
Three-Dimensional Printed Models for Preoperative Planning and Surgical Treatment of Chest Wall Disease: A Systematic Review

 , , and
, , and 
Abstract
:1. Introduction
2. Materials and Methods
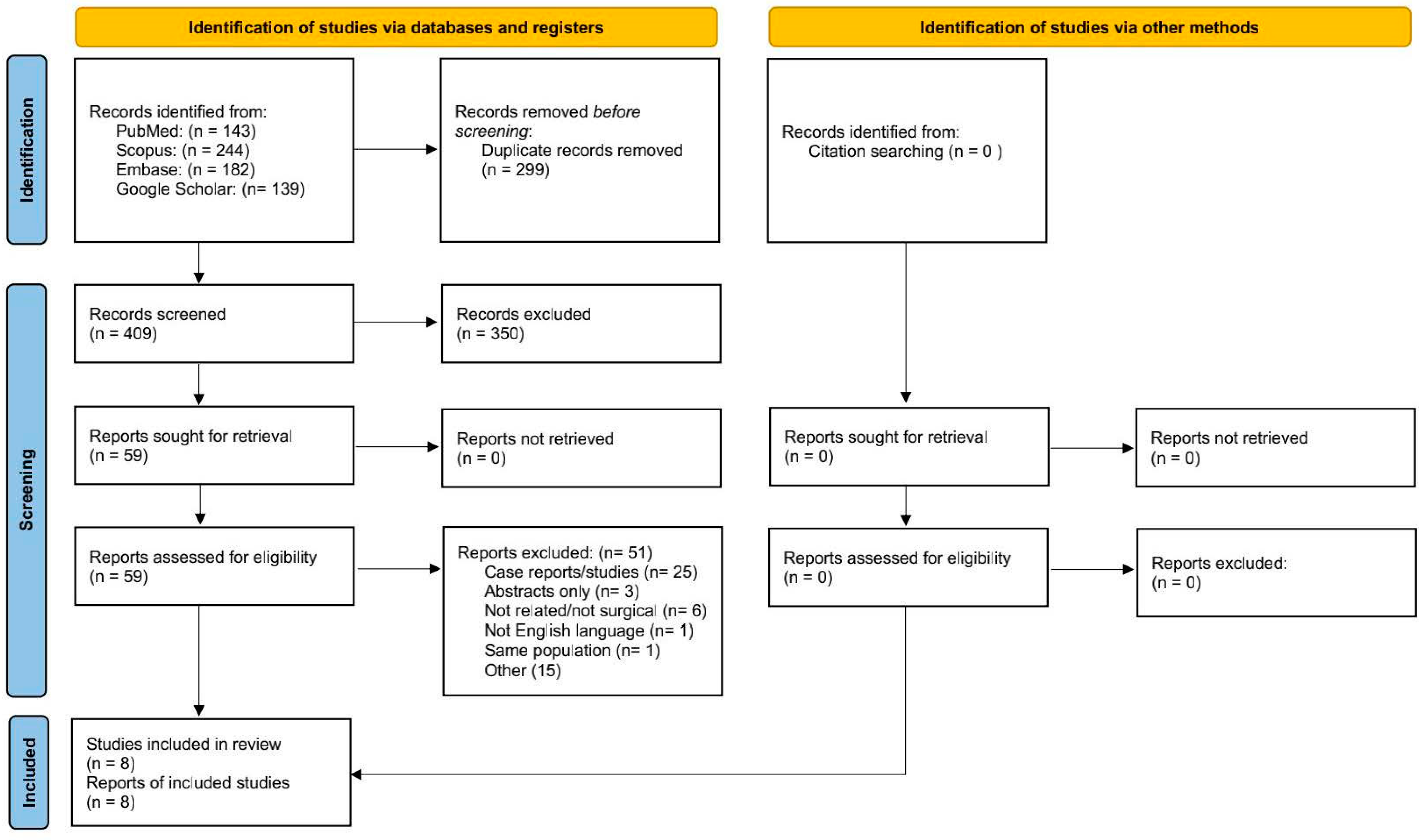
2.1. Search Strategy
2.2. Selection Process
2.3. Quality and Risk of Bias Assessment
3. Results
3.1. Study and Patient Characteristics
3.2. Rib Fracture Fixation
3.3. Pectus Excavatum Repair
3.4. Chest Wall Tumor Resection and Reconstruction
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Pascal, A.T.; Laurent, B. Prosthetic reconstruction of the chest wall. Thorac. Surg. Clin. 2010, 20, 551–558. [Google Scholar]
- Sanna, S.; Brandolini, J.; Pardolesi, A.; Argnani, D.; Mengozzi, M.; Dell’Amore, A.; Solli, P. Materials and techniques in chest wall reconstruction: A review. J. Vis. Surg. 2017, 3, 95. [Google Scholar] [CrossRef] [Green Version]
- Goldsmith, I.; Evans, P.L.; Goodrum, H. Chest wall reconstruction with an anatomically designed 3-D printed titanium ribs and hemi-sternum implant. 3D Print. Med. 2020, 6, 26. [Google Scholar] [CrossRef]
- Ganguli, A.; Pagan-Diaz, G.J.; Grant, L.; Cvetkovic, C.; Bramlet, M.; Vozenilek, J.; Kesavadas, T.; Bashir, R. 3D printing for preoperative planning and surgical training: A review. Biomed. Microdevices 2018, 20, 65. [Google Scholar] [CrossRef]
- Zhuang, Y.-D.; Zhou, M.-C.; Liu, S.-C.; Wu, J.-F.; Wang, R.; Chen, C.-M. Effectiveness of personalized 3D printed models for patient education in degenerative lumbar disease. Patient Educ. Couns. 2019, 102, 1875–1881. [Google Scholar] [CrossRef]
- Lu, T.; Shao, Z.; Liu, B.; Wu, T. Recent advance in patient-specific 3D printing templates in mandibular reconstruction. J. Mech. Behav. Biomed. Mater. 2020, 106, 103725. [Google Scholar] [CrossRef]
- Hay, J.A.; Smayra, T.; Moussa, R. Customized Polymethylmethacrylate Cranioplasty Implants Using 3-Dimensional Printed Polylactic Acid Molds: Technical Note with 2 Illustrative Cases. World Neurosurg. 2017, 105, 971–979. [Google Scholar]
- Diment, L.E.; Thompson, M.S.; Bergmann, J.H.M. Clinical efficacy and effectiveness of 3D printing: A systematic review. BMJ Open 2017, 7, e016891. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gu, B.K.; Choi, D.J.; Park, S.J.; Kim, Y.-J.; Kim, C.-H. 3D Bioprinting Technologies for Tissue Engineering Applications. Adv. Exp. Med. Biol. 2018, 1078, 15–28. [Google Scholar]
- Moher, D.; Shamseer, L.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Syst. Rev. 2015, 4, 1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Downs, S.H.; Black, N. The Feasibility of Creating a Checklist for the Assessment of the Methodological Quality Both of Randomised and Non-Randomised Studies of Health Care Interventions. J. Epidemiol. Community Health 1979, 52, 377–384. [Google Scholar] [CrossRef] [Green Version]
- Zhou, X.; Zhang, D.; Xie, Z.; Yang, Y.; Chen, M.; Liang, Z.; Zhang, G.; Li, S. Application of 3D printing and framework internal fixation technology for high complex rib fractures. J. Cardiothorac. Surg. 2021, 16, 5. [Google Scholar] [CrossRef]
- Chen, Y.-Y.; Lin, K.-H.; Huang, H.-K.; Chang, H.; Lee, S.-C.; Huang, T.-W. The beneficial application of preoperative 3D printing for surgical stabilization of rib fractures. PLoS ONE 2018, 13, e0204652. [Google Scholar] [CrossRef]
- Bellia-Munzon, G.; Martinez, J.; Toselli, L.; Peirano, M.N.; Sanjurjo, D.; Vallee, M.; Martinez-Ferro, M. From bench to bedside: 3D reconstruction and printing as a valuable tool for the chest wall surgeon. J. Pediatr. Surg. 2020, 55, 2703–2709. [Google Scholar] [CrossRef]
- Wang, L.; Guo, T.; Zhang, H.; Yang, S.; Liang, J.; Guo, Y.; Shao, Q.; Cao, T.; Li, X.; Huang, L. Three-dimensional printing flexible models: A novel technique for Nuss procedure planning of pectus excavatum repair. Ann. Transl. Med. 2020, 8, 110. [Google Scholar] [CrossRef]
- Huang, Y.-J.; Lin, K.-H.; Chen, Y.-Y.; Wu, T.-H.; Huang, H.-K.; Chang, H.; Lee, S.-C.; Chen, J.-E.; Huang, T.-W. Feasibility and Clinical Effectiveness of Three-Dimensional Printed Model-Assisted Nuss Procedure. Ann. Thorac. Surg. 2019, 107, 1089–1096. [Google Scholar] [CrossRef]
- Fillat-Gomà, F.; Coderch-Navarro, S.; Monill-Raya, N.; JE, B.A.; Martínez, S.; San Vicente Vela, B.; Jiménez-Arribas, P.; Güizzo, J.R. Initial experience with 3D printing in the use of customized Nuss bars in pectus excavatum surgery. Cir. Pediatrica 2021, 34, 186–190. [Google Scholar]
- Wu, Y.; Chen, N.; Xu, Z.; Zhang, X.; Liu, L.; Wu, C.; Zhang, S.; Song, Y.; Wu, T.; Liu, H.; et al. Application of 3D printing technology to thoracic wall tumor resection and thoracic wall reconstruction. J. Thorac. Dis. 2018, 10, 6880–6890. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.; Huang, L.; Li, X.; Zhong, D.; Li, D.; Cao, T.; Yang, S.; Yan, X.; Zhao, J.; He, J.; et al. Three-Dimensional Printing PEEK Implant: A Novel Choice for the Reconstruction of Chest Wall Defect. Ann. Thorac. Surg. 2019, 107, 921–928. [Google Scholar] [CrossRef] [PubMed]
- Torre, M.; Guerriero, V.; Wong, M.C.Y.; Palo, F.; Lena, F.; Mattioli, G. Complications and trends in minimally invasive repair of pectus excavatum: A large volume, single institution experience. J. Pediatric Surg. 2021, 56, 1846–1851. [Google Scholar] [CrossRef] [PubMed]
- Choi, J.; Kaghazchi, A.; Sun, B.; Woodward, A.; Forrester, J.D. Systematic Review and Meta-Analysis of Hardware Failure in Surgical Stabilization of Rib Fractures: Who, What, When, Where, and Why? J. Surg. Res. 2021, 268, 190–198. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.; Cao, T.; Li, X.; Huang, L. Three-dimensional printing titanium ribs for complex reconstruction after extensive posterolateral chest wall resection in lung cancer. J. Thorac. Cardiovasc. Surg. 2016, 152, e5–e7. [Google Scholar] [CrossRef] [Green Version]
- Aranda, J.L.; Jiménez, M.F.; Rodríguez, M.; Varela, G. Tridimensional titanium-printed custom-made prosthesis for sternocostal reconstruction. Eur. J. Cardiothorac. Surg. 2015, 48, e92–e94. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ballard, D.H.; Mills, P.; Duszak, R. Medical 3D Printing Cost-Savings in Orthopedic and Maxillofacial Surgery: Cost Analysis of Operating Room Time Saved with 3D Printed Anatomic Models and Surgical Guides. Acad Radiol. 2020, 27, 1103–1113. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Database | Search Results (8 November 2021) | Keywords |
|---|---|---|
| Pubmed | 143 | (3D printing OR rapid prototyping OR three-dimensional printing OR bioprinting) AND ( chest wall OR rib OR sternum OR ribcage OR pectus excavatum) |
| Scopus | 244 | (“3D printing” OR “rapid prototyping” OR “three-dimensional printing” OR “bioprinting”) AND (“chest wall” OR “rib” OR “sternum” OR “ribcage” OR “pectus excavatum”) |
| Embase | 182 | (3D printing OR rapid prototyping OR three-dimensional printing OR bioprinting) AND ( chest wall OR rib OR sternum OR ribcage OR pectus excavatum) |
| Google Scholar | 139 | (3D printing or three-dimensional printing) AND (chest wall or rib or sternum or pectus excavatum) |
| Study | Reporting (Max 11) | External Validity (Max 3) | Internal Validity/Bias (Max 7) | Internal Validity/Confounding (Max 6) | Power (Max 1) | Total (Max 28) |
|---|---|---|---|---|---|---|
| Zhou et al. | 10 | 3 | 5 | 3 | 0 | 21 |
| Bellia Munzon et al. | 10 | 3 | 5 | 3 | 1 | 22 |
| Wang et al. (2020) | 6 | 1 | 5 | 3 | 0 | 15 |
| Wu et al. | 11 | 3 | 5 | 3 | 0 | 22 |
| Wang et al. (2019) | 9 | 3 | 5 | 3 | 0 | 20 |
| Huang et al. | 11 | 3 | 5 | 3 | 1 | 23 |
| Chen et al. | 11 | 3 | 5 | 3 | 1 | 23 |
| Gaspar Pérez et al. | 10 | 3 | 5 | 3 | 0 | 21 |
| Authors, Year of Publication, Country | Study Design | N° of Patients | Application | Disease of Interest | Structure Printed | CT-Images Processing Software | 3D Printer | Materials | Limitations |
|---|---|---|---|---|---|---|---|---|---|
| Zhou et al. (7), 2021, China | Prospective | 16 | Surgical planning and prosthetic modeling | Rib fractures | Ribcage model | MDT2AB-010A, Meditool Medical Technology (Shanghai) | pangu4.1, Meditool Medical Technology | Photosensitive resin | No conventionally treated control group Small sample size |
| Bellia-Munzon et al. (6) 2020, Argentina | Prospective | 130 | Surgical planning and prosthetic modeling | Pectus excavatum | Customized implant bars template | Erkom 3D Chest Wall Pro 1.0, Pampamed (Buenos Aires) | ERKOM 3D | Polyvinyl acetate | Non controlled study nature |
| Wang et al. (9) 2020, China | Prospective | 6 | Surgical planning and prosthetic modeling | Pectus excavatum | Ribcage model | 3D-DOCTOR, Able Software Corp (Lexington) | Not specified | Polylactic acid | No conventionally treated control group Small sample size |
| Wu et al. (11), 2018, China | Retrospective | 6 | Surgical planning and prosthetic modeling | Chest wall tumor | Chest wall tumor model | Amira Thermo Fisher Scientific (Berlin) | Formlabs Form2 /MakerBot ReplicatorTM 2X | Liquid photosensitive resin | Retrospective nature Small sample size |
| Wang et al. (11), 2019,China | Prospective | 18 | Prosthetic replacement | Chest wall tumor | Ribs and sternum prostheses | Mimics 17.0, Materialise MV (Leuven) / Geomagic Studio version 2012 3D Systems (Morrisville) | Jugao-AM-Doctor, Shaanxi Jugao-AM Technology | Polyetheretherketone | No conventionally treated control group Small sample size |
| Huang et al. (8), 2019, China | Retrospective | 15 | Surgical planning and prosthetic modeling | Pectus excavatum | Customized implant bars template | Meshmixer, Autodesk (San Rafael) | UP BOX, Beijing Tiertime Technology | Polylactic acid | Retrospective nature Small 3D printing group size |
| Chen et al. (5), 2018, China | Retrospective | 16 | Surgical planning and prosthetic modeling | Rib fractures | Ribcage model | Not specified | UP-BOX 3D printer, Denford | Acrylonitrile butadiene styrene | Retrospective nature Small sample size |
| Gaspar Pérez et al. (12), 2021, Spain | Prospective | 6 | Surgical planning and prosthetic modeling | Pectus excavatum | Ribcage model, customized implant bars template | Mimics 21.0/3-matic 13.0, Materialise MV (Leuven) | Ultimaker S5 3D, Ultimaker B.V. | Polylactic acid | No conventionally treated control group Small sample size |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Leonardi, B.; Carlucci, A.; Noro, A.; Bove, M.; Natale, G.; Opromolla, G.; Mirra, R.; Pica, D.; Capasso, F.; Di Filippo, V.; et al. Three-Dimensional Printed Models for Preoperative Planning and Surgical Treatment of Chest Wall Disease: A Systematic Review. Technologies 2021, 9, 97. https://doi.org/10.3390/technologies9040097
Leonardi B, Carlucci A, Noro A, Bove M, Natale G, Opromolla G, Mirra R, Pica D, Capasso F, Di Filippo V, et al. Three-Dimensional Printed Models for Preoperative Planning and Surgical Treatment of Chest Wall Disease: A Systematic Review. Technologies. 2021; 9(4):97. https://doi.org/10.3390/technologies9040097
Chicago/Turabian StyleLeonardi, Beatrice, Annalisa Carlucci, Antonio Noro, Mary Bove, Giovanni Natale, Giorgia Opromolla, Rosa Mirra, Davide Pica, Francesca Capasso, Vincenzo Di Filippo, and et al. 2021. "Three-Dimensional Printed Models for Preoperative Planning and Surgical Treatment of Chest Wall Disease: A Systematic Review" Technologies 9, no. 4: 97. https://doi.org/10.3390/technologies9040097
APA StyleLeonardi, B., Carlucci, A., Noro, A., Bove, M., Natale, G., Opromolla, G., Mirra, R., Pica, D., Capasso, F., Di Filippo, V., Messina, G., Ferrigno, F., Izzo, A. C., Vicidomini, G., Santini, M., & Fiorelli, A. (2021). Three-Dimensional Printed Models for Preoperative Planning and Surgical Treatment of Chest Wall Disease: A Systematic Review. Technologies, 9(4), 97. https://doi.org/10.3390/technologies9040097