
Validation of the WHOQOL-BREF Quality of Life Questionnaire in an Urban Sample of Older Adults in a Neighbourhood in Zaragoza (Spain)

 , , ,
, , ,
Abstract
1. Introduction
WHOQOL-BREF Definition and Dimensions
2. Method
2.1. Subjects and Procedures
2.2. Instrument
2.3. Description of Data and Statistical Analysis
3. Results
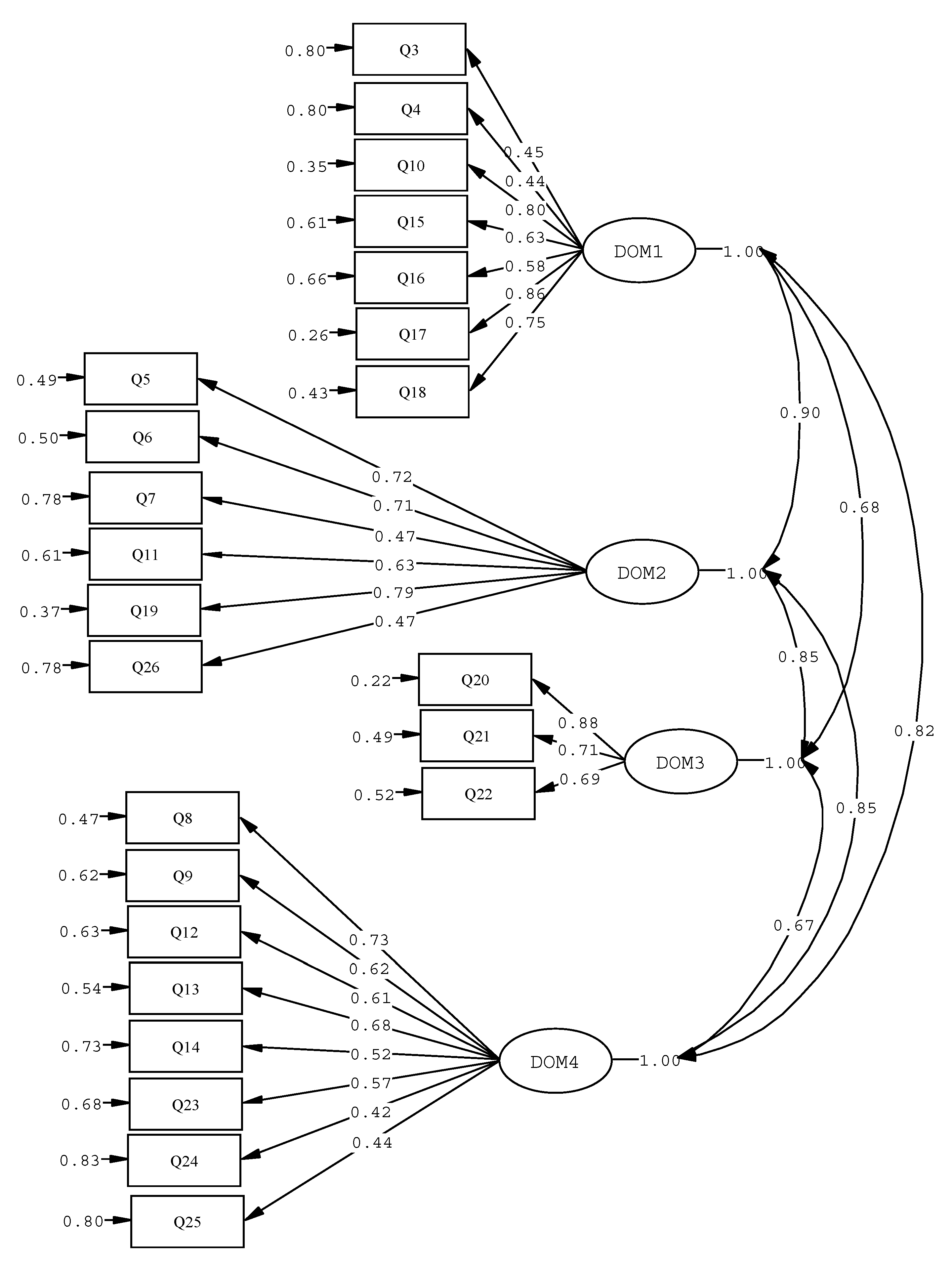
3.1. Factorial Structure
3.2. Internal Consistency
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization. World Report on Ageing and Health. 2015. Available online: https://apps.who.int/iris/handle/10665/186463186463 (accessed on 25 October 2022).
- Spanish National Institute of Statistics. Proyecciones de población. In Notas de Prensa; Spanish National Institute of Statistics: Madrid, Spain, 2016; pp. 1–20. [Google Scholar]
- Spanish General Directorate of Employment, Social Affairs and Inclusion. La Aportación de la Unión Europea al Envejecimiento Activo y a la Solidaridad entre Generaciones; Oficina de Publicaciones de la Unión Europea: Luxemburg, 2012. [Google Scholar]
- Jürschik, P.; Escobar, M.A.; Nuin, C.; Botigué, T. Criterios de fragilidad del adulto mayor. Estudio piloto. Aten Primaria 2011, 43, 190–196. [Google Scholar] [CrossRef] [PubMed]
- Salvador-Carulla, L.; Lucas-Carrasco, R.; Ayuso-Mateos, J.L.; Miret, M. Use of terms “Wellbeing” and “Quality of Life” in health sciences: A conceptual framework. Eur. J. Psychiatry 2014, 28, 50–65. [Google Scholar] [CrossRef]
- Norsted, I. Horizon 2020: European perspectives in healthcare sciences and implementation. EPMA J. 2014, 5, A1. [Google Scholar] [CrossRef] [PubMed]
- Wong, R.; Espinoza, I.; Palloni, A. Adultos mayores mexicanos en un contexto socioeconómico amplio: Salud y envejecimiento. Salud Pública Méx. 2010, 49, 436–447. [Google Scholar]
- Urzúa, A.; Bravo, M.; Ogalde, M.; Vargas, C. Factores vinculados a la calidad de vida en la adultez mayor. Rev. Med. Chile 2011, 139, 1006–1014. [Google Scholar] [CrossRef]
- Urzúa, A.; Navarrete, M. Calidad de vida en adultos mayores: Análisis factoriales de las versiones abreviadas del WHOQOL-OLD en población chilena. Rev. Med. Chile 2013, 141, 28–33. [Google Scholar] [CrossRef]
- WHOQOL Group. The World Health Organization Quality of Life Assessment. Soc. Sci. Med. 1995, 41, 1403–1409. [Google Scholar] [CrossRef]
- Vilar, M.; Simoes, M.R.; Lima, M.P.; Cruz, C.; Sousa, L.B.; Sousa, A.R.; Pires, L. Adaptation and validation of the WHOQOL-OLD for the Portuguese Population: Results of focus groups implementation. Rev. Iberoam. Diagn. Eval.-E Aval. Psicol. 2014, 37, 73–97. [Google Scholar]
- Power, M.; Bullinger, M.; Harper, A.; The WHOQOL Group. The World Health Organization WHOQOL-100: Test s of the universality of quality of life in 15 different cultural groups worldwide. Health Psychol. 1999, 18, 495–505. [Google Scholar] [CrossRef]
- Skevington, S.M.; Lofty, M.; O’Connell, K.A. The World Health Organization’s WHOQOL-BREF quality of life assessment. Psychometric properties and results of the international field trial. A Report from the WHOQOL Group. Qual. Life Res. 2004, 13, 299–310. [Google Scholar] [CrossRef]
- WHOQOL Group. Development of the World Health Organization WHOQOL-BREF quality of life assessment. Psychol. Med. 1998, 28, 551–558. [Google Scholar] [CrossRef] [PubMed]
- Hei-Fen, H.; Wen-Miin, L.; Yun-Ning, C.; Mau-Roung, L. Suitability of the WHOQOL-BREF for community-dwelling older people in Taiwan. Age Ageing 2003, 32, 593–600. [Google Scholar]
- Chachamovich, E.; Trentini, C.; Fleck, M.P. Assessment of the psychometric performance of the WHOQOL-Bref instrument in a sample of Brazilian older adults. Int. Psychogeriatr. 2006, 19, 635–646. [Google Scholar] [CrossRef] [PubMed]
- Von Steinbuchel, N.; Lischetzke, T.; Gurny, M.; Eid, M. Assessing quality of life in older people: Psychometric propierties of the WHOQOL-BREF. Eur. J. Ageing 2006, 2, 116–122. [Google Scholar] [CrossRef] [PubMed]
- Benítez, S.; Mancho, N.; Farrás-Permanyer, L.; Urzua-Morales, A.; Guardia-Olmos, J. Differential ítem functioning of WHOQOL-BREF in nine Iberoamerican Countries. Rev. Iberoam. Psicol. Salud 2016, 7, 51–59. [Google Scholar] [CrossRef]
- López, J.A.; González, R.A.; Tejada, J.M. Psychometric properties of a Spanish versión of quality of life scale WHOQOL-BREF in a Mexican Adult Sample. Rev. Iberoam. Diagn. Eval.-E Aval. Psicol. 2017, 44, 105–115. [Google Scholar]
- Chang, Y.C.; Yao, G.; Hu, S.C.; Wang, J.D. Depression affects the scores of all facets of the WHOQOL-BREF and may mediate the effects of the physical disability among community-dewlling older adults. PLoS ONE 2015, 10, e0128356. [Google Scholar] [CrossRef]
- Klis, S.; Ranchor, A.; Phillips, R.O.; Abass, K.M.; Tuah, W.; Loth, S.; Velding, K.; van der Werf, T.S.; Stienstra, Y. Good quality of life in former Buruli ulcer with small lesions: Long-Term follow-up of the BURULICO Trial. PLoS Negl. Trop. Dis. 2014, 8, e2964. [Google Scholar] [CrossRef]
- Wham, C.A.; Mclean, C.; Teh, R.; Moyes, S.; Peri, K.; Kerse, N. The bright trial: What are the factors associated with nutrition risk? J. Nutr. Health Aging 2014, 18, 692–697. [Google Scholar] [CrossRef]
- Vagetti, G.C.; Barbosa, V.C.; Moreira, N.B.; de Oliveira, V.D.; Mazzardo, O.; de Campos, W. The association between physical activity and quality of life domains among older women. J. Aging Phys. Act. 2015, 23, 524–533. [Google Scholar] [CrossRef]
- Vitorino, L.M.; Lucchetti, G.; Santos, A.E.O.; Lucchetti, A.L.G.; Ferreira, E.B.; Adame, N.P.; Vianna, L.A.C. Spiritual religious coping is associated with quality of life in institutionalized older adults. J. Relig. Health 2016, 55, 549–559. [Google Scholar] [CrossRef] [PubMed]
- Gobbens, R.J.J.; Van Assen, M.A.L.M. The prediction of quality of life by physical, psychological and social components of frailty in community—Dwelling older people. Qual. Life Res. 2014, 23, 2289–2300. [Google Scholar] [CrossRef] [PubMed]
- Helvik, A.S.; Engedal, K.; Selbaek, G. Sense of coherence and quality of life in older in-hospital patients without cognitive impairment -a 12 month follow-up study. BMC Psychiatry 2014, 14, 82. [Google Scholar] [CrossRef] [PubMed]
- Costa, P.; Driusso, P.; Oishi, J. Convergent validity between SF-36 and WHOQOL-BREF in older adults. Rev. Saude Publica 2014, 48, 63–67. [Google Scholar]
- Conrad, I.; Matschinger, H.; Riedel-Heller, S.; von Gotteberg, C.; Kilian, R. The psychometric properties of the German version of the WHOQOL-OLD in the German population aged 60 and older. Health Qual. Life Outcomes 2014, 12, 105. [Google Scholar] [CrossRef] [PubMed]
- Eser, S.; Saatli, G.; Eser, E.; Baydur, H.; Fidaner, C. The reliability and validity of the Turkish version of the World Health Organization Quality of Life Instrument—Older Adults Module (WHOQOL-OLD). Turk. Psikiyatri Derg. 2010, 21, 37–48. [Google Scholar]
- Gobbens, R.J.J.; van Assen, M.A.L.M. Psychometric properties of the Dutch WHOQOL-OLD. Health Qual. Life Outcomes 2016, 14, 103. [Google Scholar] [CrossRef]
- Leplege, A.; Perret-Guillaume, C.; Ecosse, E.; Hervy, M.P.; Ankri, J.; von Steinbuchel, N. A new instrument to measure quality of life in older people: The French version of the WHOQOL-OLD. Rev. Med. Interne 2014, 34, 78–84. [Google Scholar]
- Power, M.; Quinn, K.; Schmidt, S. WHOQOL-OLD Group. Development of the WHOQOL-OLD module. Qual. Life Res 2005, 14, 2197–21214. [Google Scholar] [CrossRef]
- WHOQOL Group 2016. User Manual. Available online: https://www.millisecond.com/download/library/v6/whoqol_bref/whoqol_bref.manual (accessed on 25 October 2022).
- Pinquart, M.; Sörensen, S. Influences of socieconomic status, social networks, and competence on subjective well-being in later life: A meta-analysis. Psychol. Aging 2000, 15, 187–224. [Google Scholar] [CrossRef] [PubMed]
- Parra, D.C.; Gómez, L.F.; Sarmiento, O.L.; Buchner, D.; Brownson, R.; Schimd, T.; Gómez, V.; Lobelo, F. Perceived and objective neighbourhood environment attributes and health related quality of life among the elderly in Bogotá. Colombia. Soc. Sci. Med. 2010, 70, 1070–1076. [Google Scholar] [CrossRef] [PubMed]
- Espinoza, I.; Osorio, P.; Torrejón, M.J.; Lucas-Carrasco, R.; Bunout, D. Validación del cuestionario de calidad de vida (WHOQOL-BREF) en adultos mayores chilenos. Rev. Med. Chile 2011, 139, 579–586. [Google Scholar] [CrossRef]
- Bunout, D.; Osorio, P.; Barrera, G.; Torrejon, M.J.; Meersohn, C.; Anigstein, M.S.; Miranda, J.P.; Espinoza, I.; Hirsch, S.; de la Maza, M.P. Quality of life of older Chilean people living in metropolitan Santiago, Chile: Influence of socioeconomic status. Ageing Res. 2012, 4, 15–18. [Google Scholar]
- Bland, A.M.; Altaman, D.G. Cronbach’s alpha. BMJ 1997, 314, 572. [Google Scholar] [CrossRef] [PubMed]
- Mardia, K.V. Measures of Multivariate Skewness and Kurtosis with Applications. Biometrika 1970, 57, 519. [Google Scholar] [CrossRef]
- Li, C.H. Confirmatory factor analysis with ordinal data: Comparing robust maximum likelihood and diagonally weighted least squares. Behav. Res. Methods 2016, 48, 936–949. [Google Scholar] [CrossRef] [PubMed]
- Hair, J.F. (Ed.) Multivariate Data Analysis, 7th ed.; Prentice Hall: Upper Saddle River, NJ, USA, 2010. [Google Scholar]
- Satorra, A.; Bentler, E.M. Corrections to test statistics and standard errors in covariance structure analysis. In Latent Variables Analysis: Applications for Developmental Research; von Eye, A., Clogg, C.C., Eds.; Sage: Thousand Oaks, CA, USA, 1994; pp. 399–419. [Google Scholar]
- Kalfoss, M.H.; Low, G.; Molzahn, A.E. The suitability of the WHOQOL-BREF for Canadian and Norwegian older adults. Eur. J. Ageing 2008, 5, 77–80. [Google Scholar] [CrossRef]
- Barrientos, J.; Páez, D. Variables of sexual satisfaction in Chile. J. Sex Marital Ther. 2006, 32, 351–368. [Google Scholar] [CrossRef]
- Campisi, J.; Kapahi, P.; Lithgow, G.J.; Melov, S.; Newman, J.C.; Verdin, E. From discoveries in ageing research to therapeutics for healthy ageing. Nature 2019, 571, 183–192. [Google Scholar] [CrossRef]
- Navarro, J.; Cañete, M.; Olivera, F.J.; Gil-Lacruz, M.; Gil-Lacruz, A.; Marijuán, P.C. The Cost of Loneliness: Assessing the Social Relationships of the Elderly via an Abbreviated Sociotype Questionnaire for inside and outside the Clinic. Int. J. Environ. Res. Public Health 2002, 19, 1253. [Google Scholar] [CrossRef]
- Puts, M.T.; Shekary, N.; Widdershoven, G.; Heldens, J.; Lips, P.; Deeg, D.J.H. What does quality of life mean to older frail and non-frail community dwelling adults in the Netherlands? Qual. Life Res. 2007, 16, 263–277. [Google Scholar] [CrossRef] [PubMed]
- Gobbens, R.J.; van Assen, M.A.; Luijkx, K.G.; Schols, J.M. The predictive validity of the Tilburg Frailty Indicator. Disability, health care utilization and quality of life in a population at risk. Gerontologist 2012, 52, 619–631. [Google Scholar] [CrossRef] [PubMed]
- Paskulin, L.M.; Molzahan, A. Quality of life of older adults in Canada and Brazil. West J. Nurs. Res. 2007, 29, 10–26. [Google Scholar] [CrossRef] [PubMed]
- Cortés, A.M.; Villareal, E.; Galicia, L.; Martínez, L.; Vargas, E.R. Evaluación geriátrica integral del adulto mayor. Rev. Med. Chile 2011, 139, 725–731. [Google Scholar] [CrossRef]


{kind=link}
| Universe | Sample | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| Men | Women | Men | Women | ||||||
| Absolute Frequency | Relative Frequency | Absolute Frequency | Relative Frequency | No. of Tests | % Test | No. of Tests | % Test | Total | |
| Third Age (60–79) | 1000 | 45% | 1180 | 55% | 106 | 40.3% | 157 | 59.7% | 263 |
| Fourth Age (80+) | 195 | 34% | 376 | 66% | 29 | 34.5% | 55 | 65.5% | 84 |
| Total | 1195 | 43% | 1556 | 57% | 135 | 38.9% | 212 | 61.1% | 347 |
| Variables | Absolute Frequency | Relative Frequency |
|---|---|---|
| Civil status | ||
| Single | 11 | 3.2 |
| Married/cohabiting | 231 | 66.6 |
| Separated/divorced | 6 | 1.7 |
| Widow/Widower | 97 | 28.0 |
| NS/NA | 2 | 0.5 |
| Education | ||
| No studies | 61 | 17.6 |
| Primary | 180 | 51.9 |
| Secondary | 63 | 18.2 |
| University | 42 | 12.1 |
| NS/NA | 1 | 0.3 |
| Area of residence | ||
| Viñedo Viejo | 231 | 66.6 |
| Fuentes Claras | 24 | 6.9 |
| Las Nieves | 82 | 23.6 |
| NS/NA | 10 | 2.9 |
| Perception of economic level | ||
| Problems of budgeting to end of month | 45 | 13.0 |
| Usually able to budget to end of month | 120 | 34.6 |
| No problem budgeting to end of month | 119 | 34.3 |
| Savings | 58 | 16.7 |
| NS/NA | 5 | 1.4 |
| Medical diagnosis | ||
| Yes | 262 | 75.5 |
| No | 64 | 18.4 |
| NS/NA | 21 | 6.1 |
| Domain | Physical Health | Psychological Health | Social Relations | Environment |
|---|---|---|---|---|
| Description | ||||
| No. of items | 7 | 6 | 3 | 8 |
| No. of valid answers | 322 | 322 | 322 | 322 |
| Median | 13.7 | 14.0 | 13.3 | 14.0 |
| Interquartile range | 4.0 | 3.2 | 4.0 | 3.5 |
| Range | 14.9 | 12.3 | 16 | 10 |
| Skewness | −0.18 | −0.26 | −0.06 | −0.04 |
| Kurtosis | −0.26 | 0.02 | 0.32 | −0.58 |
| Minimum | 5.1 | 6.7 | 4.0 | 9.5 |
| Maximum | 20.0 | 20.0 | 20.0 | 19.5 |
| Items | Corrected Item-Total Correlation |
|---|---|
| Physical Health | |
| Pain | 0.450 |
| Dependence on medication | 0.431 |
| Energy for daily life * | 0.724 |
| Mobility * | 0.625 |
| Sleep and rest | 0.417 |
| Daily life activities * | 0.772 |
| Capacity for work * | 0.702 |
| Psychological Health | |
| Positive feelings | 0.559 |
| Spirituality, religion | 0.556 |
| Thought, learning | 0.322 |
| Body image | 0.449 |
| Self-confidence * | 0.677 |
| Negative feelings | 0.396 |
| Social Relationships | |
| Personal relationships | 0.511 |
| Sexual activity | 0.557 |
| Social support ** | 0.283 |
| Environment | |
| Freedom and safety * | 0.603 |
| Physical environment | 0.434 |
| Economic resources | 0.458 |
| Opportunity for information | 0.578 |
| Leisure and rest | 0.457 |
| Home | 0.360 |
| Healthcare ** | 0.216 |
| Transport | 0.380 |
| Questionnaire Domains | Internal Consistency (<) |
|---|---|
| Physical health | 0.809 |
| Psychological Health | 0.722 |
| Social Relationships | 0.660 |
| Environment | 0.717 |
| Total WHOQOL-BREF score | 0.908 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gil-Lacruz, M.; Cañete-Lairla, M.; Navarro, J.; Montaño-Espinoza, R.; Espinoza-Santander, I.; Osorio-Parraguez, P. Validation of the WHOQOL-BREF Quality of Life Questionnaire in an Urban Sample of Older Adults in a Neighbourhood in Zaragoza (Spain). Healthcare 2022, 10, 2272. https://doi.org/10.3390/healthcare10112272
Gil-Lacruz M, Cañete-Lairla M, Navarro J, Montaño-Espinoza R, Espinoza-Santander I, Osorio-Parraguez P. Validation of the WHOQOL-BREF Quality of Life Questionnaire in an Urban Sample of Older Adults in a Neighbourhood in Zaragoza (Spain). Healthcare. 2022; 10(11):2272. https://doi.org/10.3390/healthcare10112272
Chicago/Turabian StyleGil-Lacruz, Marta, Miguel Cañete-Lairla, Jorge Navarro, Rosa Montaño-Espinoza, Iris Espinoza-Santander, and Paulina Osorio-Parraguez. 2022. "Validation of the WHOQOL-BREF Quality of Life Questionnaire in an Urban Sample of Older Adults in a Neighbourhood in Zaragoza (Spain)" Healthcare 10, no. 11: 2272. https://doi.org/10.3390/healthcare10112272
APA StyleGil-Lacruz, M., Cañete-Lairla, M., Navarro, J., Montaño-Espinoza, R., Espinoza-Santander, I., & Osorio-Parraguez, P. (2022). Validation of the WHOQOL-BREF Quality of Life Questionnaire in an Urban Sample of Older Adults in a Neighbourhood in Zaragoza (Spain). Healthcare, 10(11), 2272. https://doi.org/10.3390/healthcare10112272