Abstract
Artificial intelligence has been widely used in the field of dentistry in recent years. The present study highlights current advances and limitations in integrating artificial intelligence, machine learning, and deep learning in subfields of dentistry including periodontology, endodontics, orthodontics, restorative dentistry, and oral pathology. This article aims to provide a systematic review of current clinical applications of artificial intelligence within different fields of dentistry. The preferred reporting items for systematic reviews (PRISMA) statement was used as a formal guideline for data collection. Data was obtained from research studies for 2009–2022. The analysis included a total of 55 papers from Google Scholar, IEEE, PubMed, and Scopus databases. Results show that artificial intelligence has the potential to improve dental care, disease diagnosis and prognosis, treatment planning, and risk assessment. Finally, this study highlights the limitations of the analyzed studies and provides future directions to improve dental care.
1. Introduction
Artificial intelligence (AI) has been widely utilized in the field of medicine since its conception over 60 years ago [1,2,3,4]. Although the maturity of AI in the field of dentistry has lagged in several subfields such as periodontology, endodontics, orthodontics, restorative dentistry, and oral pathology, there has been a large interest in the past few years as artificial intelligence has become increasingly accessible to researchers. AI has made substantial progress in the diverse disciplines of dentistry including dental disease diagnosis [5], localization [6], classification [7], estimation [8], and assessment of dental disease [9].
On a broader level, AI enables the creation of intelligent machines that can achieve tasks without requiring human intervention. Machine learning (ML) [10] is a subset of AI that utilizes computational algorithms to analyze datasets to make predictions without the need for explicit instructions. Towards a more sophisticated and increasingly independent approach for diagnosis, treatment planning, and risk assessment, there has been increased interest in deep learning (DL) applications [11,12]. To provide expert support to healthcare practitioners, artificial neural networks (ANNs) can be utilized as clinical decision support systems (CDSS) [13]. Moreover, such systems aid dental clinicians in producing improved dental health outcomes [14]. Similarly, fuzzy logic (FL)-based CDSS also provides effective means for dealing with uncertainties in the decision-making process [15,16].
1.1. Background
The related background of ANNs, machine learning, deep learning, CDSS, and Fuzzy logic is discussed in the below subsections.
1.1.1. Artificial Neural Networks
ANNs evolved after McCulloch and Pitts created a model in 1943 based on many simple processing units, such as neurons connected using weighted links. In 1958, Rosenbolt published neurodynamic principles containing research ideas related to brain modeling. Later, in the 1980s, researchers developed algorithms based on the idea of backpropagation to be applied in the medical field [1].
ANNs comprise data processing mechanisms inspired by the analytical processes of the human brain. The ANNs are used extensively to solve complex real-world problems [2]. Due to ANN’s remarkable learning, generalization, inherent contextual information processing, and fault and noise tolerance capabilities, they provide exciting alternatives and have many applications including medicinal science such as disease diagnosis, image and data analysis, and biomedical identification [3,4].
1.1.2. Machine Learning
ML is the scientific study of algorithms and statistical models [10] used for a vast array of processing tasks without requiring prior knowledge or hand-crafted rules. Recent years have witnessed the widespread of ML due to its superior performance for various healthcare applications such as dentistry. ML algorithms fall into two learning types: supervised and unsupervised. The amount of data generated by healthcare service providers is huge, making the data analysis process cumbersome. ML helps in effectively analyzing the data and gaining actionable insights. Additionally, different dentistry applications can benefit from ML techniques, including disease diagnosis, prognosis, treatment, and automating the clinical workflow. Moreover, ML for clinical applications has great potential to transform traditional healthcare service delivery [17].
1.1.3. Deep Learning
Recent years have seen a surge of interest in the DL field, a subfield of ML, as it allows machines to mimic human intelligence in increasingly independent and sophisticated ways [11,12]. DL uses multiple layers of non-linear units to analyze and extract useful knowledge from huge amounts of data. The extracted knowledge is then used to produce state-of-the-art prediction results. The neural network architectures used in DL provide the capability to perform automatic and accurate detection in healthcare. Based on the study, DL has enormous potential to bring genuinely impactful applications to the field of dentistry.
1.1.4. ANNs as Clinical Decision Support Systems
AI application technology is progressing remarkably in the field of dentistry; clinical decision support systems are one example in this context. CDSS provides expert support to a health practitioner [13]. Moreover, these systems have the capability of solving problems that are too complex to be solved by using conventional methods [14]. Moreover, CDSS provides valuable information to dental practitioners that aids in producing faster and superior dental health outcomes.
1.1.5. Fuzzy Logic
In the past decade, fuzzy logic has proven to be a powerful tool for decision-making systems [15]. The fuzzy set theory derives from the fact that the natural classes and concepts are vague. This makes fuzzy logic quite suitable for complex systems as they can summarize from massive information inputs with increased effectiveness and tolerance to imprecisions [16]. The study provides brief descriptions of the key contributions made by fuzzy technology in the field of dentistry.
1.2. Motivation and Contributions
Several surveys addressing the use of AI in dentistry have been published in recent years. Ossowoska et al. [18] discuss the possibilities of using neural networks in different fields of dentistry including restorative dentistry, endodontics, orthodontics, dental surgery, and periodontology. The study indicates that artificial intelligence has developed rapidly in recent years and has the potential to be applied in routine dentistry. However, the study lacks discussion related to the limitations of the included studies. This study aims to outline the clinical support decision systems developed in recent years possess the potential to be employed in different fields of dentistry. We also discuss the limitations and formulate future directions of such approaches to contribute to improving the current state of clinical dental practice. The contributions of this study are provided below
- Identify the development of AI applications that are employed widely in dentistry for different diagnostic tasks such as disease diagnosis, risk assessment, treatment planning, and prognosis and evaluate their diagnostic performance,
- Outline the limitations of the neural networks employed for different diagnostic tasks including disease diagnosis, landmark detection, risk assessment, treatment planning, and prognosis,
- Provide future directions which may have a positive and stimulating impact on the future application of artificial intelligence-based techniques in the field of dentistry.
1.3. Article Organization
2. Methodology
For this article, the preferred reporting items for systematic reviews (PRISMA) guidelines are followed. PRISMA provides a standard peer-accepted methodology consisting of a guideline checklist to ensure the quality assurance of the work’s replicability. This section defines the article selection criteria, data sources, and the search strategy for data extraction and analysis procedure.
2.1. Research Questions
Following are the research questions formulated to analyze the relevant studies:
- RQ1.
- What are the main fields in dentistry in which AI is employed?
- RQ2.
- What are data modalities and features used for diagnosing dental diseases?
- RQ3.
- Which AI techniques (including subfields) are utilized for disease diagnosis in different fields of dentistry?
- RQ4.
- Which outcome measures are used for the performance assessment of models?
Furthermore, the research question was formatted using population, intervention, comparison, and outcome (PICO):
- Population: Dental imagery related to radiographs (bitewing, periapical, occlusal, panoramic, cephalograms, cone-beam computed tomography (CBCT)), digital photographs, high-frequency ultrasound images, 3D CBCT images, domain, near-infrared light transillumination (NILT) images, extraoral/intraoral mold images, orthodontic scans, magnetic resonance imaging, water’s view radiographs, hyperspectral images and textual data including electronic health records.
- Intervention: Artificial intelligence, machine learning, deep learning-based models for diagnosis, detection, classification, segmentation, risk assessment, treatment planning, and prognosis.
- Comparison: Reference standard, expert opinions.
- Outcome: Measurable and predictive outcomes that include accuracy, specificity, sensitivity, F1-score, intersection over union (IoU), dice co-efficient, regression co-efficient receiver operating characteristic curve (ROC), and area under the curve (AUC), successful detection rate (SDR).
2.2. Data Sources and Search Strategies
Different electronic databases were systematically searched including Google Scholar, Institute of Electrical and Electronics Engineers (IEEE) Xplore, PubMed, and Scopus. The search terms were broadened to identify as many eligible studies as possible. The search key strategy adopted for each database is given in Table 1.

Table 1.
Search strategy conducted in different databases.
2.3. Selection of Studies
After an initial literature search was conducted, the title and abstract were screened for each study. Potentially relevant studies were further assessed for eligibility. Detailed information about the selection process is depicted in Figure 1.
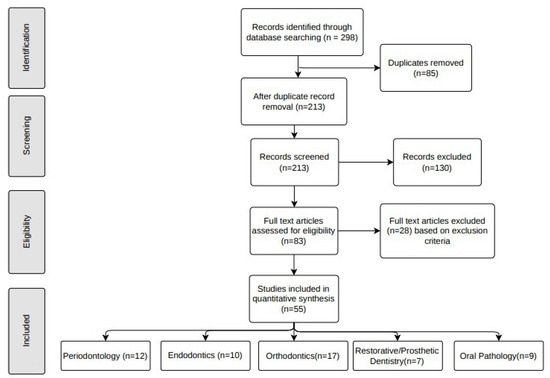
Figure 1.
Relevant data about studies included for synthesis.
For risk assessment of bias for each study, sampling and measurement bias was assessed. The articles are identified based on the library searches. A total of 298 studies (Google Scholar, n = 128, PubMed, n = 66, IEEE Xplore, n = 58, and Scopus, n = 46) were identified via the initial search process. After examining the abstracts and titles of the identified studies, duplicates (n = 85) were excluded. The remaining 213 studies were screened, out of which 130 articles without full-text availability were eliminated. The full-text articles were assessed for eligibility and based on the exclusion criteria 28 articles were excluded. Following these procedure, 55 eligible studies (periodontology, n = 12, endodontics, n = 10, orthodontics, n = 17, restorative/prosthetic dentistry, n = 7, oral pathology, n = 9) were included in this review.
2.4. Eligibility Criteria
The following inclusion criteria were used in this study
- Publications between 2009 and 2022 related to the application of artificial neural networks, machine learning, deep learning, fuzzy logic, expert systems, and clinical support decision systems (CDSS) in dentistry.
- Studies in the English language and with full-text availability.
- Published in a scholarly peer-reviewed journal.
- Publications truly implementing AI including subfields in the context of dental topics.
The studies were excluded from the review if
- Not published in a peer-reviewed journal.
- Unpublished thesis or dissertation studies.
- Studies that did not use artificial intelligence, review articles, and letter to the editor.
2.5. Risk Assessment
Each study was evaluated by the reviewers. To further minimize the risk of bias, studies dealing with AI implementation were included. Initial disagreements among the reviewers were noted while assessing the selected studies.
3. Applications of Artificial Intelligence in Dentistry
AI has made substantial progress in the diverse disciplines of medicine, specifically in the field of dentistry for diagnosis [5], localization [6], classification [7], estimation [8], and assessment of dental disease. With the recent rapid development of AI technologies designed for dental practitioners, dental clinicians make precise diagnoses and provide accurate recommendations. Figure 2 shows the areas within dentistry where AI can be used followed by a detailed description of AI applications in these fields.
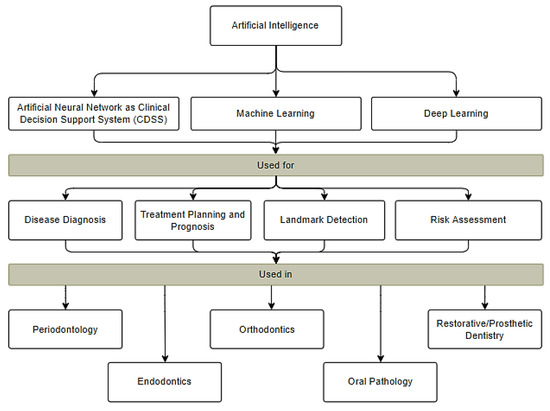
Figure 2.
Applications of AI in different subfields of dentistry.
The progressive development of AI in dentistry will benefit both researchers and clinicians in integrating different fields of knowledge to improve patient care. There are different sub-disciplines of AI that are being used to provide precise, cost-effective, and user-friendly solutions to facilitate dentists and clinicians including ANNs and ANNs as CDSS, ML, and DL. The diagnostic activities performed using different input features in dentistry are shown in Table 2.
Table 2.
Summary of input features used for different diagnostic tasks.
3.1. AI in Periodontology
In periodontology, AI has been used extensively to explore, understand and develop periodontal applications including periodontal bone loss detection, diagnosing gingivitis inflammation, and assessment of connective tissues and other periodontal caries. Table 3 shows different studies that are introduced in periodontology. These studies indicate that AI-assisted systems can be used in clinical practices to strengthen and improve dental treatment outcomes in a more sophisticated manner.
Table 3.
Summary of related studies for AI application in periodontology.
Moreover, to minimize errors in diagnosis, authors have proposed methods involving machine learning techniques. Li et al. proposed a plaque segmentation method based on a convolutional neural network (CNN) using oral endoscopic images. The results provided performance superior to that of dentists with an accuracy of 86.42% [29]. An extreme machine learning method based on contrast limited adaptive histogram and gray-level covariance matrix was evaluated by Li and fellow authors, using digital photographs. The model provided an accuracy of 74% for gingivitis identification using a small dataset [30]. For localization of alveolar bone loss, Lin et al. evaluated a level segmentation method based on a support vector machine (SVM), k nearest neighbor (KNN), and Bayesian classifier. The model was able to localize alveolar bone loss with high classification effectiveness [6].
DL-based methods have gained immense popularity in recent years. Several authors have evaluated methods for bone loss detection in intraoral radiographs, Lee et al. proposed a VGG-based neural network for diagnosing periodontal bone loss using 1740 periapical radiographs. The model achieves an accuracy of 99% and AUC of 98% outperforming the performance of three dentists [41]. Another model using deep-feed forward CNN was evaluated by Krois and fellow authors using panoramic radiographs. The model showed discrimination ability similar to that of three examiners [5]. Kim et al. and Lee et al. suggested the use of transfer learning to improve the performance of bone loss and odontogenic cyst lesion detection using panoramic radiographs. The model was useful in tooth numbering with performance superior to that of dental clinicians [44,63]. For the classification of regions based on periodontal bone destruction, Moran et al. demonstrated a ResNet model achieving an accuracy of 82% using 467 periapical radiographs [7]. To automate the process of detecting bone lesions and detecting correct shapes, Khan et al. presented a disease segmentation method based on U-Net architecture. The model was able to detect the presence and shape of caries with performance higher than three experts [44]. Another anatomically constrained dense U-Net method was proposed by Zheng et al. for bone lesion identification. Using cone beam computed tomography (CBCT) images, the model was able to detect the correct shape of the bone and lesion [8]. Duong et al. proposed a U-Net-based network for alveolar bone delineation using high-frequency ultrasound images yielding performance higher than three experts [45]. Using ResNet34 as an encoder with U-Net, Nguyen et al. assessed 1100 intraoral images for alveolar bone segmentation. The model was able to identify alveolar bone with a dice coefficient of 85.3% [46]. For periodontitis detection, Li et al. utilized Mask R-CNN with a novel calibration method. Using panoramic radiographs, the model diagnosed the severity degree of periodontitis with an accuracy of 82% outperforming that of a junior dentist [64].
In dentistry, the interpretation of data and carrying out proper diagnosis are crucial. However, medical decision-making is cumbersome for doctors in a time-compressed environment. Thus, an intelligent tool is required to assist doctors in making accurate decisions. These systems come under the category of CDSS. ANNs have been used as CDSS for diagnosis, classification, and assessment. Several ANN architectures have been employed to assist doctors in making accurate decisions in periodontology. Recently, Geetha et al. proposed a back propagation neural network for tooth decay detection. The model achieved an accuracy of 97.1% and a false positive rate of 2.8% using intraoral radiographs. The study indicates that ANNs can be employed for precise decay detection compared to traditional dental examination methods [19]. Papantonopoulos et al. evaluated multilayer perceptron ANN for bone loss assessment on medical health records. The model provided effective periodontitis classification with an accuracy of 98.1% [23]. Using 230 textual subjects, Shankarapillai et al. proposed a multilayer feed-forward propagation network for effective periodontitis risk prediction [9].
3.2. AI in Endodontics
Endodontics is the branch of dentistry concerned with diseases of the dental pulp and tissues surrounding the root or tooth. AI has gained immense popularity in aiding treatment planning in endodontics. AI with different models can help dentists to diagnose, and manage endodontic problems with encouraging performance and ensuring enhanced and precise patient care. The review is focused on extracting and analyzing AI-based approaches for disease diagnosis and treatment planning. The summary of relevant studies for AI application in endodontics to provide better dental treatment outcomes is shown in Table 4.
Table 4.
Summary of related studies for AI application in endodontics.
Ghaedi et al. presented a circular Hough transform-based segmentation method to detect and score caries lesions in intraoral occlusal tooth surface images. The model yielded an accuracy of 86.3% in detecting and scoring caries lesions [31]. A random forest-based machine learning algorithm has been proposed by Berdouses et al., evaluated on colored images, the model achieved an accuracy of 80% higher compared to two pediatric dentists [32].
Different DL models have also been employed in endodontics for disease detection, classification, and segmentation. Pauwels et al. evaluated a transfer learning-based CNN using intraoral radiographs to detect periapical lesions. The model achieved superior performance compared to three radiologists [47]. Fukuda et al. performed vertical root fracture detection using DetectNet on 300 panoramic radiographs. The model was found to be useful and provided better performance for fracture detection compared to three observers [49]. Orhan et al. proposed the U-Net model to diagnose periapical lesions using 3D CBCT images. The model was able to detect periapical lesions with 92.8% reliability [48]. A seven-layer feed-forward network was presented by Ekert et al. for diagnosing apical lesions using panoramic radiographs. Compared to six independent and experienced dentists, the model was able to detect lesions with an AUC of 85% [50]. Bayraktar and Aryan presented an interproximal caries detection method based on you look only once (YOLO) pre-trained using DarkNet-53 using bitewing radiographs. The authors achieved an accuracy of 94.59% higher compared to two experienced dentists [51]. For classification and assessment of distal roots, Hiraiwa et al. evaluated AlexNet achieving a detection performance of 87.4% superior to that of dental radiologists in differentiating whether the distal root was single or with an extra root [52]. Symmetric autoencoder with skip connections similar to U-Net and the encoding path was presented by Casalegno et al. to detect proximal occlusal caries using 217 grayscale near-infrared transilluminations (NILT) images. The model achieved higher throughput in detecting occlusal and proximal lesions compared to two dentists [53]. Kositbowornchai et al. presented a probabilistic neural network to be used as CDSS for diagnosing vertical root features. The model achieved an accuracy of 95.7% on intraoral digital radiographs [20].
3.3. AI in Orthodontics
Recent years have witnessed the immense popularity of AI in orthodontics due to its ability to make the diagnostic process more accurate and efficient. Orthodontic treatments are usually long procedures which is why more efficient solutions are required for effective and efficient planning. AI-based knowledge has the potential to automate disease diagnosis and treatment prognosis processes to help dental clinicians in making decisions more accurately and efficiently in a time-constrained environment. AI applications can further help in preventing human errors through their ability to learn and make automotive decisions. Different studies have been explored that incorporate the use of AI for orthodontic disease diagnosis and treatment planning which are shown in Table 5.
Table 5.
Summary of related studies for AI application in orthodontics.
Several authors have adopted machine learning techniques for disease diagnosis and treatment planning in the field of orthodontics. Chen et al. proposed a machine learning algorithm based on a multisource integration framework for assessing maxillary structures using CBCT images. The model achieved encouraging performance with a dice ratio of 0.80 in assessing maxillary structure variation in unilateral canine impaction [33]. An SVM-based algorithm was evaluated by Nino-Sandoval to classify skeletal patterns using craniomaxillary variables using cephalograms. The model achieved an accuracy of 74.5% in analyzing sagittal skeletal patterns [34]. Yu et al. investigated support vector regression (SVR) to rate facial attractiveness from most attractive to least attractive using colored photographs. It was found that the model can be used in finding a close correlation with facial attractiveness from orthodontic photographs with an accuracy of 71.8% [35]. Different studies explored the use of ML in treatment planning. Riri et al. proposed a tree-based classification method to identify facial and skin molds using intraoral and extraoral mold images. The model yielded an accuracy of 94.28% [37]. Suhail et al. proposed a random forest ensemble method to automate the extraction and treatment planning process. Based on patients’ medical health records, the model was able to make decisions for teeth extraction with an accuracy of 94.4% [38].
Literature addressed landmark detection problems as well using DL techniques. Song et al. evaluated a ResNet-50 model pre-trained using transfer learning on 400 cephalograms to detect cephalometric landmarks. The model achieved a superior SDR for two test cases in detecting 19 landmarks compared to two experienced doctors [60]. Kim et al. presented a two-stage deep neural network (DNN) with a stacked hourglass network for landmark detection using 2075 cephalograms followed by a web application. The model provided SDR of 82.92% and 84.53% for dataset 1 and dataset 2, respectively [65]. Gilmour et al. proposed pre-trained ResNet-50 with foveated pyramid attention algorithm achieving an SDR of 88.32% and 77.05% for dataset 1 and dataset 2, respectively [66]. Park et al. performed landmark detection using YOLOv3 on 1311 cephalograms. The model was effective in identifying 80 landmarks with 5% higher accuracy compared to top benchmarks. Moreover, attention-based networks have also been explored actively in landmark detection [61]. Zheng et al. explored attention guided deep regression model through a two-stage U-Net using 300 cephalograms. The model achieved an SDR of 86.74% which was higher compared to that of two experienced doctors [8]. Different deep learning-based methods have been employed for disease diagnosis. Makeremi et al. proposed a customized CNN to determine cervical vertebra maturation degree using cephalograms. The model achieved an accuracy of 95% helpful in determining the degree of maturation of CVM and has the potential to be implemented in real-world scenarios [68]. Yu et al. presented modified DenseNet pre-trained with ImageNet weights using lateral cephalograms. The model yielded an accuracy of 95.70% superior to that of five orthodontic specialists [69]. Deep learning for treatment planning has also gained attention in recent years. Lee et al. proposed a modified AlexNet for differential diagnosis in orthodontic surgery achieving an accuracy of 91.9% [62]. The study indicated that deep CNNs-based models can be applied for differential diagnosis in orthodontic surgery.
Different studies have explored ANNs as CDSS in orthodontics. Amasya et al. proposed ANN to diagnose cervical vertebra maturation degree using cephalograms. The model achieved an accuracy of 86.93% in CVM staging and cervical vertebral morphology classification [21]. Kok et al. proposed an ANN-based network to classify cervical vertebrae stages. It was found that ANN provided the most stable results with a 2.17 average rank on hand-wrist radiographs compared to an orthodontist [70]. Another ANN-based method was evaluated by Budiman using orthodontic scans to detect the shape of the arch form. The model achieved an accuracy of 76.32% [22]. In terms of treatment planning and prognosis, different studies explored the use of ANNs. Choi et al. proposed an ANN-based method for diagnosing and making surgery type and extraction decisions effectively [24].
3.4. AI in Restorative Dentistry and Prosthodontics
The number of studies exploring the use of AI in restorative dentistry has increased considerably in recent years. Different studies explored the use of AI in assisting the diagnosis of caries, and vertical tooth fracture, predicting restoration failure, and planning treatment. Table 6 shows the relevant studies for AI application in restorative dentistry to provide better dental treatment outcomes.
Table 6.
Summary of related studies for AI application in prosthetic/restorative dentistry.
The usefulness of AI in restorative dentistry has been investigated by several researchers. Lee et al. proposed a machine learning method based on a decision tree to determine tooth prognosis for effective treatment planning using clinical cases. The model achieved an accuracy of 84.1% [39]. A cubic SVM-based algorithm was proposed by Abdalla-Aslan et al. using panoramic radiographs. The model has the potential to detect and classify dental restorations to promote patients’ health [40].
Lee and Jeong proposed a fine-tuned and pre-trained deep CNN to diagnose dental implants using panoramic radiographs. The model yielded an AUC of 97.1% for the identification and classification of dental implants with performance similar to that of periodontists [54]. A deep CNN pre-trained with ImageNet weights was proposed by Takahashi et al. to diagnose partially edentulous arches achieving an accuracy of 99.5% for maxillar arches and 99.7% for mandible arches on oral photographs. The study showed that deep learning can be used effectively in designing removable partial dentures [71]. To preserve the teeth boundary, Xu et al. presented a two hierarchical CNN for segmentation of upper and lower teeth using 3D dental model images [72].
In terms of treatment planning and prognosis, ANNs have been utilized in different studies. Cui et al. proposed a triple classification algorithm based on extreme gradient boost (XGBoost). Using electronic health records, the model yielded an accuracy above 90% superior to that of prosthodontists in predicting tooth extracting therapy [25]. Another feed-forward ANN was presented by Javed et al. to identify occlusal dentinal caries lesions. The study proposed an iOS app for the meticulous prediction of caries using clinical cases [26].
3.5. AI in Oral Pathology
The relevant studies utilizing AI for disease diagnosis and prognosis are given in Table 7. Orhan et al. proposed a machine learning algorithm based on KNN and random forest using magnetic resonance images to diagnose temporomandibular disorders. The model achieved an accuracy of 77% in identifying condylar changes and 74% for disc displacement [36]. Hung et al. presented a three-step CNN-based on V-Net and SVR to identify maxillary sinusitis using CBCT images. The model yielded an AUC of 92% for mucosal thickening and 84% for mucous retention cyst identification [55].
Table 7.
Summary of related studies for AI application in oral pathology.
In a similar fashion, Kuwana et al. evaluated DetectNet on panoramic radiographs to detect maxillary sinus lesions with an accuracy of 90 to 91% for maxillary sinusitis and 97 to 100% for maxillary sinus cysts [56]. Moreover, a deep CNN (ResNet) was presented by Choi et al. to diagnose temporomandibular joint disorders (TMJ) osteoarthritis. The model yielded an accuracy of 78% similar to that of Oral and maxillofacial radiologists (OMFR) [58].
Kim et al. investigated the performance of CNN on water’s view radiographs to identify maxillary sinusitis. The model achieved significantly higher diagnostic performance compared to that of five radiologists [42]. Murata et al. evaluated the deep learning model AlexNet to diagnose maxillary sinusitis on panoramic radiographs. The model showed diagnostic performance similar to the radiologists and superior to the resident dentists [57]. Jeyaraj et al. proposed a partitioned CNN based on GoogleNet and InceptionV3 for diagnosing oral cancer using hyperspectral images. The model achieved an accuracy of 91.4% and 94.5% for benign and malign tissue respectively [59].
Clinical support decision systems have also been used in oral pathology. Iwasaki et al. proposed a Bayesian belief network (BNN) using magnetic resonance images to diagnose TMJ disorders. The model achieved an accuracy of 99% and can be used to determine the progression of TMD in terms of bone changes, disc displacement, and bony space by dental clinicians [27]. Moreover, a backpropagation ANN has been proposed by Bas et al. to identify clinical symptoms of TMJ disorders. It was found that the model can help diagnose the preliminary subtypes of TMJ and can be useful in the decision-making process [28].
4. Limitations and Future Direction
This study confirms the growing presence of AI in dentistry and highlights the performance of AI-based techniques as clinical support decision systems. Although AI techniques have been integrated increasingly into different subfields of dentistry, the current evidence of AI in clinical practice is still very limited. This section discusses the limitations and provides some future directions which may have a positive and stimulating impact on the future application of AI-based techniques in the field of dentistry.
4.1. Limitations
Although AI techniques have been employed increasingly within the field of dentistry, certain limitations need to be addressed to improve the performance, reliability, and generalizability of AI-based models. These limitations are discussed here
- Computational capability: AI-based techniques require a significant amount of parallel processing power to keep up with the demands. There are certain limitations of computational resources such as RAM and GPU cycles that are required to support such approaches.
- Reliability: It is essential in a clinical setting and involves ethical fairness, the accuracy of the system, and patients’ trust/acceptance of such systems. Limited reliability causes spurious consequences.
- Generalizability: Issues in generalizability are a dominant concern for clinical guidelines, and a precise level of generalizability is required for the application of AI-based models in clinical practices and ensuring that it performs well prospectively.
- Class imbalance: The difference in the number of samples representing each class within the data is referred to as class imbalance. The lack of high-quality and labeled datasets limits the deployment of robust and accurate AI-based models.
- Overfitting: Due to the high complexity in terms of parameters of deep learning models, the models are more likely to overfit with the training data, thus affecting the generalizability of the results.
The limitations of each relevant study covered in this review are given in Table 8 and Table 9. One of the most prevailing limitation in majority of the studies involving application of AI in subfields of dentistry is dataset limitation in terms of size for disease diagnosis [5,19,31,42,44,45,51,56,57,58,59,71], for treatment planning and prognosis [29,37,62], and for landmark detection [64]. Other limitations include relying on the reliability of examiners for accurate diagnosis [41], less flexibility to capture nonlinearities in data [23], limited practical use [54], poor performance on images that are not evenly illuminated [6], limited class discrimination [6], lack in terms of generalizability [29], lack in terms of performance [9,28,60,61,62,64,65,66,68,69], and computational capabilities [67].
Table 8.
Limitations of relevant studies employing AI for disease diagnosis.
Table 9.
Limitations of relevant studies employing AI for different treatment planning, landmark detection, and risk assessment.
4.2. Future Directions
Keeping in view the current limitations of studies employing AI for disease diagnosis, treatment planning and prognosis, landmark detection, and risk assessment, the following are a few research directions that can help in elevating the deep learning model’s performance, reliability, and generalizability:
4.2.1. Data Augmentation
Class-imbalanced datasets are biased towards majority classes, hence the chances for misclassification are often higher. However, different techniques can be employed to deal with the class imbalance and improve the performance of deep learning models. Certain techniques can be utilized to minimize class imbalance, such as data augmentation. To extract the increased amount of information from medical images, non-linear transformations can be applied. Generative adversarial networks (GANs) can prove to be a good alternative for creating similar images using non-linear transformations inside the network. Particularly, GANs are being used increasingly for medical data augmentation such as on pulmonary computed tomography (CT) images to detect COVID-19 lesions [73] and on small-scale medical image datasets [74]. To get a powerful variation of the generative model that can be employed to overcome the class imbalance in a more sophisticated way, known as balancing generative adversarial networks (BAGANs). It focuses on generating minority-class images of high quality.
4.2.2. Cross Center Training
One of the limitations of deep learning application in dentistry is the uncertainty about the generalizability of the models. Limited generalizability may be related to differences in terms of population characteristics such as dental status, and image characteristics such as differences in data generation protocols involved. Thus, understanding the reasons behind generalizability limitations will help in formulating strategies to mitigate generalizability problems. Further research should be focused on employing cross-center training [75] to increase the generalizability of deep learning-based models.
4.2.3. Robotics in Dentistry
Similar to other fields, dentistry is also moving forward toward a new era of data-driven medicine assisted by robots. Robotic dental assistance [76] has the potential to be applied to different fields including orthodontics, implant dentistry, and prosthodontics. To improve the applicability of AI in dentistry, more flexible systems are needed to reach human-level performance and further improve the reliability of AI-based models in clinical practice.
4.2.4. Virtual Reality and Augmented Reality
For practicing safe and efficient dentistry and gaining simultaneous feedback, virtual reality (VR) can be adopted. To generate clinical information that can be visualized by patients, augmented reality (AR) can be adopted. The use of AR and VR is increasing gradually, and there is a limited number of studies that assessed their use [77]. From providing better visualization to reducing operative time and improving patient consultation and providing promising treatment outcomes, AR and VR have the potential to enable researchers in developing high-quality tools for clinical practice. Clinicians can make use of AR to enable patients to visualize expected outcomes before undergoing the procedure. AR and VR can be employed to provide improved dental education by enhancing students’ learning experiences during pre-clinical training [78].
5. Discussion and Conclusion
It is suggested that the AI-based systems developed in recent years possess the potential to be employed in different fields of dentistry to help dental clinicians and practitioners in making precise diagnoses and providing accurate recommendations. However, AI is still unlikely to replace the dentist-patient relationship in the foreseeable future as humane elements are also of utmost importance in decision-making to manage dental care. The AI technologies are intended to support dental clinicians in reducing misdiagnosis and work synergistically with the unique abilities of dentists to provide enhanced, accessible care by taking away routine parts of dentists’ work.
Artificial intelligence has contributed substantially to different subfields of dentistry over the past decade. This review discusses numerous applications of AI in periodontology, endodontics, orthodontics, restorative dentistry, and oral pathology including studies incorporating deep learning to effectively diagnose dental disease and plan treatments. However, the current evidence of AI is still sparse due to limitations in terms of dataset availability, size, performance, and generalizability. This study highlights the limitations of the relevant studies and provides future directions which may have a positive impact on the future application of AI-based networks within dentistry. This review indicates that more flexible systems are needed to reach human-level performance and increase the reliability of AI-based clinical decision support systems in dental practice.
Author Contributions
Conceptualization, A.F. and I.S.; Data curation, A.F. and J.B.; Formal analysis, I.S., H.A. and I.D.L.T.D.; Funding acquisition, I.D.L.T.D.; Investigation, H.A. and J.C.M.E.; Methodology, I.S.; Project administration, J.B. and J.C.M.E.; Resources, I.D.L.T.D. and D.R.-S.M.L.; Software, D.R.-S.M.L. and J.B.; Supervision, I.A.; Validation, J.C.M.E. and I.A.; Visualization, D.R.-S.M.L.; Writing—original draft, A.F. and H.A.; Writing—review & editing, I.A. All authors have read and agreed to the published version of the manuscript.
Funding
This research was supported by the European University of the Atlantic.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Data is available from the authors on request.
Conflicts of Interest
The authors declare no conflict of interests.
References
- Haykin, S. Neural Networks and Learning Machines, 3/E; Pearson Education India: Noida, India, 2009. [Google Scholar]
- Basheer, I.A.; Hajmeer, M. Artificial neural networks: Fundamentals, computing, design, and application. J. Microbiol. Methods 2000, 43, 3–31. [Google Scholar] [CrossRef]
- Baxt, W.G. Application of artificial neural networks to clinical medicine. Lancet 1995, 346, 1135–1138. [Google Scholar] [CrossRef]
- Jain, A.K.; Mao, J.; Mohiuddin, K.M. Artificial neural networks: A tutorial. Computer 1996, 29, 31–44. [Google Scholar] [CrossRef]
- Krois, J.; Ekert, T.; Meinhold, L.; Golla, T.; Kharbot, B.; Wittemeier, A.; Dörfer, C.; Schwendicke, F. Deep learning for the radiographic detection of periodontal bone loss. Sci. Rep. 2019, 9, 8495. [Google Scholar] [CrossRef]
- Lin, P.; Huang, P.; Huang, P.; Hsu, H. Alveolar bone-loss area localization in periodontitis radiographs based on threshold segmentation with a hybrid feature fused of intensity and the H-value of fractional Brownian motion model. Comput. Methods Progr. Biomed. 2015, 121, 117–126. [Google Scholar] [CrossRef]
- Moran, M.B.H.; Faria, M.; Giraldi, G.; Bastos, L.; da Silva Inacio, B.; Conci, A. On using convolutional neural networks to classify periodontal bone destruction in periapical radiographs. In Proceedings of the 2020 IEEE International Conference on Bioinformatics and Biomedicine (BIBM), Seoul, Korea, 16–19 December 2020; pp. 2036–2039. [Google Scholar]
- Zheng, Z.; Yan, H.; Setzer, F.C.; Shi, K.J.; Mupparapu, M.; Li, J. Anatomically constrained deep learning for automating dental CBCT segmentation and lesion detection. IEEE Trans. Autom. Sci. Eng. 2020, 18, 603–614. [Google Scholar] [CrossRef]
- Shankarapillai, R.; Mathur, L.K.; Nair, M.A.; George, R. Periodontitis risk assessment using two artificial neural network algorithms—A comparative study. Int. J. Dental Clin. 2012, 4, 17–21. [Google Scholar]
- Carleo, G.; Cirac, I.; Cranmer, K.; Daudet, L.; Schuld, M.; Tishby, N.; Vogt-Maranto, L.; Zdeborová, L. Machine learning and the physical sciences. Rev. Mod. Phys. 2019, 91, 045002. [Google Scholar] [CrossRef]
- Hinton, G. Deep learning—A technology with the potential to transform health care. JAMA 2018, 320, 1101–1102. [Google Scholar] [CrossRef]
- Stead, W.W. Clinical implications and challenges of artificial intelligence and deep learning. JAMA 2018, 320, 1107–1108. [Google Scholar] [CrossRef]
- Park, W.J.; Park, J.B. History and application of artificial neural networks in dentistry. Eur. J. Dent. 2018, 12, 594–601. [Google Scholar] [CrossRef] [PubMed]
- Tundjungsari, V.; Sofro, A.S.M.; Sabiq, A.; Kardiana, A. Investigating clinical decision support systems success factors with usability testing. Int. J. Adv. Comput. Sci. Appl. 2017, 8. [Google Scholar] [CrossRef]
- Hajek, P. Fuzzy logic from the logical point of view. In Proceedings of the International Conference on Current Trends in Theory and Practice of Computer Science, Milovy, Czech Republic, 23 November–1 December 1995; pp. 31–49. [Google Scholar]
- Trillas, E.; Eciolaza, L. Fuzzy Logic; Springer International Publishing: Berlin, Germany, 2015; Volume 10, pp. 973–978. [Google Scholar]
- Collins, A.; Yao, Y. Machine learning approaches: Data integration for disease prediction and prognosis. In Applied Computational Genomics; Springer: Berlin/Heidelberg, Germany, 2018; pp. 137–141. [Google Scholar]
- Ossowska, A.; Kusiak, A.; Świetlik, D. Artificial Intelligence in Dentistry—Narrative Review. Int. J. Environ. Res. Public Health 2022, 19, 3449. [Google Scholar] [CrossRef] [PubMed]
- Geetha, V.; Aprameya, K.; Hinduja, D.M. Dental caries diagnosis in digital radiographs using back-propagation neural network. Health Inf. Sci. Syst. 2020, 8, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Kositbowornchai, S.; Plermkamon, S.; Tangkosol, T. Performance of an artificial neural network for vertical root fracture detection: An ex vivo study. Dental Traumatol. 2013, 29, 151–155. [Google Scholar] [CrossRef]
- Amasya, H.; Yildirim, D.; Aydogan, T.; Kemaloglu, N.; Orhan, K. Cervical vertebral maturation assessment on lateral cephalometric radiographs using artificial intelligence: Comparison of machine learning classifier models. Dentomaxillofac. Radiol. 2020, 49, 20190441. [Google Scholar] [CrossRef]
- Budiman, J.A. Neural network in developing software for Indentifying arch form. Int. J. Artif. Intell. Appl. 2013, 4, 1–11. [Google Scholar] [CrossRef]
- Papantonopoulos, G.; Takahashi, K.; Bountis, T.; Loos, B.G. Artificial neural networks for the diagnosis of aggressive periodontitis trained by immunologic parameters. PLoS ONE 2014, 9, e89757. [Google Scholar] [CrossRef]
- Choi, H.I.; Jung, S.K.; Baek, S.H.; Lim, W.H.; Ahn, S.J.; Yang, I.H.; Kim, T.W. Artificial intelligent model with neural network machine learning for the diagnosis of orthognathic surgery. J. Craniofac. Surg. 2019, 30, 1986–1989. [Google Scholar] [CrossRef]
- Cui, Q.; Chen, Q.; Liu, P.; Liu, D.; Wen, Z. Clinical decision support model for tooth extraction therapy derived from electronic dental records. J. Prosthet. Dent. 2021, 126, 83–90. [Google Scholar] [CrossRef]
- Javed, S.; Zakirulla, M.; Baig, R.U.; Asif, S.; Meer, A.B. Development of artificial neural network model for prediction of post-streptococcus mutans in dental caries. Comput. Methods Progr. Biomed. 2020, 186, 105198. [Google Scholar] [CrossRef] [PubMed]
- Iwasaki, H. Bayesian belief network analysis applied to determine the progression of temporomandibular disorders using MRI. Dentomaxillofac. Radiol. 2015, 44, 20140279. [Google Scholar] [CrossRef]
- Bas, B.; Ozgonenel, O.; Ozden, B.; Bekcioglu, B.; Bulut, E.; Kurt, M. Use of artificial neural network in differentiation of subgroups of temporomandibular internal derangements: A preliminary study. J. Oral Maxillofac. Surg. 2012, 70, 51–59. [Google Scholar] [CrossRef] [PubMed]
- Li, S.; Guo, Y.; Pang, Z.; Song, W.; Hao, A.; Xia, B.; Qin, H. Automatic Dental Plaque Segmentation Based on Local-to-Global Features Fused Self-Attention Network. IEEE J. Biomed. Health Inform. 2022, 26, 2240–2251. [Google Scholar] [CrossRef] [PubMed]
- Li, W.; Chen, Y.; Sun, W.; Brown, M.; Zhang, X.; Wang, S.; Miao, L. A gingivitis identification method based on contrast-limited adaptive histogram equalization, gray-level co-occurrence matrix, and extreme learning machine. Int. J. Imaging Syst. Technol. 2019, 29, 77–82. [Google Scholar] [CrossRef]
- Ghaedi, L.; Gottlieb, R.; Sarrett, D.C.; Ismail, A.; Belle, A.; Najarian, K.; Hargraves, R.H. An automated dental caries detection and scoring system for optical images of tooth occlusal surface. In Proceedings of the 2014 36th Annual International Conference of the IEEE Engineering in Medicine and Biology Society, Chicago, IL, USA, 26–30 August 2014; pp. 1925–1928. [Google Scholar]
- Berdouses, E.D.; Koutsouri, G.D.; Tripoliti, E.E.; Matsopoulos, G.K.; Oulis, C.J.; Fotiadis, D.I. A computer-aided automated methodology for the detection and classification of occlusal caries from photographic color images. Comput. Biol. Med. 2015, 62, 119–135. [Google Scholar] [CrossRef] [PubMed]
- Chen, S.; Wang, L.; Li, G.; Wu, T.H.; Diachina, S.; Tejera, B.; Kwon, J.J.; Lin, F.C.; Lee, Y.T.; Xu, T.; et al. Machine learning in orthodontics: Introducing a 3D auto-segmentation and auto-landmark finder of CBCT images to assess maxillary constriction in unilateral impacted canine patients. Angle Orthod. 2020, 90, 77–84. [Google Scholar] [CrossRef]
- Niño-Sandoval, T.C.; Perez, S.V.G.; Gonzalez, F.A.; Jaque, R.A.; Infante-Contreras, C. An automatic method for skeletal patterns classification using craniomaxillary variables on a Colombian population. Forens. Sci. Int. 2016, 261, 159-e1. [Google Scholar] [CrossRef]
- Yu, X.; Liu, B.; Pei, Y.; Xu, T. Evaluation of facial attractiveness for patients with malocclusion: A machine-learning technique employing Procrustes. Angle Orthod. 2014, 84, 410–416. [Google Scholar] [CrossRef]
- Orhan, K.; Driesen, L.; Shujaat, S.; Jacobs, R.; Chai, X. Development and validation of a magnetic resonance imaging-based machine learning model for TMJ pathologies. BioMed Res. Int. 2021, 2021, 6656773. [Google Scholar] [CrossRef]
- Riri, H.; Ed-Dhahraouy, M.; Elmoutaouakkil, A.; Beni-Hssane, A.; Bourzgui, F. Extracted features based multi-class classification of orthodontic images. Int. J. Electr. Comput. Eng. 2020, 10, 3558–3567. [Google Scholar] [CrossRef]
- Suhail, Y.; Upadhyay, M.; Chhibber, A. Machine learning for the diagnosis of orthodontic extractions: A computational analysis using ensemble learning. Bioengineering 2020, 7, 55. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.J.; Chung, D.; Asano, A.; Sasaki, D.; Maeno, M.; Ishida, Y.; Kobayashi, T.; Kuwajima, Y.; Da Silva, J.D.; Nagai, S. Diagnosis of Tooth Prognosis Using Artificial Intelligence. Diagnostics 2022, 12, 1422. [Google Scholar] [CrossRef] [PubMed]
- Abdalla-Aslan, R.; Yeshua, T.; Kabla, D.; Leichter, I.; Nadler, C. An artificial intelligence system using machine-learning for automatic detection and classification of dental restorations in panoramic radiography. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2020, 130, 593–602. [Google Scholar] [CrossRef]
- Lee, C.T.; Kabir, T.; Nelson, J.; Sheng, S.; Meng, H.W.; Van Dyke, T.E.; Walji, M.F.; Jiang, X.; Shams, S. Use of the deep learning approach to measure alveolar bone level. J. Clin. Periodontol. 2022, 49, 260–269. [Google Scholar] [CrossRef]
- Kim, Y.; Lee, K.J.; Sunwoo, L.; Choi, D.; Nam, C.M.; Cho, J.; Kim, J.; Bae, Y.J.; Yoo, R.E.; Choi, B.S.; et al. Deep Learning in Diagnosis of Maxillary Sinusitis Using Conventional Radiography. Investig. Radiol. 2019, 54, 7–15. [Google Scholar] [CrossRef]
- Lee, J.H.; Kim, D.H.; Jeong, S.N. Diagnosis of cystic lesions using panoramic and cone beam computed tomographic images based on deep learning neural network. Oral Dis. 2020, 26, 152–158. [Google Scholar] [CrossRef]
- Khan, H.A.; Haider, M.A.; Ansari, H.A.; Ishaq, H.; Kiyani, A.; Sohail, K.; Muhammad, M.; Khurram, S.A. Automated feature detection in dental periapical radiographs by using deep learning. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2021, 131, 711–720. [Google Scholar] [CrossRef]
- Duong, D.Q.; Nguyen, K.C.T.; Kaipatur, N.R.; Lou, E.H.M.; Noga, M.; Major, P.W.; Punithakumar, K.; Le, L.H. Fully Automated Segmentation of Alveolar Bone Using Deep Convolutional Neural Networks from Intraoral Ultrasound Images. In Proceedings of the 2019 41st Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Berlin, Germany, 23–27 July 2019; pp. 6632–6635. [Google Scholar]
- Nguyen, K.; Duong, D.; Almeida, F.; Major, P.; Kaipatur, N.; Pham, T.; Lou, E.; Noga, M.; Punithakumar, K.; Le, L. Alveolar Bone Segmentation in Intraoral Ultrasonographs with Machine Learning. J. Dental Res. 2020, 99, 1054–1061. [Google Scholar] [CrossRef]
- Pauwels, R.; Brasil, D.M.; Yamasaki, M.C.; Jacobs, R.; Bosmans, H.; Freitas, D.Q.; Haiter-Neto, F. Artificial intelligence for detection of periapical lesions on intraoral radiographs: Comparison between convolutional neural networks and human observers. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2021, 131, 610–616. [Google Scholar] [CrossRef]
- Orhan, K.; Bayrakdar, I.S.; Ezhov, M.; Kravtsov, A.; Özyürek, T. Evaluation of artificial intelligence for detecting periapical pathosis on cone-beam computed tomography scans. Int. Endod. J. 2020, 53, 680–689. [Google Scholar] [CrossRef] [PubMed]
- Fukuda, M.; Inamoto, K.; Shibata, N.; Ariji, Y.; Yanashita, Y.; Kutsuna, S.; Nakata, K.; Katsumata, A.; Fujita, H.; Ariji, E. Evaluation of an artificial intelligence system for detecting vertical root fracture on panoramic radiography. Oral Radiol. 2019, 36, 337–343. [Google Scholar] [CrossRef] [PubMed]
- Ekert, T.; Krois, J.; Meinhold, L.; Elhennawy, K.; Emara, R.; Golla, T.; Schwendicke, F. Deep Learning for the Radiographic Detection of Apical Lesions. J. Endod. 2019, 45, 917–922.e5. [Google Scholar] [CrossRef] [PubMed]
- Bayraktar, Y.; Ayan, E. Diagnosis of interproximal caries lesions with deep convolutional neural network in digital bitewing radiographs. Clin. Oral Investig. 2021, 26, 623–632. [Google Scholar] [CrossRef] [PubMed]
- Hiraiwa, T.; Ariji, Y.; Fukuda, M.; Kise, Y.; Nakata, K.; Katsumata, A.; Fujita, H.; Ariji, E. A deep-learning artificial intelligence system for assessment of root morphology of the mandibular first molar on panoramic radiography. Dentomaxillofac. Radiol. 2019, 48, 20180218. [Google Scholar] [CrossRef]
- Casalegno, F.; Newton, T.; Daher, R.; Abdelaziz, M.; Lodi-Rizzini, A.; Schürmann, F.; Krejci, I.; Markram, H. Caries Detection with Near-Infrared Transillumination Using Deep Learning. J. Dental Res. 2019, 98, 1227–1233. [Google Scholar] [CrossRef]
- Lee, J.H.; Jeong, S.N. Efficacy of deep convolutional neural network algorithm for the identification and classification of dental implant systems, using panoramic and periapical radiographs. Medicine 2020, 99, e20787. [Google Scholar] [CrossRef]
- Hung, K.F.; Ai, Q.Y.H.; King, A.D.; Bornstein, M.M.; Wong, L.M.; Leung, Y.Y. Automatic detection and segmentation of morphological changes of the maxillary sinus mucosa on cone-beam computed tomography images using a three-dimensional convolutional neural network. Clin. Oral Investig. 2022, 26, 3987–3998. [Google Scholar] [CrossRef]
- Kuwana, R.; Ariji, Y.; Fukuda, M.; Kise, Y.; Nozawa, M.; Kuwada, C.; Muramatsu, C.; Katsumata, A.; Fujita, H.; Ariji, E. Performance of deep learning object detection technology in the detection and diagnosis of maxillary sinus lesions on panoramic radiographs. Dentomaxillofac. Radiol. 2020, 50, 20200171. [Google Scholar] [CrossRef]
- Murata, M.; Ariji, Y.; Ohashi, Y.; Kawai, T.; Fukuda, M.; Funakoshi, T.; Kise, Y.; Nozawa, M.; Katsumata, A.; Fujita, H.; et al. Deep-learning classification using convolutional neural network for evaluation of maxillary sinusitis on panoramic radiography. Oral Radiol. 2018, 35, 301–307. [Google Scholar] [CrossRef]
- Choi, E.; Kim, D.; Lee, J.Y.; Park, H.K. Artificial intelligence in detecting temporomandibular joint osteoarthritis on orthopantomogram. Sci. Rep. 2021, 11, 10246. [Google Scholar] [CrossRef] [PubMed]
- Jeyaraj, P.R.; Nadar, E.R.S. Computer-assisted medical image classification for early diagnosis of oral cancer employing deep learning algorithm. J. Cancer Res. Clin. Oncol. 2019, 145, 829–837. [Google Scholar] [CrossRef] [PubMed]
- Song, Y.; Qiao, X.; Iwamoto, Y.; wei Chen, Y. Automatic Cephalometric Landmark Detection on X-ray Images Using a Deep-Learning Method. Appl. Sci. 2020, 10, 2547. [Google Scholar] [CrossRef]
- Park, J.H.; Hwang, H.W.; Moon, J.H.; Yu, Y.; Kim, H.; Her, S.B.; Srinivasan, G.; Aljanabi, M.N.A.; Donatelli, R.E.; Lee, S.J. Automated identification of cephalometric landmarks:Comparisons between the latest deep-learning methods YOLOV3 and SSD. Angle Orthod. 2019, 89, 903–909. [Google Scholar] [CrossRef]
- Lee, K.S.; Ryu, J.J.; Jang, H.S.; Lee, D.Y.; Jung, S.K. Deep Convolutional Neural Networks Based Analysis of Cephalometric Radiographs for Differential Diagnosis of Orthognathic Surgery Indications. Appl. Sci. 2020, 10, 2124. [Google Scholar] [CrossRef]
- Kim, J.; Lee, H.S.; Song, I.S.; Jung, K.H. DeNTNet: Deep Neural Transfer Network for the detection of periodontal bone loss using panoramic dental radiographs. Sci. Rep. 2019, 9, 17615. [Google Scholar] [CrossRef] [PubMed]
- Li, H.; Zhou, J.; Zhou, Y.; Chen, J.; Gao, F.; Xu, Y.; Gao, X. Automatic and interpretable model for periodontitis diagnosis in panoramic radiographs. In Proceedings of the International Conference on Medical Image Computing and Computer-Assisted Intervention, Lima, Peru, 4–8 October 2020; pp. 2454–2463. [Google Scholar]
- Kim, H.; Shim, E.; Park, J.; Kim, Y.J.; Lee, U.; Kim, Y. Web-based fully automated cephalometric analysis by deep learning. Comput. Methods Progr. Biomed. 2020, 194, 105513. [Google Scholar] [CrossRef]
- Gilmour, L.; Ray, N. Locating Cephalometric X-Ray Landmarks with Foveated Pyramid Attention. In Proceedings of the Third Conference on Medical Imaging with Deep Learning, Montreal, QC, Canada, 6–8 July 2020; Volume 121, pp. 262–276. [Google Scholar]
- Zhong, Z.; Li, J.; Zhang, Z.; Jiao, Z.; Gao, X. An Attention-Guided Deep Regression Model for Landmark Detection in Cephalograms. arXiv 2019, arXiv:1906.07549. [Google Scholar]
- Makaremi, M.; Lacaule, C.; Mohammad-Djafari, A. Deep Learning and Artificial Intelligence for the Determination of the Cervical Vertebra Maturation Degree from Lateral Radiography. Entropy 2019, 21, 1222. [Google Scholar] [CrossRef]
- Yu, H.; Cho, S.; Kim, M.; Kim, W.; Kim, J.; Choi, J. Automated Skeletal Classification with Lateral Cephalometry Based on Artificial Intelligence. J. Dental Res. 2020, 99, 249–256. [Google Scholar] [CrossRef]
- Kök, H.; Acilar, A.M.; İzgi, M.S. Usage and comparison of artificial intelligence algorithms for determination of growth and development by cervical vertebrae stages in orthodontics. Prog. Orthod. 2019, 20, 41. [Google Scholar] [CrossRef] [PubMed]
- Takahashi, T.; Nozaki, K.; Gonda, T.; Ikebe, K. A system for designing removable partial dentures using artificial intelligence. Part 1. Classification of partially edentulous arches using a convolutional neural network. J. Prosthodont. Res. 2021, 65, 115–118. [Google Scholar] [CrossRef] [PubMed]
- Xu, X.; Liu, C.; Zheng, Y. 3D Tooth Segmentation and Labeling Using Deep Convolutional Neural Networks. IEEE Trans. Vis. Comput. Graph. 2019, 25, 2336–2348. [Google Scholar] [CrossRef] [PubMed]
- Sedik, A.; Iliyasu, A.M.; El-Rahiem, B.A.; Samea, M.E.A.; Abdel-Raheem, A.; Hammad, M.; Peng, J.; El-Samie, F.E.A.; El-Latif, A.A.A. Deploying Machine and Deep Learning Models for Efficient Data-Augmented Detection of COVID-19 Infections. Viruses 2020, 12, 769. [Google Scholar] [CrossRef]
- Huang, G.; Jafari, A.H. Enhanced balancing GAN: Minority-class image generation. arXiv 2021, arXiv:2011.00189. [Google Scholar] [CrossRef]
- Krois, J.; Cantu, A.G.; Chaurasia, A.; Patil, R.; Chaudhari, P.K.; Gaudin, R.; Gehrung, S.; Schwendicke, F. Generalizability of deep learning models for dental image analysis. Sci. Rep. 2021, 11, 6102. [Google Scholar] [CrossRef]
- Grischke, J.; Johannsmeier, L.; Eich, L.; Griga, L.; Haddadin, S. Dentronics: Towards robotics and artificial intelligence in dentistry. Dental Mater. 2020, 36, 765–778. [Google Scholar] [CrossRef]
- Fahim, S.; Maqsood, A.; Das, G.; Ahmed, N.; Saquib, S.; Lal, A.; Khan, A.A.G.; Alam, M.K. Augmented Reality and Virtual Reality in Dentistry: Highlights from the Current Research. Appl. Sci. 2022, 12, 3719. [Google Scholar] [CrossRef]
- Monterubbianesi, R.; Tosco, V.; Vitiello, F.; Orilisi, G.; Fraccastoro, F.; Putignano, A.; Orsini, G. Augmented, Virtual and Mixed Reality in Dentistry: A Narrative Review on the Existing Platforms and Future Challenges. Appl. Sci. 2022, 12, 877. [Google Scholar] [CrossRef]


Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).