
The Provision of Powered Mobility Devices in Italy: Linking Process with Outcomes

 ,
,
Abstract
:1. Introduction
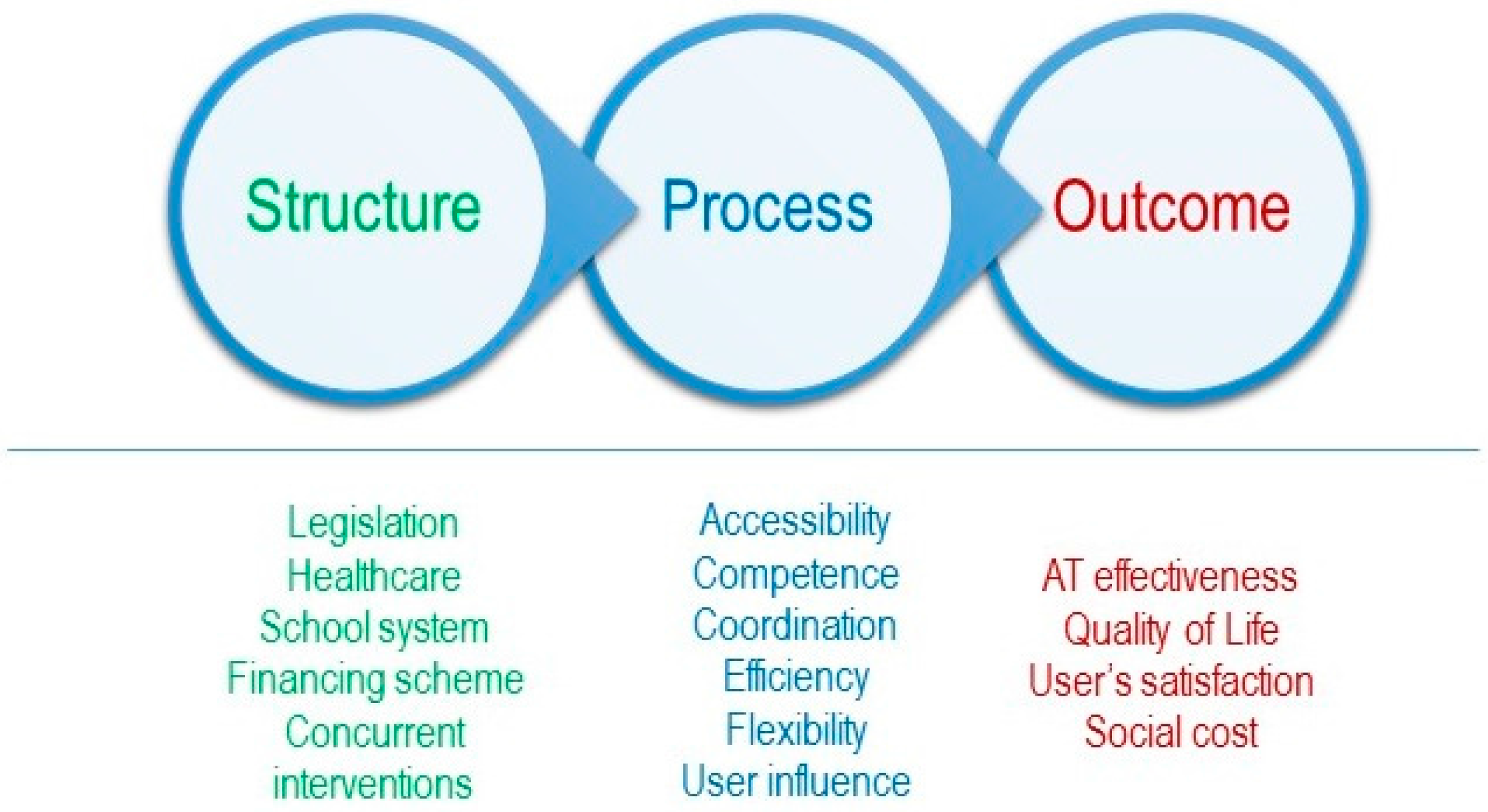
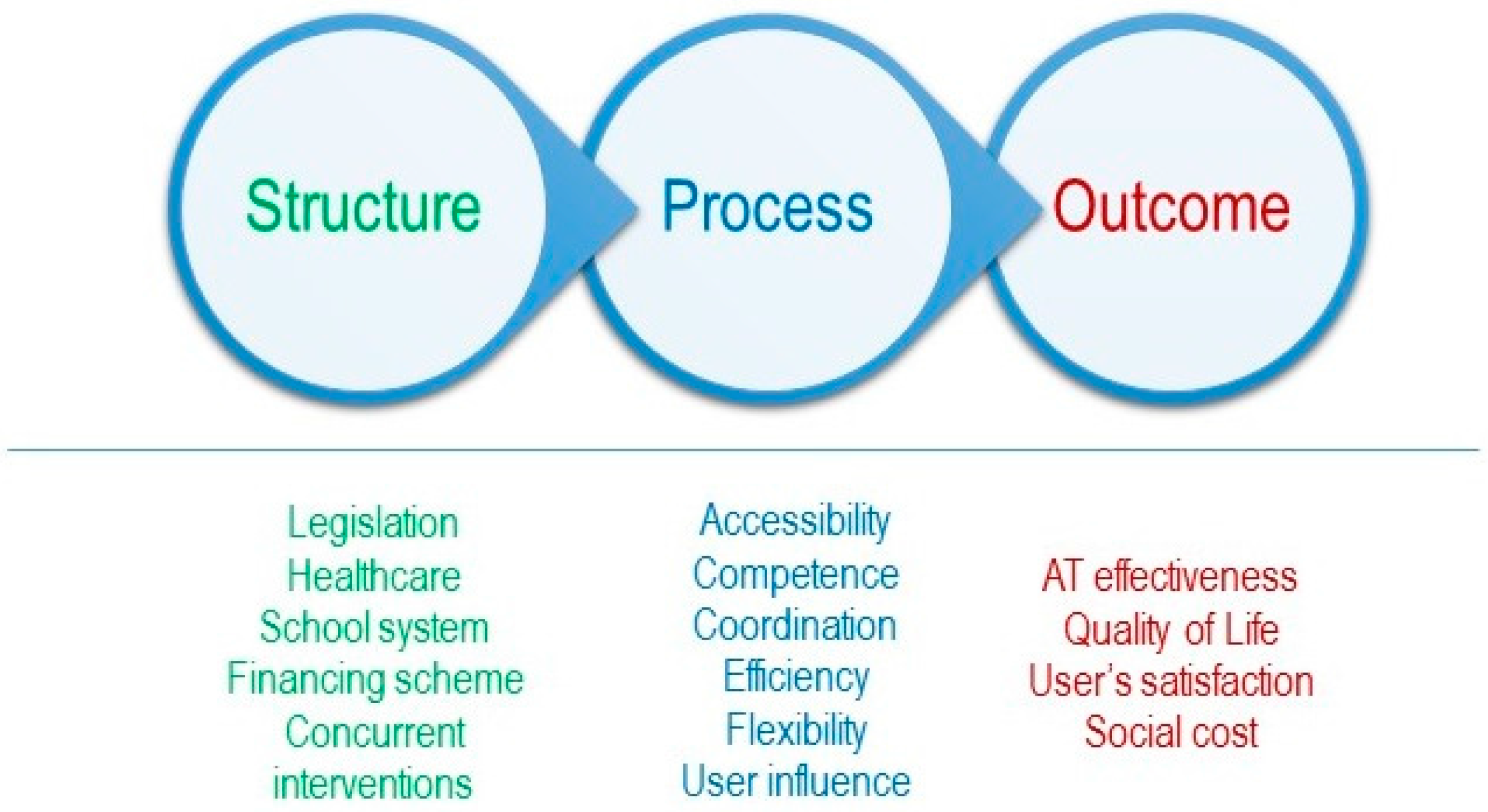
2. Materials and Methods
2.1. Context of the Studies
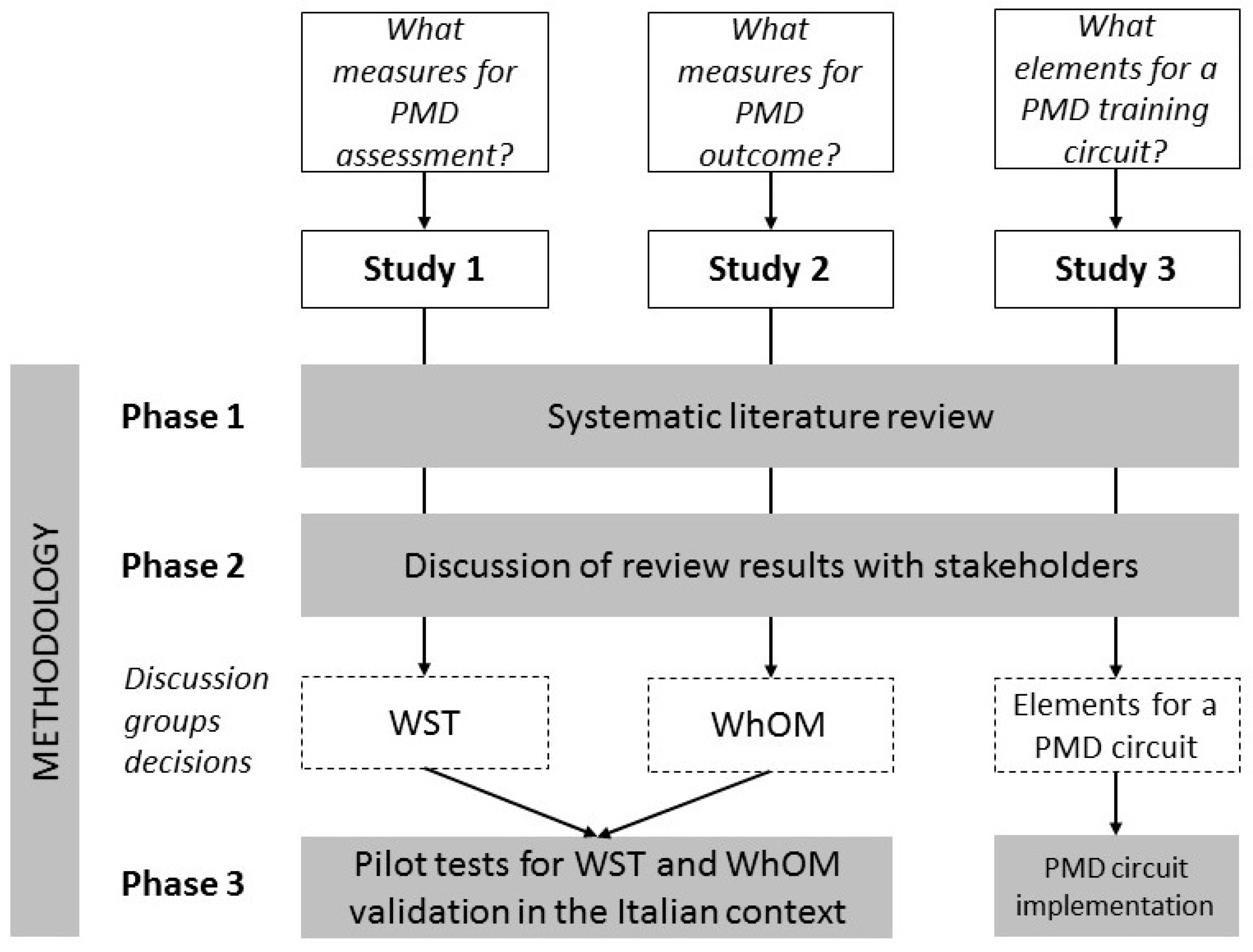
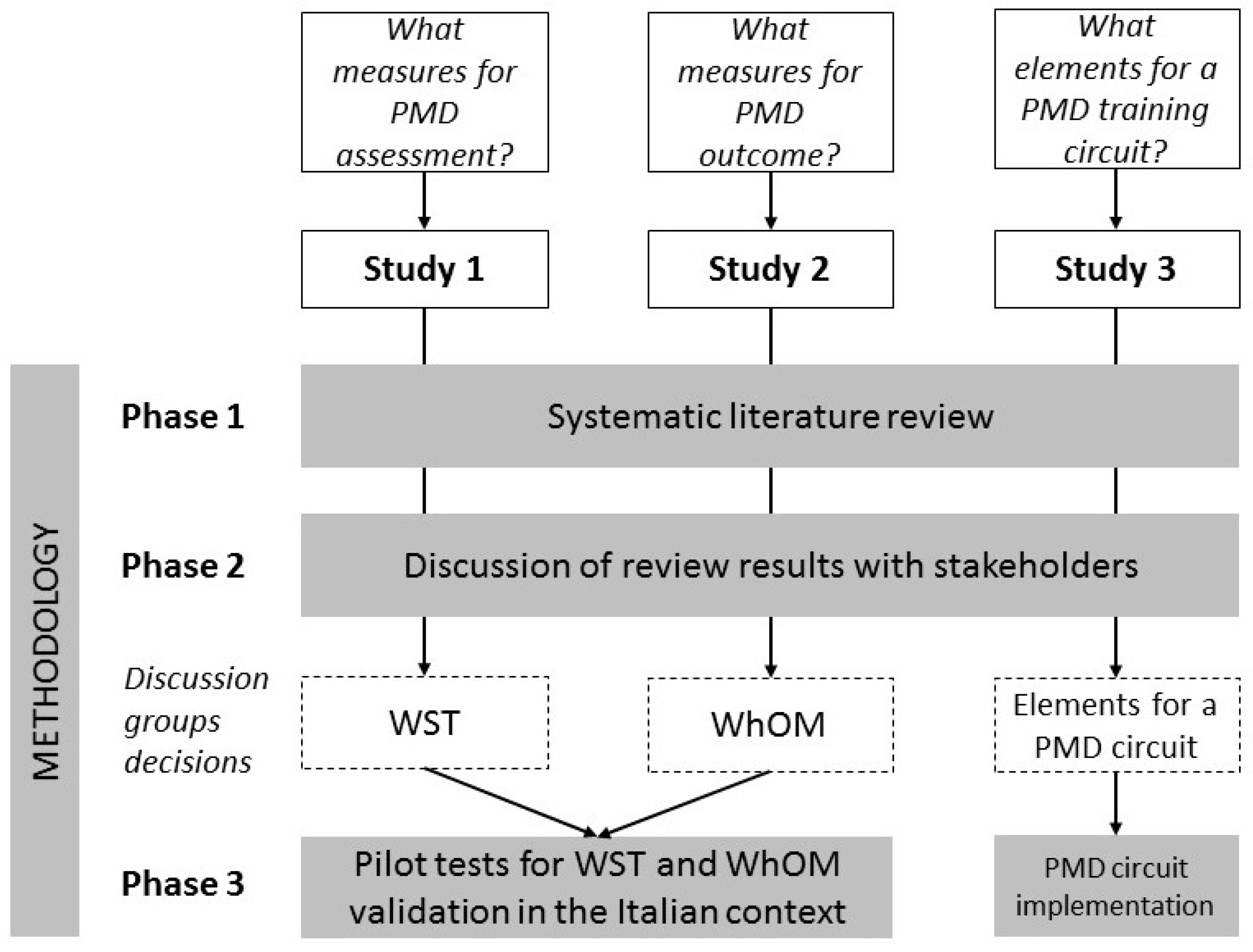
2.2. Design of the Studies
2.2.1. Phase One: Systematic Literature Reviews
2.2.2. Phase Two: Discussion Groups with Stakeholders
2.2.3. Phase Three: Pilot Testing of the Measures Selected and Test Usability
3. Results
3.1. Participants
3.2. Study 1
3.3. Study 2
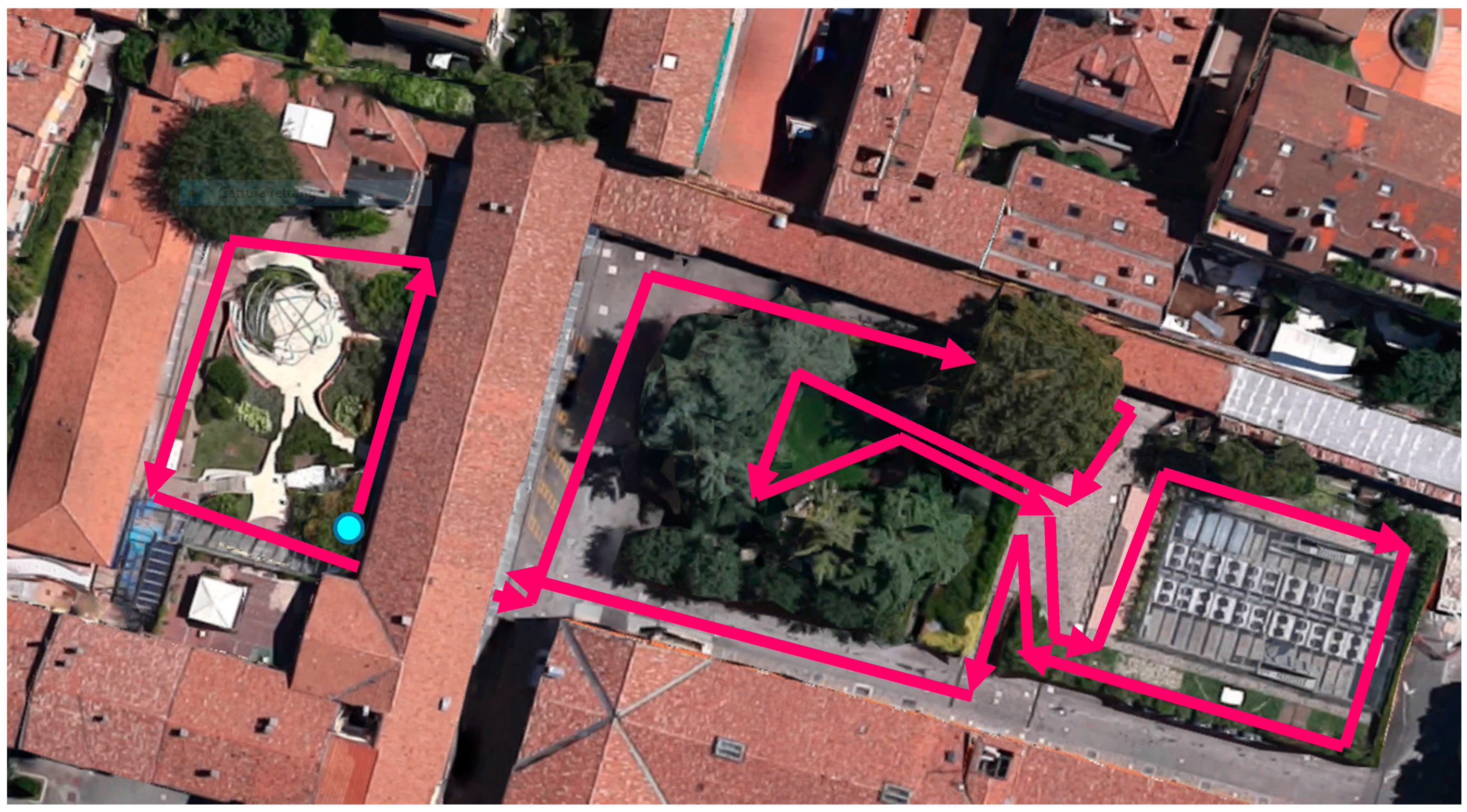
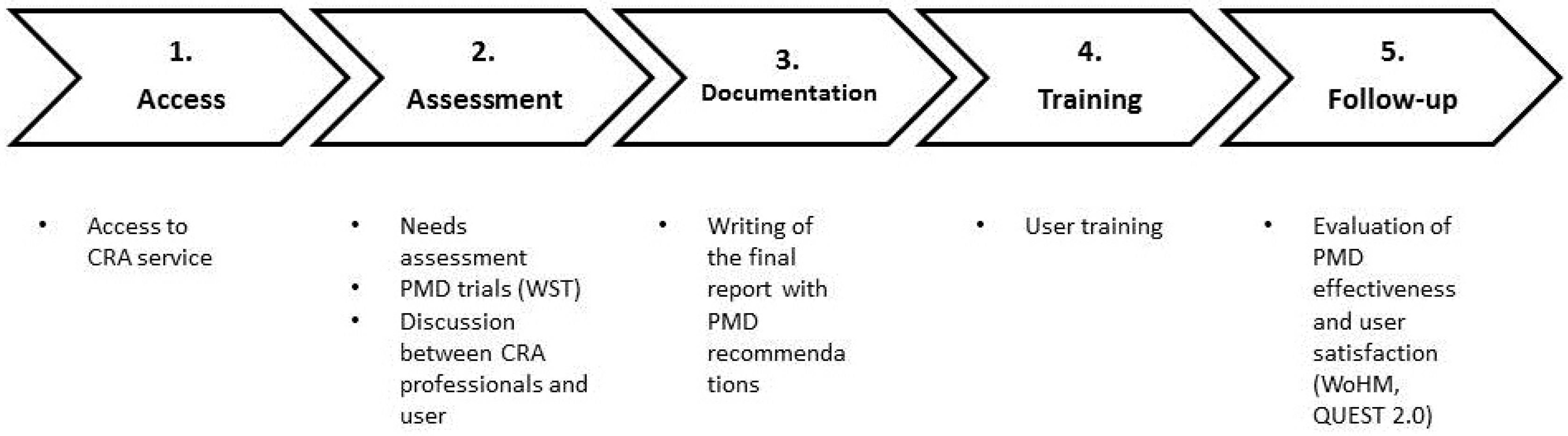
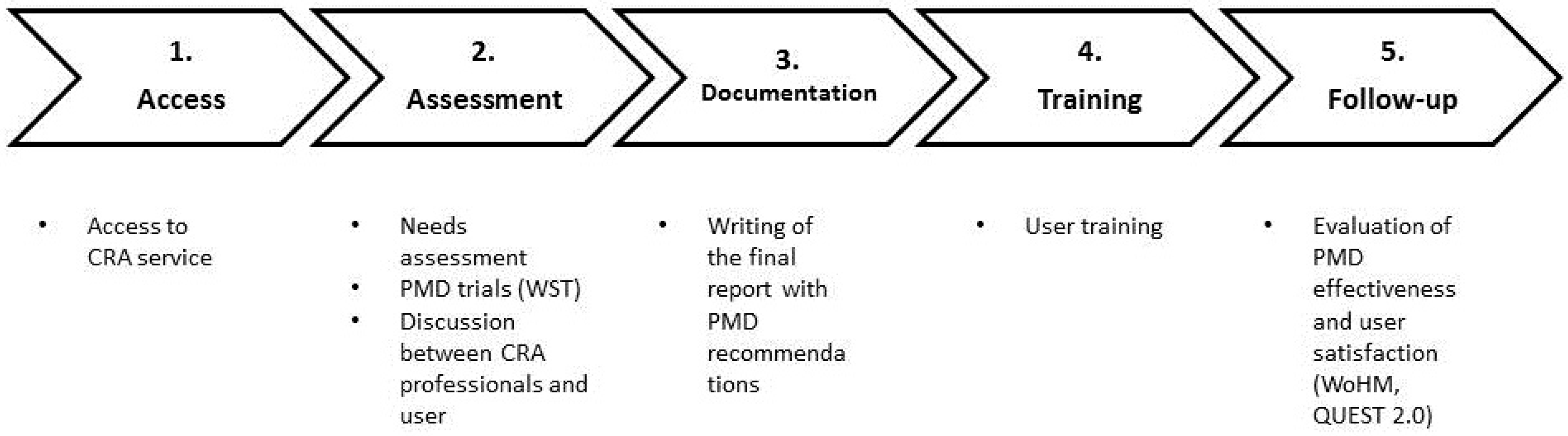
3.4. Study 3
4. Discussion
Acknowledgments
Author Contributions
Conflicts of Interest
Appendix A. Assistive Technology Service Provision in Italy
Appendix B

| Original Version | Italian Version | n | % Success | Kappa | ||
|---|---|---|---|---|---|---|
| Rater 1 | Rater 2 | Rater 1 | Rater 2 | |||
| 1. Moves controller/tiller away and back | 1. Sposti il comando di guida avanti e indietro e infine lo rilasci | 34 | 35 | 100 | 100 | 0.69 |
| 2. Turns controller on and off | 2. Accenda e spenga la carrozzina | 34 | 34 | 94 | 94 | 0.98 |
| 3. Selects drive modes and speeds | 3. Selezioni le diverse modalità (profili) di guida e le varie velocità possibili | 31 | 32 | 90 | 94 | 0.35 |
| 4. Operates body positioning options | 4. Utilizzi i comandi per variare la postura | 34 | 33 | 82 | 85 | 0.80 |
| 5. Disengages and engages motors | 5. Disinserisca e inserisca i motori | 10 | 9 | 20 | 0 | 0.43 |
| - | 6. Dia le istruzioni per disinserire e inserire i motori | 14 | 14 | 64 | 71 | 0.58 |
| 6. Operates battery charger | 7. Colleghi la carrozzina al caricabatterie | 10 | 10 | 20 | 30 | 0.28 |
| - | 8. Dia le istruzioni per collegare la carrozzina al caricabatterie | 13 | 14 | 69 | 86 | 0.45 |
| 7. Rolls forwards (10 m) | 9. Si sposti avanti per 10 m | 35 | 35 | 100 | 100 | 0.65 |
| 8. Rolls backwards (2 m) | 10. Si sposti indietro per 2 m | 31 | 30 | 97 | 100 | 0.45 |
| 9. Turns while moving forwards (90°) | 11. Esegua una svolta di 90° mentre sta andando avanti | 35 | 35 | 100 | 100 | 1.00 |
| 10. Turns while moving backwards (90°) | 12. Esegua una svolta di 90° mentre sta andando indietro | 31 | 30 | 100 | 100 | 0.55 |
| 11. Turns in place (180°) | 13. Giri di 180° sul posto | 35 | 32 | 100 | 100 | 0.30 |
| 12. Maneuvers sideways (0.5 m) | 14. Si sposti lateralmente di 50 cm (con manovre combinate) | 23 | 24 | 91 | 92 | 0.71 |
| 13. Gets through hinged door | 15. Varchi una porta a battente (in entrambe le direzioni) | 24 | 25 | 96 | 100 | 0.67 |
| 14. Reaches high object (1.5 m) | 16. Raggiunga un oggetto a 1.5 m di altezza | 22 | 22 | 64 | 64 | 0.78 |
| 15. Picks object up from floor | 17. Raggiunga un oggetto da terra (es. quaderno ad anelle) | 23 | 22 | 56 | 54 | 0.83 |
| 16. Relieves weight from buttocks (3 s) | 18. Sollevi il peso dal sedile per 3 secondi (anche un lato per volta) | 23 | 21 | 52 | 48 | 0.81 |
| 17. Transfer to and from bench | 19. Si trasferisca su una panca e ritorni sulla carrozzina | 25 | 27 | 48 | 55 | 0.72 |
| 18. Rolls 100 m | 20. Si sposti in avanti per 100 m | 25 | 25 | 96 | 96 | 1.00 |
| 19. Avoids moving obstacles | 21. Eviti degli ostacoli con movimenti a zig zag | 24 | 24 | 96 | 96 | 0.88 |
| 20. Ascends 5° incline | 22. Salga su una superficie con una pendenza di 5° (circa 8%) | 25 | 25 | 100 | 100 | 0.71 |
| 21. Descends 5° incline | 23. Scenda da una superficie con una pendenza di 5° (circa 8%) | 25 | 25 | 100 | 100 | 0.93 |
| 22. Ascends 10° incline | 24. Salga su una superficie con una pendenza di 10° | 16 | 16 | 75 | 81 | 0.65 |
| 23. Descends 10° incline | 25. Scenda da una superficie con una pendenza di 10° | 22 | 22 | 86 | 86 | 0.75 |
| 24. Rolls across side-slope (5°) | 26. Avanzi su una superficie inclinata lateralmente di 5° | 22 | 22 | 95 | 91 | 0.76 |
| 25. Rolls on soft surface (2 m) | 27. Avanzi 2 m su una superficie cedevole (es. prato) | 21 | 20 | 90 | 85 | 0.66 |
| 26. Gets over gap (15 cm) | 28. Superi un avvallamento di 15 cm | 17 | 17 | 82 | 82 | 0.62 |
| 27. Gets over threshold (2 cm) | 29. Superi una soglia di 2 cm | 17 | 17 | 88 | 94 | 0.28 |
| 28. Ascends low curb (5 cm) | 30. Salga uno scalino di 5 cm | 17 | 17 | 76 | 71 | 0.85 |
| 29. Descends low curb (5 cm) | 31. Scenda da uno scalino di 5 cm | 17 | 17 | 82 | 76 | 0.74 |
| 30. Gets from ground into wheelchair | 32. Partendo da terra salga sulla carrozzina | 16 | 16 | 6 | 0 | 0.30 |
References
- Guidelines on the Provision of Manual Wheelchairs in Less-Resourced Settings. Available online: http://www.who.int/disabilities/publications/technology/wheelchairguidelines/en/ (accessed on 10 April 2016).
- Livingstone, R.; Field, D. Systematic review of power mobility outcomes for infants, children and adolescents with mobility limitations. Clin. Rehabil. 2014, 28. [Google Scholar] [CrossRef] [PubMed]
- Sund, T.; Iwarsson, S.; Anttila, H.; Brandt, Å. Effectiveness of powered mobility devices in enabling community mobility-related participation: A prospective study among people with mobility restrictions. PM R 2015, 7, 859–870. [Google Scholar] [CrossRef] [PubMed]
- Fomiatti, R.; Richmond, J.; Moir, L.; Millsteed, J. A systematic review of the impact of powered mobility devices on older adults’ activity engagement. Phys. Occup. Ther. Geriatr. 2013, 31, 297–309. [Google Scholar] [CrossRef]
- Greer, N.; Brasure, M.; Wilt, T.J. Wheeled mobility (wheelchair) service delivery: Scope of the evidence. Ann. Intern. Med. 2012, 156, 141–146. [Google Scholar] [CrossRef] [PubMed]
- Hoenig, H.; Landerman, L.R.; Shipp, K.M.; Pieper, C.; Pieper, C.; Richardson, M.; Pahel, N.; George, L. A clinical trial of a rehabilitation expert clinician versus usual care for providing manual wheelchairs. J. Am. Geriatr. Soc. 2005, 53, 1712–1720. [Google Scholar] [CrossRef] [PubMed]
- Archambault, P.S.; Tremblay, S.; Cachecho, S.; Routhier, F.; Boissy, P. Driving performance in a power wheelchair simulator. Disabil. Rehabil. Assist. Technol. 2012, 7, 226–233. [Google Scholar] [CrossRef] [PubMed]
- Letts, L.; Dawson, D.; Bretholz, I.; Kaiserman-Goldenstein, E.; Gleason, J.; McLellan, E.; Roth, C. Reliability and validity of the power-mobility community driving assessment. Assist. Technol. 2007, 19, 154–163. [Google Scholar] [CrossRef] [PubMed]
- Furumasu, J.; Guerette, P.; Tefft, D. The development of a powered wheelchair mobility program for young children. Technol. Disabil. 1996, 5, 41–48. [Google Scholar] [CrossRef]
- Dawson, D.; Chan, R.; Kaiserman, E. Development of the power mobility indoor driving assessment for residents of long-term care facilities: A preliminary report. Can. J. Occup. Ther. 1994, 61, 269–276. [Google Scholar] [CrossRef]
- Mortenson, W.B.; Miller, W.C.; Miller-Pogar, J. Measuring wheelchair intervention outcomes: Development of the wheelchair outcome measure. Disabil. Rehabil. Assist. Technol. 2007, 2, 275–285. [Google Scholar] [CrossRef] [PubMed]
- Brandt, A.; Löfqvist, C.; Jónsdottir, I.; Sund, T.; Salminen, A.L.; Werngren-Elgström, M.; Iwarsson, S. Towards an instrument targeting mobility-related participation: Nordic cross-national reliability. J. Rehabil. Med. 2008, 40, 766–772. [Google Scholar] [CrossRef] [PubMed]
- Harris, F.; Sprigle, S.; Sonenblum, S.E.; Maurer, C.L. The Participation and activity measurement system: An example application among people who use wheeled mobility devices. Disabil. Rehabil. Assist. Technol. 2010, 5, 48–57. [Google Scholar] [CrossRef] [PubMed]
- Steel, E.J.; de Witte, L.P. Advances in European Assistive Technology service delivery and recommendations for further improvement. Technol. Disabil. 2011, 23, 131–138. [Google Scholar]
- Spagnolin, G. Mobilità e postura in carrozzina nella disabilità dell’adulto (Mobility and posture in the adult with disability). In Proceedings of the L’ausilio Nel Progetto Riabilitativo Della Persona Disabile, Abano Terme, Italy, 5–7 November 2008; pp. 30–31.
- HEART Final Report on Service Delivery. Available online: http://portale.siva.it/files/doc/library/a416_1_ATServiceDelivery_HEART_ReportC51.pdf (accessed on 20 November 2014).
- Lenker, J.A.; Fuhrer, M.J.; Jutai, J.W.; Demers, L.; Scherer, M.J.; DeRuyter, F. Treatment theory, intervention specification, and treatment fidelity in assistive technology outcomes research. Assist. Technol. 2010, 22, 129–138. [Google Scholar] [CrossRef] [PubMed]
- Lenker, J.A.; Shoemaker, L.L.; Fuhrer, M.J.; Jutai, J.W.; Demers, L.; Tan, C.H.; DeRuyter, F. Classification of assistive technology services: Implications for outcomes research. Technol. Disabil. 2012, 24, 59–70. [Google Scholar]
- Steel, E.J.; Layton, N.A.; Foster, M.M.; Bennett, S. Shopping without a prescription: Challenges of user-centred assistive technology provision in Australia. Disabil. Rehabil. Assist. Technol. 2014, 11, 235–240. [Google Scholar] [CrossRef] [PubMed]
- Desideri, L. Assistive Technology Service Delivery for Children with Multiple Disabilities: A Family-Centerd Approach to Assure Quality. Ph.D. Thesis, University of Maastricht, Maastricht, The Netherlands, October 2015. [Google Scholar]
- Andrich, R.; Mathiassen, N.E.; Hoogerwerf, E.J.; Gelderblom, G.J. Service delivery systems for assistive technology in Europe: An AAATE/EASTIN position paper. Technol. Disabil. 2013, 25, 127–146. [Google Scholar]
- Donabedian, A. An. Introduction to Quality Assurance in Health Care; Oxford University Press: New York, NY, USA, 2003. [Google Scholar]
- Campbell, S.; Roland, M.; Buetow, S. Defining quality of care. Soc. Sci. Med. 2000, 51, 1611–1625. [Google Scholar] [CrossRef]
- Maximo, T.; Clift, L. Assessing service delivery systems for assistive technology in Brazil using HEART study quality indicators. Technol. Disabil. 2015, 27, 161–170. [Google Scholar] [CrossRef]
- Desideri, L.; Mingardi, A.; Stefanelli, B.; Tanzini, D.; Bitelli, C.; Roentgen, U.; de Witte, L. Assessing children with multiple disabilities for assistive technology: A framework for quality assurance. Technol. Disabil. 2013, 25, 159–166. [Google Scholar]
- Muscari, G. Ausili Elettronici Per la Mobilità e Valutazione Delle Abilità di Guida: Quali Strumenti? Revisione Sistematica Della Letteratura e Localizzazione di Una Scala di Osservazione in Contesto Clinico (Power Mobility Devices and Driving Skills Assessment: What Measures? A Systematic Review of the Literature). Master’s Thesis, University of Ferrara, Ferrara, Italy, March 2013. [Google Scholar]
- Desideri, L.; Roentgen, U.; Hoogerwerf, E.J.; de Witte, L. Recommending assistive technology (AT) for children with multiple disabilities: A systematic review and qualitative synthesis of models and instruments for AT professionals. Technol. Disabil. 2013, 25, 3–13. [Google Scholar]
- Beaton, D.E.; Bombardier, C.; Guillemin, F.; Ferraz, M.B. Guidelines for the process of cross-cultural adaptation of self-report measures. Spine 2000, 25, 3186–3191. [Google Scholar] [CrossRef] [PubMed]
- Demers, L.; Weiss-Lambrou, R.; Ska, B. The Quebec User Evaluation of Satisfaction with Assistive Technology (QUEST 2.0): An overview and recent progress. Technol. Disabil. 2002, 14, 101–105. [Google Scholar]
- Kirby, R.L.; Swuste, J.; Dupuis, D.J.; MacLeod, D.A.; Monroe, R. The Wheelchair Skills Test: A pilot study of a new outcome measure. Arch. Phys. Med. Rehabil. 2002, 83, 10–18. [Google Scholar] [CrossRef] [PubMed]
- Orizio, G. Ausili Elettronici per la Mobilità e Impatto Sulla Partecipazione: Quali Strumenti? Traduzione e Adattamento di Una Scala di Valutazione in un Contesto Clinico (Power Mobility Devices and Their Impact on Participation: What Measures? A Systematic Review of the Literature and Adaptation of a Tool in a Clinical Context). Master’s Thesis, University of Bologna, Bologna, Italy, July 2013. [Google Scholar]
- WhOM-I Termini di Utilizzo. Available online: http://millerresearch.osot.ubc.ca/whom-i-termini-di-utilizzo/?login (accessed on 8 September 2016).
- Desideri, L.; Bizzarri, M.; Bitelli, C.; Roentgen, U.; Gelderblom, G.J.; de Witte, L. Implementing a routine outcome assessment procedure to evaluate the quality of assistive technology service delivery for children with physical or multiple disabilities: Perceived effectiveness, social cost, and user satisfaction. Assist. Technol. 2016, 28, 30–40. [Google Scholar] [CrossRef] [PubMed]
- Desideri, L.; Stefanelli, B.; Bitelli, C.; Roentgen, U.; Gelderblom, G.J.; de Witte, L. Satisfaction of users with assistive technology service delivery: An exploratory analysis of experiences of parents of children with physical and multiple disabilities. Dev. Neurorehabil. 2016, 19, 255–266. [Google Scholar] [CrossRef] [PubMed]
- Lahm, E.A.; Sizemore, L. Factors that influence assistive technology decision making. J. Spec. Educ. Technol. 2002, 17, 15–26. [Google Scholar]
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| User | Study | Gender | Age | Experienced with PMD | Health Condition | Track | Type of Controller |
|---|---|---|---|---|---|---|---|
| 1 | 1 | M | 65 | Experienced user | Amputee | R | Joystick |
| 2 | 1 | M | 68 | Experienced user | Polio | M | Joystick |
| 3 | 1 | M | 33 | Experienced user | SCI | R | Self-propulsion with manual wheelchair |
| 4 | 1 | F | 16 | Experienced user | CP | R | Joystick |
| 5 | 1 | M | 27 | Experienced user | MD | F | Mini-joystick |
| 6 | 1 | M | 68 | Experienced user | Polio | M | Joystick |
| 7 | 1 | M | 12 | Experienced user | CP | M | Joystick |
| 8 | 1 | M | 50 | First PMD | SCI | F | Chin control |
| 9 | 1 | F | 54 | First PMD | Myopathy | M | Joystick |
| 10 | 1 | M | 19 | Experienced user | MD | R | Joystick |
| 11 | 1 | M | 22 | Experienced user | MD | R | Mini-joystick |
| 12 | 1 | M | 18 | Experienced user | CP | R | Joystick |
| 13 | 1 | F | 28 | First PMD | TBI | M | Joystick |
| 14 | 1 | F | 43 | Experienced user | CP | R | Joystick |
| 15 | 1 | M | 24 | Experienced user | MD | R | Joystick |
| 16 | 1 | M | 52 | First PMD | ALS | M | Foot control |
| 17 | 1 | F | 33 | First PMD | MS | M | Mini-joystick |
| 18 | 1 | M | 25 | Experienced user | MD | M | Mini-joystick |
| 19 | 1 | M | 58 | First PMD | MND | R | Joystick |
| 20 | 1 | M | 51 | First PMD | ALS | R | Joystick |
| 21 | 1 | F | 69 | First PMD | Stroke | R | Joystick |
| 22 | 1 | M | 52 | Experienced user | CP | M | Joystick |
| 23 | 1 | M | 24 | Experienced user | CP | R | Joystick |
| 24 | 1 | M | 31 | Experienced user | SCI | R | Joystick (via Smartphone) |
| 25 | 1 | M | 51 | Experienced user | SCI | M | Joystick |
| 26 | 1 | M | 58 | First PMD | ALS | M | Head control |
| 27 | 1 | M | 23 | First PMD | MD | R | Joystick |
| 28 | 1 | M | 53 | First PMD | MD | M | Mini-joystick |
| 29 | 1 | M | 52 | First PMD | SCI | M | Joystick |
| 30 | 1 | F | 84 | First PMD | ALS | M | Joystick |
| 31 | 1 | M | 54 | First PMD | RA | R | Joystick |
| 32 | 1 | M | 14 | First PMD | CP | M | Joystick |
| 33 | 1 | M | 54 | First PMD | ALS | M | Joystick |
| 34 | 1 | F | 33 | First PMD | MS | M | Mini-joystick |
| 35 | 1 | M | 51 | First PMD | ALS | M | Joystick |
| 36 | 2 | M | 33 | First PMD | CP | R | Handlebars |
| 37 | 2 | F | 44 | First PMD | CP | R | Joystick |
| 38 | 2 | F | 84 | First PMD | CP | M | Joystick |
| 39 | 2 | M | 71 | First PMD | ALS | M | Joystick |
| 40 | 2 | M | 26 | Experienced user | MD | F | Mini-joystick |
| 41 | 2 | M | 43 | Experienced user | ALS | M | Head control |
| 42 | 2 | M | 14 | First PMD | CP | M | Joystick |
| 43 | 2 | M | 68 | Experienced user | SCI | F | Joystick |
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Desideri, L.; Trioschi, D.; Agusto, R.; Bizzarri, M.; Spagnolin, G.; Cantelli, S.; Paolini, C.; Malavasi, M.; Bitelli, C. The Provision of Powered Mobility Devices in Italy: Linking Process with Outcomes. Technologies 2016, 4, 31. https://doi.org/10.3390/technologies4030031
Desideri L, Trioschi D, Agusto R, Bizzarri M, Spagnolin G, Cantelli S, Paolini C, Malavasi M, Bitelli C. The Provision of Powered Mobility Devices in Italy: Linking Process with Outcomes. Technologies. 2016; 4(3):31. https://doi.org/10.3390/technologies4030031
Chicago/Turabian StyleDesideri, Lorenzo, Devis Trioschi, Roberta Agusto, Martina Bizzarri, Gianantonio Spagnolin, Sabrina Cantelli, Caterina Paolini, Massimiliano Malavasi, and Claudio Bitelli. 2016. "The Provision of Powered Mobility Devices in Italy: Linking Process with Outcomes" Technologies 4, no. 3: 31. https://doi.org/10.3390/technologies4030031
APA StyleDesideri, L., Trioschi, D., Agusto, R., Bizzarri, M., Spagnolin, G., Cantelli, S., Paolini, C., Malavasi, M., & Bitelli, C. (2016). The Provision of Powered Mobility Devices in Italy: Linking Process with Outcomes. Technologies, 4(3), 31. https://doi.org/10.3390/technologies4030031