

Underreporting and Triggering Factors for Reporting ADRs of Two Ophthalmic Drugs: A Comparison between Spontaneous Reports and Active Pharmacovigilance Databases

 ,
, 
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Spontaneous Reporting
2.3. Active Surveillance Reporting
2.4. Categorization
2.5. Calculating Defined Daily Dose Indicators
2.6. Factors Related to Reporting
2.7. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Santoro, A.; Genov, G.; Spooner, A.; Raine, J.; Arlett, P. Promoting and Protecting Public Health: How the European Union Pharmacovigilance System Works. Drug Saf. 2017, 40, 855–869. [Google Scholar] [CrossRef] [PubMed]
- Montastruc, J.-L.; Benevent, J.; Montastruc, F.; Bagheri, H.; Despas, F.; Lapeyre-Mestre, M.; Sommet, A. What Is Pharmacoepidemiology? Definition, Methods, Interest and Clinical Applications. Therapie 2019, 74, 169–174. [Google Scholar] [CrossRef]
- Aronson, J.K. Post-Marketing Drug Withdrawals: Pharmacovigilance Success, Regulatory Problems. Therapie 2017, 72, 555–561. [Google Scholar] [CrossRef] [PubMed]
- Mazzitello, C.; Esposito, S.; De Francesco, A.; Capuano, A.; Russo, E.; De Sarro, G. Pharmacovigilance in Italy: An Overview. J. Pharmacol. Pharmacother. 2013, 4, 20–28. [Google Scholar] [CrossRef] [PubMed]
- Inácio, P.; Cavaco, A.; Airaksinen, M. The Value of Patient Reporting to the Pharmacovigilance System: A Systematic Review. Br. J. Clin. Pharmacol. 2017, 83, 227–246. [Google Scholar] [CrossRef]
- Wise, L.; Parkinson, J.; Raine, J.; Breckenridge, A. New Approaches to Drug Safety: A Pharmacovigilance Tool Kit. Nat. Rev. Drug Discov. 2009, 8, 779–782. [Google Scholar] [CrossRef]
- World Health Organization. A Practical Handbook on the Pharmacovigilance of Medicines Used in the Treatment of Tuberculosis: Enhancing the Safety of the TB Patient; World Health Organization: Geneva, Switzerland, 2012. [Google Scholar]
- Yun, I.S.; Koo, M.J.; Park, E.H.; Kim, S.-E.; Lee, J.-H.; Park, J.-W.; Hong, C.-S. A Comparison of Active Surveillance Programs Including a Spontaneous Reporting Model for Phamacovigilance of Adverse Drug Events in a Hospital. Korean J. Intern. Med. 2012, 27, 443–450. [Google Scholar] [CrossRef]
- Jacob, D.; Marrón, B.; Ehrlich, J.; Rutherford, P.A. Pharmacovigilance as a Tool for Safety and Monitoring: A Review of General Issues and the Specific Challenges with End-Stage Renal Failure Patients. Drug. Healthc. Patient Saf. 2013, 5, 105–112. [Google Scholar] [CrossRef]
- Hazell, L.; Shakir, S.A.W. Under-Reporting of Adverse Drug Reactions: A Systematic Review. Drug Saf. 2006, 29, 385–396. [Google Scholar] [CrossRef]
- Khalili, M.; Mesgarpour, B.; Sharifi, H.; Golozar, A.; Haghdoost, A.A. Estimation of Adverse Drug Reaction Reporting in Iran: Correction for Underreporting. Pharmacoepidemiol. Drug Saf. 2021, 30, 1101–1114. [Google Scholar] [CrossRef]
- Mann, M.; Mengistu, A.; Gaeseb, J.; Sagwa, E.; Mazibuko, G.; Babigumira, J.B.; Garrison, L.P.J.; Stergachis, A. Active Surveillance versus Spontaneous Reporting for First-Line Antiretroviral Medicines in Namibia: A Cost-Utility Analysis. Drug Saf. 2016, 39, 859–872. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. The Use of the WHO-UMC System for Standardised Case Causality Assessment; World Health Organization: Geneva, Switzerland, 2013. [Google Scholar]
- Hartwig, S.C.; Siegel, J.; Schneider, P.J. Preventability and Severity Assessment in Reporting Adverse Drug Reactions. Am. J. Hosp. Pharm. 1992, 49, 2229–2232. [Google Scholar] [CrossRef] [PubMed]
- Petrova, G.; Stoimenova, A.; Dimitrova, M.; Kamusheva, M.; Petrova, D.; Georgiev, O. Assessment of the Expectancy, Seriousness and Severity of Adverse Drug Reactions Reported for Chronic Obstructive Pulmonary Disease Therapy. SAGE Open Med. 2017, 5, 2050312117690404. [Google Scholar] [CrossRef] [PubMed]
- European Medicines Agency. Guideline on Good Pharmacovigilance Practices (GVP); European Medicines Agency: London, UK, 2014. [Google Scholar]
- World Health Organization. DDD Indicators. Available online: https://www.who.int/tools/atc-ddd-toolkit/indicators (accessed on 9 March 2022).
- Liu, R.; Zhang, P. Towards Early Detection of Adverse Drug Reactions: Combining Pre-Clinical Drug Structures and Post-Market Safety Reports. BMC Med. Inform. Decis. Mak. 2019, 19, 279. [Google Scholar] [CrossRef]
- Yawson, A.A.; Abekah-Nkrumah, G.; Okai, G.A.; Ofori, C.G. Awareness, Knowledge, and Attitude toward Adverse Drug Reaction (ADR) Reporting among Healthcare Professionals in Ghana. Ther. Adv. drug Saf. 2022, 13, 20420986221116468. [Google Scholar] [CrossRef]
- Fraunfelder, F.W.; Fraunfelder, F.T. Scientific Challenges in Postmarketing Surveillance of Ocular Adverse Drug Reactions. Am. J. Ophthalmol. 2007, 143, 145–149. [Google Scholar] [CrossRef]
- Miguel, A.; Henriques, F.; Azevedo, L.F.; Pereira, A.C. Ophthalmic Adverse Drug Reactions to Systemic Drugs: A Systematic Review. Pharmacoepidemiol. Drug Saf. 2014, 23, 221–233. [Google Scholar] [CrossRef]
- Hughes, M.L.; Weiss, M. Adverse Drug Reaction Reporting by Community Pharmacists-The Barriers and Facilitators. Pharmacoepidemiol. Drug Saf. 2019, 28, 1552–1559. [Google Scholar] [CrossRef]
- Kitisopee, T.; Assanee, J.; Sorofman, B.A.; Watcharadmrongkun, S. Consumers’ Adverse Drug Event Reporting via Community Pharmacists: Three Stakeholder Perception. J. Pharm. Policy Pract. 2022, 15, 19. [Google Scholar] [CrossRef]
- Syed, A.; Azhar, S.; Raza, M.M.; Saeed, H.; Jamshed, S.Q. Assessment of Knowledge, Attitude and Barriers towards Pharmacovigilance among Physicians and Pharmacists of Abbottabad, Pakistan. Pharmacy 2018, 6, 29. [Google Scholar] [CrossRef]
- Li, R.; Curtain, C.; Bereznicki, L.; Zaidi, S.T.R. Community Pharmacists’ Knowledge and Perspectives of Reporting Adverse Drug Reactions in Australia: A Cross-Sectional Survey. Int. J. Clin. Pharm. 2018, 40, 878–889. [Google Scholar] [CrossRef] [PubMed]
- Al Dweik, R.; Stacey, D.; Kohen, D.; Yaya, S. Factors Affecting Patient Reporting of Adverse Drug Reactions: A Systematic Review. Br. J. Clin. Pharmacol. 2017, 83, 875–883. [Google Scholar] [CrossRef]
- Brabete, A.C.; Greaves, L.; Maximos, M.; Huber, E.; Li, A.; Lê, M.-L. A Sex- and Gender-Based Analysis of Adverse Drug Reactions: A Scoping Review of Pharmacovigilance Databases. Pharmaceuticals 2022, 15, 298. [Google Scholar] [CrossRef] [PubMed]
- Zucker, I.; Prendergast, B.J. Sex Differences in Pharmacokinetics Predict Adverse Drug Reactions in Women. Biol. Sex Differ. 2020, 11, 32. [Google Scholar] [CrossRef] [PubMed]
- Contreras-Salinas, H.; Baiza-Durán, L.M.; Barajas-Hernández, M.; Vázquez-Álvarez, A.O.; Rodríguez-Herrera, L.Y. A Drug Safety Surveillance Study of a Ciprofloxacin/Dexamethasone Ophthalmic Fixed Combination in Peruvian Population. Pharmacy 2021, 9, 15. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Drug | Time | ADRs | DDD | Use in DDD | ADRs per 10,000 DDDs |
|---|---|---|---|---|---|
| Antiglaucoma | 2005 days | 75 | 0.14 mL | 195,334,179 | 0.003840 |
| Artificial tears | 2005 days | 26 | 0.54 mL | 133,029,769 | 0.001955 |
| Drug | Time | Patients | ADRs | DDD | Use in DDD | ADRs per 10,000 DDDs |
|---|---|---|---|---|---|---|
| Antiglaucoma | 60 days | 246 | 94 | 0.14 mL | 14,760 | 63.68563686 |
| Artificial tears | 30 days | 212 | 35 | 0.54 mL | 6360 | 55.03144654 |
| Antiglaucoma | Artificial Tears | ||||
|---|---|---|---|---|---|
| AS, n (%) | SN, n (%) | AS, n (%) | SN, n (%) | ||
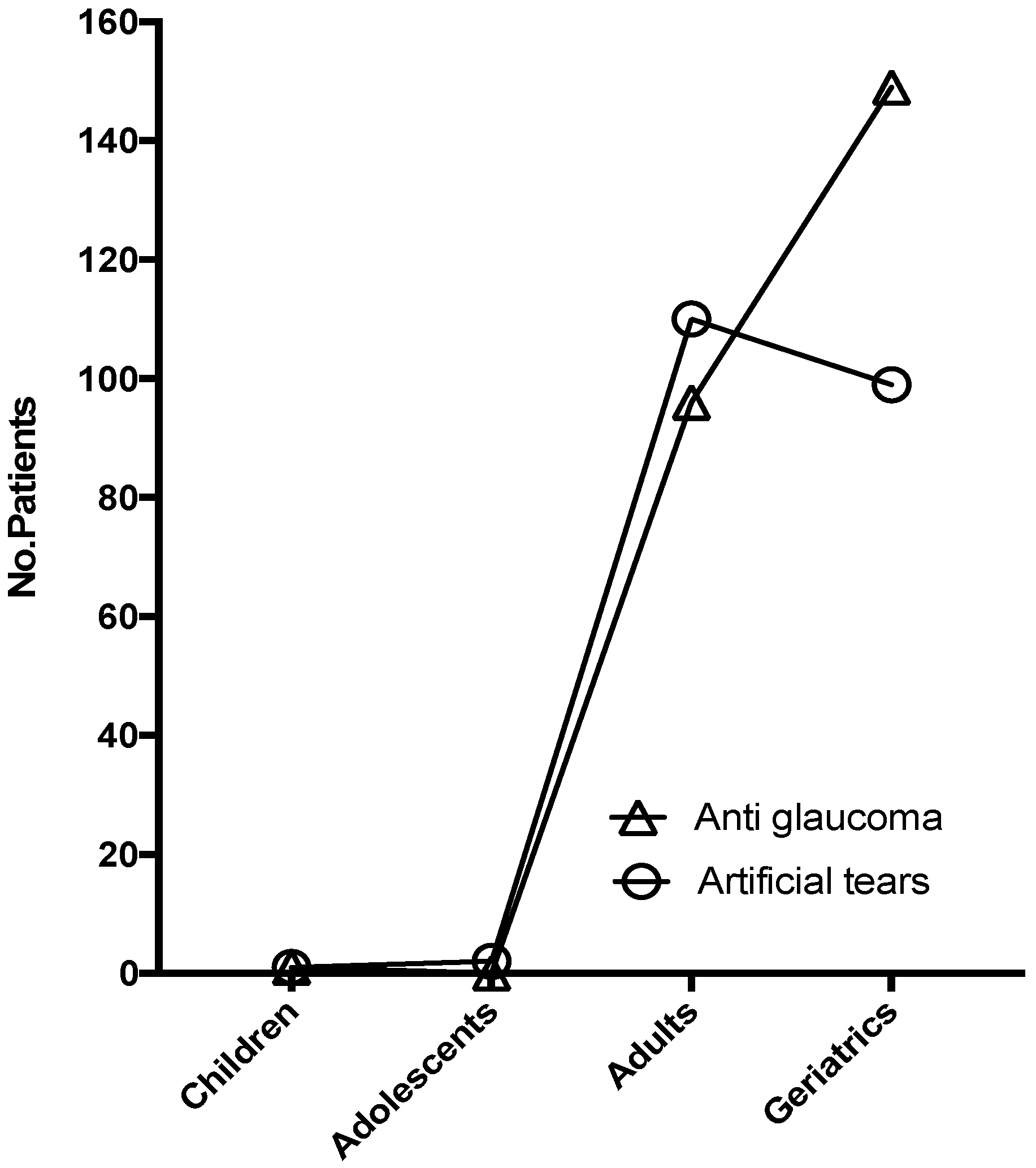
| Age group | Children | 0 (0) | 1 (1.3) | 0 (0) | 0 (0) |
| Adolescents | 0 (0) | 0 (0) | 0 (0) | 0 (0) | |
| Adults | 43 (45.7) | 16 (21.3) | 22 (62.9) | 18 (69.2) | |
| Geriatrics | 51 (54.3) | 52 (69.4) | 13 (37.1) | 4 (15.4) | |
| Unknown | 0 (0) | 6 (8) | 0 (0) | 4 (15.4) | |
| Gender | Male | 38 (40.4) | 30 (40.0) | 15 (42.9) | 8 (30.8) |
| Female | 56 (59.6) | 45 (60.0) | 20 (57.1) | 14 (53.8) | |
| Unknown | 0 (0) | 0 (0) | 0 (0) | 4 (15.4) | |
| Severity | Mild | 94 (100) | 51 (68.0) | 35 (100) | 17 (65.4) |
| Moderate | 0 (0) | 16 (21.3) | 0 (0) | 5 (19.2) | |
| Severe | 0 (0) | 2 (2.7) | 0 (0) | 0 (0) | |
| Unknown | 0 (0) | 6 (8) | 0 (0) | 4 (15.4) | |
| Seriousness | Not-Serious | 94 (100) | 73 (97.3) | 35 (100) | 22 (84.6) |
| Serious | 0 (0) | 2 (2.7) | 0 (0) | 0 (0) | |
| Unknown | 0 (0) | 0 (0) | 0 (0) | 4 (15.4) | |
| Total | ADRs | 94 | 75 | 35 | 26 |
| Antiglaucoma | |||
|---|---|---|---|
| PT | Labeled * | AS, n (%) | SN, n (%) |
| Eye irritation | Y | 76 (80.9) | 19 (25.3) |
| Vision blurred | Y | 5 (5.3) | 6 (8.0) |
| Lacrimation increased | Y | 0 (0) | 5 (6.7) |
| Eye pain | Y | 1 (1.1) | 4 (5.3) |
| Eye inflammation | Y | 0 (0) | 4 (5.3) |
| Headache | N | 1 (1.1) | 3 (4.0) |
| Ocular hyperaemia | Y | 1 (1.1) | 3 (4.0) |
| Eye pruritus | Y | 3 (3.2) | 2 (2.7) |
| Somnolence | Y | 1 (1.1) | 2 (2.7) |
| Blood pressure decreased | Y | 1 (1.1) | 2 (2.7) |
| Diffuse alopecia | N | 0 (0) | 2 (2.7) |
| Eyelid skin dryness | N | 0 (0) | 2 (2.7) |
| Cough | N | 0 (0) | 2 (2.7) |
| Dysgeusia | Y | 2 (2.1) | 1 (1.3) |
| Dry mouth | Y | 1 (1.1) | 1 (1.3) |
| Arthralgia | N | 0 (0) | 1 (1.3) |
| Eye allergy | Y | 0 (0) | 1 (1.3) |
| Asthenopia | N | 0 (0) | 1 (1.3) |
| Blepharitis | Y | 0 (0) | 1 (1.3) |
| Nasal congestion | Y | 0 (0) | 1 (1.3) |
| Neck pain | N | 0 (0) | 1 (1.3) |
| Musculoskeletal pain | N | 0 (0) | 1 (1.3) |
| Administration site oedema | Y | 0 (0) | 1 (1.3) |
| Eye discharge | N | 0 (0) | 1 (1.3) |
| Photophobia | Y | 0 (0) | 1 (1.3) |
| Rash maculo-papular | N | 0 (0) | 1 (1.3) |
| Periorbital swelling | N | 0 (0) | 1 (1.3) |
| Hyperhidrosis | N | 0 (0) | 1 (1.3) |
| Nephrostomy | N | 0 (0) | 1 (1.3) |
| Nasal obstruction | N | 0 (0) | 1 (1.3) |
| Pruritus allergic | Y | 0 (0) | 1 (1.3) |
| Rhinorrhoea | Y | 0 (0) | 1 (1.3) |
| Nasopharyngitis | N | 2 (2.1) | 0 (0) |
| Artificial Tears | |||
|---|---|---|---|
| PT | Labeled * | AS, n (%) | SN, n (%) |
| Burning sensation | Y | 26 (74.3) | 11 (42.3) |
| Vision blurred | Y | 7 (20) | 2 (7.7) |
| Ocular hyperaemia | N | 0 (0) | 2 (7.7) |
| Lacrimation increased | N | 0 (0) | 2 (7.7) |
| Ageusia | N | 0 (0) | 1 (3.8) |
| Visual impairment | N | 0 (0) | 1 (3.8) |
| Anosmia | N | 0 (0) | 1 (3.8) |
| Dry eye | N | 0 (0) | 1 (3.8) |
| Eye pruritus | N | 0 (0) | 1 (3.8) |
| Instillation site discharge | N | 0 (0) | 1 (3.8) |
| Eye discharge | N | 0 (0) | 1 (3.8) |
| Abnormal sensation in eye | N | 0 (0) | 1 (3.8) |
| Foreign body sensation in eyes | N | 0 (0) | 1 (3.8) |
| Ocular pain | N | 1 (2.9) | 0 (0) |
| Headache | N | 1 (2.9) | 0 (0) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Contreras-Salinas, H.; Baiza-Durán, L.M.; Bautista-Castro, M.A.; Alonso-Rodríguez, D.R.; Rodríguez-Herrera, L.Y. Underreporting and Triggering Factors for Reporting ADRs of Two Ophthalmic Drugs: A Comparison between Spontaneous Reports and Active Pharmacovigilance Databases. Healthcare 2022, 10, 2182. https://doi.org/10.3390/healthcare10112182
Contreras-Salinas H, Baiza-Durán LM, Bautista-Castro MA, Alonso-Rodríguez DR, Rodríguez-Herrera LY. Underreporting and Triggering Factors for Reporting ADRs of Two Ophthalmic Drugs: A Comparison between Spontaneous Reports and Active Pharmacovigilance Databases. Healthcare. 2022; 10(11):2182. https://doi.org/10.3390/healthcare10112182
Chicago/Turabian StyleContreras-Salinas, Homero, Leopoldo Martín Baiza-Durán, Manuel Alejandro Bautista-Castro, Diego Rodrigo Alonso-Rodríguez, and Lourdes Yolotzin Rodríguez-Herrera. 2022. "Underreporting and Triggering Factors for Reporting ADRs of Two Ophthalmic Drugs: A Comparison between Spontaneous Reports and Active Pharmacovigilance Databases" Healthcare 10, no. 11: 2182. https://doi.org/10.3390/healthcare10112182
APA StyleContreras-Salinas, H., Baiza-Durán, L. M., Bautista-Castro, M. A., Alonso-Rodríguez, D. R., & Rodríguez-Herrera, L. Y. (2022). Underreporting and Triggering Factors for Reporting ADRs of Two Ophthalmic Drugs: A Comparison between Spontaneous Reports and Active Pharmacovigilance Databases. Healthcare, 10(11), 2182. https://doi.org/10.3390/healthcare10112182