Abstract
The aim of this study was to discuss the differences in pre-hospital time intervals between rural and urban communities regarding emergency medical services (EMS). A systematic search was conducted through various relevant databases, together with a manual search to find relevant articles that compared rural and urban communities in terms of response time, on-scene time, and transport time. A total of 37 articles were ultimately included in this review. The sample sizes of the included studies was also remarkably variable, ranging between 137 and 239,464,121. Twenty-nine (78.4%) reported a difference in response time between rural and urban areas. Among these studies, the reported response times for patients were remarkably variable. However, most of them (number (n) = 27, 93.1%) indicate that response times are significantly longer in rural areas than in urban areas. Regarding transport time, 14 studies (37.8%) compared this outcome between rural and urban populations. All of these studies indicate the superiority of EMS in urban over rural communities. In another context, 10 studies (27%) reported on-scene time. Most of these studies (n = 8, 80%) reported that the mean on-scene time for their populations is significantly longer in rural areas than in urban areas. On the other hand, two studies (5.4%) reported that on-scene time is similar in urban and rural communities. Finally, only eight studies (21.6%) reported pre-hospital times for rural and urban populations. All studies reported a significantly shorter pre-hospital time in urban communities compared to rural communities. Conclusions: Even with the recently added data, short pre-hospital time intervals are still superior in urban over rural communities.
1. Introduction
Immediate, essential emergency medical services (EMS) are well-known systems for patients suffering from accidents and other individuals with acute or exacerbating emergency conditions on top of other chronic conditions [1]. These services are critical in saving patients’ lives and enhancing the prognoses of their conditions. In this context, relevant previous studies show that with a lack of EMS-related interventions, affected patients will eventually suffer long-term or short-term outcomes after worsening of their medical condition or traumatic injury [2,3]. On the other hand, research shows that enhancing the quality of immediate pre-hospital care can remarkably decrease the incidence of health-related complications and enhance the prognoses of patients [4,5,6].
Pre-hospital time intervals have a huge impact on patients receiving EMS. Evidence shows that these intervals are remarkably different in urban and rural communities [7]. In this context, different metrics have been proposed in the literature, including response time (which is the time taken from receiving the alarm to arriving on-scene), on-scene time (which is the time taken from arriving on-scene to leaving), transport time (which is the time between leaving the scene and arriving at a specialized management centre), and pre-hospital time (which includes all pre-hospital time intervals combined, i.e., the time taken from receiving the alarm to arriving at a specialized management centre). Previous data suggest that pre-hospital time intervals are better in urban areas than in rural areas [3,8]. Moreover, in a previous review, Cabral et al. [8] concluded that studying response time is essential to improving the integrity of EMS in a healthcare system.
There are many factors to consider when evaluating the success of EMS. These include the availability of necessary services, including appropriate vehicles, socioeconomic factors, access to appropriate materials, well-equipped personnel, and coordination of the response process [9,10]. Accordingly, different studies have investigated the impact of these factors, which can affect EMS in rural and urban communities [7,11,12,13,14]. For instance, previous investigations show that patients living in rural countries have longer waiting times for ambulances [12,15,16,17,18]. This is usually associated with severe health-related adverse events and worsens their survival rates [19]. Accordingly, healthcare authorities should enhance the quality of care for this group by considering the delivery of adequate and timely medical services regardless of geographical difficulties [16,20].
Many recent studies have been published to provide more data on whether rural pre-hospital time intervals are comparable to those of urban communities [7,12,14,21,22,23]. Moreover, it is logical that initial management guidelines have remarkably changed since previous data were published. This indicates the need to assess current pre-hospital time intervals, which can help healthcare authorities plan adequate interventions and enhance their EMS and patients’ outcomes. However, no cumulative evidence exists regarding the differences in these metrics and intervals between urban and rural communities. Therefore, this systematic review aims to discuss and update the current knowledge of the differences in pre-hospital time intervals between rural and urban communities regarding EMS.
2. Materials and Methods
2.1. Study Outcomes and Inclusion Criteria
The main of the present investigation is to compare EMS in rural (all population, housing, and territory not included within an urbanized area or urban cluster) and urban areas (community belonging to, or relating to, a city or town). The terms of comparison will include on-scene time, transport time, response time, and pre-hospital time. Therefore, inclusion criteria include (1) original investigations that (2) compared ground pre-hospital EMS time intervals in rural and urban communities and (3) included patients that required or called EMS secondary to any acute and/or chronic conditions. On the other hand, citations that (1) were not original; (2) included only limited cases (like case reports and case series); (3) did not report either on-scene time, transport time, response time, or pre-hospital time; (4) did not compare between EMS in rural and urban communities; (5) did not include patients in their sample (like studies that obtained their outcomes from surveying healthcare officials and paramedics); (6) were not human studies; (7) were editorials, theses, protocols, commentaries, or reviews; (8) were not published in English; or (9) did not have an accessible full-text were excluded from this study. Finally, definitions of rural and urban settings were established as recognized by the authors of each included study.
2.2. Search Strategy
The steps of this systematic review were conducted based on the recommendations of the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA). Based on the study outcomes, the relevant keywords were obtained to develop and perform the search strategy, mainly composed of electronic database searching and manual searching, to obtain all relevant investigations. Finally, the following search term was used: (“Emergency Service” OR “Emergency Medical Services” OR “Emergency Medical Technicians” OR “Emergency medicine” OR paramedic* OR ambulance* OR emergency OR trauma OR EMT OR “pre-hospital” OR “out of hospital” OR “EMS”) AND (“Hospitals, Urban” OR “Urban Population” OR “Urban Health Services” OR “Urban Health” OR “Rural Health Personnel” OR “Urban Areas” OR “Hospitals, Rural” OR “Rural Health Services” OR “Rural Areas” OR “Rural Population” OR “Rural Health” OR “Rural Health Centres”) AND (“Response Time” OR “Golden Hour” OR “Duration Time” OR “Transport Time” OR “On-Scene time”). In addition, the following databases were searched: PubMed, Scopus, Web of Science, Cochrane Library and Cochrane Central Register of Controlled Trials (CENTRAL), and Google Scholar in March 2022. It should be noted that only relevant articles published since 1990 were included in this study. This was decided based on a previous meta-analysis by Carr et al. [24], which showed that the quality of EMS care was significantly different in 1990–2005 compared to 1975–1989 in the United States. Accordingly, only articles published since 1990 were included to provide more updated evidence regarding pre-hospital time intervals in rural and urban communities.
2.3. Screening Process
After completing the search strategy, articles went through screening and data extraction. The screening was conducted at first by title/abstract, and then by full texts of the included articles. This was performed based on the aforementioned inclusion and exclusion criteria. Next, all the relevant citations were exported from each database into one Endnote library. The program was then used to exclude all the duplicates among these databases to prevent overlapping. The remaining citations were then exported into a standardized Excel sheet designed to fit these articles, based on their titles, authors, DOIs, URLs, and abstracts, to facilitate the screening process. Each step was conducted by at least two reviewers who independently reviewed each article to judge its relevance to the intended outcomes of this study. Finally, a public discussion resolved each disagreement under the supervision of the senior author, who was consulted whenever needed. Before excluding studies published in English or with no available full texts, members searched for relevant data regarding these articles and contacted their authors. Otherwise, these were excluded.
2.4. Data Extraction
This step was also conducted by at least two reviewers, similar to the previous step. The extraction sheet was designed by a senior author who conducted a pilot version of extracting relevant data from some included studies to check the suitability of the sheet before going through the extraction process. The sheet was mainly composed of three main parts: a part for baseline characteristics of included studies and their populations, another part for outcomes, and a third part that was particular to quality assessment. Extracted baseline characteristics included the first author’s last name and the year of publication as the reference for the included study, the study design, the data collection process, the sample size, and the age and gender of the included populations. On the other hand, the extracted outcomes include response time, on-scene time, transport time, and pre-hospital time for both rural and urban settings, as well as the significance of each variable and authors’ conclusions. The third part of the sheet included the domains of the quality assessment tools, which will be discussed in the following section.
2.5. Quality Assessment
This step was conducted alongside the extraction process, and the assessment process was similarly performed by the study members. For assessing the quality of included observational studies, the National Institutes of Health Quality Assessment Tool was used. In addition, the Cochrane Collaboration’s proposal to assess the risk of bias (RoB 2) for clinical trials was also used [25].
3. Results
3.1. Search Results
After performing the comprehensive database search, 2445 relevant citations were found since 1990. Endnote was used to remove all potential duplicates and managed to find and exclude 1657 duplicates among the different databases. After title/abstract screening of the remaining citations (n = 788), the full texts of relevant articles (n = 84) were also reviewed. Finally, 26 articles and another 11 relevant articles (obtained via manually searching references of relevant reviews and similar investigations) were included. These steps are summarized in the PRISMA flow chart in Figure 1.
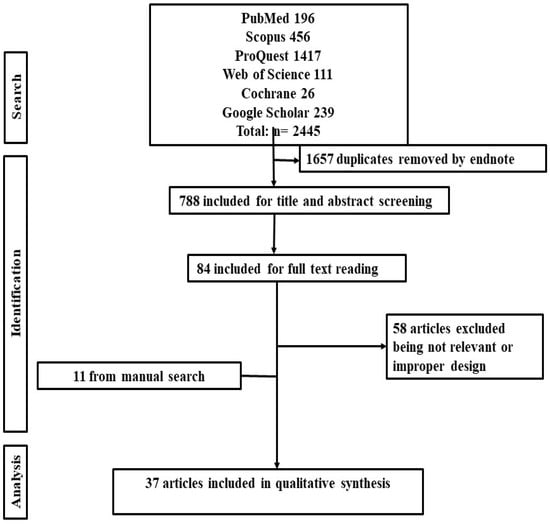
Figure 1.
PRISMA flow diagram showing the search strategy of the current systematic review.
3.2. Characteristics of Included Studies
In total, 37 articles were ultimately included in this review. These studies were published between 1991 and 2022. Most studies (n = 17, 45.95%) were conducted in the United States. In contrast, others were conducted in Finland (n = 3, 8.1%), Ireland (n = 3, 8.1%), Sweden (n = 2, 5.4%), the Kingdom of Saudi Arabia (n = 2, 5.4%), Qatar (n = 2, 5.4%), Poland, Denmark, Australia, Scotland, Norway, Taiwan, Iran, and Spain (n = 1, 2.7% each). In addition, the study design for almost all studies (n = 35, 94.6%) was observational, while only two (5.4%) were randomized clinical trials. Twenty-five studies (67.67%) depended on retrospective data collection, while the rest (n = 12, 32.4%) included patients prospectively. The sample size of included studies was also remarkably variable, being highest in the study by Byrne et al. [18] (n = 239,464,121) and lowest in that by Layon et al. [26] (n = 137). However, some studies did not report their total sample size. After assessing the quality of the included studies, nine studies scored 6, nine scored 8, ten scored 7, and six scored 9. Moreover, the assessment of bias in the two trials showed that they had a low risk of bias. These characteristics, together with other variables, are detailed in Table 1.

Table 1.
Baseline characteristics and quality assessment results of the included studies in this review.
3.3. Study Outcomes
Among the 37 studies in this review, 29 (78.4%) reported a difference in response time between rural and urban areas. Among these studies, the reported response times for their patients were remarkably variable. However, most of them (n = 27, 93.1%) indicate that response times are significantly longer in rural areas than in urban areas. On the other hand, only the study by Grossman et al. [30] showed that mean response time in rural areas is significantly shorter than that in urban areas (7 versus 13.6 min, p-value < 0.0001). Moreover, Stripe and Susman [46] reported that response times in both types of communities were similar (Table 2). Regarding transport time, 14 studies (37.8%) compared this outcome between rural and urban populations. All of these studies indicate the superiority of EMS in urban over rural communities. However, the reported mean transport times are also variable among these studies (Table 3). In another context, 10 studies (27%) reported on-scene time. Most of these studies (n = 8, 80%) reported that the mean on-scene time for their populations is significantly longer in rural areas than in urban areas. On the other hand, two studies (20%) reported that on-scene time is similar in urban and rural communities (Table 4). Finally, only eight studies (21.6%) reported pre-hospital time fo r rural and urban populations. All of these studies reported that pre-hospital time is significantly shorter in urban communities than in rural communities. The different pre-hospital time values of each study are detailed in Table 5.
Table 2.
Differences between rural and urban areas regarding response time.
Table 3.
Differences between rural and urban areas regarding transport time.
Table 4.
Differences between rural and urban areas regarding on-scene time.
Table 5.
Differences between rural and urban areas regarding pre-hospital time.
4. Discussion
The present systematic review provides cumulative evidence from the relevant studies in the literature regarding the differences between EMS in rural and urban communities in terms of response, transport, and on-scene time. The current findings indicate the superiority of EMS services within urban communities, as most studies indicate that response, transport, and on-scene times are significantly shorter for patients in these areas.
These findings are similar to the results of the previous systematic review by Alanazy et al. [50]. However, the current study provides more updated evidence by including more relevant recent investigations. Moreover, the meta-analysis by Carr et al. also demonstrated that ground urban EMS services are superior to ground rural EMS ones in terms of different pre-hospital time intervals. This indicates the superiority of EMS in urban settings over rural settings, indicating the need to enhance the quality of EMS in the latter settings. However, it should also be noted that the pre-hospital time intervals are remarkably variable among the different studies in the literature, indicating remarkable heterogeneity among these studies and the need for future relevant investigations.
Various factors can contribute to these differences. These include geographical distance (which is usually longer in rural settings); the number and type of available ambulances; the location, number, and preparedness of healthcare facilities; EMS workload, which could determine ambulance queue and the efficiency of the dispatch centre in dispatching ambulances; and transport infrastructure [29,33,51]. These factors can significantly impact response time. Therefore, attempts should be made to enhance the response process. This can be achieved by enhancing the aforementioned factors in rural areas to bring them to a standardized level similar to that of urban areas and improving the quality of EMS by providing well-trained personnel and well-equipped ambulances, according to previous investigations [49,52,53].
However, it should be noted that a position paper in 2003 by the National Association of EMS Physicians recommended that transport and response time intervals have regional variations [54]. Therefore, no specific standards can be applied to adjust these intervals, and they should be determined locally. This encourages conducting further studies per country to help healthcare officials enhance their interventions. In this context, a previous study indicated that using firefighters as medical first responders enhances pre-hospital time and patient outcomes in Sweden [55]. Moreover, in South Korea, the National Ambulance Service suggested that EMS for specific events (like cardiac arrest) might be conducted by moderate care ambulances and non-front-line officers to reduce response time, as such events might not require high levels of training and management resources, which might save time in those situations [56]. Moreover, an RCT by Pappinen et al. [42] compared response times for community first-response models with 1–3 responders and the fire department model. The authors reported that community first-response models might have reduced pre-hospital time compared to the fire department model when emergency vehicles are not used in these events. However, the authors demonstrated that these favourable events are insignificant in rural communities.
In addition, it might be controversial among some studies whether the reduced pre-hospital time is beneficial for patients with traumatic injuries. For instance, the degree of stabilizing traumatized patients in pre-hospital settings is debatable and might impact the outcomes. Accordingly, this might impact on-scene time. Only Grossman et al. [30] reported that rural patients had a shorter mean transport time than urban patients with major traumas. However, establishing a comparison between these patients and other patients with other presenting aetiologies is difficult because of the lack of adequate data in the current literature. It should be noted that the manual by the American College of Surgeons Advanced Trauma Life Support supports reducing on-scene time and rapidly transporting patients to trauma centres [57]. In this context, different relevant studies indicated that these approaches could significantly enhance patients’ outcomes [30,58,59,60,61].
Many studies in the literature indicated socio-spatial disparities in having access to EMS in rural and urban settings [50,62,63,64,65,66,67]. These studies also highlighted the impact of these disparities on patients’ outcomes and mortality rates following various events, like cardiac arrest, stroke, and trauma, and the results favour patients within urban communities [50,68,69]. However, socioeconomic and demographic disparities were also significant variables affecting these outcomes. For instance, previous studies showed that populations with limited resources and foreign individuals usually have limited access to specialized trauma centres [70,71]. In this context, residential discrimination might limit healthcare accessibility to certain ethnic groups and minorities more than others [71,72,73,74]. In addition, reduced levels of accessibility might also be associated with old age, not having medical insurance, and low income levels [64,71,72,75,76].
Although this study included many relevant investigations, there are limitations affecting the interpretation of the current results. The main limitation would be the absence of adjustment of variables that might affect EMS regardless of the geography or distribution of patients. These factors mainly include the probability of patients to seek EMS, such as calling the ambulance, and defining personnel involved in delivering EMS, which might significantly impact the outcomes. For instance, evidence shows that having limited knowledge about whether some symptoms are indicative of a need to call an ambulance or not might hinder EMS. In addition, the probability of calling an ambulance might also be impacted by the patient’s perception of the healthcare system, having social support, self-reported quality of life, and anxiety or loneliness. Another limitation to this study is that we did not investigate the impact of EMS on patients’ outcomes, which is a significant domain that might determine the quality of EMS. Therefore, we encourage future investigations to consider this limitation.
Finally, although studies from different countries were included, evidence from these countries still needs further support by additional investigations to elaborate on the factors that might affect EMS-related patients’ outcomes in rural settings. Furthermore, the absence of adjustment of variables and other co-founders might affect EMS regardless of the geography or distribution of patients. These factors mainly include the probability of patients to seek EMS, such as calling an ambulance, and defining personnel involved in delivering EMS, which might impact outcomes. In addition, evidence from low-to-middle income countries is still lacking; therefore, future investigations from these countries are encouraged to provide more insight regarding their EMS.
5. Conclusions
The present systematic review provides cumulative global evidence about the differences in the quality of EMS in rural and urban communities in terms of pre-hospital time intervals. Despite many recently published studies comparing the differences in pre-hospital time intervals between rural and urban communities, the current findings indicate the superiority of urban EMS over rural services, as affected patients in these areas usually have lower response, on-scene, and transport times. This, according to previous studies, is usually associated with better outcomes and favourable prognoses. However, it should be noted that it is difficult in the current study to determine a standardized pre-hospital time interval because of the huge variations among the included global studies. Therefore, future studies are needed to investigate the current limitations and enhance the quality of EMS, particularly for patients living in rural communities.
Author Contributions
Conceptualization, A.A. and A.R.M.A.; methodology, A.A.; software, A.A.; validation, A.A. and A.R.M.A.; formal analysis, A.A. and A.R.M.A.; investigation, A.A. and A.R.M.A.; resources, A.A. and A.R.M.A.; data curation, A.A. and A.R.M.A.; writing—original draft preparation, A.A.; writing—review and editing, A.A. and A.R.M.A.; visualization, A.A. and A.R.M.A.; supervision, A.A. and A.R.M.A.; project administration, A.A. and A.R.M.A. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Conflicts of Interest
The authors declare no conflict of interest.
References
- AlShammari, T.; Jennings, P.; Williams, B. Evolution of emergency medical services in Saudi Arabia. J. Emerg. Med. Trauma Acute Care 2017, 2017, 4. [Google Scholar] [CrossRef]
- Jennings, P.; Cameron, P.; Walker, T.; Bernard, S.; Smith, K. Out-of-Hospital Cardiac Arrest in Victoria: Rural and Urban Outcomes. Med. J. Aust. 2006, 185, 135–139. [Google Scholar] [CrossRef] [PubMed]
- Harmsen, A.; Giannakopoulos, G.; Moerbeek, P.; Jansma, E.; Bonjer, H.; Bloemers, F. The Influence of Prehospital Time on Trauma Patients Outcome: A Systematic Review. Injury 2015, 46, 602–609. [Google Scholar] [CrossRef] [PubMed]
- Mehmood, A.; Rowther, A.A.; Kobusingye, O.; Hyder, A.A. Assessment of Pre-Hospital Emergency Medical Services in Low-Income Settings Using a Health Systems Approach. Int. J. Emerg. Med. 2018, 11, 53. [Google Scholar] [CrossRef]
- Lin, C.B.; Peterson, E.D.; Smith, E.E.; Saver, J.L.; Liang, L.; Xian, Y.; Olson, D.M.; Shah, B.R.; Hernandez, A.F.; Schwamm, L.H.; et al. Emergency Medical Service Hospital Prenotification Is Associated with Improved Evaluation and Treatment of Acute Ischemic Stroke. Circ. Cardiovasc. Qual. Outcomes 2012, 5, 514–522. [Google Scholar] [CrossRef]
- Rogers, F.B.; Rittenhouse, K.J.; Gross, B.W. The Golden Hour in Trauma: Dogma or Medical Folklore? Injury 2015, 46, 525–527. [Google Scholar] [CrossRef]
- Hassler, J.; Ceccato, V. Socio-Spatial Disparities in Access to Emergency Health Care-a Scandinavian Case Study. PLoS ONE 2021, 16, e0261319. [Google Scholar] [CrossRef]
- Cabral, E.L.; Castro, W.R.; Florentino, D.R.; Viana, D.D.; Costa Junior, J.F.; Souza, R.P.; Rêgo, A.C.; Araújo-Filho, I.; Medeiros, A.C. Response Time in the Emergency Services. Systematic Review. Acta Cir. Bras. 2018, 33, 1110–1121. [Google Scholar] [CrossRef]
- Kironji, A.G.; Hodkinson, P.; De Ramirez, S.S.; Anest, T.; Wallis, L.; Razzak, J.; Jenson, A.; Hansoti, B. Identifying Barriers for out of Hospital Emergency Care in Low and Low-Middle Income Countries: A Systematic Review. BMC Health Serv. Res. 2018, 18, 291. [Google Scholar] [CrossRef]
- Haghparast-Bidgoli, H.; Hasselberg, M.; Khankeh, H.; Khorasani-Zavareh, D.; Johansson, E. Barriers and Facilitators to Provide Effective Pre-Hospital Trauma Care for Road Traffic Injury Victims in Iran: A Grounded Theory Approach. BMC Emerg. Med. 2010, 10, 20. [Google Scholar] [CrossRef]
- Fatovich, D.M.; Phillips, M.; Langford, S.A.; Jacobs, I.G. A Comparison of Metropolitan vs Rural Major Trauma in Western Australia. Resuscitation 2011, 82, 886–890. [Google Scholar] [CrossRef] [PubMed]
- Adeyemi, O.J.; Paul, R.; Arif, A. An Assessment of the Rural-Urban Differences in the Crash Response Time and County-Level Crash Fatalities in the United States. J. Rural Health 2021, 4, 999–1010. [Google Scholar] [CrossRef] [PubMed]
- Gonzalez, R.P.; Cummings, G.R.; Phelan, H.A.; Mulekar, M.S.; Rodning, C.B. Does Increased Emergency Medical Services Prehospital Time Affect Patient Mortality in Rural Motor Vehicle Crashes? A Statewide Analysis. Am. J. Surg. 2009, 197, 30–34. [Google Scholar] [CrossRef] [PubMed]
- Hashtarkhani, S.; Kiani, B.; Mohammadi, A.; MohammadEbrahimi, S.; Dehghan-Tezerjani, M.; Samimi, T.; Tara, M.; Matthews, S.A. Spatio-Temporal Epidemiology of Emergency Medical Requests in a Large Urban Area. A Scan-Statistic Approach. Geospat. Health 2021, 16. [Google Scholar] [CrossRef] [PubMed]
- Aftyka, A.; Rybojad, B.; Rudnicka-Drozak, E. Are There Any Differences in Medical Emergency Team Interventions between Rural and Urban Areas? A Single-Centre Cohort Study. Aust. J. Rural Health 2014, 22, 223–228. [Google Scholar] [CrossRef]
- Alanazy, A.R.; Wark, S.; Fraser, J.; Nagle, A. A Comparison of Pre-Hospital Emergency Medical Services’ Response and Duration Times in Urban Versus Rural Areas of Saudi Arabia. Australas. J. Paramed. 2020, 17. [Google Scholar] [CrossRef]
- Al-Thani, H.; Mekkodathil, A.; Hertelendy, A.J.; Howland, I.; Frazier, T.; El-Menyar, A. Emergency Medical Services (Ems) Transportation of Trauma Patients by Geographic Locations and in-Hospital Outcomes: Experience from Qatar. Int. J. Environ. Res. Public Health 2021, 18, 4016. [Google Scholar] [CrossRef] [PubMed]
- Byrne, J.P.; Mann, N.C.; Dai, M.; Mason, S.A.; Karanicolas, P.; Rizoli, S.; Nathens, A.B. Association between Emergency Medical Service Response Time and Motor Vehicle Crash Mortality in the United States. JAMA Surg. 2019, 154, 286–293. [Google Scholar] [CrossRef] [PubMed]
- Waalwijk, J.F.; van der Sluijs, R.; Lokerman, R.D.; Fiddelers, A.A.A.; Hietbrink, F.; Leenen, L.P.H.; Poeze, M.; van Heijl, M. The Impact of Prehospital Time Intervals on Mortality in Moderately and Severely Injured Patients. J. Trauma Acute Care Surg. 2022, 92, 520–527. [Google Scholar] [CrossRef]
- Mathiesen, W.T.; Bjørshol, C.A.; Kvaløy, J.T.; Søreide, E. Effects of Modifiable Prehospital Factors on Survival after out-of-Hospital Cardiac Arrest in Rural Versus Urban Areas. Crit. Care 2018, 22, 99. [Google Scholar] [CrossRef]
- Cui, E.R.; Beja-Glasser, A.; Fernandez, A.R.; Grover, J.M.; Mann, N.C.; Patel, M.D. Emergency Medical Services Time Intervals for Acute Chest Pain in the United States, 2015–2016. Prehosp. Emerg. Care 2020, 24, 557–565. [Google Scholar] [CrossRef] [PubMed]
- Cui, E.R.; Fernandez, A.R.; Zegre-Hemsey, J.K.; Grover, J.M.; Honvoh, G.; Brice, J.H.; Rossi, J.S.; Patel, M.D. Disparities in Emergency Medical Services Time Intervals for Patients with Suspected Acute Coronary Syndrome: Findings from the North Carolina Prehospital Medical Information System. J. Am. Heart Assoc. 2021, 10, e019305. [Google Scholar] [CrossRef] [PubMed]
- Hsu, Y.C.; Wu, W.T.; Huang, J.B.; Lee, K.H.; Cheng, F.J. Association between Prehospital Prognostic Factors and out-of-Hospital Cardiac Arrest: Effect of Rural-Urban Disparities. Am. J. Emerg Med. 2021, 46, 456–461. [Google Scholar] [CrossRef] [PubMed]
- Carr, B.G.; Caplan, J.M.; Pryor, J.P.; Branas, C.C. A Meta-Analysis of Prehospital Care Times for Trauma. Prehosp. Emerg. Care 2006, 10, 198–206. [Google Scholar] [CrossRef]
- Higgins, J.P.; Altman, D.G.; Gøtzsche, P.C.; Jüni, P.; Moher, D.; Oxman, A.D.; Savović, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A. The Cochrane Collaboration’s Tool for Assessing Risk of Bias in Randomised Trials. BMJ 2011, 343, d5928. [Google Scholar] [CrossRef]
- Layon, A.J.; Gabrielli, A.; Goldfeder, B.W.; Hevia, A.; Idris, A.H. Utstein Style Analysis of Rural out-of-Hospital Cardiac Arrest [Oohca]: Total Cardiopulmonary Resuscitation (Cpr) Time Inversely Correlates with Hospital Discharge Rate. Resuscitation 2003, 56, 59–66. [Google Scholar] [CrossRef]
- Ashburn, N.P.; Snavely, A.C.; Angi, R.M.; Scheidler, J.F.; Crowe, R.P.; McGinnis, H.D.; Hiestand, B.C.; Miller, C.D.; Mahler, S.A.; Stopyra, J.P. Prehospital Time for Patients with Acute Cardiac Complaints: A Rural Health Disparity. Am. J. Emerg. Med. 2022, 52, 64–68. [Google Scholar] [CrossRef]
- Breen, N.; Woods, J.; Bury, G.; Murphy, A.W.; Brazier, H. A National Census of Ambulance Response Times to Emergency Calls in Ireland. J. Accid. Emerg. Med. 2000, 17, 392–395. [Google Scholar] [CrossRef]
- Gonzalez, R.P.; Cummings, G.; Mulekar, M.; Rodning, C.B. Increased Mortality in Rural Vehicular Trauma: Identifying Contributing Factors through Data Linkage. J. Trauma 2006, 61, 404–409. [Google Scholar] [CrossRef]
- Grossman, D.C.; Kim, A.; Macdonald, S.C.; Klein, P.; Copass, M.K.; Maier, R.V. Urban-Rural Differences in Prehospital Care of Major Trauma. J. Trauma 1997, 42, 723–729. [Google Scholar] [CrossRef]
- Horeczko, T.; Marcin, J.P.; Kahn, J.M.; Sapien, R.E. Urban and Rural Patterns in Emergent Pediatric Transfer: A Call for Regionalization. J. Rural Health 2014, 30, 252–258. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.; Abdel-Aty, M.; Cai, Q.; Wang, L. Effects of Emergency Medical Services Times on Traffic Injury Severity: A Random Effects Ordered Probit Approach. Traffic Inj. Prev. 2018, 19, 577–581. [Google Scholar] [CrossRef]
- Masterson, S.; Wright, P.; O’Donnell, C.; Vellinga, A.; Murphy, A.W.; Hennelly, D.; Sinnott, B.; Egan, J.; O’Reilly, M.; Keaney, J.; et al. Urban and Rural Differences in out-of-Hospital Cardiac Arrest in Ireland. Resuscitation 2015, 91, 42–47. [Google Scholar] [CrossRef] [PubMed]
- McGuffie, A.C.; Graham, C.A.; Beard, D.; Henry, J.M.; Fitzpatrick, M.O.; Wilkie, S.C.; Kerr, G.W.; Parke, T.R. Scottish Urban Versus Rural Trauma Outcome Study. J. Trauma 2005, 59, 632–638. [Google Scholar] [PubMed]
- Mell, H.K.; Mumma, S.N.; Hiestand, B.; Carr, B.G.; Holland, T.; Stopyra, J. Emergency Medical Services Response Times in Rural, Suburban, and Urban Areas. JAMA Surg. 2017, 152, 983–984. [Google Scholar] [CrossRef]
- Jones, M.D.; Paulus, J.A.; Jacobs, J.V.; Bogert, J.N.; Chapple, K.M.; Soe-Lin, H.; Weinberg, J.A. Trauma Patient Transport Times Unchanged Despite Trauma Center Proliferation: A 10-Year Review. J. Trauma Acute Care Surg. 2021, 90, 421–425. [Google Scholar] [CrossRef] [PubMed]
- Moafa, H.N.; van Kuijk, S.M.J.; Alqahtani, D.M.; Moukhyer, M.E.; Haak, H.R. Disparities between Rural and Urban Areas of the Central Region of Saudi Arabia in the Utilization and Time-Centeredness of Emergency Medical Services. Int. J. Environ. Res. Public Health 2020, 17, 7944. [Google Scholar] [CrossRef]
- Moore, M.J.; Hamilton, A.J.; Cairns, K.J.; Marshall, A.; Glover, B.M.; McCann, C.J.; Jordan, J.; Kee, F.; Adgey, A.A. The Northern Ireland Public Access Defibrillation (Nipad) Study: Effectiveness in Urban and Rural Populations. Heart 2008, 94, 1614–1619. [Google Scholar] [CrossRef][Green Version]
- Morales-Gabardino, J.A.; Redondo-Lobato, L.; Ribeiro, J.M.; Buitrago, F. Geographical Distribution of Emergency Services Times in Traffic Accidents in Extremadura. Port. J. Public Health 2021, 39, 78–87. [Google Scholar] [CrossRef]
- Newgard, C.D.; Fu, R.; Bulger, E.; Hedges, J.R.; Mann, N.C.; Wright, D.A.; Lehrfeld, D.P.; Shields, C.; Hoskins, G.; Warden, C.; et al. Evaluation of Rural vs Urban Trauma Patients Served by 9-1-1 Emergency Medical Services. JAMA Surg. 2017, 152, 11–18. [Google Scholar] [CrossRef]
- Nordberg, P.; Jonsson, M.; Forsberg, S.; Ringh, M.; Fredman, D.; Riva, G.; Hasselqvist-Ax, I.; Hollenberg, J. The Survival Benefit of Dual Dispatch of Ems and Fire-Fighters in out-of-Hospital Cardiac Arrest May Differ Depending on Population Density--a Prospective Cohort Study. Resuscitation 2015, 90, 143–149. [Google Scholar] [CrossRef] [PubMed]
- Pappinen, J.; Olkinuora, A.; Laukkanen-Nevala, P. Medical First Response Models in Rural Villages and Towns: A Simulation Study of Response Times. Australas. J. Paramed. 2021, 18. [Google Scholar] [CrossRef]
- Peters, G.A.; Ordoobadi, A.J.; Panchal, A.R.; Cash, R.E. Differences in out-of-Hospital Cardiac Arrest Management and Outcomes across Urban, Suburban, and Rural Settings. Prehosp. Emerg. Care 2021, 2021, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Raatiniemi, L.; Liisanantti, J.; Niemi, S.; Nal, H.; Ohtonen, P.; Antikainen, H.; Martikainen, M.; Alahuhta, S. Short-Term Outcome and Differences between Rural and Urban Trauma Patients Treated by Mobile Intensive Care Units in Northern Finland: A Retrospective Analysis. Scand. J. Trauma Resusc. Emerg. Med. 2015, 23, 91. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Sørensen, J.T.; Terkelsen, C.J.; Nørgaard, B.L.; Trautner, S.; Hansen, T.M.; Bøtker, H.E.; Lassen, J.F.; Andersen, H.R. Urban and Rural Implementation of Pre-Hospital Diagnosis and Direct Referral for Primary Percutaneous Coronary Intervention in Patients with Acute St-Elevation Myocardial Infarction. Eur. Heart J. 2011, 32, 430–436. [Google Scholar] [CrossRef] [PubMed]
- Stripe, S.C.; Susman, J. A Rural-Urban Comparison of Prehospital Emergency Medical Services in Nebraska. J. Am. Board Fam. Pract. 1991, 4, 313–318. [Google Scholar] [PubMed]
- Varjoranta, T.; Raatiniemi, L.; Majamaa, K.; Martikainen, M.; Liisanantti, J.H. Prehospital and Hospital Delays for Stroke Patients Treated with Thrombolysis: A Retrospective Study from Mixed Rural-Urban Area in Northern Finland. Australas. Emerg. Care 2019, 22, 76–80. [Google Scholar] [CrossRef]
- Vukmir, R.B. The Influence of Urban, Suburban, or Rural Locale on Survival from Refractory Prehospital Cardiac Arrest. Am. J. Emerg. Med. 2004, 22, 90–93. [Google Scholar] [CrossRef]
- Wilson, P.; Alinier, G.; Reimann, T.; Morris, B. Influential Factors on Urban and Rural Response Times for Emergency Ambulances in Qatar. Mediterr. J. Emerg. Med. 2018, 26, 8–13. [Google Scholar]
- Alanazy, A.R.M.; Wark, S.; Fraser, J.; Nagle, A. Factors Impacting Patient Outcomes Associated with Use of Emergency Medical Services Operating in Urban Versus Rural Areas: A Systematic Review. Int. J. Environ. Res. Public Health 2019, 16, 1728. [Google Scholar] [CrossRef]
- Razzak, J.A.; Kellermann, A.L. Emergency Medical Care in Developing Countries: Is It Worthwhile? Bull. World Health Organ. 2002, 80, 900–905. [Google Scholar] [PubMed]
- Gale, J.; Coburn, A.; Pearson, K.; Croll, Z.; Shaler, G. Developing Program Performance Measures for Rural Emergency Medical Services. Prehosp. Emerg. Care 2017, 21, 157–165. [Google Scholar] [CrossRef] [PubMed]
- Pennel, C.L.; Tamayo, L.; Wells, R.; Sunbury, T. Emergency Medical Service-Based Care Coordination for Three Rural Communities. J. Health Care Poor Underserved 2016, 27, 159–180. [Google Scholar] [CrossRef] [PubMed]
- Bailey, E.D.; Sweeney, T. Considerations in Establishing Emergency Medical Services Response Time Goals. Prehosp. Emerg. Care 2003, 7, 397–399. [Google Scholar] [CrossRef] [PubMed]
- Svensson, A.; Elmqvist, C.; Fridlund, B.; Rask, M.; Andersson, R.; Stening, K. Using Firefighters as Medical First Responders to Shorten Response Time in Rural Areas in Sweden. Aust. J. Rural Health 2020, 28, 6–14. [Google Scholar] [CrossRef]
- Ro, Y.S.; Shin, S.D.; Song, K.J.; Lee, E.J.; Kim, J.Y.; Ahn, K.O.; Chung, S.P.; Kim, Y.T.; Hong, S.O.; Choi, J.A.; et al. A Trend in Epidemiology and Outcomes of out-of-Hospital Cardiac Arrest by Urbanization Level: A Nationwide Observational Study from 2006 to 2010 in South Korea. Resuscitation 2013, 84, 547–557. [Google Scholar] [CrossRef]
- Subcommittee, A.T.; International ATLS Working Group. Advanced Trauma Life Support (Atls®): The Ninth Edition. J. Trauma Acute Care Surg. 2013, 74, 1363–1366. [Google Scholar]
- Liberman, M.; CBranas, C.H.; Mulder, D.S.; Lavoie, A.; Sampalis, J.S. Advanced Versus Basic Life Support in the Pre-Hospital Setting—the Controversy between the ‘Scoop and Run’ and the ‘Stay and Play’ Approach to the Care of the Injured Patient. Int. J. Disaster Med. 2004, 2, 9–17. [Google Scholar] [CrossRef]
- Gervin, A.S.; Fischer, R.P. The Importance of Prompt Transport of Salvage of Patients with Penetrating Heart Wounds. J. Trauma 1982, 22, 443–448. [Google Scholar] [CrossRef]
- Esposito, T.J.; Maier, R.V.; Rivara, F.P.; Pilcher, S.; Griffith, J.; Lazear, S.; Hogan, S. The Impact of Variation in Trauma Care Times: Urban Versus Rural. Prehosp. Disaster Med. 1995, 10, 161–166; discussion 66-7. [Google Scholar] [CrossRef]
- Sampalis, J.S.; Lavoie, A.; Williams, J.I.; Mulder, D.S.; Kalina, M. Impact of on-Site Care, Prehospital Time, and Level of in-Hospital Care on Survival in Severely Injured Patients. J. Trauma 1993, 34, 252–261. [Google Scholar] [CrossRef] [PubMed]
- Yasunaga, H.; Miyata, H.; Horiguchi, H.; Tanabe, S.; Akahane, M.; Ogawa, T.; Koike, S.; Imamura, T. Population Density, Call-Response Interval, and Survival of out-of-Hospital Cardiac Arrest. Int. J. Health Geogr. 2011, 10, 26. [Google Scholar] [CrossRef] [PubMed]
- Lyon, R.M.; Cobbe, S.M.; Bradley, J.M.; Grubb, N.R. Surviving out of Hospital Cardiac Arrest at Home: A Postcode Lottery? Emerg. Med. J. 2004, 21, 619–624. [Google Scholar] [CrossRef]
- Lilley, R.; de Graaf, B.; Kool, B.; Davie, G.; Reid, P.; Dicker, B.; Civil, I.; Ameratunga, S.; Branas, C. Geographical and Population Disparities in Timely Access to Prehospital and Advanced Level Emergency Care in New Zealand: A Cross-Sectional Study. BMJ Open 2019, 9, e026026. [Google Scholar] [CrossRef]
- Hameed, S.M.; Schuurman, N.; Razek, T.; Boone, D.; van Heest, R.; Taulu, T.; Lakha, N.; Evans, D.C.; Brown, D.R.; Kirkpatrick, A.W.; et al. Access to Trauma Systems in Canada. J. Trauma 2010, 69, 1350–1361; discussion 61. [Google Scholar] [CrossRef] [PubMed]
- Emerson, P.; Dodds, N.; Green, D.R.; Jansen, J.O. Geographical Access to Critical Care Services in Scotland. J. Intensive Care Soc. 2018, 19, 6–14. [Google Scholar] [CrossRef]
- Goto, Y.; Funada, A.; Goto, Y. Relationship between Emergency Medical Services Response Time and Bystander Intervention in Patients with out-of-Hospital Cardiac Arrest. J. Am. Heart Assoc. 2018, 7, e007568. [Google Scholar] [CrossRef]
- Georgakakos, P.K.; Swanson, M.B.; Ahmed, A.; Mohr, N.M. Rural Stroke Patients Have Higher Mortality: An Improvement Opportunity for Rural Emergency Medical Services Systems. J. Rural Health 2022, 38, 217–227. [Google Scholar] [CrossRef]
- Gomez, D.; Berube, M.; Xiong, W.; Ahmed, N.; Haas, B.; Schuurman, N.; Nathens, A.B. Identifying Targets for Potential Interventions to Reduce Rural Trauma Deaths: A Population-Based Analysis. J. Trauma 2010, 69, 633–639. [Google Scholar] [CrossRef]
- do Nascimento Silva, K.S.; Padeiro, M. Assessing Inequalities in Geographical Access to Emergency Medical Services in Metropolitan Lisbon: A Cross-Sectional and Ecological Study. BMJ Open 2020, 10, e033777. [Google Scholar] [CrossRef]
- Hsia, R.; Shen, Y.C. Possible Geographical Barriers to Trauma Center Access for Vulnerable Patients in the United States: An Analysis of Urban and Rural Communities. Arch. Surg. 2011, 146, 46–52. [Google Scholar] [CrossRef] [PubMed]
- Kleindorfer, D.O.; Lindsell, C.J.; Broderick, J.P.; Flaherty, M.L.; Woo, D.; Ewing, I.; Schmit, P.; Moomaw, C.; Alwell, K.; Pancioli, A.; et al. Community Socioeconomic Status and Prehospital Times in Acute Stroke and Transient Ischemic Attack: Do Poorer Patients Have Longer Delays from 911 Call to the Emergency Department? Stroke 2006, 37, 1508–1513. [Google Scholar] [CrossRef] [PubMed]
- Bissonnette, L.; Wilson, K.; Bell, S.; Shah, T.I. Neighbourhoods and Potential Access to Health Care: The Role of Spatial and Aspatial Factors. Health Place 2012, 18, 841–853. [Google Scholar] [CrossRef] [PubMed]
- White, K.; Haas, J.S.; Williams, D.R. Elucidating the Role of Place in Health Care Disparities: The Example of Racial/Ethnic Residential Segregation. Health Serv. Res. 2012, 47 Pt 2, 1278–1299. [Google Scholar] [CrossRef] [PubMed]
- Carr, B.G.; Bowman, A.J.; Wolff, C.S.; Mullen, M.T.; Holena, D.N.; Branas, C.C.; Wiebe, D.J. Disparities in Access to Trauma Care in the United States: A Population-Based Analysis. Injury 2017, 48, 332–338. [Google Scholar] [CrossRef] [PubMed]
- Hsia, R.Y.; Huang, D.; Mann, N.C.; Colwell, C.; Mercer, M.P.; Dai, M.; Niedzwiecki, M.J. A Us National Study of the Association between Income and Ambulance Response Time in Cardiac Arrest. JAMA Netw. Open 2018, 1, e185202. [Google Scholar] [CrossRef]
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).