
A Case of Oral Health Management for a Patient with Extensive Ulceration of the Oral Mucosa Due to Herpes Zoster


{kind=link}
{kind=link}
{kind=link}
Abstract
1. Introduction
2. Case Presentation
2.1. Case History
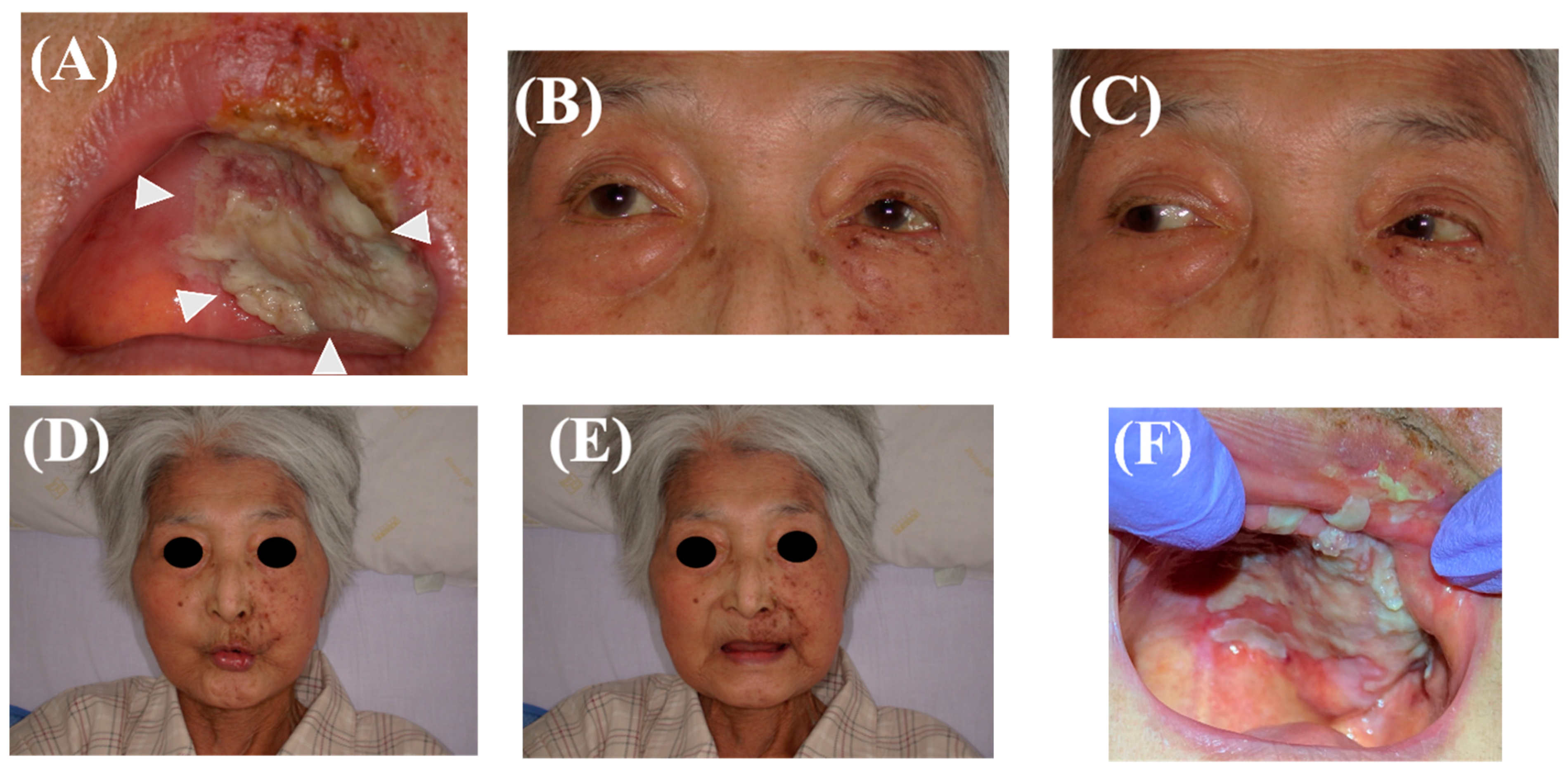
2.2. Initial Oral Evaluation
2.3. Oral Hygiene Management
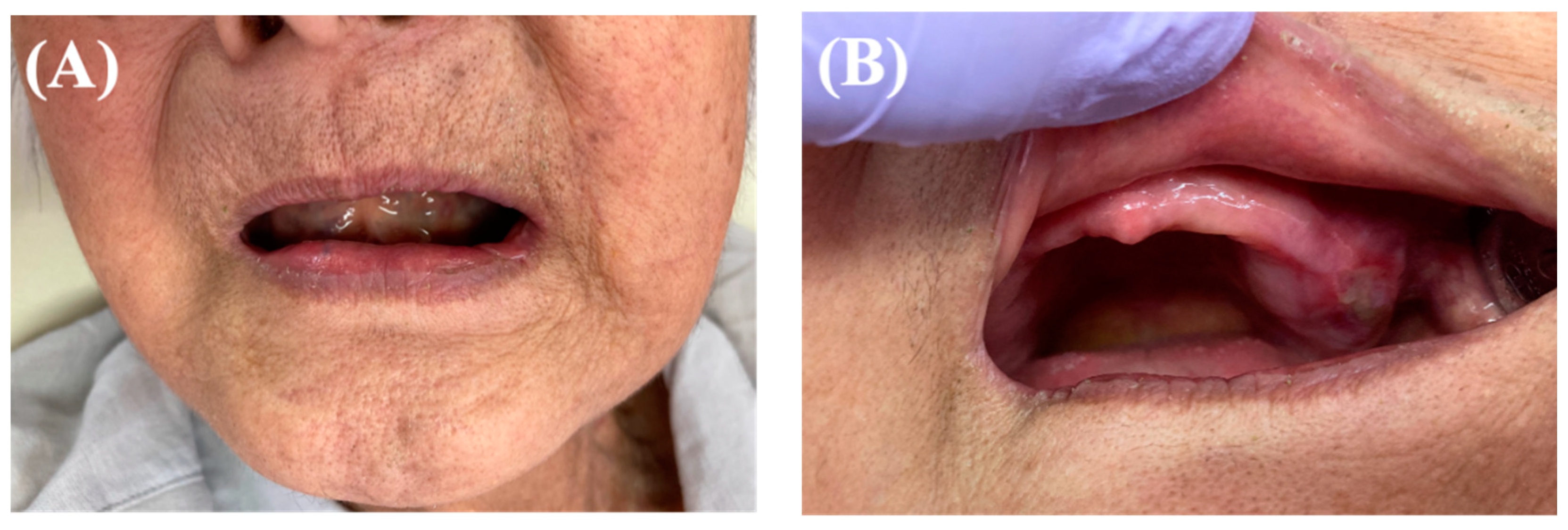
2.4. Follow-Up after Discharge
2.5. Treatment Result
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sadaksharam, J.; Kathiresan, I. Palatal fibroma in a geriatric patient: A rarity. Indian J. Med. Res. 2020, 152, S27–S28. [Google Scholar] [CrossRef] [PubMed]
- Bharti, V.; Singh, J. Capillary hemangioma of palatal mucosa. J. Indian Soc. Periodontol. 2012, 16, 475–478. [Google Scholar] [CrossRef] [PubMed]
- Aboh, I.V.; Chisci, G.; Salini, C.; Gennaro, P.; Cascino, F.; Gabriele, G.; Iannetti, G. Submandibular ossifying lipoma. J. Craniofac. Surg. 2015, 26, 973–974. [Google Scholar] [CrossRef] [PubMed]
- Orenuga, O.O.; Oluwo, A.; Oluwakuyide, R.T.; Olawuyi, A.B. Recurrent oral squamous papilloma in a pediatric patient: Case report and review of the literature. Niger J. Clin. Pract. 2018, 21, 1674–1677. [Google Scholar] [CrossRef]
- Aboh, I.V.; Chisci, G.; Cascino, F.; Parigi, S.; Gennaro, P.; Gabriele, G.; Iannetti, G. Giant palatal schwannoma. J. Craniofac. Surg. 2014, 25, e418–e420. [Google Scholar] [CrossRef]
- Pappas, D.A.; Hooper, M.M.; Kremer, J.M.; Reed, G.; Shan, Y.; Wenkert, D.; Greenberg, J.D.; Curtis, J.R. Herpes Zoster Reactivation in Patients With Rheumatoid Arthritis: Analysis of Disease Characteristics and Disease-Modifying Antirheumatic Drugs. Arthritis Care Res. 2015, 67, 1671–1678. [Google Scholar] [CrossRef]
- Nair, P.; Gharote, H.; Singh, P.; Jain-Choudhary, P. Herpes zoster on the face in the elderly. BMJ Case Rep. 2014, 2014, bcr2013200101. [Google Scholar] [CrossRef]
- Schmader, K. Herpes Zoster. Ann. Intern. Med. 2018, 169, ITC19–ITC31. [Google Scholar] [CrossRef]
- Toyama, N.; Shiraki, K.; Society of the Miyazaki Prefecture, D. Epidemiology of herpes zoster and its relationship to varicella in Japan: A 10-year survey of 48,388 herpes zoster cases in Miyazaki prefecture. J. Med. Virol. 2009, 81, 2053–2058. [Google Scholar] [CrossRef]
- Decroix, J.; Partsch, H.; Gonzalez, R.; Mobacken, H.; Goh, C.L.; Walsh, L.; Shukla, S.; Naisbett, B. Factors influencing pain outcome in herpes zoster: An observational study with valaciclovir. Valaciclovir International Zoster Assessment Group (VIZA). J. Eur. Acad. Dermatol. Venereol. 2000, 14, 23–33. [Google Scholar] [CrossRef]
- Koshy, E.; Mengting, L.; Kumar, H.; Jianbo, W. Epidemiology, treatment and prevention of herpes zoster: A comprehensive review. Indian J. Dermatol. Venereol. Leprol. 2018, 84, 251–262. [Google Scholar] [CrossRef] [PubMed]
- Freites-Martinez, A.; Santana, N.; Arias-Santiago, S.; Viera, A. Using the Common Terminology Criteria for Adverse Events (CTCAE—Version 5.0) to Evaluate the Severity of Adverse Events of Anticancer Therapies. Actas Dermosifiliogr. 2021, 112, 90–92. [Google Scholar] [CrossRef] [PubMed]
- Kakuta, R.; Okata, U.; Funakoshi, T.; Fujio, Y.; Inoue, N.; Takahashi, S.; Amagai, M.; Ohyama, M. Unusually extensive disseminated herpes zoster with multiple ulcer formation in a methotrexate-treated rheumatoid arthritis patient. J. Dermatol. 2014, 41, 181–182. [Google Scholar] [CrossRef]
- Kolokotronis, A.; Louloudiadis, K.; Fotiou, G.; Matiais, A. Oral manifestations of infections of infections due to varicella zoster virus in otherwise healthy children. J. Clin. Pediatr. Dent. 2001, 25, 107–112. [Google Scholar] [CrossRef]
- Elad, S.; Cheng, K.K.F.; Lalla, R.V.; Yarom, N.; Hong, C.; Logan, R.M.; Bowen, J.; Gibson, R.; Saunders, D.P.; Zadik, Y.; et al. MASCC/ISOO clinical practice guidelines for the management of mucositis secondary to cancer therapy. Cancer 2020, 126, 4423–4431. [Google Scholar] [CrossRef] [PubMed]
- Kiyomi, A.; Yoshida, K.; Arai, C.; Usuki, R.; Yamazaki, K.; Hoshino, N.; Kurokawa, A.; Imai, S.; Suzuki, N.; Toyama, A.; et al. Salivary inflammatory mediators as biomarkers for oral mucositis and oral mucosal dryness in cancer patients: A pilot study. PLoS ONE 2022, 17, e0267092. [Google Scholar] [CrossRef] [PubMed]
- Patil, A.; Goldust, M.; Wollina, U. Herpes zoster: A Review of Clinical Manifestations and Management. Viruses 2022, 14, 192. [Google Scholar] [CrossRef] [PubMed]
- Sio, T.T.; Le-Rademacher, J.G.; Leenstra, J.L.; Loprinzi, C.L.; Rine, G.; Curtis, A.; Singh, A.K.; Martenson, J.A., Jr.; Novotny, P.J.; Tan, A.D.; et al. Effect of Doxepin Mouthwash or Diphenhydramine-Lidocaine-Antacid Mouthwash vs Placebo on Radiotherapy-Related Oral Mucositis Pain: The Alliance A221304 Randomized Clinical Trial. JAMA 2019, 321, 1481–1490. [Google Scholar] [CrossRef]
- Ueno, T.; Yatsuoka, W.; Ishiki, H.; Miyano, K.; Uezono, Y. Effects of an oral mucosa protective formulation on chemotherapy- and/or radiotherapy-induced oral mucositis: A prospective study. BMC Cancer 2022, 22, 90. [Google Scholar] [CrossRef]
- Ogata, J.; Minami, K.; Horishita, T.; Shiraishi, M.; Okamoto, T.; Terada, T.; Sata, T. Gargling with sodium azulene sulfonate reduces the postoperative sore throat after intubation of the trachea. Anesth. Analg. 2005, 101, 290–293. [Google Scholar] [CrossRef]
- Keefe, D.M.; Schubert, M.M.; Elting, L.S.; Sonis, S.T.; Epstein, J.B.; Raber-Durlacher, J.E.; Migliorati, C.A.; McGuire, D.B.; Hutchins, R.D.; Peterson, D.E.; et al. Updated clinical practice guidelines for the prevention and treatment of mucositis. Cancer 2007, 109, 820–831. [Google Scholar] [CrossRef] [PubMed]
- Sekiya, H.; Kurasawa, Y.; Kaneko, K.; Takahashi, K.I.; Maruoka, Y.; Michiwaki, Y.; Takeda, Y.; Ochiai, R. Preventive Effects of Sustainable and Developmental Perioperative Oral Management Using the "Oral Triage" System on Postoperative Pneumonia after Cancer Surgery. Int. J. Environ. Res. Public Health 2021, 18, 6296. [Google Scholar] [CrossRef] [PubMed]



Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Matsuda, Y.; Mizuno, R.; Miyajima, S.; Arakawa, S.; Kabasawa, Y. A Case of Oral Health Management for a Patient with Extensive Ulceration of the Oral Mucosa Due to Herpes Zoster. Healthcare 2022, 10, 2249. https://doi.org/10.3390/healthcare10112249
Matsuda Y, Mizuno R, Miyajima S, Arakawa S, Kabasawa Y. A Case of Oral Health Management for a Patient with Extensive Ulceration of the Oral Mucosa Due to Herpes Zoster. Healthcare. 2022; 10(11):2249. https://doi.org/10.3390/healthcare10112249
Chicago/Turabian StyleMatsuda, Yuhei, Ruriko Mizuno, Saki Miyajima, Shinichi Arakawa, and Yuji Kabasawa. 2022. "A Case of Oral Health Management for a Patient with Extensive Ulceration of the Oral Mucosa Due to Herpes Zoster" Healthcare 10, no. 11: 2249. https://doi.org/10.3390/healthcare10112249
APA StyleMatsuda, Y., Mizuno, R., Miyajima, S., Arakawa, S., & Kabasawa, Y. (2022). A Case of Oral Health Management for a Patient with Extensive Ulceration of the Oral Mucosa Due to Herpes Zoster. Healthcare, 10(11), 2249. https://doi.org/10.3390/healthcare10112249