

Door to Disposition Key Performance Indicator in Three Saudi Arabian Hospitals’ Emergency Departments during COVID-19 Pandemic

Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Source
2.2. Outcome Variable
2.3. Statistical Analysis
2.4. Ethical Considerations
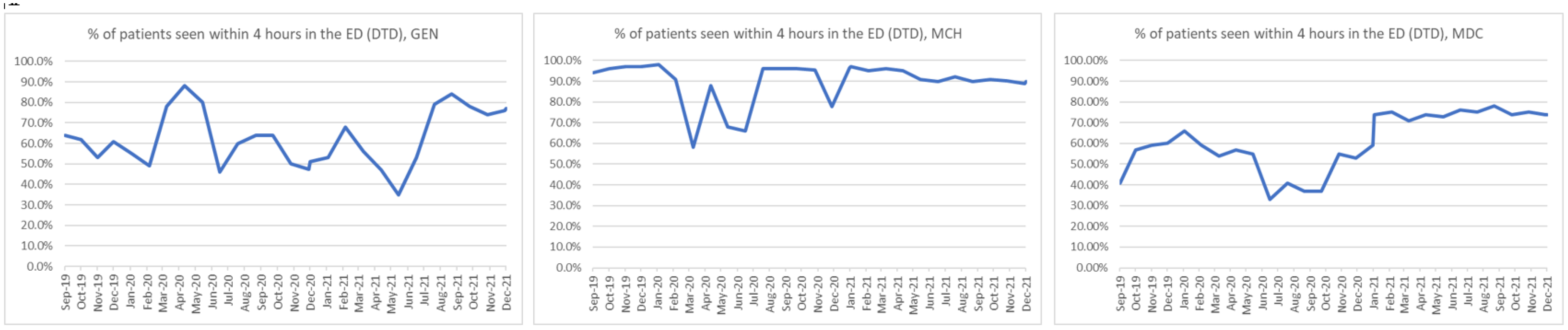
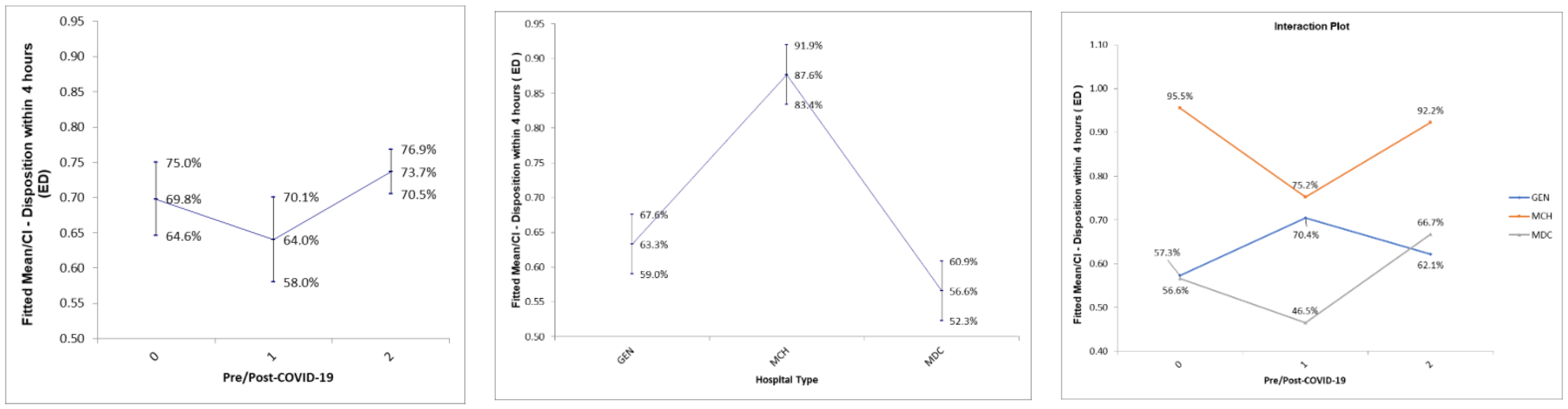
3. Results
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
| Year | MCH 300-Bed | GEN 643-Bed | MDC 1230-Bed |
|---|---|---|---|
| 2019 | 116,517 | 94,225 | 91,910 |
| 2020 | 56,645 | 33,441 | 82,099 |
| 2021 | 79,365 | 28,793 | 87,700 |
References
- WHO Director-General’s Opening Remarks at the Media Briefing on COVID-19—21 December 2020. Available online: https://www.who.int/director-general/speeches/detail/who-director-general-s-opening-remarks-at-the-media-briefing-on-covid-19---21-december-2020 (accessed on 14 October 2022).
- Al-Ahdal, M.N.; Al-Ahdal, M.N. COVID-19 pandemic in Saudi Arabia: The decline continues. Glob. J. Infect. Dis. Clin. Res. 2020, 6, 57–59. [Google Scholar]
- World Health Organization (WHO). Coronavirus (COVID-19) Statistics. Available online: https://covid19.who.int (accessed on 22 August 2022).
- Alzahrani, A.; Kujawski, S.A.; Abedi, G.R.; Tunkar, S.; Biggs, H.M.; Alghawi, N.; Jokhdar, H.; Assiri, A.M.; Watson, J.T. Surveillance and Testing for Middle East Respiratory Syndrome Coronavirus, Saudi Arabia, March 2016–March 2019. Emerg. Infect. Dis. 2020, 26, 1571–1574. [Google Scholar] [CrossRef]
- The Saudi Ministry of Health. COVID-19 Guidelines. Ministry of Health Saudi Arabia. Available online: https://www.moh.gov.sa/en/Ministry/MediaCenter/Publications/Pages/covid19.aspx (accessed on 16 October 2022).
- The Saudi Ministry of Health. Self-Assessment Exams through Mobile App “Mawid”. Ministry Of Health Saudi Arabia. Available online: https://www.moh.gov.sa/en/Ministry/MediaCenter/News/Pages/News-2020-04-25-001.aspx (accessed on 16 October 2022).
- Saudi Ministry of Health. Specialized Drive-through Testing Centers. Ministry of Health Saudi Arabia. Available online: https://www.moh.gov.sa/en/Ministry/MediaCenter/News/Pages/News-2020-07-14-008.aspx (accessed on 16 October 2022).
- Alsofayan, Y.M.; Althunayyan, S.M.; Khan, A.A.; Hakawi, A.M.; Assiri, A.M. Clinical characteristics of COVID-19 in Saudi Arabia: A national retrospective study. J. Infect. Public Health 2020, 13, 920–925. [Google Scholar] [CrossRef] [PubMed]
- Araja, D.; Berkis, U.; Murovska, M. COVID-19 Pandemic-Revealed Consistencies and Inconsistencies in Healthcare: A Medical and Organizational View. Healthcare 2022, 10, 1018. [Google Scholar] [CrossRef] [PubMed]
- Modenese, A.; Loney, T.; Gobba, F. COVID-19-Related Mortality amongst Physicians in Italy: Trend Pre- and Post-SARS-CoV-2 Vaccination Campaign. Healthcare 2022, 10, 1187. [Google Scholar] [CrossRef]
- Sono-Setati, M.E.; Mphekgwana, P.M.; Mabila, L.N.; Mbombi, M.O.; Muthelo, L.; Matlala, S.F.; Tshitangano, T.G.; Ramalivhana, N.J. Health System- and Patient-Related Factors Associated with COVID-19 Mortality among Hospitalized Patients in Limpopo Province of South Africa’s Public Hospitals. Healthcare 2022, 10, 1338. [Google Scholar] [CrossRef]
- Suppapitnarm, N.; Saengpattrachai, M. Physician Engagement before and during the COVID-19 Pandemic in Thailand. Healthcare 2022, 10, 1394. [Google Scholar] [CrossRef]
- Crowding & Boarding. Available online: https://www.acep.org/administration/crowding--boarding/ (accessed on 18 July 2022).
- af Ugglas, B.; Skyttberg, N.; Wladis, A.; Djärv, T.; Holzmann, M.J. Emergency department crowding and hospital transformation during COVID-19, a retrospective, descriptive study of a university hospital in Stockholm, Sweden. Scand. J. Trauma Resusc. Emerg. Med. 2020, 28, 107. [Google Scholar] [CrossRef]
- Guo, F.; Qin, Y.; Fu, H.; Xu, F. The impact of COVID-19 on Emergency Department length of stay for urgent and life-threatening patients. BMC Health Serv. Res. 2022, 22, 696. [Google Scholar] [CrossRef]
- Chun, S.Y.; Kim, H.J.; Kim, H.B. The effect of COVID-19 pandemic on the length of stay and outcomes in the emergency department. Clin. Exp. Emerg. Med. 2022, 9, 128–133. [Google Scholar] [CrossRef]
- Islam, M.I.; Freeman, J.; Chadwick, V.; Martiniuk, A. Healthcare Avoidance before and during the COVID-19 Pandemic among Australian Youth: A Longitudinal Study. Healthcare 2022, 10, 1261. [Google Scholar] [CrossRef] [PubMed]
- Cedrone, F.; Di Martino, G.; Di Giovanni, P.; Greco, E.; Trebbi, E.; Romano, F.; Staniscia, T. Reduction in Hospital Admissions for Cardiovascular Diseases (CVDs) during the Coronavirus Disease 2019 (COVID-19) Pandemic: A Retrospective Study from a Southern Italian Region in the Year 2020. Healthcare 2022, 10, 871. [Google Scholar] [CrossRef] [PubMed]
- Abdelhadi, A. The Effects on the Number of Patients Visiting the Emergency Units: Comparison Study Before and During COVID-19 Pandemic in Saudi Arabia. J. Multidiscip. Healthc. 2021, 14, 1207–1211. [Google Scholar] [CrossRef] [PubMed]
- Kastritis, E.; Tsitsimpis, K.; Anninos, E.; Stamatelopoulos, K.; Kanakakis, I.; Lampropoulos, C.; Chatzidou, S.; Michopoulos, S.; Papamichail, C.; Kostis, E.; et al. Significant reduction in the visits to the emergency room department during the COVID-19 pandemic in a tertiary hospital in Greece. Medicine 2020, 99, e23845. [Google Scholar] [CrossRef] [PubMed]
- Alharthi, S.; Al-Moteri, M.; Plummer, V.; Al Thobiaty, A. The Impact of COVID-19 on the Service of Emergency Department. Healthcare 2021, 9, 1295. [Google Scholar] [CrossRef] [PubMed]
- Wartelle, A.; Mourad-Chehade, F.; Yalaoui, F.; Chrusciel, J.; Laplanche, D.; Sanchez, S. Effect of the COVID-19 pandemic lockdown on non-COVID-19 emergency department visits in Eastern France: Reduced risk or avoidance behavior? Public Health Pract. 2021, 2, 100109. [Google Scholar] [CrossRef]
- Verdoni, F.; Ricci, M.; Di Grigoli, C.; Rossi, N.; Lombardo, M.; Curci, D.; Accetta, R.; Viganò, M.; Peretti, G.; Mangiavini, L. Effect of the COVID-19 Outbreak on Pediatric Patients’ Admissions to the Emergency Department in an Italian Orthopedic Trauma Hub. Child 2021, 8, 645. [Google Scholar] [CrossRef]
- Asplin, B.R.; Magid, D.J.; Rhodes, K.V.; Solberg, L.I.; Lurie, N.; Camargo, C.A. A conceptual model of emergency department crowding. Ann. Emerg. Med. 2003, 42, 173–180. [Google Scholar] [CrossRef]
- Rivera-Sepulveda, A.; Maul, T.; Dong, K.; Crate, K.; Helman, T.; Bria, C.; Martin, L.; Bogers, K.; Pearce, J.W.; Glass, T.F. Effect of the COVID-19 Pandemic on the Pediatric Emergency Department Flow. Disaster Med. Public Health Prep. 2021, 20, 1–7. [Google Scholar] [CrossRef]
- Sibbritt, D.; Isbister, G.K.; Walker, R. Emergency Department Performance Indicators That Encompass the Patient Journey. Qual. Manag. Healthc. 2006, 15, 27–38. [Google Scholar] [CrossRef]
- Wu, X.; Zhang, Y.; Guo, X. Research on the Equity and Influencing Factors of Medical and Health Resources Allocation in the Context of COVID-19: A Case of Taiyuan, China. Healthcare 2022, 10, 1319. [Google Scholar] [CrossRef] [PubMed]
| KPI: Door to Disposition (Percentage of Patient Seen within Four Hours) | |
|---|---|
| Sample size | All patient volume |
| Numerator | Number of patient Door to Disposition < 4 h. |
| Denominator | Total number of patients |
| Calculation | [Numerator/denominator] × 100 |
| Exclusion | DAMA *, LAMA ** & Morgue |
| Disposition | patient either Admission or Discharge |
| Patient admission | ICU and WARD |
| Patient discharge | DAMA, LAMA, Home, Transferred to another facility and deceased. |
| World class | more than 95% |
| Acceptable | 75–95% |
| Need Improvement | 60–75% |
| Unacceptable | less than 60% |
| Source | DF | SS | MS | F | p |
|---|---|---|---|---|---|
| Pre/Post-COVID-19 | 2 | 0.106306131 | 0.053153066 | 4.121 | 0.0200 |
| Hosp. Type | 2 | 1.109494876 | 0.554747 | 43.007 | <0.001 |
| Interaction | 4 | 0.238680 | 0.05967011 | 4.626 | 0.0022 |
| Error | 75 | 0.967428 | 0.012899034 | ||
| Total | 83 | 2.764 | 0.033304285 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Almana, R.S.; Alharbi, A. Door to Disposition Key Performance Indicator in Three Saudi Arabian Hospitals’ Emergency Departments during COVID-19 Pandemic. Healthcare 2022, 10, 2193. https://doi.org/10.3390/healthcare10112193
Almana RS, Alharbi A. Door to Disposition Key Performance Indicator in Three Saudi Arabian Hospitals’ Emergency Departments during COVID-19 Pandemic. Healthcare. 2022; 10(11):2193. https://doi.org/10.3390/healthcare10112193
Chicago/Turabian StyleAlmana, Ranya S., and Abeer Alharbi. 2022. "Door to Disposition Key Performance Indicator in Three Saudi Arabian Hospitals’ Emergency Departments during COVID-19 Pandemic" Healthcare 10, no. 11: 2193. https://doi.org/10.3390/healthcare10112193
APA StyleAlmana, R. S., & Alharbi, A. (2022). Door to Disposition Key Performance Indicator in Three Saudi Arabian Hospitals’ Emergency Departments during COVID-19 Pandemic. Healthcare, 10(11), 2193. https://doi.org/10.3390/healthcare10112193