
Factor Analysis of Quality Management Systems Implementation in Healthcare: An Online Survey
 , and
, and
Abstract
1. Introduction
2. Materials and Methods
2.1. Operational Research Model Development
2.2. Survey Design and Exclusion Criteria
2.3. Sampling Approach
2.4. Pilot Test
3. Results
3.1. The Exploratory Factor Analysis (EFA)
3.2. Reliability Analysis (Cronbach’s Alpha)
3.3. Analysis of Relationships
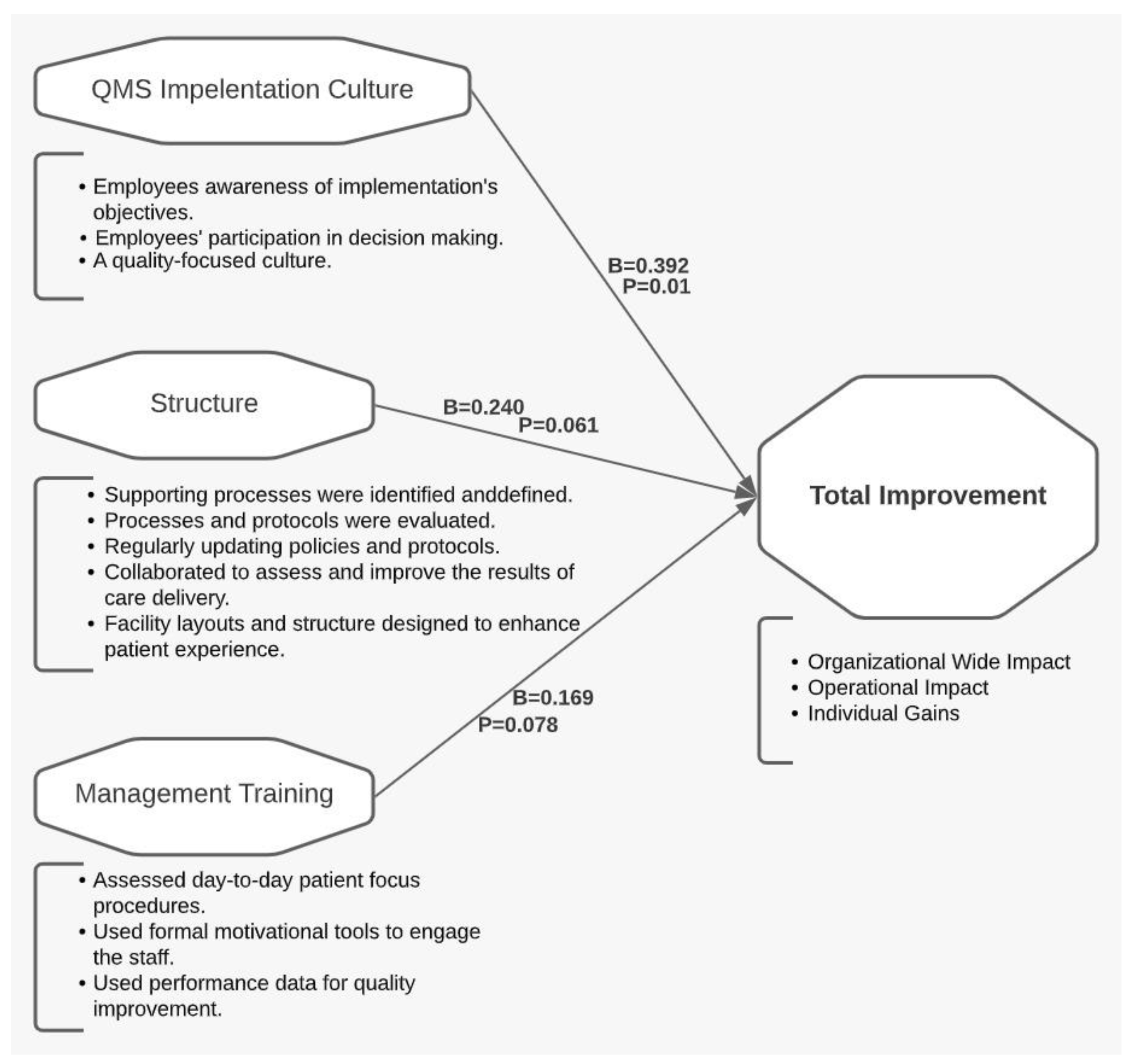
3.4. Regression Modeling
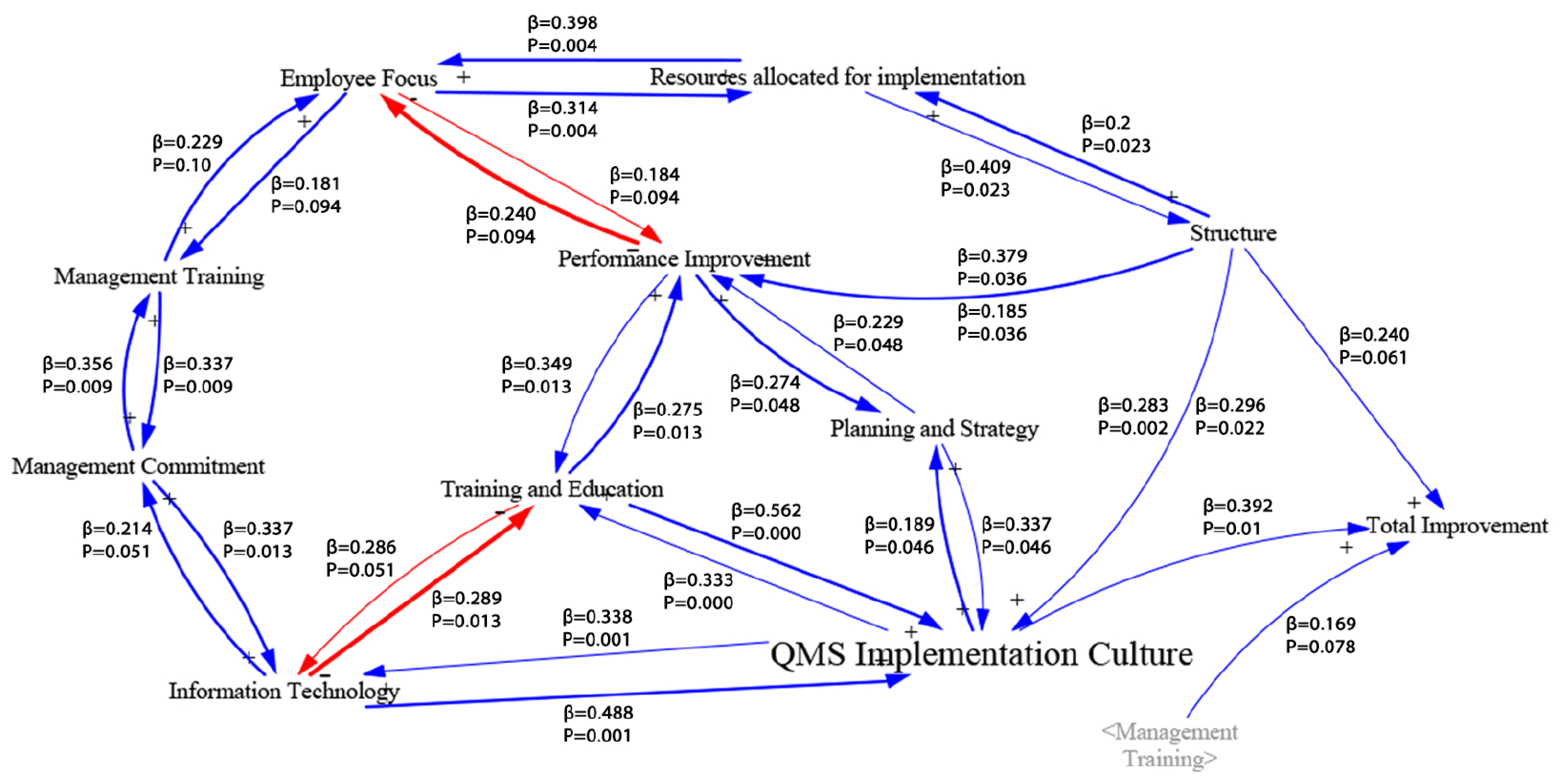
3.5. Investigation of Interrelationships among Factors
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Conflicts of Interest
Appendix A. Survey Protocol
- “Factors that Affect the Successful Implementation of Quality Management Systems in Healthcare”
| Skip To: Beginning of Survey If Factors that Affect the Successful Implementation of Quality Management Systems in Healthcare Y = Yes, I would like to complete the survey |
| Skip To: End of Survey If Factors that Affect the Successful Implementation of Quality Management Systems in Healthcare N = No, I do not want to participate in this survey |
- General demographic information.
- Likert-style questions to assess factors and outcomes of implementation based on your experience.
| Q1.1 Instructions: This section consists of a few questions to gain more information about your background and provides the context for your responses. Consider the last QMS implementation that you participated in or observed in healthcare. |
| Q1.2 What is your Current Position? |
| Quality Professional |
| Administrative |
| Medical Staff (Physician, Nurses, etc.) |
| Researcher |
| Other ________________________________________________ |
| Q1.3 How many years of experience do you have in quality management? |
| Less than 2 years |
| 3–5 years |
| 6–10 years |
| More than 10 years |
| Q1.4 When was the last time that you participated in or observed the implementation of a new or significantly redesigned Quality Management System (QMS) in a healthcare organization? |
| 1–2 years |
| 3–5 years |
| More than 5 years ago |
| I have never observed or implemented a QMS in a healthcare organization. |
| Skip To: End of Survey If When was the last time that you participated in or observed the implementation of a new or modified QMS = I have never observed or implemented a QMS in a healthcare organization |
| Q1.5 Which type of healthcare did you experience or observe QMS implementation in? |
| Public |
| Private |
| Q1.6 Which area(s) of healthcare was the focus on the QMS implementation? |
| Hospital |
| College Medical Center |
| Single department (i.e., operating room) |
| Outpatient care center (i.e., urgent care) |
| Physician’s offices |
| Medical and Diagnostic laboratories |
| Other ________________________________________________ |
| Q1.7 Which best describes the size of the healthcare organizations? |
| Small: Fewer than 99 employees |
| Medium: 100 to 499 employees |
| Large: 500 to 2499 employees |
| Corporate: More than 2500 employees |
| Q1.8 Which of the following accreditation/certifications/philosophies were used to develop the QMS that you helped to implement? (select all that apply) |
| ISO 9001 (International Standards Organization) |
| EFQM (European Foundation for Quality Management) |
| MBNQA (Malcolm Baldrige National Quality Award) |
| TQM (Total Quality Management) |
| None/customized system |
| Other ________________________________________________ |
| Q1.9 What role (or roles) did you serve during the QMS implementation? (select all that apply) |
| Team Leader |
| Facilitator |
| Champion |
| Process Owner |
| Team Member |
| Management |
| Observer/Studying |
| Other ________________________________________________ |
| Q1.10 In general, how successful was the last implementation that you participated in or observed? |
| Extremely successful |
| Very successful |
| Moderately successful |
| Slightly successful |
| Not successful at all |
| Q2.1 Instructions: Below are questions regarding QMS implementation factors that are studied in the literature. It is important to note that we are interested in your experiences or opinions. |
| Q2.2 To what Extent do You Agree or Disagree with the Following Statements? | Strongly Disagree | Disagree | Neither Agree nor Disagree | Agree | Strongly Agree |
| Management was involved in quality improvement activities. | 1 | 2 | 3 | 4 | 5 |
| Management was committed to high-quality services. | 1 | 2 | 3 | 4 | 5 |
| Management monitored the execution of quality improvement plans. | 1 | 2 | 3 | 4 | 5 |
| Management clearly communicated expectations for care professionals regarding quality improvement. | 1 | 2 | 3 | 4 | 5 |
| Management used performance data for quality improvement. | 1 | 2 | 3 | 4 | 5 |
| Management assessed care-professionals’ compliance with day-to-day patient safety procedures. | 1 | 2 | 3 | 4 | 5 |
| Management used formal motivational tools to engage the staff. | 1 | 2 | 3 | 4 | 5 |
| Q3.1 Instructions: Below are questions regarding QMS implementation factors that are studied in the literature. It is important to note that we are interested in your experiences. |
| Q3.2 To what Extent do You Agree or Disagree with the Following Statements? | Strongly Disagree | Disagree | Neither Agree nor Disagree | Agree | Strongly AGREE |
| Differences in patients’ expectations and actual service was communicated to employees. | 1 | 2 | 3 | 4 | 5 |
| Employees’ feedback was part of decision making. | 1 | 2 | 3 | 4 | 5 |
| Employees were involved in quality activities. | 1 | 2 | 3 | 4 | 5 |
| Employees were aware of the QMS implementation objectives. | 1 | 2 | 3 | 4 | 5 |
| Adequate quality education and training were provided when needed. | 1 | 2 | 3 | 4 | 5 |
| Learning and comprehension of quality tools and principles were evaluated. | 1 | 2 | 3 | 4 | 5 |
| Employees assigned to QMS tasks were competent. | 1 | 2 | 3 | 4 | 5 |
| Employees’ satisfaction with the QMS was measured. | 1 | 2 | 3 | 4 | 5 |
| Employees were appropriately recognized or rewarded for engagement in the implementation effort. | 1 | 2 | 3 | 4 | 5 |
| There were sufficient resources to support quality projects/processes. | 1 | 2 | 3 | 4 | 5 |
| There were adequate staff in support of the QMS. | 1 | 2 | 3 | 4 | 5 |
| There was adequate funding for QMS purposes. | 1 | 2 | 3 | 4 | 5 |
| Data generated from information management systems were used for improvement. | 1 | 2 | 3 | 4 | 5 |
| The organization used an information management system. | 1 | 2 | 3 | 4 | 5 |
| Quality data and information were analyzed. | 1 | 2 | 3 | 4 | 5 |
| Communication between different levels of management was effective. | 1 | 2 | 3 | 4 | 5 |
| Adequate time was allocated for staff to conduct quality tasks. | 1 | 2 | 3 | 4 | 5 |
| The organization had a quality-focused culture. | 1 | 2 | 3 | 4 | 5 |
| Staff easily adopted quality concepts. | 1 | 2 | 3 | 4 | 5 |
| Q4.1 Instructions: Below are questions regarding QMS implementation factors that are studied in the literature. It is important to note that we are interested in your experiences. |
| Q4.2 To what Extent do You Agree or Disagree with the Following Statements? | Strongly Disagree | Disagree | Neither Agree nor Disagree | Agree | Strongly Agree |
| Supporting processes were identified and defined. | 1 | 2 | 3 | 4 | 5 |
| The organization regularly updated their policies and protocols. | 1 | 2 | 3 | 4 | 5 |
| Processes and protocols were regularly evaluated. | 1 | 2 | 3 | 4 | 5 |
| The organization had a formal process to continuously revise the QMS. | 1 | 2 | 3 | 4 | 5 |
| The organization considered customer needs in process improvement activities. | 1 | 2 | 3 | 4 | 5 |
| The organization regularly evaluated the QMS function (i.e., internal audits). | 1 | 2 | 3 | 4 | 5 |
| Different roles collaborated to assess and improve the results of care delivery. | 1 | 2 | 3 | 4 | 5 |
| Performance indicators were compared with other healthcare organizations to identify opportunities for improvement. | 1 | 2 | 3 | 4 | 5 |
| Patients were periodically requested to give their opinions on the care provided. | 1 | 2 | 3 | 4 | 5 |
| A periodical evaluation of complaints was used to implement improvements. | 1 | 2 | 3 | 4 | 5 |
| The organization pursued long-term organizational goals and policies. | 1 | 2 | 3 | 4 | 5 |
| The organization integrated quality in the strategic plan. | 1 | 2 | 3 | 4 | 5 |
| Policies and strategies were developed according to current and future needs. | 1 | 2 | 3 | 4 | 5 |
| Facility layouts and structure were designed to enhance patient experience. | 1 | 2 | 3 | 4 | 5 |
| Q5.1 Instructions: Below are questions regarding the primary benefits of successfully implementing a QMS. It is important to note that we are interested in your experiences. |
| Q5.2 To what Extent do You Agree or Disagree that QMS Implementation Resulted in: | Strongly Disagree | Disagree | Neither Agree nor Disagree | Agree | Strongly Agree |
| Improved organizational performance. | 1 | 2 | 3 | 4 | 5 |
| Achievement of related accreditation or awards. | 1 | 2 | 3 | 4 | 5 |
| Increased quality of services provided. | 1 | 2 | 3 | 4 | 5 |
| Developing a sense of responsibility sharing. | 1 | 2 | 3 | 4 | 5 |
| Enhanced stakeholders’ satisfaction. | 1 | 2 | 3 | 4 | 5 |
| Redesigned procedures and standards. | 1 | 2 | 3 | 4 | 5 |
| Enhanced communication among different levels of employees. | 1 | 2 | 3 | 4 | 5 |
| Increased employee organizational commitment. | 1 | 2 | 3 | 4 | 5 |
| Increased employee motivation. | 1 | 2 | 3 | 4 | 5 |
References
- A’Aqoulah, A.; Kuyini, A.B.; Ajlouni, M.T. Addressing Quality Management System Obstacles in Jordanian Hospitals. Int. Bus. Res. 2016, 9, 34. [Google Scholar] [CrossRef][Green Version]
- World Health Organization. Improving Healthcare Quality in Europe Characteristics, Effectiveness and Implementation of Different Strategies: Characteristics, Effectiveness and Implementation of Different Strategies; WHO: Geneva, Switzerland, 2019.
- Wagner, C.; De Bakker, D.H.; Groenewegen, P. A measuring instrument for evaluation of quality systems. Int. J. Qual. Health Care 1999, 11, 119–130. [Google Scholar] [CrossRef] [PubMed]
- Psychogios, A.G.; Atanasovski, J.; Tsironis, L.K. Lean Six Sigma in a service context: A multi-factor application approach in the telecommunications industry. Int. J. Qual. Reliab. Manag. 2012, 29, 122–139. [Google Scholar] [CrossRef]
- Hietschold, N.; Reinhardt, R.; Gurtner, S. Measuring critical success factors of TQM implementation successfully—A systematic literature review. Int. J. Prod. Res. 2014, 52, 6254–6272. [Google Scholar] [CrossRef]
- Aquilani, B.; Silvestri, C.; Ruggieri, A.; Gatti, C. A systematic literature review on total quality management critical success factors and the identification of new avenues of research. TQM J. 2017, 29, 184–213. [Google Scholar] [CrossRef]
- Donabedian, A. The quality of care: How can it be assessed? JAMA 1988, 260, 1743–1748. [Google Scholar] [CrossRef]
- Tamer, G.; Çetinkaya, H. Impact of quality management system on health institutions. Health Care Acad. J. 2018, 5, 97–101. [Google Scholar] [CrossRef]
- Moldovan, F.; Blaga, P.; Moldovan, L.; Bataga, T. An Innovative Framework for Sustainable Development in Healthcare: The Human Rights Assessment. Int. J. Environ. Res. Public Health 2022, 19, 2222. [Google Scholar] [CrossRef] [PubMed]
- Abdallah, A. Implementing quality initiatives in healthcare organizations: Drivers and challenges. Int. J. Health Care Qual. Assur. 2014, 27, 166–181. [Google Scholar] [CrossRef]
- Committee, H.T. A Hospital-Based Healthcare Quality Management System Model; Healthcare Technical Committee: Milwaukee, WI, USA, 2016. [Google Scholar]
- Sousa, R.; Voss, C. Quality management re-visited: A reflective review and agenda for future research. J. Oper. Manag. 2002, 20, 91–109. [Google Scholar] [CrossRef]
- Moukhafi, S. Hospital quality management: A historical foundation. Rev. Econ. Gest. Soc. 2021, 1, 32. [Google Scholar]
- Bortolotti, T.; Boscari, S.; Danese, P.; Suni, H.A.M.; Rich, N.; Romano, P. The social benefits of kaizen initiatives in healthcare: An empirical study. Int. J. Oper. Prod. Manag. 2018, 38, 554–578. [Google Scholar] [CrossRef]
- Parast, M.M.; Golmohammadi, D. Quality management in healthcare organizations: Empirical evidence from the baldrige data. Int. J. Prod. Econ. 2019, 216, 133–144. [Google Scholar] [CrossRef]
- Kelly, D.L. Applying Quality Management in Healthcare: A Systems Approach; Health Administration Press: Chicago, IL, USA, 2007. [Google Scholar]
- Alaraki, M.S. The Impact of Critical Total Quality Management Practices on Hospital Performance in the Ministry of Health Hospitals in Saudi Arabia. Qual. Manag. Health Care 2014, 23, 59–63. [Google Scholar] [CrossRef]
- Unger, K.L. An Investigation into the Effects of Winning the Malcolm Baldrige National Quality Award on the Performance of Hospitals/Healthcare Systems; Colorado State University: Fort Collins, CO, USA, 2013. [Google Scholar]
- Aburayya, A.; Alshurideh, M.; Marzouqi, A.A.; Diabat, O.A.; Alfarsi, A.; Suson, R.; Bash, M.; Salloum, S.A. An empirical examination of the effect of TQM practices on hospital service quality: An assessment study in UAE hospitals. Syst. Rev. Pharm. 2020, 11, 347–362. [Google Scholar]
- Wardhani, V.; Utarini, A.; van Dijk, J.P.; Post, D.; Groothoff, J.W. Determinants of quality management systems implementation in hospitals. Health Policy 2009, 89, 239–251. [Google Scholar] [CrossRef]
- Ali Mohammad, M. Why TQM does not work in Iranian healthcare organisations. Int. J. Health Care Qual. Assur. 2014, 27, 320–335. [Google Scholar] [CrossRef]
- Ali Mohammad, M. Obstacles to TQM success in health care systems. Int. J. Health Care Qual. Assur. 2013, 26, 147–173. [Google Scholar] [CrossRef]
- Hasanali, F. Critical Success Factors of Knowledge Management. 2002. Available online: http://www.providersedge.com/docs/km_articles/Critical_Success_Factors_of_KM.pdf (accessed on 3 November 2020).
- Mosadeghrad, A.M.; Jaafaripooyan, E.; Dehnavi, H. Critical success factors of hospitals: A qualitative study. J. Iran. Inst. Health Sci. Res. 2022, 21, 237–253. [Google Scholar] [CrossRef]
- Aburayya, A.; Alshurideh, M.; Al Marzouqi, A.; Al Diabat, O.; Alfarsi, A.; Suson, R.; Salloum, S.A.; Alawadhi, D.; Alzarouni, A. Critical Success Factors Affecting the Implementation of TQM in Public Hospitals: A Case Study in UAE Hospitals. Syst. Rev. Pharm. 2020, 11, 230–242. [Google Scholar]
- Claver, E.; Tarí, J.J.; Molina, J.F. Critical factors and results of quality management: An empirical study. Total Qual. Manag. Bus. Excel. 2003, 14, 91–118. [Google Scholar] [CrossRef]
- Rawshdeh, M. Factors that Affect the Successful Implementation of Quality Management Systems in Healthcare; University of Central Florida: Orlando, FL, USA, 2021. [Google Scholar]
- Mosadeghrad, A.M. Developing and validating a total quality management model for healthcare organisations. TQM J. 2015, 27, 544–564. [Google Scholar] [CrossRef]
- Joshi, A.; Kale, S.; Chandel, S.; Pal, D.K. Likert scale: Explored and explained. Curr. J. Appl. Sci. Technol. 2015, 7, 396–403. [Google Scholar] [CrossRef]
- Etikan, I.; Musa, S.A.; Alkassim, R.S. Comparison of Convenience Sampling and Purposive Sampling. Am. J. Theor. Appl. Stat. 2016, 5, 1–4. [Google Scholar] [CrossRef]
- de Winter, J.C.F.; Dodou, D.; Wieringa, P.A. Exploratory Factor Analysis with Small Sample Sizes. Multivar. Behav. Res. 2009, 44, 147–181. [Google Scholar] [CrossRef]
- Sapnas, K.G.; Zeller, R.A. Minimizing Sample Size When Using Exploratory Factor Analysis for Measurement. J. Nurs. Meas. 2002, 10, 135–154. [Google Scholar] [CrossRef]
- Watkins, M.W. Exploratory Factor Analysis: A Guide to Best Practice. J. Black Psychol. 2018, 44, 219–246. [Google Scholar] [CrossRef]
- Baruch, Y.; Holtom, B.C. Survey response rate levels and trends in organizational research. Hum. Relat. 2008, 61, 1139–1160. [Google Scholar] [CrossRef]
- Hair, J.F. Multivariate Data Analysis; Prentice Hall: Upper Saddle River, NJ, USA, 1998; Volume 5. [Google Scholar]
- Andrich, D. Relationships Between the Thurstone and Rasch Approaches to Item Scaling. Appl. Psychol. Meas. 1978, 2, 451–462. [Google Scholar] [CrossRef]
- Thompson, B. Exploratory and Confirmatory Factor Analysis: Understanding Concepts and Applications. Appl. Psychol. Meas. 2017, 31, 245–248. [Google Scholar]
- Cohen, P.; West, S.G.; Aiken, L.S. Applied Multiple Regression/Correlation Analysis for the Behavioral Sciences; Routledge: London, UK, 2013. [Google Scholar]
- Oladimeji, O. Developing Causal Relationships for the Performance Measurement Implementation Process. In Proceedings of the International Annual Conference of the American Society for Engineering Management, Philadelphia, PA, USA, 23–26 October 2019; American Society for Engineering Management (ASEM): Huntsville, AL, USA, 2019. [Google Scholar]
- Sterman, J.D. System Dynamics Modeling: Tools for Learning in a Complex World. Calif. Manag. Rev. 2001, 43, 8–25. [Google Scholar] [CrossRef]
- Littlejohns, L.B.; Baum, F.; Lawless, A.; Freeman, T. The value of a causal loop diagram in exploring the complex interplay of factors that influence health promotion in a multisectoral health system in Australia. Health Res. Policy Syst. 2018, 16, 126. [Google Scholar] [CrossRef] [PubMed]
- Rad, A.M.M. The impact of organizational culture on the successful implementation of total quality management. TQM Mag. 2006, 18, 606–625. [Google Scholar]
- Buciuniene, I.; Malciankina, S.; Lydeka, Z.; Kazlauskaite, R. Managerial attitude to the implementation of quality management systems in Lithuanian support treatment and nursing hospitals. BMC Health Serv. Res. 2006, 6, 120. [Google Scholar] [CrossRef] [PubMed]
- Kash, B.A.; Spaulding, A.; Johnson, C.E.; Gamm, L. Success factors for strategic change initiatives: A qualitative study of healthcare administrators’ perspectives. J. Health Manag. 2014, 59, 65–81. [Google Scholar] [CrossRef]
- Bravi, L.; Murmura, F.; Santos, G. The ISO 9001: 2015 quality management system standard: Companies’ drivers, benefits and barriers to its implementation. Qual. Innov. Prosper. 2019, 23, 64–82. [Google Scholar] [CrossRef]
- Creswell, J.W.; Klassen, A.C.; Clark, V.L.P.; Smith, K.C. Best Practices for Mixed Methods Research in Health Sciences, 2nd ed.; National Institutes of Health: Bethesda, MD, USA, 2011. [Google Scholar]
- Seetharaman, A.; Sreenivasan, J.; Boon, L.P. Critical Success Factors of Total Quality Management. Qual. Quant. 2006, 40, 675–695. [Google Scholar] [CrossRef]
- Sila, I.; Ebrahimpour, M. Examination and comparison of the critical factors of total quality management (TQM) across countries. Int. J. Prod. Res. 2003, 41, 235–268. [Google Scholar] [CrossRef]
- Sila, I.; Ebrahimpour, M. An investigation of the total quality management survey based research published between 1989 and 2000. Int. J. Qual. Reliab. Manag. 2002, 19, 902–970. [Google Scholar] [CrossRef]
- Karuppusami, G.; Gandhinathan, R. Pareto analysis of critical success factors of total quality management: A literature review and analysis. TQM Mag. 2006, 18, 372–385. [Google Scholar] [CrossRef]
- Alves, J.; Meneses, R. Silos mentality in healthcare services. In Proceedings of the 11th Annual Conference of the EuroMed Academy of Business, Valletta, Malta, 12–14 September 2018. [Google Scholar]
- Caseiro, J.; Meneses, R. Is Silo Mentality Relevant in Healthcare? The Healthcare Professional’s View. In Proceedings of the STRATEGICA, Bucharest, Romania, 10–11 October 2019; p. 636. [Google Scholar]
- Mosadeghrad, A.M. Essentials of total quality management: A meta-analysis. Int. J. Health Care Qual. Assur. 2014, 27, 544–558. [Google Scholar] [CrossRef]
- Adeoti, J.O. Total quality management (TQM) factors: An empirical study of Kwara state government hospitals. Stud. Ethno-Med. 2011, 5, 17–23. [Google Scholar] [CrossRef]
- Friedrich, T.L.; Byrne, C.L.; Mumford, M.D. Methodological and theoretical Considerations in survey research. Leadership Q. 2009, 20, 57–60. [Google Scholar] [CrossRef]
- Cattell, R. The Scientific Use of Factor Analysis In Behavioral and Life Sciences; Springer Science & Business Media: Berlin, Germany, 2012. [Google Scholar]



{kind=link}
{kind=link}
| Factor Group | Factor | Acronyms and Item No. | Sub-Code | Integrated Frequency |
|---|---|---|---|---|
| Management | Management Commitment | MC1 | Management Involvement | 9% |
| MC2 | Management Oversight | |||
| MC3 | Engagement of Top Leaders | |||
| Management Training | MT1 | Clear Expectation | 4% | |
| MT2 | Compliance Assessment | |||
| MT3 | Motivate Staff | |||
| MT4 | Analyze Data | |||
| Organization Culture | Employees Involvement | EI1 | Employee Engagement | 10% |
| EI2 | Reward | |||
| EI3 | Awareness of QMS | |||
| EI4 | Employee Satisfaction | |||
| EI5 | Feedback Role | |||
| Resistance to Change | RC1 | Adoption | 6.5% | |
| RC2 | Quality-Focused | |||
| Training and Education | TE1 | Quality Education | 11% | |
| TE2 | Learning Evaluation | |||
| TE3 | Competency | |||
| Communication | C1 | Deliver Expectation | 10.5% | |
| C2 | Communication Among Levels | |||
| Resources Allocated for Implementation | R1 | Support Process | 14.5% | |
| R2 | Funding | |||
| R3 | Adequate Staffing | |||
| R4 | Dedicate Time | |||
| Information Technology | IT1 | Information Management System | 5.5% | |
| IT2 | Data for Improvement | |||
| IT3 | Data Analysis | |||
| Structure | Processes and Procedures | PP1 | Identify Process | 6.5% |
| PP2 | Evaluate Process | |||
| PP3 | Update Protocols | |||
| Performance | PER1 | Complaints’ Evaluation | 3.5% | |
| PER2 | Performance Indicators | |||
| PER3 | Continuous Improvement | |||
| Customer Focus | CF1 | Patient Focus | 5% | |
| CF2 | Patient Feedback | |||
| CF3 | Patient Experience | |||
| QMSs’ Review and Audit | AUD1 | Internal Audit | 4.5% | |
| AUD2 | Collaboration | |||
| Strategic Planning | SP1 | Long-term Goals | 16.5% | |
| SP2 | Align Strategies | |||
| SP3 | Quality Integration |
| Outcome | Acronym | Sub-Code | Aggregate Frequency |
|---|---|---|---|
| Organizational Wide Impact | OI1 | ORG Performance | 35% |
| OI2 | ORG Achievement | ||
| OI3 | Responsibility Sense | ||
| Operational Impact | OP1 | Service Improvement | 30% |
| OP2 | Processes Redesign | ||
| OP3 | Enhanced Communication | ||
| Individual gains | IG1 | Raised Commitment | 35% |
| IG2 | Improved Motivation | ||
| IG3 | Increased Satisfaction |
| Model | Emergent Factor | Items | ||||||
|---|---|---|---|---|---|---|---|---|
| Model 1 | Factor 1 (Management Commitment) | MC1 | MC2 | MC3 | MT1 | |||
| Factor 2 (Management Training) | MT2 | MT3 | MT4 | |||||
| Factor 3 (Planning and Strategy) | SP1 | SP2 | SP3 | |||||
| Model 2 | Factor 4 (QMSs’ Implementation Culture) | EI5 | EI3 | RC2 | ||||
| Factor 5 (Employee Focus) | C2 | EI2 | EI4 | |||||
| Model 3 | Factor 6 (Resources allocated for implementation) | R1 | R2 | R3 | R4 | |||
| Factor 7 (Training and Education) | TE1 | TE2 | TE3 | |||||
| Factor 8 (Information Technology) | IT1 | IT2 | IT3 | |||||
| Model 4 | Factor 9 (Performance Improvement) | PP3 | PER3 | CF1 | AUD1 | PER2 | CF2 | PER1 |
| Factor 10 (Structure) | PP2 | PP3 | PP1 | AUD2 | CF3 | |||
| Outcome | Outcome (Total Improvement) | OI1 | OI2 | OI3 | OP1 | OP2 | OP3 | IG1 |
| IG2 | IG3 | |||||||
| Model | Initial Factor | K | N:P | KMO | Cumulative Variance | Determinant | Number of New Factors |
|---|---|---|---|---|---|---|---|
| Model 1: Management |
| 10 | 7:1 | 0.837 | 66% | 0.002 | 3 |
| Model 2: Culture |
| 9 | 8:1 | 0.805 | 55% | 0.023 | 2 |
| Model 3: Implementation resources |
| 10 | 7:1 | 0.809 | 63% | 0.004 | 3 |
| Model 4: Structure |
| 11 | 7:1 | 0.833 | 52% | 0.001 | 2 |
| Model 5: Implementation outcomes |
| 9 | 8:1 | 0.833 | 52% | 0.001 | 1 |
| Factor | Reliability |
|---|---|
| Management Commitment | 0.903 |
| Management Training | 0.740 |
| Planning and Strategy | 0.856 |
| QMSs’ Implementation Culture | 0.841 |
| Employee Focus | 0.716 |
| Resources Allocated for Implementation | 0.852 |
| Training and Education | 0.814 |
| Information Technology | 0.818 |
| Performance Improvement | 0.875 |
| Structure | 0.749 |
| Implementation Success Outcomes | 0.908 |
| Model | STD. Coefficients (BETA) | B | T | SIG | |
|---|---|---|---|---|---|
| R2 | 0.713 | Constant | 1.134 | 0.0261 | |
| ADJ.R2 | 0.666 | Factor 1 (Management Commitment) | 0.063 | 0.645 | 0.522 |
| STD Error | 0.418 | Factor 2 (Management Training) | 0.169 | 1.795 | 0.078 |
| Durbin−Watson | 2.3 | Factor 3 (Planning and Strategy) | −0.043 | −0.389 | 0.699 |
| ANOVA | Factor 4 (QMSs’ Implementation Culture) | 0.392 | 2.643 | 0.010 | |
| F | 14.936 | Factor 5 (Employee Focus | −0.020 | −0.187 | 0.852 |
| Sig | 0.000 | Factor 6 (Resources Allocated For Implementation) | 0.161 | 1.593 | 0.116 |
| Factor 7 (Training and Education) | 0.185 | 1.645 | 0.105 | ||
| Factor 8 (Information Technology) | −0.149 | −1.242 | 0.219 | ||
| Factor 9 (Performance Imrovment) | 0.146 | 1.444 | 0.154 | ||
| Factor 10 (Structure) | 0.240 | 1.909 | 0.061 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rawshdeh, M.; Keathley, H.; Obeidat, S.; Athamenh, R.; Tanash, M.; Bani Hani, D. Factor Analysis of Quality Management Systems Implementation in Healthcare: An Online Survey. Healthcare 2022, 10, 1828. https://doi.org/10.3390/healthcare10101828
Rawshdeh M, Keathley H, Obeidat S, Athamenh R, Tanash M, Bani Hani D. Factor Analysis of Quality Management Systems Implementation in Healthcare: An Online Survey. Healthcare. 2022; 10(10):1828. https://doi.org/10.3390/healthcare10101828
Chicago/Turabian StyleRawshdeh, Mustafa, Heather Keathley, Shahed Obeidat, Raed Athamenh, Moayad Tanash, and Dania Bani Hani. 2022. "Factor Analysis of Quality Management Systems Implementation in Healthcare: An Online Survey" Healthcare 10, no. 10: 1828. https://doi.org/10.3390/healthcare10101828
APA StyleRawshdeh, M., Keathley, H., Obeidat, S., Athamenh, R., Tanash, M., & Bani Hani, D. (2022). Factor Analysis of Quality Management Systems Implementation in Healthcare: An Online Survey. Healthcare, 10(10), 1828. https://doi.org/10.3390/healthcare10101828