CrossRef]
- Seitz, T.; Raschauer, B.; Längle, A.S.; Löffler-Stastka, H. Competency in Medical History Taking—The Training Physicians’ View. Wien. Klin. Wochenschr. 2019, 131, 17–22. [Google Scholar] [CrossRef] [PubMed]
- Corrao, S.; Argano, C. Rethinking clinical decision-making to improve clinical reasoning. Front. Med. 2022, 9, 900543. [Google Scholar] [CrossRef] [PubMed]
- Kilbourne, A.; Switzer, G.; Hyman, K.; Crowley-Matoka, M.; Fine, M. Advancing Health Disparities Research Within the Health Care System: A Conceptual Framework. Am. J. Public Health 2006, 96, 2113–2121. [Google Scholar] [CrossRef] [PubMed]
- Reason, J. Beyond the organisational accident: The need for “error wisdom” on the frontline. Qual. Saf. Health Care 2004, 13 (Suppl. 2), ii28–ii33. [Google Scholar] [CrossRef]
- Reason, J. Human error: Models and management. BMJ 2000, 320, 768–770. [Google Scholar] [CrossRef]
- Turk, B.; Ertl, S.; Wong, G.; Wadowski, P.P.; Löffler-Stastka, H. Does case-based blended-learning expedite the transfer of declarative knowledge to procedural knowledge in practice? BMC Med. Educ. 2019, 19, 447. [Google Scholar] [CrossRef]
- Chin, M. Quality Improvement Implementation and Disparities. Med. Care 2010, 48, 668–675. [Google Scholar] [CrossRef] [PubMed]
| Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).







{kind=link}
{kind=link}
{kind=link}