
Education/Training Interventions to Improve Oral Health of Adults with Intellectual Disability


Abstract
1. Introduction
- Oral health education/training interventions for adults with intellectual disability that target dental health professionals. (Dental health professionals diagnose and treat diseases of the teeth, gums, and mouth, including the prevention of dental diseases. They include dentists, dental hygienists, dental therapists, dental prosthetists, and oral health therapists);
- Education/training programs about the importance of oral health for adults with intellectual disability, which target non-dental health professionals who support people with intellectual disability. (Non-dental health professionals include general medical practitioners, nurses, diabetes educators, speech pathologists, pharmacists, midwives, etc. Non-dental health professionals could provide oral health promotion, temporary relief of oral symptoms and referral rather than definitive treatment due to lack of oral health training and scope of practice limitations);
- Education/training programs about the importance of oral health that target adults with intellectual disability;
- Education/training programs relating to oral health interventions that target primary carers and support workers of adults with intellectual disability.
2. Materials and Methods
2.1. Inclusion Criteria
2.2. Exclusion Criteria
2.3. Literature Search
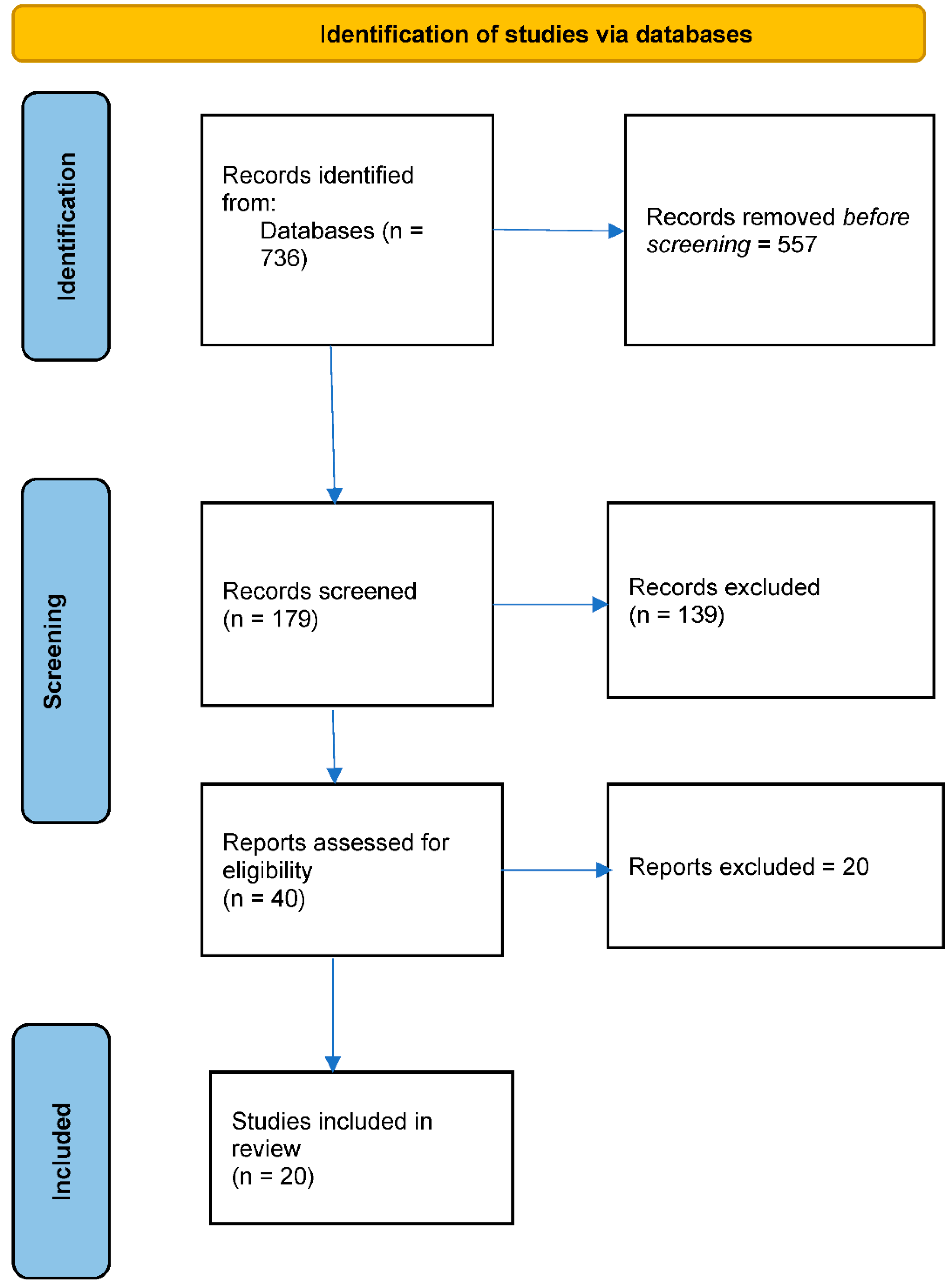
2.4. Study Selection
3. Results
3.1. Characteristics of Participants
3.2. Interventions
3.3. Synthesis of Results
3.3.1. Objective 1: Education/Training-Related Interventions for Dental Health Professionals
3.3.2. Category 1: Experimental Studies
3.3.3. Category 2: Exploratory Studies
3.3.4. Objective 2: Education/Training-Related Interventions for Non-Dental Professionals
3.3.5. Objective 3: Education/Training-Related Interventions for People with Intellectual Disability
3.3.6. Objective 4: Education/Training-Related Interventions for Carers of People with Intellectual Disability
4. Discussion
4.1. Implications for Research, Policy, and Practice
4.2. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Wilson, N.J.; Lin, Z.; Villarosa, A.; Lewis, P.; Philip, P.; Sumar, B.; George, A. Countering the poor oral health of people with intellectual and developmental disability: A scoping literature review. BMC Public Health 2019, 19, 1530. [Google Scholar] [CrossRef] [PubMed]
- Hillebrecht, A.-L.; Hrasky, V.; Anten, C.; Wiegand, A. Changes in the oral health-related quality of life in adult patients with intellectual disabilities after dental treatment under general anesthesia. Clin. Oral Investig. 2019, 23, 3895–3903. [Google Scholar] [CrossRef] [PubMed]
- Couto, P.; Pereira, P.A.; Nunes, M.; Mendes, R.A. Oral health-related quality of life of Portuguese adults with mild intellectual disabilities. PLoS ONE 2018, 13, e0193953. [Google Scholar] [CrossRef] [PubMed]
- Masood, M.; Newton, J.T.; Bakri, N.N.; Khalid, T.; Masood, Y. The relationship between oral health and oral health related quality of life among elderly people in United Kingdom. J. Dent. 2017, 56, 78–83. [Google Scholar] [CrossRef]
- Sischo, L.; Broder, H.L. Oral Health-related Quality of Life: What, Why, How, and Future Implications. J. Dent. Res. 2011, 90, 1264–1270. [Google Scholar] [CrossRef]
- Aida, J.; Kondo, K.; Yamamoto, T.; Hirai, H.; Nakade, M.; Osaka, K.; Sheiham, A.; Tsakos, G.; Watt, R.G. Oral Health and Cancer, Cardiovascular, and Respiratory Mortality of Japanese. J. Dent. Res. 2011, 90, 1129–1135. [Google Scholar] [CrossRef]
- Lamster, I.B. Diabetes Mellitus and Oral Health: An Interprofessional Approach; John Wiley & Sons, Inc.: Hoboken, NJ, USA, 2014. [Google Scholar]
- Wu, B.; Fillenbaum, G.G.; Plassman, B.L.; Guo, L. Association between Oral Health and Cognitive Status: A Systematic Review. J. Am. Geriatr. Soc. 2016, 64, 739–751. [Google Scholar] [CrossRef]
- Holmlund, A.; Lampa, E.; Lind, L. Oral health and cardiovascular disease risk in a cohort of periodontitis patients. Atherosclerosis 2017, 262, 101–106. [Google Scholar] [CrossRef]
- World Health Organization. Disability and Health. 2022. Available online: https://www.who.int/news-room/fact-sheets/detail/disability-and-health (accessed on 12 May 2022).
- United Nations. Convention on the Rights of Persons with Disabilities. 2006. Available online: https://www.un.org/development/desa/disabilities/convention-on-the-rights-of-persons-with-disabilities.html (accessed on 27 April 2018).
- Anders, P.L.; Davis, E. Oral health of patients with intellectual disabilities: A systematic review. Spéc. Care Dent. 2010, 30, 110–117. [Google Scholar] [CrossRef]
- Australian Institute of Health and Welfare. Oral Health of Adults in the Public Dental Sector; Australian Institute of Health and Welfare, Australian Government Department of Health: Bruce, Australia, 2017.
- Cumella, S.; Ransford, N.; Lyons, J.; Burnham, H. Needs for oral care among people with intellectual disability not in contact with Community Dental Services. J. Intellect. Disabil. Res. 2000, 44, 45–52. [Google Scholar] [CrossRef]
- Glick, M. The Oral-Systemic Health Connection: A Guide to Patient Care, 2nd ed.; International Quin-Tessence Publishing Group: Berlin, Germany, 2019. [Google Scholar]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. Syst. Rev. 2021, 10, 89. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.J.; Welch, V.A. (Eds.) Cochrane Handbook for Systematic Reviews of Interventions Version 6.3 (Updated February 2022); Cochrane: London, UK, 2022; Available online: www.training.cochrane.org/handbook (accessed on 7 October 2022).
- Ahmad, M.S.; Razak, I.A.; Borromeo, G.L. Special Needs Dentistry: Perception, attitudes and educational experience of Malaysian dental students. Eur. J. Dent. Educ. 2014, 19, 44–52. [Google Scholar] [CrossRef] [PubMed]
- Catteau, C.; Faulks, D.; Mishellany-Dutour, A.; Collado, V.; Tubert-Jeannin, S.; Tardieu, C.; Hugues, P.; Roger-Leroi, V.; Hennequin, M. Using e-learning to train dentists in the development of standardised oral health promotion interventions for persons with disability. Eur. J. Dent. Educ. 2013, 17, 143–153. [Google Scholar] [CrossRef] [PubMed]
- Dellavia, C.; Allievi, C.; Ottolina, P.; Sforza, C. Special care dentistry for people with intellectual disability in dental education: An Italian experience. Eur. J. Dent. Educ. 2009, 13, 218–222. [Google Scholar] [CrossRef]
- Faulks, D.; Dougall, A.; Ting, G.; Ari, T.; Nunn, J.; Friedman, C.; John, J.; Daly, B.; Roger-Leroi, V.; Newton, J.T. Development of a battery of tests to measure attitudes and intended behaviours of dental students towards people with disability or those in marginalised groups. Eur. J. Dent. Educ. 2017, 22, e278–e290. [Google Scholar] [CrossRef] [PubMed]
- Isobe, A.; Izumi, M.; Akifusa, S. Attitudes towards people with dementia: A cross-sectional study comparing dental hygiene students with registered dental hygienists. Gerodontology 2019, 36, 45–54. [Google Scholar] [CrossRef]
- Phadraig, C.M.G.; Guerin, S.; Nunn, J. Should we educate care staff to improve the oral health and oral hygiene of people with intellectual disability in residential care? Real world lessons from a randomized controlled trial. Spéc. Care Dent. 2015, 35, 92–98. [Google Scholar] [CrossRef]
- Mohebbi, S.Z.; Chinipardaz, Z.; Batebi, A. Effectiveness of training senior dental students on oral health care for disabled patients. Eur. J. Dent. Educ. 2014, 18, 214–221. [Google Scholar] [CrossRef] [PubMed]
- Jones, D.M.; Miller, S.R. Effectiveness of an Educational Module on Dental Hygiene Students’ Attitudes Towards Persons with Disabilities. J. Dent. Hyg. 2018, 92, 27–34. [Google Scholar]
- Nagarajappa, R.; Tak, M.; Sharda, A.J.; Asawa, K.; Jalihal, S.; Kakatkar, G. Dentists’ attitude to provision of care for people with learning disabilities in Udaipur, India. Scand. J. Caring Sci. 2012, 27, 57–62. [Google Scholar] [CrossRef]
- Smith, G.; Rooney, Y.; Nunn, J. Provision of dental care for special care patients: The view of Irish dentists in the Republic of Ireland. J. Ir. Dent. Assoc. 2010, 56, 80–84. [Google Scholar] [PubMed]
- Phadraig, C.M.G.; Nunn, J.; Guerin, S.; Normand, C. Should we provide oral health training for staff caring for people with intellectual disabilities in community based residential care? A cost-effectiveness analysis. Eval. Program Plan. 2016, 55, 46–54. [Google Scholar] [CrossRef]
- Mac Giolla Phadraig, C.; Nunn, J.H.; Tornsey, O.; Timms, M. Does Special Care Dentistry undergraduate teaching improve dental student attitudes towards people with disabilities? Eur. J. Dent. Educ. 2015, 19, 107–112. [Google Scholar] [CrossRef] [PubMed]
- Blaizot, A.; Catteau, C.; Delfosse, C.; Hamel, O.; Trentesaux, T. Obstacles to comprehensive dental care in patients with sustained limitations of their decision-making abilities: Findings from a Delphi study. Eur. J. Oral Sci. 2018, 126, 222–233. [Google Scholar] [CrossRef] [PubMed]
- Lees, C.; Poole, H.; Brennan, M.; Irvine, F. Adults with learning disabilities experiences of using community dental services: Service user and carer perspectives. Br. J. Learn. Disabil. 2017, 45, 114–120. [Google Scholar] [CrossRef]
- Phadraig, C.M.G.; Dougall, A.; Stapleton, S.; McGeown, D.; Nunn, J.; Guerin, S. What should dental services for people with disabilities in Ireland be like? Agreed priorities from a focus group of people with learning disabilities. Br. J. Learn. Disabil. 2015, 44, 259–268. [Google Scholar] [CrossRef]
- Eijsink, A.; Schipper, G.; Vermaire, J. AQ-methodology study among caregivers of people with moderate intellectual disabilities on their clients’ health care: An example in oral health. J. Appl. Res. Intellect. Disabil. 2018, 31, 915–926. [Google Scholar] [CrossRef]
- Pradhan, A.; Keuskamp, D.; Brennan, D. Pre-and post-training evaluation of dental efficacy and activation measures in carers of adults with disabilities in South Australia—A pilot study. Health Soc. Care Community 2016, 24, 739–746. [Google Scholar] [CrossRef] [PubMed]
- Phadraig, C.M.G.; Guerin, S.; Nunn, J. Train the trainer? A randomized controlled trial of a multi-tiered oral health education programme in community-based residential services for adults with intellectual disability. Community Dent. Oral Epidemiol. 2012, 41, 182–192. [Google Scholar] [CrossRef]
- Phlypo, I.; De Tobel, J.; Marks, L.; De Visschere, L.; Koole, S. Integrating community service learning in undergraduate dental education: A controlled trial in a residential facility for people with intellectual disabilities. Spéc. Care Dent. 2018, 38, 201–207. [Google Scholar] [CrossRef]
- Rozas, N.S.; Sadowsky, J.M.; Jeter, C.B. Strategies to improve dental health in elderly patients with cognitive impairment: A systematic review. J. Am. Dent. Assoc. 2017, 148, 236–245. [Google Scholar] [CrossRef] [PubMed]
- Petersen, P.E.; Ogawa, H. The global burden of periodontal disease: Towards integration with chronic disease prevention and control. Periodontology 2000 2012, 60, 15–39. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Objective 1 | |||
|---|---|---|---|
| Oral health related | People with disability related | Knowledge related | |
| “oral health” “oral hygiene” “dental health” “dental care” “oral care” “mouth care” | “people with disabilit*” “disabled people” “special needs people” “people with intellectual disabilit*” “people with dementia” “people with cognitive disorder*” | Knowledge Attitude* Perception* Belie* View* Feeling* Experience* Literacy | |
| Objective 2 | |||
| Education related | Carers related | Oral health related | People with disability related |
| Education training program curriculum | carer* caregiver* “family member*” relative* “informal carer*” “paid carer*” “unpaid carer*” | “oral health” “oral hygiene” “dental health” “dental care” “oral care” “mouth care” | “people with disabilit*” “disabled people” “special needs people” “people with intellectual disabilit*” “people with dementia” “people with cognitive disorder*” |
| Author, Year, Country | Title | Study Type and Category | Study Population | Sample Size | Key Findings |
|---|---|---|---|---|---|
| Objective 1: Education/training-related interventions for dental health professionals | |||||
| Blaizot et al., 2018 France | Obstacles to comprehensive dental care in patients with sustained limitations of their decision-making abilities: findings from a Delphi study | Quantitative/ qualitative/ exploratory/ knowledge, skills, and attitude | Dental practitioners | 72 | Using the Delphi technique with a panel of 72 dental practitioners, the researchers explored obstacles to comprehensive dental care for people with limited decision-making abilities. Agreement was reached that oral health care requires a high degree of co-operation in care and in hygiene. Obstacles include difficulties in establishing and maintaining long-term oral hygiene behaviours, low caregivers’ priority for oral health, and difficulties in follow-up care. The undergraduate and postgraduate curriculum developed by the International Association of Disability and Oral Health was recommended to enhance a holistic patient-centred approach. Training for dentists, information and training for caregivers, and oral health screening in nursing homes were recommended. Cultural change including oral health specialists, general practitioners, dental organisations, patients, and caregivers was sought. |
| Ahmad et al., 2014 Malaysia | Special Needs Dentistry: perception, attitudes, and educational experience of Malaysian dental students | Quantitative/ exploratory/ knowledge, skills, and attitude | Final year dental students of 6 universities | 289 | Questionnaire results revealed 31.7% of dental students were comfortable treating patients with intellectual disability; 50.5% of responding students felt training in SND was inadequate; 89.6% felt clinical training was needed at undergraduate level; 61.2% of students, the majority of whom were women, were interested in postgraduate SND training; 96.9% of respondents felt they needed didactic training on the topic. Earlier exposure to SND training, liaison with external organisations and different clinical settings, support to gain specialist qualifications, and continuous professional development were recommended by the researchers. |
| Catteau et al., 2013 France | Using e-learning to train dentists in the development of standardised oral health promotion interventions for persons with disability | Quantitative/ experimental | Dental health professionals | 24 | Dentists completed a 10-module online training course and implemented a standardised intervention in a disability institution. Results of pre- and post-questionnaires used to measure self-efficacy and course satisfaction indicate the online training contributed to positive outcomes. |
| Dellavia et al., 2009 Italy | Special care dentistry for people with intellectual disability in dental education: an Italian experience | Quantitative/ exploratory/ knowledge, skills, and attitude | Final-year dental students and Deans of Schools | 248 students and 4 Deans of Universities | Surveys distributed to 20 Italian dental schools received a 51% student response rate but only 20% response rate from Deans. Surveys sought data on curriculum content, satisfaction with curriculum, and attitudes of students toward dental care for people with intellectual disability. Responses suggest low levels of didactic and clinical training and poor training content. Revised curricular standards were recommended to improve training in treatment of people with intellectual disability. |
| Faulks et al., 2018 France | Development of a battery of tests to measure attitudes and intended behaviours of dental students towards people with disability or those in marginalised groups | Quantitative/scales or tools to assess knowledge, skills, and attitudes. | Dental health students, graduates, and practitioners who have studied in 4 countries | 130 | The researchers developed a survey tool and test battery to evaluate values, attitudes, and intentions of dental students towards people with disability. Three adapted scales and the theory of planned behaviour were piloted in 4 countries with students and dental health practitioners at 5 different professional stages. Scales were assessed for internal reliability, variance, distribution and face, and content validation. The tool will be validated for use by educators to evaluate the impact of clinical exposure and teaching on their students |
| Isobe et al., 2018 Japan | Attitudes towards people with dementia: a cross-sectional study comparing dental hygiene students with registered dental hygienists | Quantitative/ exploratory/ knowledge, skills, and attitude | Registered dental hygienists and dental hygiene students | 255 | Surveys were used to assess attitudes and knowledge. Likert scale analysis and the Fraboni Ageism Scale found registered dental hygienists had more knowledge and positive attitudes towards people with dementia compared with dental hygiene students. Training in treatment of people with dementia should be added to dental hygienists’ curriculum. |
| Mac Giolla Phadraig et al., 2015 Ireland | Does special care dentistry undergraduate teaching improve dental student attitudes towards people with disabilities? | Quantitative/ experimental | Third-year dental health students | 109 | The researchers used pre- and post-testing to assess the impact of a brief blended learning module on special care dentistry over 3 years. No statistically significant difference was found in student attitudes toward people with disability before and after educational intervention. Dental students in this study had neither particularly positive nor negative attitudes towards people with disability. Researchers proposed the scale used to measure attitudinal change was inadequate for the purpose. |
| Mohebbi et al., 2014 Iran | Effectiveness of training senior dental students on oral health care for disabled patients | Quantitative/ experimental | Dental health students | 70 (Control group = 34, experimental group = 36) | Likert scale analysis of pre- and post-surveys of final year dental students about a 10-day intervention comprising presentations, peer discussion, visit to childcare centre for autistic children, and discussion about communication with patients with disability. Results indicated improvements in knowledge and attitudes of the intervention group from short-term training programmes, but researchers recommended further longitudinal research on retention of knowledge and attitudes. |
| Jones et al., 2018 U.S.A. | Effectiveness of an educational module on dental hygiene students’ attitudes towards persons with disabilities | Quantitative | Dental health students | Pre-training survey = 81 Post-training survey = 65 | Questionnaires measured effectiveness of DVD educational module developed inclusively with people with disability and used with 2nd- or 3rd-year dental students. A range of scales was used to measure attitudes and empathy toward people with disabilities pre and post. Results indicated the module was an effective model for patient-centred training. Researchers recommended further qualitative study and longitudinal research into the effect of the module. |
| Nagarajappa et al., 2012 India | Dentists’ attitude to provision of care for people with learning disabilities in Udaipur, India | Quantitative/ exploratory/ knowledge, skills, and attitudes | Private dental health professionals, faculty, and postgraduate students across Udalpur, India | 247 | Analysis of questionnaires using Statistical Package for Social Sciences (SPSS) Version 16 found the overall attitude of respondents toward treating people with learning difficulties was positive, with a statistically significant correlation between the mean attitude of dentists and their previous experience of treating people with learning difficulties. |
| Smith et al., 2010 Ireland | Provision of dental care for special care patients: the view of Irish dentists in the Republic of Ireland | Quantitative/ exploratory/ knowledge, skills, and attitude | Dental health professionals | 236 | This survey received only a 35% response rate. Analysis using SPSS found 41% of respondents had trained in SND, and 65% expressed willingness to train; 66% had experience in treating people with disability; 59% of respondents who had received no training in treating people with disability were doing so. The. most common service provided in SND was management of dental emergencies. Only 25% of respondents were aware of legal obligations to people with disability. There was emphasis on a need for clinical training at undergraduate and postgraduate level and education and training for carers and community-based preventative care. Behaviour and communication were perceived to be the main obstacles to the provision of dental care. |
| Objectives 1 & 4 | |||||
| Mac Giolla Phadraig et al., 2016 Ireland | Should we educate care staff to improve the oral health and oral hygiene of people with intellectual disability in residential care? Real world lessons from a randomized controlled trial | Quantitative/ experimental | Carers and adults with intellectual disabilities in residential care | 76 (Intervention group = 35, control group = 41) | Researchers trained 22 residential care nurses in oral hygiene, who then trained peers in residential care. Pre- and post-data collection and dental examination of residents by experienced dentist were followed by analysis of clinical and descriptive data and comparison between intervention and control groups. Results suggested the intervention did not lead to improved oral hygiene, but there were improvements in knowledge, attitudes, and beliefs of carers about oral hygiene of people with intellectual disability. |
| Objective 3: Education/training-related interventions for people with intellectual disabilities | |||||
| Lees et al., 2016 U.K. | Adults with learning disabilities experience of using community dental services: Service user and carer perspectives | Qualitative/ exploratory | Carers and adults with intellectual disabilities | 4 adults with learning difficulties and 6 carers | Participant interviews and thematic analysis found people with intellectual disability expected dental staff to understand their needs. Positive factors were effective interpersonal communication between dental staff and participants, providing information, relieving anxiety, actively listening, and showing dignity. Setting aside enough time for explaining procedures during consultations enhanced the experience patients. Further studies are required with a wider population of people with intellectual disability who use dentists. |
| Mac Giolla Phadraig et al., 2016 Ireland | What should dental services for people with disabilities in Ireland be like? Agreed priorities from a focus group of people with learning disabilities | Qualitative/ experimental | People with intellectual disabilities | 6 | The researchers conducted a single focus group with six adults with learning difficulties and cognitive/communication disorders, using accessible methods. Priorities identified by people with learning disabilities were information, treatment, access, quality of care, and cost. The researchers identified disempowerment of people with learning difficulties and proposed dental services could improve the accessibility and content of information for this group. The researchers identified the need to train dental health professionals in communication with people with learning disabilities and argued that people with learning disabilities should be involved in planning and evaluating oral health services. |
| Objective 4: Education/training-related interventions for carers of people with intellectual disability | |||||
| Pradhan et al., 2016 Australia | Pre- and post-training evaluation of dental efficacy and activation measures in carers of adults with disabilities in South Australia—A pilot study | Quantitative/ experimental | Carers | 41 carers of 103 adults with disabilities | Carers were trained by a SND in oral health care, supported by dental hygienist for 2 months and dental visit at 3 months. Pre- and post-questionnaires on dental behaviours of carers and carers’ knowledge, skill, confidence, and dental efficacy. Results indicated increased knowledge and confidence but not skills. Carers were better able to assess the referral needs of their care recipients’ oral health similar to the dentist, indicating combined theoretical and practical training and continued support can improve the knowledge and confidence of non-dental health professionals such as carers in providing oral care for their recipients. Further research in a larger study is needed. |
| Phlypo et al., 2018 Belgium | Integrating community service learning in undergraduate dental education: A controlled trial in a residential facility for people with intellectual disabilities | Quantitative | Carers of adults with intellectual disability in residential care | 37 = Residents (Intervention group = 18); 55 = Caregivers (Intervention group = 24) | An intervention in a residential care service for people with intellectual disability comprised information for caregivers, pre-and post-test dental examinations of residents, and a questionnaire assessing caregivers’ knowledge. Compared with the control group, the gingival health of residents after the test was found to have improved. Overall, there was some but limited impact on caregivers’ knowledge and residents’ oral health. Researchers made recommendations on future research in community service learning. |
| Mac Giolla Phadraig et al., 2012 Ireland | Train the trainer? A randomized controlled trial of a multi-tiered oral health education programme in community-based residential services for adults with intellectual disability | Quantitative/ experimental | Carers | Intervention group =21, control group =29 | 21 residential care staff received multi-tiered, day-long training from dental health professionals on oral health, oral disease, and prevention of oral disease. Topics were brushing, diet, dealing with challenging behaviours, and care of complete dentures. A control group received no training. Pre- and post-tests of knowledge, attitude, self-efficacy, and self-reported behaviour indicated some improvement in knowledge but no statistical improvement in attitudes. Researchers partially attributed results to increased awareness on the part of the control group (Hawthorne effect) and limitations in research methods but concluded that multi-tiered training programs can improve oral-health-related knowledge, attitude, self-efficacy, and reported behaviour in residential care settings for people with intellectual disability. |
| Mac Giolla Phadraig et al., 2015 Ireland | Should we provide oral health training for staff caring for people with intellectual disabilities in community based residential care? A cost-effectiveness analysis | Cost effectiveness evaluation/experimental | N/A | N/A | Analysis of capital and operating expenses in conducting the above train-the-trainer intervention, despite its small effect, found it to be cost-effective in improving oral-health-related knowledge and reported behaviour, attitudes, and self-efficacy. Ongoing research into cost benefit is required. |
| Eijsink et al., 2018 Netherlands | A Q-methodology study among caregivers of people with moderate intellectual disabilities on their clients’ health care: An example in oral health | Qualitative/ quantitative exploratory | Carers of people with moderate intellectual disabilities living in institutions | 40 | The researchers used Q-methodology to explore carers’ viewpoints about oral hygiene. By-person factor analysis was used to cluster caregivers’ views. Four factors were identified: 1. Responsible and perseverant; 2. Motivated and aware of obstacles; 3. Social-minded and knowledgeable; 4. Concerned and insecure. Researchers concluded that results can be used to determine attitudes of caregivers regarding oral healthcare and to consider dental care professionals’ adaptation of advice to carers’ specific characteristics. |
| Rozas et al., 2017 | Strategies to improve dental health in elderly patients with cognitive impairment | Systematic review | Elderly people with cognitive impairment or dementia and carers | 9 full-text articles | Basic oral care plans for people with cognitive impairment should, at minimum, focus on preventative strategies recommended for healthy older patients. Oral hygiene education should be promoted by dental health professionals for caregivers of people with cognitive impairment. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kangutkar, T.; Calache, H.; Watson, J.; Taylor, S.; Balandin, S. Education/Training Interventions to Improve Oral Health of Adults with Intellectual Disability. Healthcare 2022, 10, 2061. https://doi.org/10.3390/healthcare10102061
Kangutkar T, Calache H, Watson J, Taylor S, Balandin S. Education/Training Interventions to Improve Oral Health of Adults with Intellectual Disability. Healthcare. 2022; 10(10):2061. https://doi.org/10.3390/healthcare10102061
Chicago/Turabian StyleKangutkar, Tejashree, Hanny Calache, Joanne Watson, Susan Taylor, and Susan Balandin. 2022. "Education/Training Interventions to Improve Oral Health of Adults with Intellectual Disability" Healthcare 10, no. 10: 2061. https://doi.org/10.3390/healthcare10102061
APA StyleKangutkar, T., Calache, H., Watson, J., Taylor, S., & Balandin, S. (2022). Education/Training Interventions to Improve Oral Health of Adults with Intellectual Disability. Healthcare, 10(10), 2061. https://doi.org/10.3390/healthcare10102061