
Herbal Medicines for Post-Acute Sequelae (Fatigue or Cognitive Dysfunction) of SARS-CoV-2 Infection: A Phase 2 Pilot Clinical Study Protocol

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Methods
2.1. Objectives
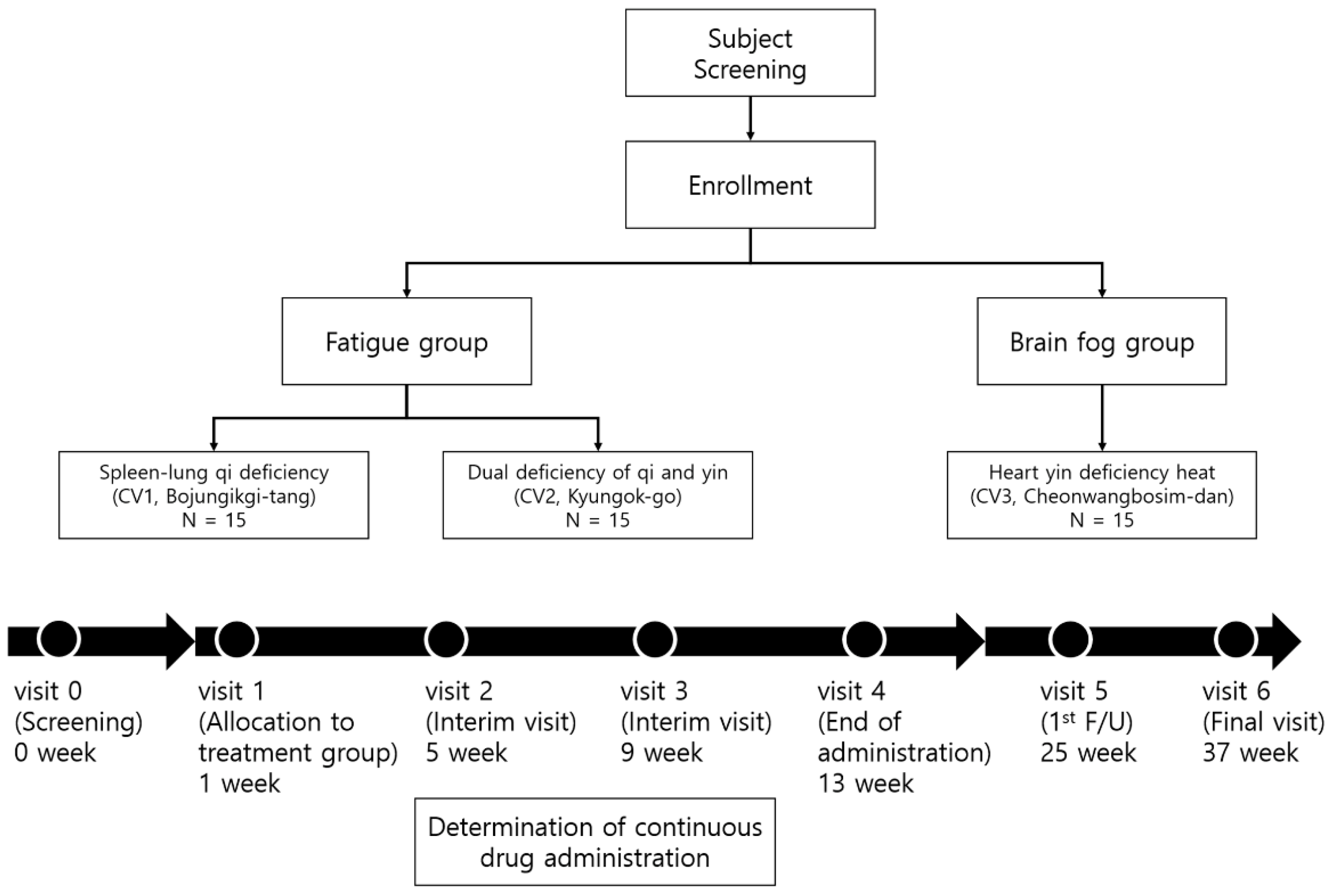
2.2. Study Design
2.3. Sample Size
2.4. Participants
2.4.1. Inclusion Criteria
- Those aged >19 years and have been diagnosed with COVID-19 and recovered. To confirm the COVID-19 diagnosis and recovery, medical history will be examined by reviewing the submitted medical records about the diagnosis, hospitalization, and certificate of SARS-CoV-2 negative or conduct COVID-19 antibody test using the COVID-19 IgM/IgG Plus Test kit (Sugentech, Inc., Daejeon, Korea) approved by the Korean Ministry of Food and Drug Safety. If submission of medical records is possible, the antibody test can be skipped.
- Those who are continuously complaining of fatigue or cognitive dysfunction for >4 weeks that they did not experience before their COVID-19 diagnosis.
- Those who scored a total of >76 points on the Checklist Individual Strength (CIS).
- Participants do not have any problems with overall cognitive function and must be capable of providing written informed consent to participate in the study.
2.4.2. Exclusion Criteria
- Those who have been diagnosed with diseases that can cause fatigue (cancer, sleep disturbance, chronic hepatitis, liver cirrhosis, chronic renal failure, tuberculosis, asthma, multiple sclerosis).
- Those who have been diagnosed with diseases that can cause brain fog (cerebral hemorrhage, cerebral infarction, brain tumor, Parkinson’s disease, epilepsy, major depressive disorder, bipolar affective disorder, schizophrenia, delusional disorder, or dementia).
- Those who have medical problems that may affect the intake or absorption of drugs (dysphagia, clinically serious digestive disorders, galactose intolerance, Lapp lactase deficiency, or glucose-galactose malabsorption).
- Those currently with or have a medical history of allergy to clinical trial drugs (herbal medicines).
- Those who have been diagnosed with liver or kidney disease, or have abnormal levels in blood tests (exceed 3 times the upper limit of normal aspartate aminotransferase (AST), alanine aminotransferase (ALT), blood urine nitrogen (BUN), or creatinine level).
- Pregnant, lactating, and fertile women who have a pregnancy plan.
- Those who have participated in other clinical trials within 30 days of participating in this study.
- Those who are judged to be inappropriate for the clinical trial by the researchers due to clinically significant psychiatric symptoms, physical conditions, laboratory findings or other medical states.
2.4.3. Withdrawal and Discontinuation Criteria
- Acute reaction (allergy, hypersensitivity, and others) to herbal medicine.
- A violation of the inclusion/exclusion criteria is confirmed during the trial.
- No longer possible to administer or make observations due to unexpected diseases or accidents.
- No longer possible to administer or make observations due to severe adverse events or adverse drug reaction.
- The patient is pregnant.
- Withdrawal of consent by patients or their agents.
- It is judged by researchers that the trial is difficult to continue.
2.5. Recruitment
2.6. Blinding and Treatment Allocation
2.7. Intervention
2.8. Outcomes
2.8.1. Primary Outcome
2.8.2. Secondary Outcome
Medication Adherence
Checklist Individual Strength (CIS)
Chalder Fatigue Scale (ChFS) and Subscale
EQ-5D-5L
Pittsburgh Sleep Quality Index (PSQI)-K
Korean-Montreal Cognitive Assessment (K-MoCA)
Cognitive Failure Questionnaire (CFQ)
Beck’s Depression Inventory (BDI)
Digit Span Test in Korean-Wechsler Adult Intelligence Scale (WAIS)
Korean-Boston Naming Test-15 (K-BNT-15)
Analysis of Patient Recruitment Rate, Enrolment Rate, Dropout Rate, and Reasons for Dropout for Feasibility Evaluation
Analysis of Immune Responses and Metabolites
- Single-cell RNA sequencing (scRNA-seq) for immune related gene expressions.
- Flowcytometric analysis for immunophenotyping SARS-CoV-2-specific T cell response.
- Quantitative analysis for inflammatory cytokines, and chemokines in serum sample.
- Quantitative analysis for SARS-CoV-2 antigens (spike or nucleoprotein), specific antibodies (IgG, IgM, or IgA), and neutralizing antibodies in serum samples.
2.9. Safety Evaluation
2.10. Adverse Event Reporting
2.10.1. Assessment of Subjective and Objective Symptoms
2.10.2. Assessment of Measured Tests Such as Laboratory Tests and Vital Signs
2.11. Ethics
2.12. Statistical Analysis
3. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Chopra, V.; Flanders, S.A.; Malani, A.N.; Prescott, H.C. Sixty-Day Outcomes Among Patients Hospitalized with COVID-19. Ann. Intern. Med. 2021, 174, 576–578. [Google Scholar] [CrossRef] [PubMed]
- Townsend, L.; Dyer, A.H.; Jones, K.; Dunne, J.; Mooney, A.; Gaffney, F.; O’Connor, L.; Leavy, D.; O’Brien, K.; Dowds, J.; et al. Persistent fatigue following SARS-CoV-2 infection is common and independent of severity of initial infection. PLoS ONE 2020, 15, e0240784. [Google Scholar] [CrossRef] [PubMed]
- Hampshire, A.; Trender, W.; Chamberlain, S.R.; Jolly, A.E.; Grant, J.E.; Patrick, F.; Mazibuko, N.; Williams, S.C.; Barnby, J.M.; Hellyer, P.; et al. Cognitive deficits in people who have recovered from COVID-19. eClinicalMedicine 2021, 39, 101044. [Google Scholar] [CrossRef] [PubMed]
- Crook, H.; Raza, S.; Nowell, J.; Young, M.; Edison, P. Long covid-mechanisms, risk factors, and management. BMJ 2021, 374, n1648. [Google Scholar] [CrossRef] [PubMed]
- Vercoulen, J.H.M.M.; Swanink, C.M.A.; Fennis, J.F.M.; Galama, J.M.D.; van der Meer, J.W.M.; Bleijenberg, G. Dimensional assessment of chronic fatigue syndrome. J. Psychosom. Res. 1994, 38, 383–392. [Google Scholar] [CrossRef]
- Ha, H.; Jeong, D.; Hahm, B.J.; Shim, E.J. Cross-Cultural Validation of the Korean Version of the Chalder Fatigue Scale. Int. J. Behav. Med. 2018, 25, 351–361. [Google Scholar] [CrossRef]
- Jung, Y.I.; Jeong, E.H.; Lee, H.; Seo, J.; Yu, H.J.; Hong, J.Y.; Sunwoo, M.K. Validation of MoCA-MMSE Conversion Scales in Korean Patients with Cognitive Impairments. Dement. Neurocogn. Disord. 2018, 17, 148–155. [Google Scholar] [CrossRef]
- Broadbent, D.E.; Cooper, P.F.; FitzGerald, P.; Parkes, K.R. The Cognitive Failures Questionnaire (CFQ) and its correlates. Br. J. Clin. Psychol. 1982, 21, 1–16. [Google Scholar] [CrossRef]
- Beck, A.T.; Ward, C.H.; Mendelson, M.; Mock, J.; Erbaugh, J. An inventory for measuring depression. Arch. Gen. Psychiatry 1961, 4, 561–571. [Google Scholar] [CrossRef]
- Kim, H.-K.; Park, T.J. Korean norm for the difference between digits forward and digits backward. Korean J. Clin. Psychol. 2003, 22, 599–613. [Google Scholar]
- Kang, Y.; Kim, H.; Na, D.L. Parallel Short Forms for the Korean-Boston Naming Test (K-BNT). J. Korean Neurol. Assoc. 2000, 18, 144–150. [Google Scholar]
- Kim, H.H.; Kim, S.R. Development of Short Form of the Korean Version- the Boston Naming Test (K-BNT-15) Based on Item Response Theory. J. Korea Contents Assoc. 2013, 13, 321–327. [Google Scholar] [CrossRef] [Green Version]
- Kim, Y.; Kim, S.W.; Chang, H.H.; Kwon, K.T.; Bae, S.; Hwang, S. Significance and Associated Factors of Long-Term Sequelae in Patients after Acute COVID-19 Infection in Korea. Infect. Chemother. 2021, 53, 463–476. [Google Scholar] [CrossRef]
- Bell, M.L.; Catalfamo, C.J.; Farland, L.V.; Ernst, K.C.; Jacobs, E.T.; Klimentidis, Y.C.; Jehn, M.; Pogreba-Brown, K. Post-acute sequelae of COVID-19 in a non-hospitalized cohort: Results from the Arizona CoVHORT. PLoS ONE 2021, 16, e0254347. [Google Scholar] [CrossRef] [PubMed]
- Pellegrini, L.; Albecka, A.; Mallery, D.L.; Kellner, M.J.; Paul, D.; Carter, A.P.; James, L.C.; Lancaster, M.A. SARS-CoV-2 Infects the Brain Choroid Plexus and Disrupts the Blood-CSF Barrier in Human Brain Organoids. Cell Stem Cell 2020, 27, 951–961.e5. [Google Scholar] [CrossRef] [PubMed]
- Peterson, D.; Brenu, E.W.; Gottschalk, G.; Ramos, S.; Nguyen, T.; Staines, D.; Marshall-Gradisnik, S. Cytokines in the cerebrospinal fluids of patients with chronic fatigue syndrome/myalgic encephalomyelitis. Mediat. Inflamm. 2015, 2015, 929720. [Google Scholar] [CrossRef]
- Natelson, B.H.; Weaver, S.A.; Tseng, C.L.; Ottenweller, J.E. Spinal fluid abnormalities in patients with chronic fatigue syndrome. Clin. Diagn. Lab. Immunol. 2005, 12, 52–55. [Google Scholar] [CrossRef]
- Nalbandian, A.; Sehgal, K.; Gupta, A.; Madhavan, M.V.; McGroder, C.; Stevens, J.S.; Cook, J.R.; Nordvig, A.S.; Shalev, D.; Sehrawat, T.S.; et al. Post-acute COVID-19 syndrome. Nat. Med. 2021, 27, 601–615. [Google Scholar] [CrossRef]
- Reichard, R.R.; Kashani, K.B.; Boire, N.A.; Constantopoulos, E.; Guo, Y.; Lucchinetti, C.F. Neuropathology of COVID-19: A spectrum of vascular and acute disseminated encephalomyelitis (ADEM)-like pathology. Acta Neuropathol. 2020, 140, 1–6. [Google Scholar] [CrossRef]
- Garcia, M.A.; Barreras, P.V.; Lewis, A.; Pinilla, G.; Sokoll, L.J.; Kickler, T.; Mostafa, H.; Caturegli, M.; Moghekar, A.; Fitzgerald, K.C.; et al. Cerebrospinal fluid in COVID-19 neurological complications: Neuroaxonal damage, anti-SARS-Cov2 antibodies but no evidence of cytokine storm. J. Neurol. Sci. 2021, 427, 117517. [Google Scholar] [CrossRef]
- Kim, J.W.; Kim, H.J.; Jang, E.S.; Jung, H.; Hwang, M.W.; Nam, D.H. Survey on Pattern Identification and Treatment of Chronic Fatigue in Korea Medicine. J. Physiol. Pathol. Korean Med. 2018, 32, 126–133. [Google Scholar] [CrossRef]
- Nam, D. The Effectiveness of Bojungikgi-tang and its modifications on Chronic Fatigue Syndrome: A Systematic Review And Meta-analysis. J. Korean Med. 2020, 41, 93–106. [Google Scholar] [CrossRef]
- Jang, S.; Kim, D.; Yi, E.; Choi, G.; Song, M.; Lee, E.K. Telemedicine and the Use of Korean Medicine for Patients With COVID-19 in South Korea: Observational Study. JMIR Public Health Surveill. 2021, 7, e20236. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.A.; Jin, S.W.; Kim, S.M.; Lee, G.H.; Kim, S.J.; Lee, W.L.; Na, M.; Jeong, H.G. Anti-fatigue Effect of Kyung-Ok-Ko. Korean J. Pharmacogn. 2016, 47, 258–263. [Google Scholar]
- Choi, K.-W.; Jung, I.-C. The effects of Chenwhangbosindan (CBD) hot water extract & ultra-fine powder on the Alzheimer’s disease model. J. Orient. Neuropsychiatry 2008, 19, 77–93. [Google Scholar]
- Zhu, L.; Xu, X.; Zhu, B.; Guo, X.; Xu, K.; Song, C.; Fu, J.; Yu, H.; Kong, X.; Peng, J.; et al. Kinetics of SARS-CoV-2 Specific and Neutralizing Antibodies over Seven Months after Symptom Onset in COVID-19 Patients. Microbiol. Spectr. 2021, 9, e0059021. [Google Scholar] [CrossRef]
- Pan, Y.; Jiang, X.; Yang, L.; Chen, L.; Zeng, X.; Liu, G.; Tang, Y.; Qian, C.; Wang, X.; Cheng, F.; et al. SARS-CoV-2-specific immune response in COVID-19 convalescent individuals. Signal Transduct. Target Ther. 2021, 6, 256. [Google Scholar] [CrossRef]
- Batabyal, R.; Freishtat, N.; Hill, E.; Rehman, M.; Freishtat, R.; Koutroulis, I. Metabolic dysfunction and immunometabolism in COVID-19 pathophysiology and therapeutics. Int. J. Obes. 2021, 45, 1163–1169. [Google Scholar] [CrossRef]
- Shen, B.; Yi, X.; Sun, Y.; Bi, X.; Du, J.; Zhang, C.; Quan, S.; Zhang, F.; Sun, R.; Qian, L.; et al. Proteomic and Metabolomic Characterization of COVID-19 Patient Sera. Cell 2020, 182, 59–72.e15. [Google Scholar] [CrossRef]
- Naviaux, R.K.; Naviaux, J.C.; Li, K.; Bright, A.T.; Alaynick, W.A.; Wang, L.; Baxter, A.; Nathan, N.; Anderson, W.; Gordon, E. Metabolic features of chronic fatigue syndrome. Proc. Natl. Acad. Sci. USA 2016, 113, E5472–E5480. [Google Scholar] [CrossRef]
- Tomas, C.; Newton, J. Metabolic abnormalities in chronic fatigue syndrome/myalgic encephalomyelitis: A mini-review. Biochem. Soc. Trans. 2018, 46, 547–553. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Visit | 0 | 1 | 2 | 3 | 4 | 5 | 6 | UV * |
|---|---|---|---|---|---|---|---|---|
| Week | −7 | 1 | 5 | 9 | 13 | 25 | 37 | - |
| Visit Window | - | 2 | ±7 | ±7 | ±7 | ±7 | ±7 | - |
| Informed consent for the study | ● | |||||||
| Demographic information | ● | |||||||
| Participation in other clinical trials | ● | |||||||
| Medical history | ● | |||||||
| Confirmation of diagnosis of COVID-19 infection | ● | |||||||
| Medication history | ● | |||||||
| Vital signs | ● | ● | ● | ● | ● | ● | ● | ● |
| Electrocardiogram | ● | ● | ● | |||||
| Laboratory test | ● | ● | ● | |||||
| Blood collection for immune response and metabolite analysis | ● | ● | ● | ● | ● | |||
| Pregnancy ** | ● | |||||||
| Evaluation of fatigue or brain fog | ● | |||||||
| CIS | ● | ● | ● | ● | ● | ● | ● | |
| VAS (0–100) score for fatigue or brain fog | ● | ● | ● | ● | ● | ● | ● | |
| Inclusion/exclusion criteria | ● | |||||||
| KM syndrome differentiation | ● | |||||||
| Prescription of herbal medicine *** | ● | ○ | ○ | |||||
| Drug adherence | ● | ● | ● | ● | ||||
| Check for combination therapy | ● | ● | ● | ● | ● | ● | ||
| ChFQ | ● | ● | ● | ● | ● | ● | ● | |
| EQ-5D-5L | ● | ● | ● | ● | ● | ● | ● | |
| PSQI-K | ● | ● | ● | ● | ● | ● | ● | |
| K-MoCA | ● | ● | ● | ● | ● | ● | ● | |
| CFQ | ● | ● | ● | |||||
| BDI | ● | ● | ● | ● | ● | ● | ● | |
| Digit span test in K-WAIS (DF, DB, and DF-DB) | ● | ● | ● | ● | ||||
| K-BNT-15 | ● | ● | ● | ● | ||||
| Adverse events check | ● | ● | ● | ● | ● | ● | ● |
| Fatigue | Cognitive Dysfunction | ||
|---|---|---|---|
| Code | CV1 | CV2 | CV3 |
| Syndrome differentiation classification | Spleen-lung qi deficiency pattern | Dual deficiency of qi and yin pattern | Heart yin deficiency heat pattern |
| Symptom | Fatigue, appetite loss, cold sweat, shortness of breath, chest tightness, anxiety and others | Fatigue, dry cough and others | Forgetfulness, fever, insomnia, heart palpitation, stomatitis, tongue needles and others |
| Tongue diagnosis | Pale tongue, thin white fur | Dry mouth, dry tongue | Red tongue and low tongue coated |
| Pulse diagnosis | Vacuous, large, weak pulse/surging, large pulse | Fine pulse/vacuous, weak pulse | Fine, rapid pulse |
| Urine/feces | Difficult stool to pass/sloppy stool | Dry stool | Inhibited stool/sloppy stool |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jegal, K.H.; Yoon, J.; Kim, S.; Jang, S.; Jin, Y.-H.; Lee, J.-H.; Choi, S.-M.; Kim, T.H.; Kwon, S. Herbal Medicines for Post-Acute Sequelae (Fatigue or Cognitive Dysfunction) of SARS-CoV-2 Infection: A Phase 2 Pilot Clinical Study Protocol. Healthcare 2022, 10, 1839. https://doi.org/10.3390/healthcare10101839
Jegal KH, Yoon J, Kim S, Jang S, Jin Y-H, Lee J-H, Choi S-M, Kim TH, Kwon S. Herbal Medicines for Post-Acute Sequelae (Fatigue or Cognitive Dysfunction) of SARS-CoV-2 Infection: A Phase 2 Pilot Clinical Study Protocol. Healthcare. 2022; 10(10):1839. https://doi.org/10.3390/healthcare10101839
Chicago/Turabian StyleJegal, Kyung Hwan, Jiwon Yoon, Sanghyun Kim, Soobin Jang, Young-Hee Jin, Jun-Hwan Lee, Sun-Mi Choi, Tae Hun Kim, and Sunoh Kwon. 2022. "Herbal Medicines for Post-Acute Sequelae (Fatigue or Cognitive Dysfunction) of SARS-CoV-2 Infection: A Phase 2 Pilot Clinical Study Protocol" Healthcare 10, no. 10: 1839. https://doi.org/10.3390/healthcare10101839
APA StyleJegal, K. H., Yoon, J., Kim, S., Jang, S., Jin, Y.-H., Lee, J.-H., Choi, S.-M., Kim, T. H., & Kwon, S. (2022). Herbal Medicines for Post-Acute Sequelae (Fatigue or Cognitive Dysfunction) of SARS-CoV-2 Infection: A Phase 2 Pilot Clinical Study Protocol. Healthcare, 10(10), 1839. https://doi.org/10.3390/healthcare10101839