

“Pandemic Fatigue! It’s Been Going On since March 2020”: A Photovoice Study of the Experiences of BIPOC Older Adults and Frontline Healthcare Workers during the Pandemic

 ,
,
Abstract
:1. Introduction
1.1. Impact of the Ongoing Pandemic on BIPOC Older Adults and Frontline Healthcare Workers
1.2. Why Use Photovoice?
1.3. The Current Study
2. Materials and Methods
2.1. Design
2.2. Participants
2.3. Training of Research Assistants (RAs)
2.4. Procedure
2.4.1. Stage 1: Introduction of Photovoice Methodology
2.4.2. Stage 2: Taking the Photos
2.4.3. Stage 3: Photo Selection Process
2.4.4. Stage 4: Focus Group Discussion
2.5. Data Analysis
3. Results
3.1. Challenges of the COVID-19 Pandemic
3.1.1. Fear of COVID-19 Exposure
“The picture (Figure 1) shows you how the room you are going into is a yellow zone which indicates a potential to contract COVID-19. Whoever goes into the room has a higher chance of getting COVID-19; whenever we go in, we don’t know the potential risks, and we don’t know who we will come across. Many loved ones have entered the ED for something we did not see as COVID-19 and could not get back to their loved ones.”[FLWH 03]

3.1.2. Struggles Adopting COVID-19 Mitigation Measures
“Frontline healthcare workers use it for eight hours, eight straight hours. We only can take it off when we go for a break or when we’re alone, but we almost have to wear it the whole time. People complain about using masks for 30 min to go to the grocery store. We have to use it all the time when interacting with patients, walking in the halls, walking into the building. We must wear it because it’s now part of our uniform. People should just wear masks to help protect others; if we can do it for eight hours or even more for those that work for twelve hours, people should not be reluctant to use them.”[FLHW 03]
“Not everyone likes wearing masks, especially working with elderly people at home care; they don’t always agree with the COVID-19 protections we are taking. About half of the elderly don’t like the mask rules, but they just have to be reminded that it is for their protection. We let them know that these precautions are being taken in different settings around the world and in casual settings like work. Just keep reminding those that we are working with in a home why we are taking these precautions and keep practicing the precautions.”[FLHW 01]
“Because of the pandemic, like with the masks, hand sanitizers are also being used a lot. Hand sanitizers can be annoying to have to use constantly. That could also be a problem in-home care, especially if we go out with our older adult clients. Say, like they have a baseball event or something, you have to constantly remind them to “oh, make sure you are using your hand sanitizer”. Sometimes that can be a bit difficult and frustrating for them, but it’s not too much difficult, but it’s just the precautions that have to be taken as much as we can.”[FLHW 06]
“Pandemic fatigue! It’s been going on since March 2020. A lot of us are sick. It’s been literally years of social distancing, and isolation, quarantining, testing, vaccinations, and discussions about that, and wearing masks.”[FLHW 11]
“I see the staircase down to the basement (Figure 2) where I quarantined a couple many times during this COVID-19 of more than two years and a half, you know, more than two years. As a nurse, you know, I’ve been working with COVID-19 patients, on and off, though not very serious patients, you know, despite all of the PPE you wear, there’s every chance of exposure, so I always go down to quarantine for 4–5 days. That just reminds one of the difficult periods of this pandemic. It was mentally difficult.”[OA 17]

3.1.3. Workplaces Challenges
“There have been mornings where I’m by myself for the first few hours and have to take care of about 40 residents. Although it’s technically doable, as a residency assistant, I normally get about 20 residents to care for. So it’d be about 40 residents by myself, which can be stressful.”[FLHW 03]
“You know, we, as healthcare workers, need breaks as well. There’s like such a high level of burnout and turnover in the medical field; people are just straight up quitting and retiring early, leaving the profession completely. So, like, we’re already stressed. And then we’re short-staffed. And so, it’s like, having to manage our own sanity and health amidst this crazy thing (COVID-19 pandemic), you know, is really difficult.”[FLHW 11]
“When the pandemic started, we didn’t have as many supplies. But now that we have built up the supplies, we are using a lot of single-use masks. We are trying our best with our PPE, which is one of the best ways to prevent it from patient to provider, providers to other providers.”[FLHW 11]
“We have that set of rules, those set of things that we have to do, which makes it hard to do what I really love about my job, which is the talking and communicating with others. So the majority of my time, I’m doing med passes, and I’m giving my residents their medication. Then I’m just simply moving on to the next place.”[FLHW 01]
“I have a nurse who is very organized and structured but has never been a Certified Nursing Assistant before. The nurse will call and yell at us over the phone for not being at the right place at the right time. I distinctly remember being with a resident and getting a call asking where I was. Then, the nurse was upset with me that I was behind on my schedule, despite being short-staffed. The first thing the nurse thought to do in that situation was to be argumentative instead of understanding the situation. The lack of understanding or the feeling of not being respected, especially during that stressful time, was painful.”[FLHW 01]
3.1.4. Social Isolation
“This is the window (Figure 4) that when my children came, they looked there. They left some little things there, and they left. It was very sad in here. They only entered the porch. I only looked out the window looking at them, it took a long time, it took me a long time. I was very sad because when my children came before the pandemic, they came in, and we ate here at the table. And that was no longer there. So, I suffered because they couldn’t get in. They said because they could infect me. What can I say? I felt bad. I felt bad because they couldn’t come in as usual and talk. They just came from a distance and left. Sometimes I even cried because my children could not come in. That suffering was very hard for me, if not for everyone; we distanced ourselves for a long time.”[OA 01]

3.2. Overcoming the Challenges of the COVID-19 Pandemic
3.3. Positive Reappraisal
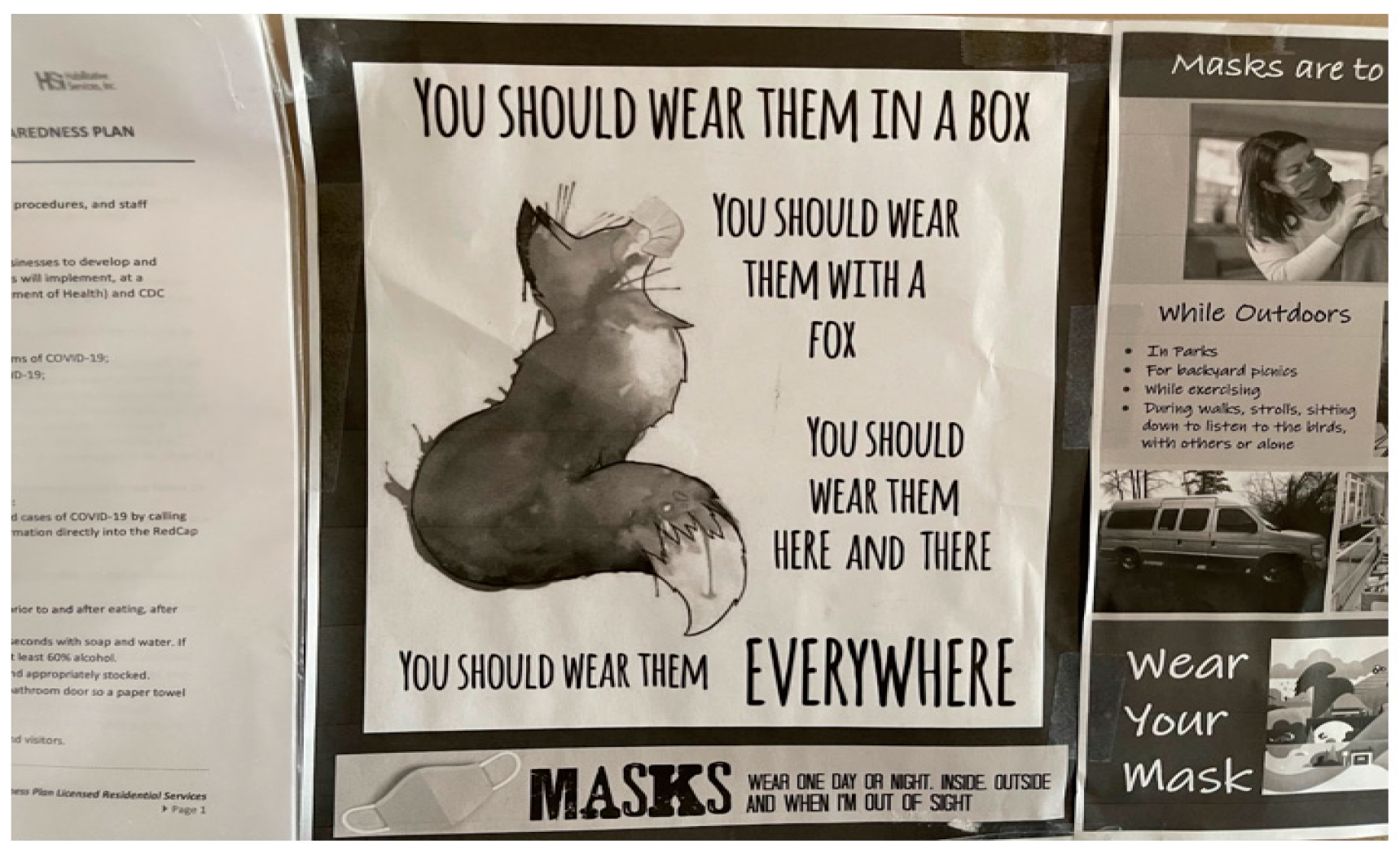
“It’s hung up in our work area (Figure 5). The photo shows a fox along with some rhymes promoting the use of masks. With the pandemic, there are mask mandates everywhere so masks are a big part of our lives. The fact that there is a doodle along with the rhymes just makes it more lighthearted. It reminds me a little of Dr. Seuss, with all of the rhymes that just automatically lighten the darkness the pandemic has brought. It encourages people to wear masks in a different way that isn’t so demanding. I guess continuing to lighten the mask situation for others can really help others who are struggling with wearing masks.”[FLHW 06]

“Here is a funny picture that my co-worker posted to help bring laughter to patients getting the COVID-19 test. It sparks conversation and serves as a bit of distraction and a little joke, saying it could be worse. Back in the day, my co-worker used it to say, ‘this is how the COVID-19 test was done in the 1550s’, as a joke. The public must get COVID-19 tests regularly, like a vaccine, to keep us all safe. Although the process is painful, still, we have to endure it because this could have been worse. We can always try to find the light in the dark tunnel. We can find a burst of laughter out of it.”[FLHW 03]
3.4. Self-Care Practices
3.4.1. Emotional Self-Care
“I am standing in front of a tree (Figure 6), out in nature, completely immersed in my energy work (more specifically, the energy ball) and holding my drum in the image to the right. I have found purpose, meaning, and solace throughout the pandemic by centering myself in good energy, nature, practices that ground myself and others, artistic expression through staying active in my community, and through my musical expression of drumming. Despite the chaos of the world around me due to the pandemic, I am able to ground myself in my passions. Life is often centered around meaning. My aim is to provide hope through these images, that despite such a difficult and catastrophic event such as this pandemic, people can still find meaning and joy through things and hobbies that they love. Suppose more people begin to focus on the things that they enjoy. In that case, it may help alleviate some of the stress and anxiety that has clearly resulted from the public crisis at hand.”[OA 03]

“I participate in the elder lodge family on Easter by coloring eggs and decorating cookies. It brings us together as a family and keeping us active with what we have been doing in our lives with our children. It helps us be involved with the outside celebrations. It keeps our elder family strong by participating together. It brings the elder lodge family together. We enjoy group activities, and sometimes we do crafts. Just make sure that we keep these activities alive and it helps strengthen our minds. We have to concentrate on crafts.”[OA 10]
“I see myself sitting, you know, there behind the table… I am just starting to read. This was especially helpful during the pandemic and especially in the winter times when you cannot go out and do any gardening. So reading takes you to a different world even if you’re in quarantine and sitting alone, yet you are not alone.”[OA 17]
3.4.2. Spiritual Self-Care
“I do a lot of reflection about my time on the job because I absolutely love my residents and like you’re at this heightened sense of awareness. It’s a lot of understanding, knowing my own limitations, and my limitations in relation to things that I cannot change.”[FLHW 01]
“This is Minnehaha Falls in Minneapolis (Figure 8), and the waterfall is frozen, creating a cool icicle effect. You can see the branches and the water freezing over and see that it is winter. I, my daughter, and my wife were enjoying the outside, bundled up, and my daughter was on a little sled. Taking walks like this is a respite from pandemic fatigue and the day-to-day existence of living inside a global pandemic. So, it’s a nice little break from that. In terms of pandemic fatigue, it’s been going on since March of 2020… it’s been literally years of social distancing, isolation, quarantine, testing, vaccinations, wearing masks, and all of the discussions that revolve around it. Especially working in the healthcare field, it’s been taking its toll of having to work and seeing people affected by that. Getting back into enjoying nature and understanding that nature still exists outside of this very human problem is important, and it’s helpful to take a break, rest, and reflect to get to one’s self.”[FLHW 11]

“Gratitude flows from a heightened sense of awareness, increasing as one takes the time to go within and be quiet. Expression of gratitude was another important source of strength for participants, who described it as the feeling of thankfulness for God’s protection and appreciation of others’ kindness and generosity.
My son goes out to the street for his first job working with children. In his second job, he works with clients, and thank God we have not had any type of infection because among the three of us who live in this house we take great care of ourselves. So, we are fine and happily healthy, which is the most important.”[OA 02]
“In the medical facilities, we’re wearing cloth masks. It was really inspiring to see so many community members donating masks and stuff.”[FLHW 11]
“I am a member of a group that provides aid for those outside their community, such as food, clothes, and furniture. I want to present some of the people behind the work of my church (picture not shown) who provides food, clothing, household appliances, and furniture. I love being a part of their church. It is part of what I have been doing all my life to ensure everything gets delivered—especially the food and clothing. Besides a spiritual need, there is a need for food and clothing. Still, now there is a line for these food shelves. It can give them hope that there are people out there that have the means to distribute food and clothing to other reservations. We can pray for them to keep their work growing and expanding.”[OA 10]
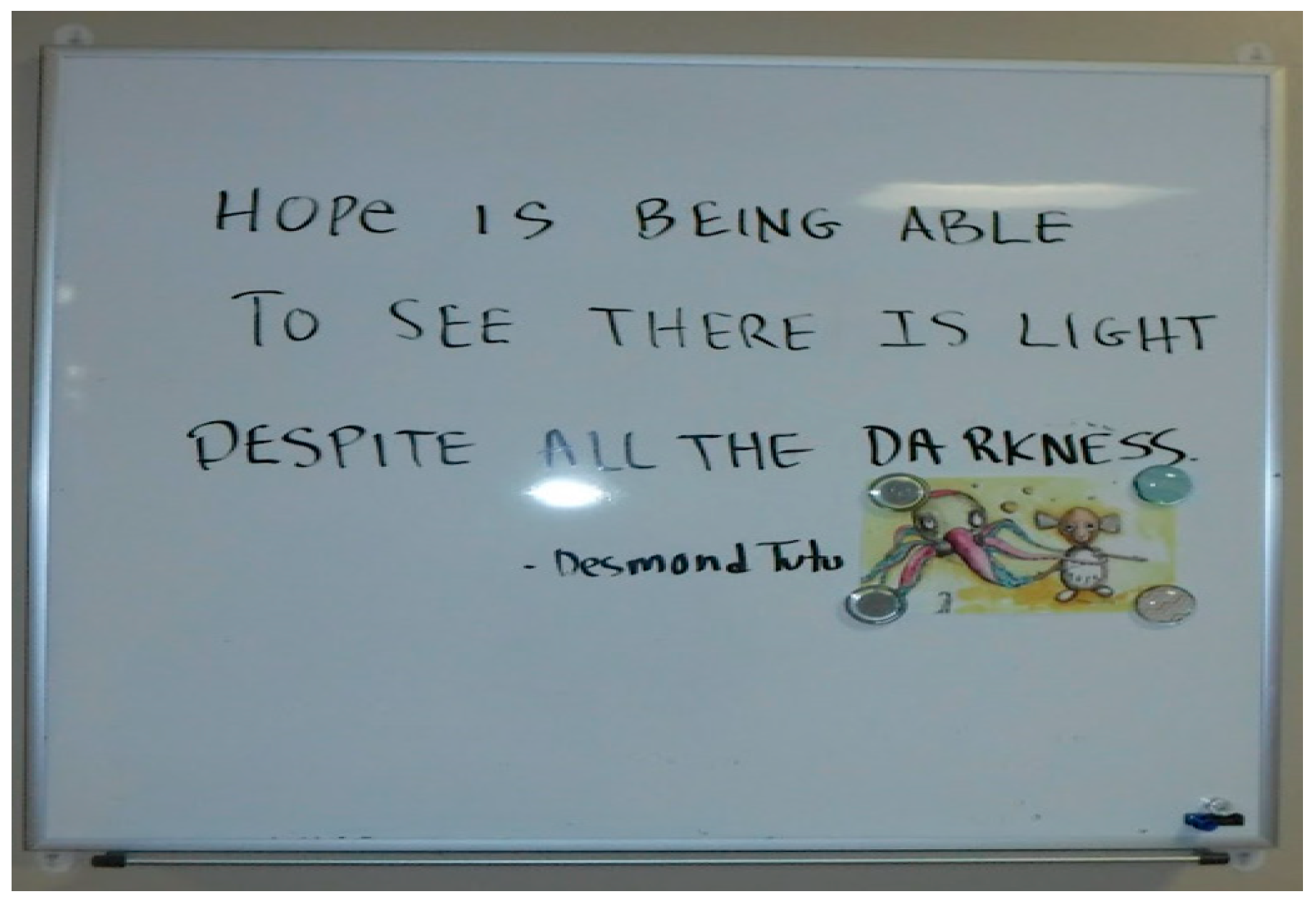
“The staff in the hospital took the time to write this quote (Figure 9), and when other staff come in through a specific location, they see this quote and bring it with them throughout their day. Yes, this pandemic sucks, but it will get better. Sometimes, we go through so many hardships and want to give up, and this quote motivates us to keep going. The quote is a strength to help encourage people, and it gives a few words of encouragement. Most of us are overworked, and we don’t get recognition from our managers, and just saying this always inspires and motivates us. And it’s hard to keep your head up, even though it has been only two years, but it could be three or four. It will get better.”[FLHW 03]
3.4.3. Social Self-Care
“We are both smiling deeply and very happy to be with one another. The relationship between us emulates unconditional love and that we care about each other dearly. My granddaughter provides help to me by serving as my Personal Care Assistant. Not only this, but she also both gives and receives that familial love, aiding me as my constant companion and close friend. I have been able to see my granddaughter in person throughout the entirety of the pandemic. Despite being isolated from so many people, being able to share love and time with her has brought me so much meaning and lots of joy despite such a fearful time. Since the onset of the COVID-19 pandemic, many of my in-person interactions have ceased to exist due to safety precautions. However, this image shows my ability to stay close in connection with a few individuals despite feeling isolated from a great number. Until the safety of the virus is clear, finding solace in time with my close loved ones and those in my circle is key.”[OA 03]
“I prefer doing more care over medicine, and some people prefer the opposite. I like the care because I can interact, communicate, talk to my clients, and actually get to know my residents and better bond with them.”[FLHW 01]
3.4.4. Physical Self-Care
4. Discussion
4.1. Strengths, Limitations, and Opportunities for Future Research
4.2. Implications for Practice
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Fang, C.Y.; Ragin, C.C. Addressing Disparities in Cancer Screening among U.S. Immigrants: Progress and Opportunities. Cancer Prev. Res. 2020, 13, 253–260. [Google Scholar] [CrossRef] [Green Version]
- Lieberman-Cribbin, W.; Tuminello, S.; Flores, R.M.; Taioli, E. Disparities in COVID-19 Testing and Positivity in New York City. Am. J. Prev. Med. 2020, 59, 326–332. [Google Scholar] [CrossRef]
- Gravlee, C.C. Systemic racism, chronic health inequities, and COVID-19: A syndemic in the making? Am. J. Hum. Biol. 2020, 32, e23482. [Google Scholar] [CrossRef]
- Ekwonye, A.U.; Ezumah, B.A.; Nwosisi, N. Meaning in life and impact of COVID-19 pandemic on African immigrants in the United States. Wellbeing Space Soc. 2021, 2, 100033. [Google Scholar] [CrossRef]
- Cunningham, T.J.; Croft, J.B.; Liu, Y.; Lu, H.; Eke, P.I.; Giles, W.H. Vital Signs: Racial Disparities in Age-Specific Mortality Among Blacks or African Americans—United States 1999–2015. MMWR Morb. Mortal. Wkly. Rep. 2017, 66, 444–456. [Google Scholar] [CrossRef]
- Walker, R.E.; Keane, C.R.; Burke, J.G. Disparities and access to healthy food in the United States: A review of food deserts literature. Health Place 2010, 16, 876–884. [Google Scholar] [CrossRef]
- Hughes, H.K.; Matsui, E.C.; Tschudy, M.M.; Pollack, C.E.; Keet, C.A. Pediatric Asthma Health Disparities: Race, Hardship, Housing, and Asthma in a National Survey. Acad. Pediatr. 2017, 17, 127–134. [Google Scholar] [CrossRef] [Green Version]
- Jacobs, D.E. Environmental Health Disparities in Housing. Am. J. Public Health 2011, 101 (Suppl. S1), S115–S122. [Google Scholar] [CrossRef]
- Rho, H.J.; Brown, H.; Fremstad, S. A basic demographic profile of workers in frontline industries. Center Econ. Policy Res. 2020, 7, 1. [Google Scholar]
- Nguyen, L.H.; Drew, D.A.; Graham, M.S.; Joshi, A.D.; Guo, C.G.; Ma, W.; Mehta, R.S.; Warner, E.T.; Sikavi, D.R.; Lo, C.H.; et al. Risk of COVID-19 among front-line health-care workers and the general community: A prospective cohort study. Lancet Public Health 2020, 5, e475–e483. [Google Scholar] [CrossRef]
- Sepúlveda-Loyola, W.; Rodríguez-Sánchez, I.; Pérez-Rodríguez, P.; Ganz, F.; Torralba, R.; Oliveira, D.V.; Rodríguez-Mañas, L. Impact of social isolation due to COVID-19 on health in older people: Mental and physical effects and recommendations. J. Nutr. Health Aging 2020, 24, 938–947. [Google Scholar] [CrossRef]
- Smith, B.J.; Lim, M.H. How the COVID-19 pandemic is focusing attention on loneliness and social isolation. Public Health Res. Pract. 2020, 30, e3022008. [Google Scholar] [CrossRef]
- Brooke, J.; Jackson, D. Older people and COVID-19: Isolation, risk and ageism. J. Clin. Nurs. 2020, 29, 2044–2046. [Google Scholar] [CrossRef]
- Tai, D.B.G.; Shah, A.; Doubeni, C.A.; Sia, I.G.; Wieland, M.L. The Disproportionate Impact of COVID-19 on Racial and Ethnic Minorities in the United States. Clin. Infect. Dis. 2020, 72, 703–706. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention. Health Equity Considerations and Racial and Ethnic Minority Groups. Available online: https://www.cdc.gov/coronavirus/2019-ncov/need-extra-precautions/racial-ethnicminorities.html.2020 (accessed on 3 September 2022).
- National Center for Immunization and Respiratory Diseases & the Division of Viral Diseases. COVID-19 in Racial and Ethnic Minority Groups. Available online: https://www.cdc.gov/coronavirus/2019-ncov/need-extraprecautions/racial-ethnic-minorities.html.Published2020 (accessed on 1 September 2022).
- Paul-Emile, K.; Critchfield, J.M.; Wheeler, M.; de Bourmont, S.; Fernandez, A. Addressing Patient Bias Toward Health Care Workers: Recommendations for Medical Centers. Ann. Intern. Med. 2020, 173, 468–473. [Google Scholar] [CrossRef]
- Paul-Emile, K. COVID-19 and the ‘Essential’ Yet Underappreciated Front-Line Health Care Worker Harvard Law Petrie-Flom Center. Bill of Health: Examing the Intersection of Health, Law, Biotechnology and Bioethics. 2020. Available online: https://blog.petrieflom.law.harvard.edu/2020/09/17/covid19-essential-frontlinehealthcare-worker-race/ (accessed on 1 September 2022).
- Paul-Emile, K. Patients’ Racial Preferences and the Medical Culture of Accommodation. UCLA Law Rev. 2012, 60, 462. [Google Scholar]
- Yi, S. I’m an Asian American Doctor on the Front Lines of Two Wars: Coronavirus and Racism. The Lily. 2020. Available online: https://www.thelily.com/gdpr-consent/?destination=%2fim-an-asian-american-doctor-on-the-front-lines-of-two-wars-coronavirus-and-racism%2f%3f (accessed on 30 August 2022).
- Campbell, S. Paraprofessional Healthcare Institute. Racial and Gender Disparities within the Direct Care Workforce: Five Key Findings; PHI National: New York, NY, USA, 2017. [Google Scholar]
- Kinder, M. Essential but Undervalued: Millions of Health Care Workers aren’t Getting the Pay or Respect They Deserve in the COVID-19 Pandemic. Metropolitan Policy Program (No. 2). 2020. Available online: https://www.brookings.edu/research/essential-but-undervalued-millions-of-health-care-workers-arent-getting-the-pay-or-respect-they-deserve-in-the-covid-19-pandemic/ (accessed on 5 September 2022).
- Wang, C.; Burris, M.A. Photovoice: Concept, methodology, and use for participatory needs assessment. Health Educ. Behav. 1997, 24, 369–387. [Google Scholar] [CrossRef] [Green Version]
- Fortuna, L.R.; Tolou-Shams, M.; Robles-Ramamurthy, B.; Porche, M.V. Inequity and the disproportionate impact of COVID-19 on communities of color in the United States: The need for a trauma-informed social justice response. Psychol. Trauma 2020, 12, 443–445. [Google Scholar] [CrossRef]
- Latoya Hill, L.; Artiga, S. COVID-19 Cases and Deaths by Race/Ethnicity: Current Data and Changes Over Time. Available online: https://www.kff.org/coronavirus-covid-19/issue-brief/covid-19-cases-and-deaths-by-race-ethnicity-current-data-and-changes-over-time/9 (accessed on 4 September 2022).
- Centers for Disease Control and Prevention [CDC]. COVID Data Tracker. Atlanta, GA: US Department of Health and Human Services. 2022. Available online: https://covid.cdc.gov/covid-data-tracker (accessed on 1 September 2022).
- Sequist, T.D. The Disproportionate Impact of COVID-19 on Communities of Color. Available online: https://catalyst.nejm.org/doi/full/10.1056/CAT.20.0370 (accessed on 30 July 2020).
- Garfield, R.; Rae, M.; Claxton, G.; Orgera, K. Double Jeopardy: Low Wage Workers at Risk for Health and Financial Implications of COVID-19. KFF. 2020. Available online: https://www.kff.org/coronavirus-covid-19/issue-brief/doublejeopardy-low-wage-workers-at-risk-for-health-and-financial-implications-of-covid-19/ (accessed on 13 August 2022).
- Bui, C.N.; Peng, C.; Mutchler, J.E.; Burr, J.A. Race and ethnic group disparities in emotional distress among older adults during the COVID-19 pandemic. The Gerontologist 2021, 61, 262–272. [Google Scholar] [CrossRef]
- Ekwonye, A.U.; Hearst, M.O.; Howard, H. Reducing the impact of COVID-19 pandemic using meaning-based coping strategies: Voices of Somali, Karen and Latinx immigrant and refugee communities in the Twin Cities, Minnesota. J. Immigr. Refug. Stud. 2021, 1–16. [Google Scholar] [CrossRef]
- Usher, K.; Bhullar, N.; Jackson, D. Life in the pandemic: Social isolation and mental health. J. Clin. Nurs. 2020, 29, 2756–2757. Available online: https://onlinelibrary.wiley.com/doi/pdfdirect/10.1111/jocn.15290 (accessed on 6 September 2022). [CrossRef] [PubMed] [Green Version]
- Smith, K.; Bhui, K.; Cipriani, A. COVID-19, mental health and ethnic minorities. Evid. Based Ment. Health 2020, 23, 89. [Google Scholar] [CrossRef]
- Valtorta, N.K.; Kanaan, M.; Gilbody, S.; Ronzi, S.; Hanratty, B. Loneliness and social isolation as risk factors for coronary heart disease and stroke: Systematic review and meta-analysis of longitudinal observational studies. Heart 2016, 102, 1009–1016. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Millett, G.A.; Jones, A.T.; Benkeser, D.; Baral, S.; Mercer, L.; Beyrer, C.; Honermann, B.; Lankiewicz, E.; Mena, L.; Crowley, J.S.; et al. Assessing differential impacts of COVID-19 on black communities. Ann. Epidemiol. 2020, 47, 37–44. [Google Scholar] [CrossRef] [PubMed]
- Sneed, R.S.; Key, K.; Bailey, S.; Johnson-Lawrence, V. Social and psychological consequences of the COVID-19 pandemic in African-American communities: Lessons from Michigan. Psychol. Trauma 2020, 12, 446–448. [Google Scholar] [CrossRef]
- Saltzman, L.Y.; Lesen, A.E.; Henry, V.; Hansel, T.C.; Bordnick, P.S. COVID-19 mental health disparities. Health Secur. 2021, 19 (Suppl. S1), S5–S13. [Google Scholar] [CrossRef] [PubMed]
- Freire, P. Education for Critical Consciousness; Bloomsbury Publishing: London, UK, 2021. [Google Scholar]
- Ronzi, S.; Pope, D.; Orton, L.; Bruce, N. Using photovoice methods to explore older people’s perceptions of respect and social inclusion in cities: Opportunities, challenges and solutions. SSM Popul. Health 2016, 2, 732–745. [Google Scholar] [CrossRef] [Green Version]
- Miller, E.; Buys, L.; Donoghue, G. Photovoice in aged care: What do residents value? Australas. J. Ageing 2019, 38, e93–e97. [Google Scholar] [CrossRef] [Green Version]
- Rush, K.L.; Murphy, M.A.; Kozak, J.F. A photovoice study of older adults’ conceptualizations of risk. J. Aging Stud. 2012, 26, 448–458. [Google Scholar] [CrossRef]
- Tornbom, K.; Lundalv, J.; Palstam, A.; Sunnerhagen, K.S. “My life after stroke through a camera lens”—A photovoice study on participation in Sweden. PLoS ONE 2019, 14, e0222099. [Google Scholar] [CrossRef]
- Adekeye, O.; Kimbrough, J.; Obafemi, B.; Strack, R.W. Health literacy from the perspective of African immigrant youth and elderly: A PhotoVoice project. J. Health Care Poor Underserved 2014, 25, 1730–1747. [Google Scholar] [CrossRef] [Green Version]
- Ekwonye, A.U.; Truong, N. Searching and Making Meaning of the COVID-19 Pandemic: Perspectives of African Immigrants in the United States. J. Humanist. Psychol. 2022, 62, 79–103. [Google Scholar] [CrossRef]
- Malterud, K.; Siersma, V.D.; Guassora, A.D. Sample size in qualitative interview studies: Guided by information power. Qual. Health Res. 2016, 26, 1753–1760. [Google Scholar] [CrossRef] [PubMed]
- Crist, J.D.; Tanner, C.A. Interpretation/analysis methods in hermeneutic interpretive phenomenology. Nurs. Res. 2003, 52, 202–205. [Google Scholar] [CrossRef] [PubMed]
- Skaggs, B.G.; Barron, C.R. Searching for meaning in negative events: Concept analysis. J. Adv. Nurs. 2006, 52, 559–570. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.J.; Miller, S.E. A self-care framework for social workers: Building a strong foundation for practice. Fam. Soc. 2013, 94, 96–103. [Google Scholar] [CrossRef]
- Puchalski, C.M.; Vitillo, R.; Hull, S.K.; Reller, N. Improving the spiritual dimension of whole person care: Reaching national and international consensus. J. Palliat. Med. 2014, 17, 642–656. [Google Scholar] [CrossRef]
- Ekwonye, A.U.; Nwosisi, N.G. The impact of negative life events (NLEs) on spirituality: A qualitative study on the perspectives of Nigerian Catholic women religious in the United States. J. Spirit. Ment. Health 2019, 23, 155–179. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention (CDC). Characteristics of Health Care Personnel with COVID-19—United States, 12 February–9 April 2020. MMWR Morb. Mortal. Wkly. Rep. 2020, 69, 477–481. [Google Scholar] [CrossRef] [Green Version]
- Dudzinski, D.M. Moral Outrage Toward Willfully Unvaccinated COVID-19 Patients. J. Gen. Intern. Med. 2022, 37, 2070–2071. [Google Scholar] [CrossRef]
- Andel, S.A.; Tedone, A.M.; Shen, W.; Arvan, M.L. Safety implications of different forms of understaffing among nurses during the COVID-19 pandemic. J. Adv. Nurs. 2022, 78, 121–130. [Google Scholar] [CrossRef] [PubMed]
- Xu, H.; Intrator, O.; Bowblis, J.R. Shortages of staff in nursing homes during the COVID-19 pandemic: What are the driving factors? J. Am. Med. Dir. Assoc. 2020, 21, 1371–1377. [Google Scholar] [CrossRef] [PubMed]
- Wingfield, A.H. The Disproportionate Impact of Covid-19 on Black Health Care Workers in the U.S.HBR.org. Available online: https://hbr.org/2020/05/the-disproportionate-impact-of-covid-19-on-black-health-careworkers-in-the-u-s (accessed on 9 September 2022).
- Dos Santos, M.A.; Pereira, F.H.; Caliari, J.D.S.; Oliveira, H.C.; Ceolim, M.F.; Andrechuk, C.R.S. Sleep and Professional Burnout in Nurses, Nursing Technicians, and Nursing Assistants during the COVID-19 Pandemic. J. Nurs. Res. 2022, 30, e218. [Google Scholar] [CrossRef] [PubMed]
- Martínez-López, J.Á.; Lázaro-Pérez, C.; Gómez-Galán, J. Burnout among direct-Care Workers in Nursing Homes during the COVID-19 pandemic in Spain: A preventive and educational focus for sustainable workplaces. Sustainability 2021, 13, 2782. [Google Scholar] [CrossRef]
- Finlay, J.M.; Kobayashi, L.C. Social isolation and loneliness in later life: A parallel convergent mixed-methods case study of older adults and their residential contexts in the Minneapolis metropolitan area, USA. Soc. Sci. Med. 2018, 208, 25–33. [Google Scholar] [CrossRef] [PubMed]
- Vrach, I.T.; Tomar, R. Mental health impacts of social isolation in older people during COVID pandemic. Prog. Neurol. Psychiatry 2020, 24, 25–29. [Google Scholar] [CrossRef]
- Mendoza-Ruvalcaba, N.M.; Gutiérrez-Herrera, R.; López, C.; Hesse, H.; Soto-Añari, M.; Ramos-Henderson, M.; Cárdenas-Valverde, J.C.; Camargo, L.; Caldichoury, N.; Herrera-Pino, J.; et al. Impact of quarantine due to COVID-19 pandemic on health and lifestyle conditions in older adults from Centro American countries. PLoS ONE 2022, 17, e0264087. [Google Scholar] [CrossRef] [PubMed]
- Yildirim, H.; Işik, K.; Aylaz, R. The effect of anxiety levels of elderly people in quarantine on depression during covid-19 pandemic. Soc. Work Public Health 2021, 36, 194–204. [Google Scholar] [CrossRef] [PubMed]
- Garland, E.; Gaylord, S.; Park, J. The role of mindfulness in positive reappraisal. Explore 2009, 5, 37–44. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Duker, A.; Green, D.J.; Onyeador, I.N.; Richeson, J.A. Managing emotions in the face of discrimination: The differential effects of self-immersion, self-distanced reappraisal, and positive reappraisal. Emotion 2021, 22, 1435–1449. [Google Scholar] [CrossRef] [PubMed]
- Aliche, J.C.; Onyishi, I.E. Mindfulness and wellbeing in older adults’ survivors of herdsmen attack. The mediating effect of positive reappraisal. Aging Ment. Health 2020, 24, 1132–1140. [Google Scholar] [CrossRef] [PubMed]
- Nowlan, J.S.; Wuthrich, V.M.; Rapee, R.M. Positive reappraisal in older adults: A systematic literature review. Aging Ment. Health 2015, 19, 475–484. [Google Scholar] [CrossRef]
- Luis, E.; Bermejo-Martins, E.; Martinez, M.; Sarrionandia, A.; Cortes, C.; Oliveros, E.Y.; Fernández-Berrocal, P. Relationship between self-care activities, stress and well-being during COVID-19 lockdown: A cross-cultural mediation model. BMJ Open 2021, 11, e048469. [Google Scholar] [CrossRef] [PubMed]
- Braus, M.; Morton, B. Art therapy in the time of COVID-19. Psychol. Trauma Theory Res. Pract. Policy 2020, 12 (Suppl. S1), S267. [Google Scholar] [CrossRef] [PubMed]
- Martin, L.; Oepen, R.; Bauer, K.; Nottensteiner, A.; Mergheim, K.; Gruber, H.; Koch, S.C. Creative arts interventions for stress management and prevention—A systematic review. Behav. Sci. 2018, 8, 28. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Achour, M.; Azmi, I.B.A.G.; Isahak, M.B.; Nor, M.R.M.; Yusoff, M.Y.Z.M. Job stress and nurses well-being: Prayer and age as moderators. Community Ment. Health J. 2019, 55, 1226–1235. [Google Scholar] [CrossRef] [PubMed]
- Chirico, F.; Sharma, M.; Zaffina, S.; Magnavita, N. Spirituality and prayer on teacher stress and burnout in an Italian cohort: A pilot, before-after controlled study. Front. Psychol. 2020, 10, 2933. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kılınç, T.; Çelik, A.S. Relationship between the social support and psychological resilience levels perceived by nurses during the COVID-19 pandemic: A study from Turkey. Perspect. Psychiatr. Care 2021, 57, 1000–1008. [Google Scholar] [CrossRef]
- Ekwonye, A.U.; Gerdes, S. Exploring the effectiveness of virtual compassionate presence sessions in reducing loneliness and isolation among assisted-living older adults: A pilot study. J. Relig. Spirit. Aging 2021, 34, 174–193. [Google Scholar] [CrossRef]
- Jiménez-Pavón, D.; Carbonell-Baeza, A.; Lavie, C.J. Physical exercise as therapy to fight against the mental and physical consequences of COVID-19 quarantine: Special focus in older people. Prog. Cardiovasc. Dis. 2020, 63, 386. [Google Scholar] [CrossRef] [PubMed]
- Brown, L.; Haines, S.; Amonoo, H.L.; Jones, C.; Woods, J.; Huffman, J.C.; Morris, M.E. Sources of resilience in frontline health professionals during COVID-19. Healthcare 2021, 9, 1699. [Google Scholar] [CrossRef]
- Callow, D.D.; Arnold-Nedimala, N.A.; Jordan, L.S.; Pena, G.S.; Won, J.; Woodard, J.L.; Smith, J.C. The mental health benefits of physical activity in older adults survive the COVID-19 pandemic. Am. J. Geriatr. Psychiatry 2020, 28, 1046–1057. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Demographics | OAs n (%) | FLHWs n (%) |
|---|---|---|
| Gender | ||
| Female | 6 (86%) | 4 (80%) |
| Male | 1 (14%) | 1 (20%) |
| Race/Ethnicity | ||
| Hispanic or Latino | 5 (71%) | 2 (40%) |
| Asian | 1 (14%) | 2 (40%) |
| Native America | 1 (14%) | |
| Black/African American | 1 (20%) | |
| Education | ||
| Some Secondary school | 1 (14% | |
| Some College | 4 (57%) | |
| Undergraduate | 1 (14%) | |
| Post-graduate | 1 (14%) | |
| Freshman | 1 (20%) | |
| Sophomore | 1 (20%) | |
| Junior | 2 (40%) | |
| Graduate | 1 (20%) | |
| Major | ||
| Public Health | 2 (40%) | |
| Pre-nursing | 1 (20%) | |
| Public Policy | 1 (20%) | |
| Masters of Public Health | 1 (20%) | |
| First generation college student | ||
| Yes | 2 (40%) | |
| No | 3 (60%) | |
| Relationship status | ||
| Single (Never married/divorced) | 5 (71%) | 3 (60%) |
| Married | 2 (29%) | 1 (20%) |
| Did not answer | 1 (20%) | |
| Occupation | ||
| Retired | 3 (43%) | |
| Nanny | 1 (14%) | |
| Nurse | 1 (14%) | |
| Clergy | 1 (14%) | |
| Unemployed | 1 (14%) | |
| Religion | ||
| Catholic | 2 (29%) | 1 (20%) |
| Evangelist | 1 (14%) | |
| Christian | 2 (29%) | |
| Buddhism | 1 (14%) | |
| Agnostic | 1 (14%) | 2 (40%) |
| Islam | 1 (20%) | |
| None | 1 (20%) | |
| Born in USA | ||
| Yes | 3 (43%) | 3 (60%) |
| No | 4 (57%) | 2 (40%) |
| Primary language | ||
| Spanish | 4 (57%) | 1 (20%) |
| English | 2 (29%) | 4 (80%) |
| Tibetan | 1 (14%) |
| Session | Content | Objectives | Assessment |
|---|---|---|---|
| Day 1: 3 h | Study overview, grant aims, ethics, methodology | Describe grant rationale, aims, and human subjects research. Explain key aspects of participant engagement, retention, and relationship. Explain ethical photography. | Group Discussion Written Reflection |
| Day 2: 3 h | Detail photovoice implementation plan | Describe photovoice implementation procedure. Demonstrate proficiency in describing the process and tasks to others. | Group Discussion Written Reflection Role play |
| Day 3: 3 h | Myth busting, use of camera, troubleshooting | Explain some misconceptions about aging and working with older adults. Practice using the camera, including troubleshooting. | Group discussion Role play |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ekwonye, A.U.; Malek, A.; Chonyi, T.; Nguyen, S.; Ponce-Diaz, V.; Lau Haller, L.; Farah, I.; Hearst, M. “Pandemic Fatigue! It’s Been Going On since March 2020”: A Photovoice Study of the Experiences of BIPOC Older Adults and Frontline Healthcare Workers during the Pandemic. Healthcare 2022, 10, 1967. https://doi.org/10.3390/healthcare10101967
Ekwonye AU, Malek A, Chonyi T, Nguyen S, Ponce-Diaz V, Lau Haller L, Farah I, Hearst M. “Pandemic Fatigue! It’s Been Going On since March 2020”: A Photovoice Study of the Experiences of BIPOC Older Adults and Frontline Healthcare Workers during the Pandemic. Healthcare. 2022; 10(10):1967. https://doi.org/10.3390/healthcare10101967
Chicago/Turabian StyleEkwonye, Angela U., Abigail Malek, Tenzin Chonyi, Stephanie Nguyen, Valerie Ponce-Diaz, Lisa Lau Haller, Iqra Farah, and Mary Hearst. 2022. "“Pandemic Fatigue! It’s Been Going On since March 2020”: A Photovoice Study of the Experiences of BIPOC Older Adults and Frontline Healthcare Workers during the Pandemic" Healthcare 10, no. 10: 1967. https://doi.org/10.3390/healthcare10101967
APA StyleEkwonye, A. U., Malek, A., Chonyi, T., Nguyen, S., Ponce-Diaz, V., Lau Haller, L., Farah, I., & Hearst, M. (2022). “Pandemic Fatigue! It’s Been Going On since March 2020”: A Photovoice Study of the Experiences of BIPOC Older Adults and Frontline Healthcare Workers during the Pandemic. Healthcare, 10(10), 1967. https://doi.org/10.3390/healthcare10101967