The Effects of Long-Term Child–Robot Interaction on the Attention and the Engagement of Children with Autism

 ,
, 
Abstract
1. Introduction
2. Background
2.1. ASD and Pivotal Response Treatment
2.2. Attention
2.3. Engagement
3. Methodology
3.1. Participants
3.2. Procedures
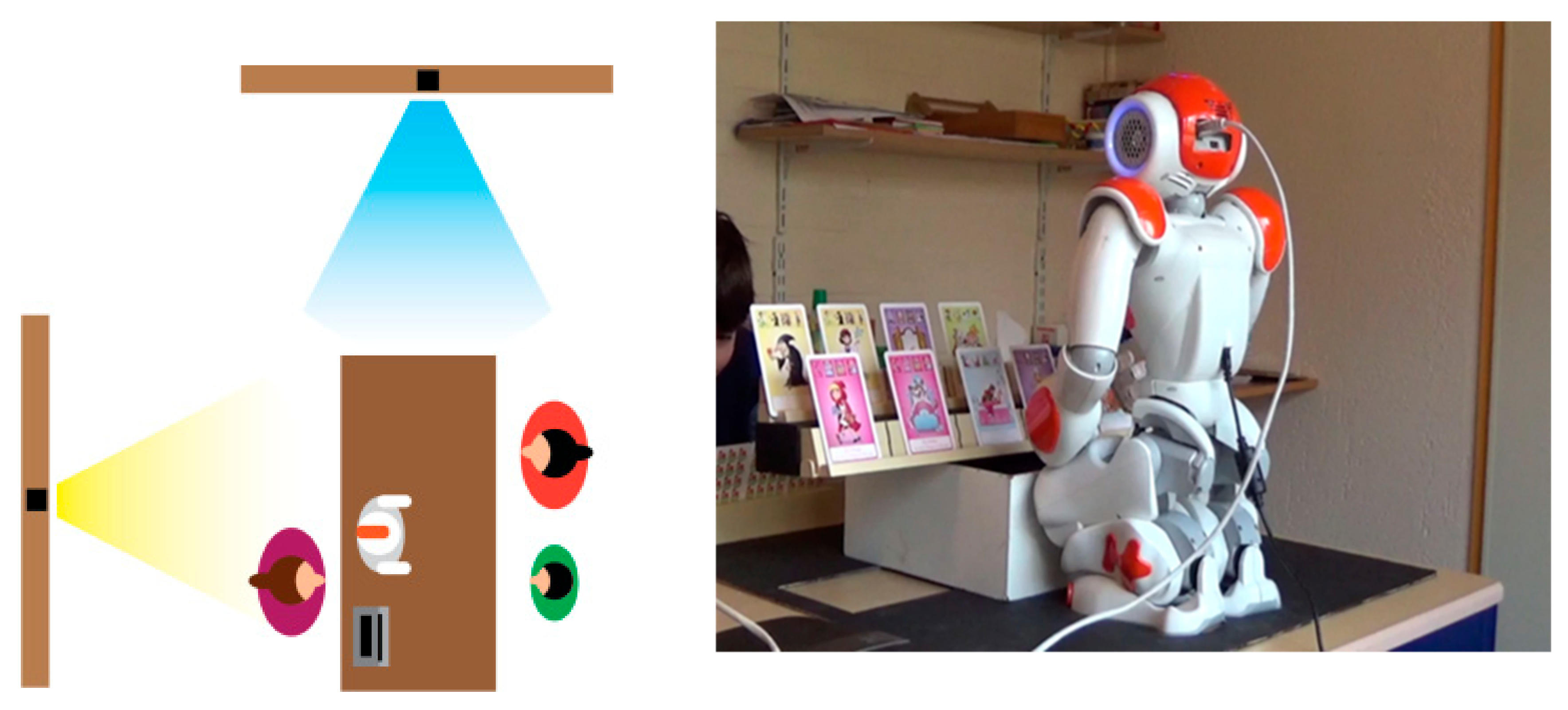
3.3. Setting
3.4. Design and Materials
3.4.1. Game Flow
3.4.2. The Robot Behavior
3.4.3. Building the Coding Scheme
3.4.4. Video Material
3.5. Data Analysis
4. Results
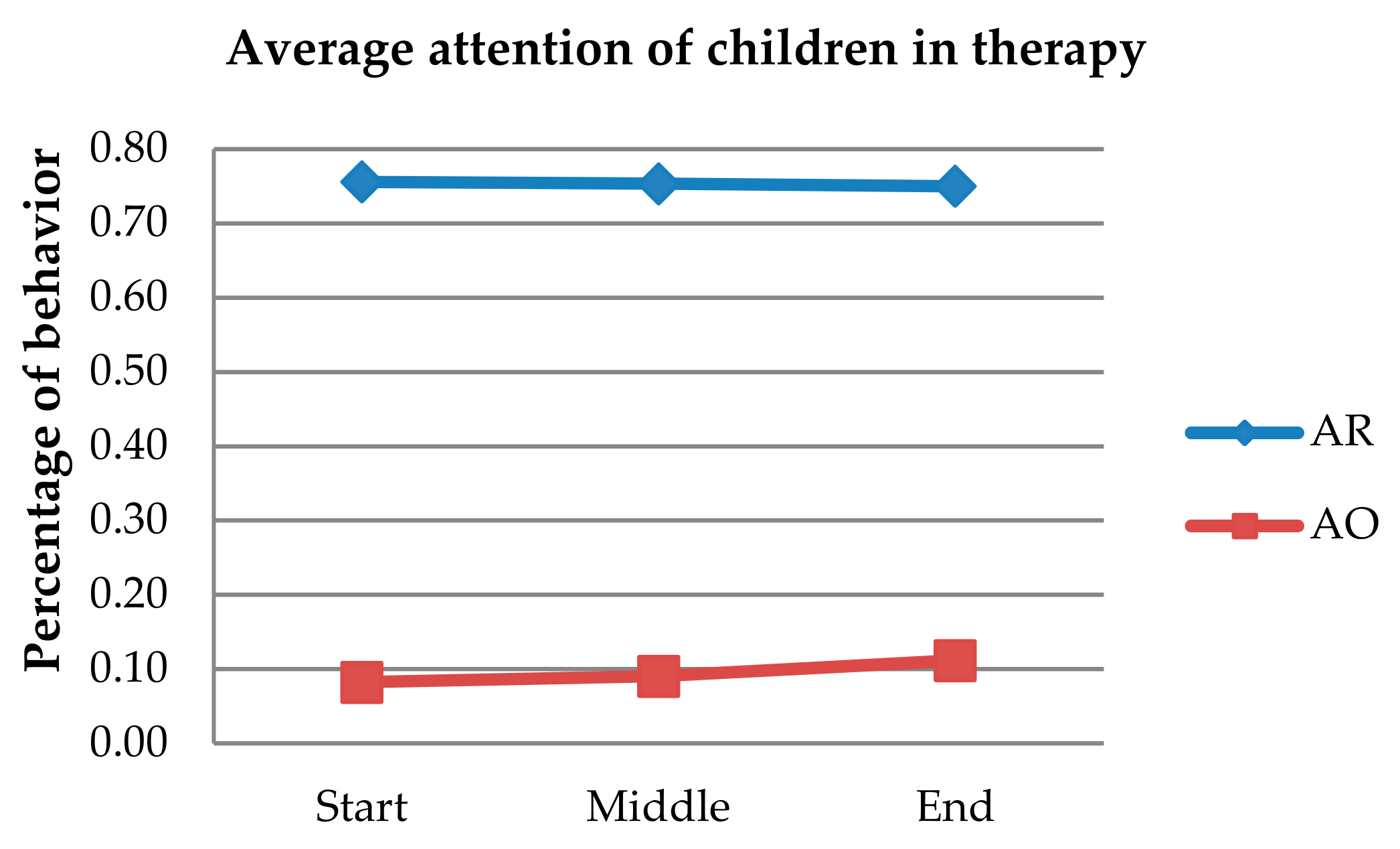
4.1. Attention towards the Robot
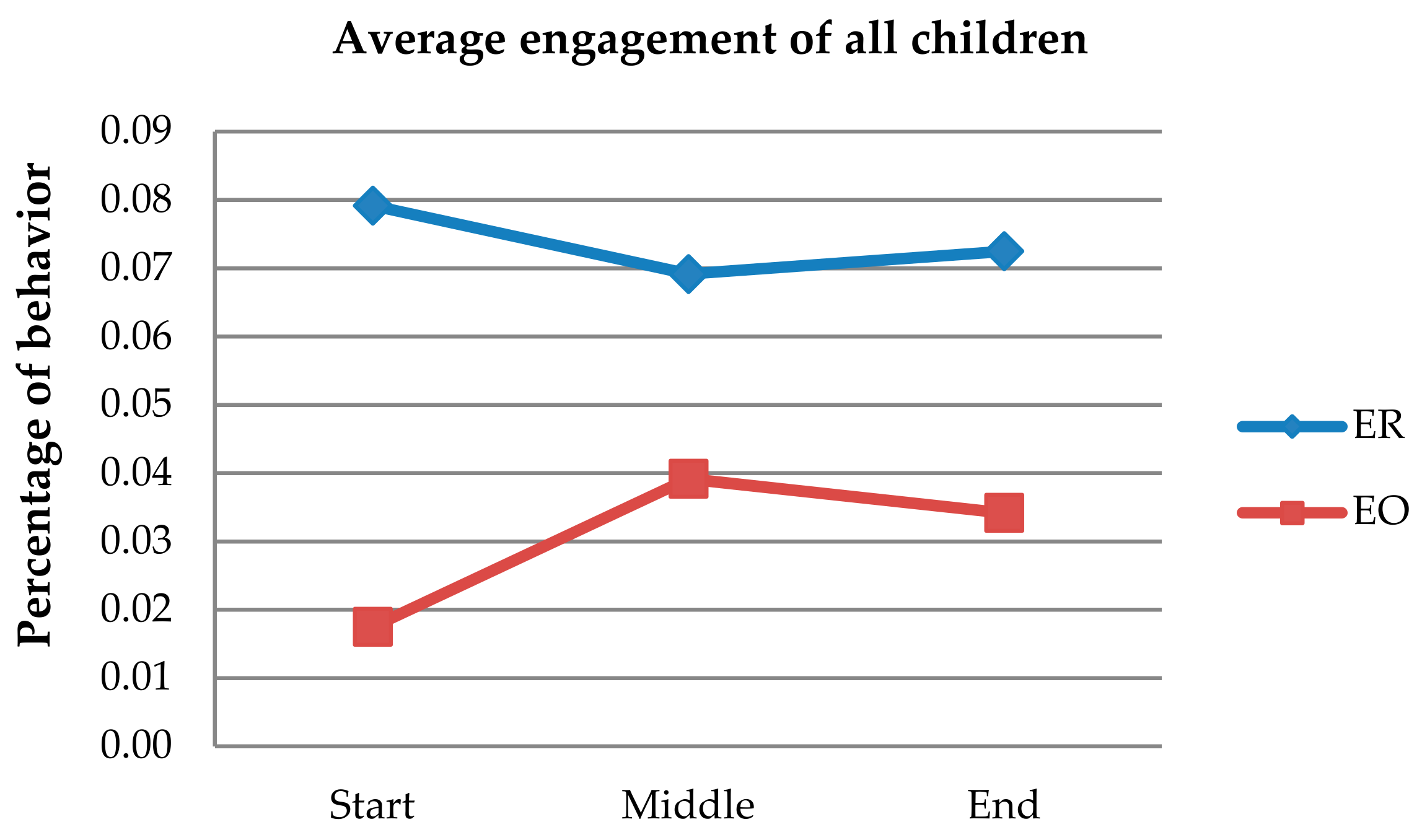
4.2. Engagement with the Robot
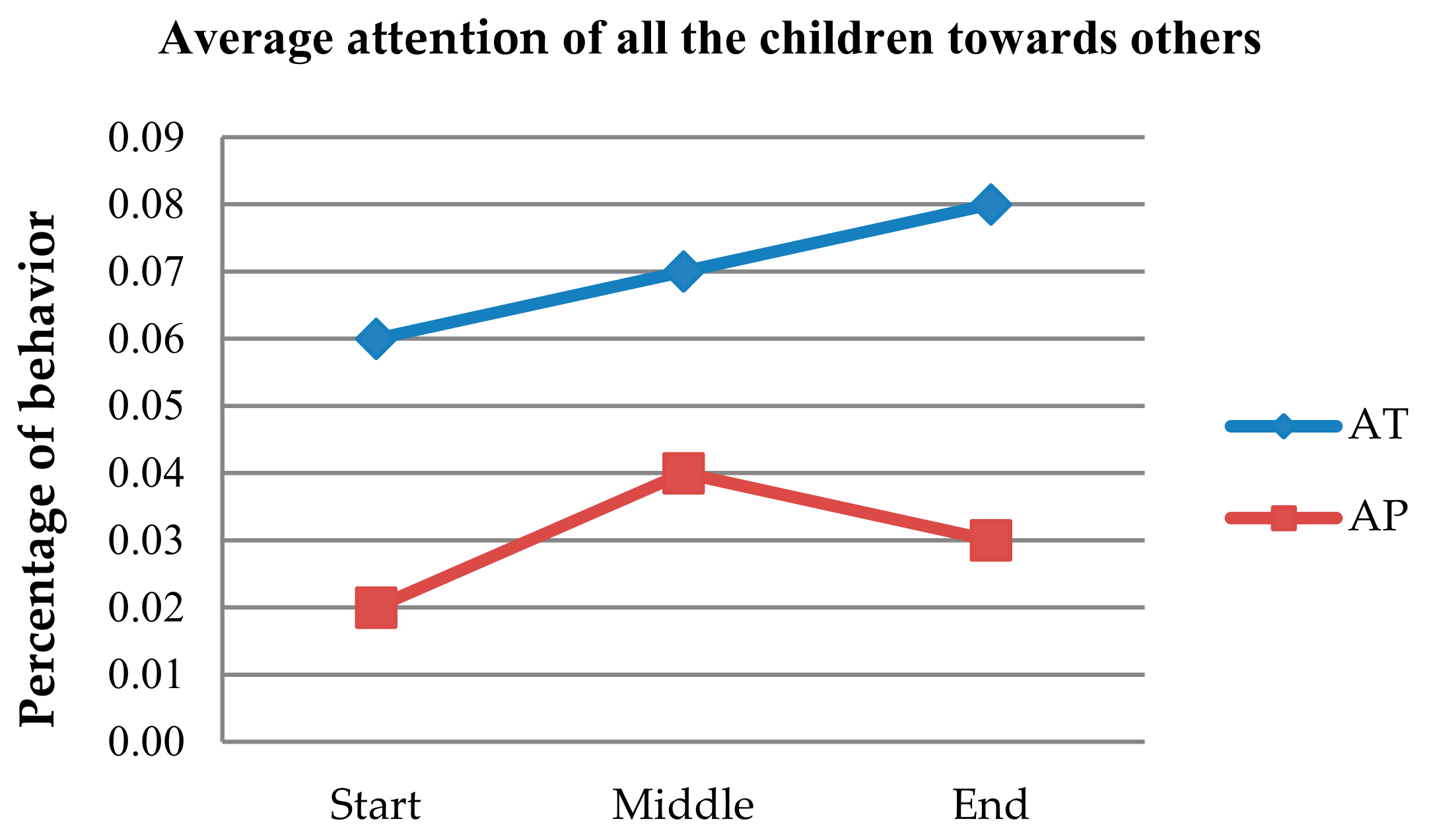
4.3. Attention towards Others in the Therapy
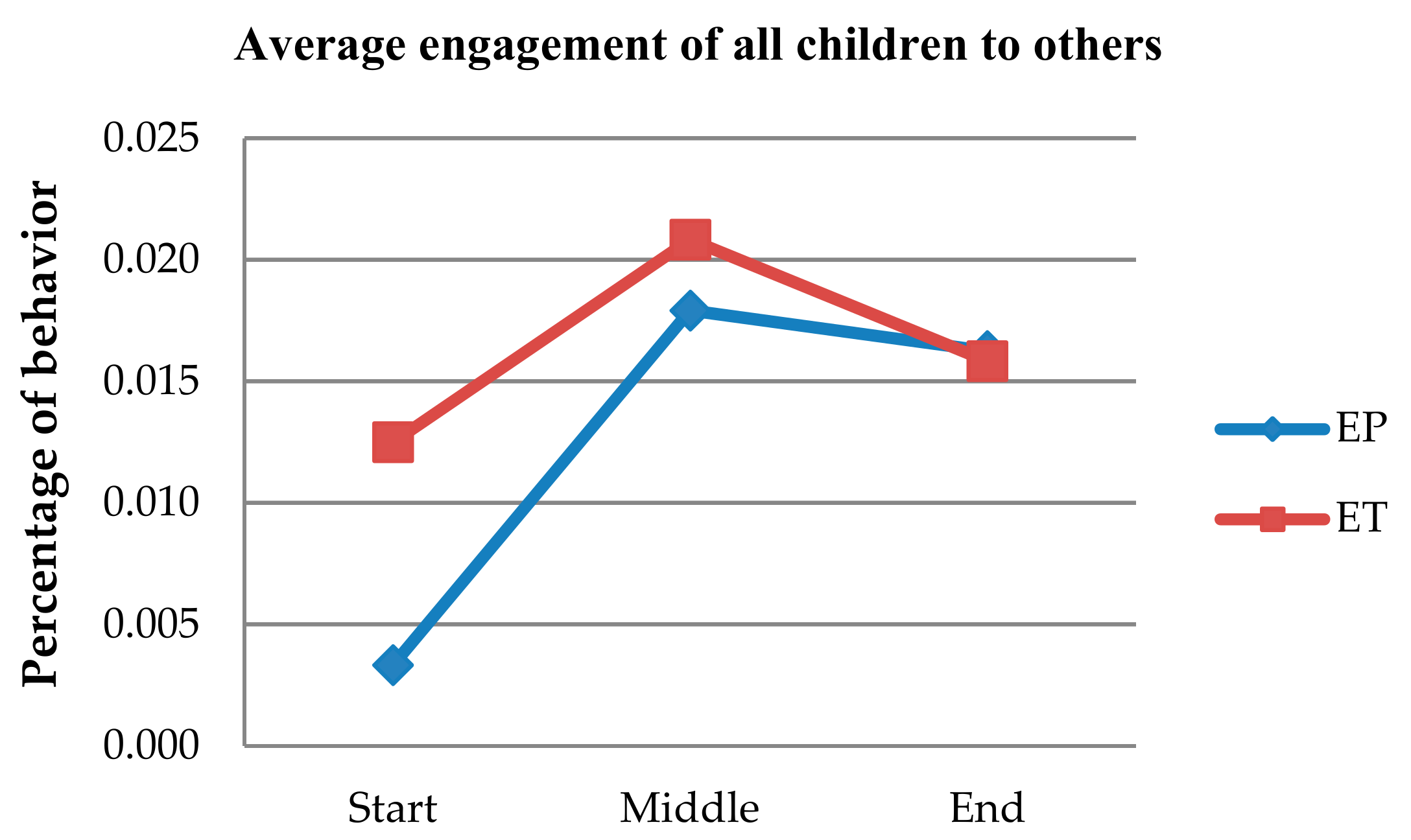
4.4. Engagement with Others in the Therapy
5. Discussion
6. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Scassellati, B.; Admoni, H.; Matarić, M. Robots for Use in Autism Research. Annu. Rev. Biomed. Eng. 2012, 14, 275–294. [Google Scholar] [CrossRef] [PubMed]
- Huijnen, C.A.G.J.; Lexis, M.A.S.; Jansens, R.; De Witte, L.P. Mapping Robots to Therapy and Educational Objectives for Children with Autism Spectrum Disorder. J. Autism Dev. Disord. 2016, 46, 2100–2114. [Google Scholar] [CrossRef] [PubMed]
- Huskens, B.; Verschuur, R.; Gillesen, J.; Didden, R.; Barakova, E.I. Promoting question-asking in school-aged children with autism spectrum disorders: Effectiveness of a robot intervention compared to a human-trainer intervention. Dev. Neurorehabilit. 2013, 16, 345–356. [Google Scholar] [CrossRef] [PubMed]
- De Korte, M.W.; van den Berk-Smeekens, I.; van Dongen-Boomsma, M.; Oosterling, I.J.; Den Boer, J.C.; Barakova, E.I.; Lourens, T.; Buitelaar, J.K.; Glennon, J.C.; Staal, W.G. Self-initiations in young children with autism during Pivotal Response Treatment with and without robot assistance. Autism 2020, 1362361320935006. [Google Scholar] [CrossRef] [PubMed]
- Rudovic, O.; Lee, J.; Mascarell-Maricic, L.; Schuller, B.W.; Picard, R.W. Measuring Engagement in Robot-Assisted Autism Therapy: A Cross-Cultural Study. Front. Robot. AI 2017, 4, 36. [Google Scholar] [CrossRef]
- McDuffie, A.; Lieberman, R.G.; Yoder, P.J. Object interest in autism spectrum disorder: A treatment comparison. Autism 2011, 16, 398–405. [Google Scholar] [CrossRef]
- Tapus, A.; Peca, A.; Aly, A.; Pop, C.; Jisa, L.; Pintea, S.; Rusu, A.S.; David, O.A. Children with autism social engagement in interaction with Nao, an imitative robot: A series of single case experiments. Interact. Stud. 2012, 13, 315–347. [Google Scholar] [CrossRef]
- Coninx, A.; Baxter, P.; Oleari, E.; Bellini, S.; Bierman, B.; Henkemans, O.B.; Cañamero, L.; Cosi, P.; Enescu, V.; Espinoza, R.R.; et al. Towards Long-Term Social Child-Robot Interaction: Using Multi-Activity Switching to Engage Young Users. J. Hum. Robot Interact. 2015, 5, 32–67. [Google Scholar] [CrossRef]
- Ahmad, M.I.; Mubin, O.; Orlando, J. Adaptive Social Robot for Sustaining Social Engagement during Long-Term Children–Robot Interaction. Int. J. Hum. Comput. Interact. 2017, 33, 943–962. [Google Scholar] [CrossRef]
- Barakova, E.I.; Bajracharya, P.; Willemsen, M.; Lourens, T.; Huskens, B. Long-term LEGO therapy with humanoid robot for children with ASD. Expert Syst. 2014, 32, 698–709. [Google Scholar] [CrossRef]
- Van den Berk-Smeekens, I.V.D.; Van Dongen-Boomsma, M.; De Korte, M.W.P.; Boer, J.C.D.; Oosterling, I.J.; Peters-Scheffer, N.C.; Buitelaar, J.K.; Barakova, E.I.; Lourens, T.; Staal, W.G.; et al. Adherence and acceptability of a robot-assisted Pivotal Response Treatment protocol for children with autism spectrum disorder. Sci. Rep. 2020, 10, 8110. [Google Scholar] [CrossRef]
- Leite, I.; Martinho, C.; Paiva, A. Social Robots for Long-Term Interaction: A Survey. Int. J. Soc. Robot. 2013, 5, 291–308. [Google Scholar] [CrossRef]
- Cautionary Statement for Forensic Use of DSM-5. In Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; American Psychiatric Association Publishing: Washington, DC, USA, 2014.
- Marino, F.; Chilà, P.; Sfrazzetto, S.T.; Carrozza, C.; Crimi, I.; Failla, C.; Busà, M.; Bernava, G.; Tartarisco, G.; Vagni, D.; et al. Outcomes of a Robot-Assisted Social-Emotional Understanding Intervention for Young Children with Autism Spectrum Disorders. J. Autism Dev. Disord. 2019, 50, 1973–1987. [Google Scholar] [CrossRef] [PubMed]
- Happé, F. The Autistic Spectrum: A Guide for Parents and Professionals. By L. Wing. (Pp. 239) Constable: London. 1999. Psychol. Med. 2000, 30, 231–239. [Google Scholar] [CrossRef][Green Version]
- Staal, W. Autismespectrumstoornissen. In Leerboek Ontwikkelingsstroonissen in de Levensloop: Een Integrale Medische en Psychologische Visie; De Tijdstroom: Utrecht, The Netherlands, 2016; pp. 221–241. [Google Scholar]
- Shamsuddin, S.; Yussof, H.; Ismail, L.; Hanapiah, F.A.; Mohamed, S.; Piah, H.A.; Zahari, N.I. Initial response of autistic children in human-robot interaction therapy with humanoid robot NAO. In Proceedings of the 2012 IEEE 8th International Colloquium on Signal Processing and its Applications, Melaka, Malaysia, 23–25 March 2012; pp. 188–193. [Google Scholar]
- Matson, J.L. Determining treatment outcome in early intervention programs for autism spectrum disorders: A critical analysis of measurement issues in learning based interventions. Res. Dev. Disabil. 2007, 28, 207–218. [Google Scholar] [CrossRef]
- Koegel, R.L.; Koegel, L.K.; McNerney, E.K. Pivotal Areas in Intervention for Autism. J. Clin. Child Adolesc. Psychol. 2001, 30, 19–32. [Google Scholar] [CrossRef] [PubMed]
- Joustra, H.; van Lommel, S. Pivotal Response Treatment: Een gedragstherapeutische behandeling gericht op motivatie en communicatie. In Applied Behavior Analysis Bij Kinderen en Adolescenten Met Autism; 2013; Available online: https://metadata.isbn.nl/843679/applied-behavior-analysis-bij-kinderen-en-adolescenten-met-autisme.html (accessed on 28 September 2020).
- Koegel, L.K.; Koegel, R.L.; Harrower, J.K.; Carter, C.M. Pivotal Response Intervention I: Overview of Approach. J. Assoc. Pers. Sev. Handicap. 1999, 24, 174–185. [Google Scholar] [CrossRef]
- Zimbardo, P.G.; Johnson, R.L.; McCann, V. Psychologie een Inleiding, 7th ed.; Pearson Benelux: Amsterdam, The Netherlands, 2013. [Google Scholar]
- Egeth, H.; Kahneman, D. Attention and Effort. Am. J. Psychol. 1975, 88, 339. [Google Scholar] [CrossRef]
- Noterdaeme, M.; Amorosa, H.; Mildenberger, K.; Sitter, S.; Minow, F. Evaluation of attention problems in children with autism and children with a specific language disorder. Eur. Child Adolesc. Psychiatry 2001, 10, 58–66. [Google Scholar] [CrossRef]
- Mayes, S.D.; Calhoun, S.L. Learning, Attention, Writing, and Processing Speed in Typical Children and Children with ADHD, Autism, Anxiety, Depression, and Oppositional-Defiant Disorder. Child Neuropsychol. 2007, 13, 469–493. [Google Scholar] [CrossRef]
- McDuffie, A.; Yoder, P.J.; Stone, W.L. Labels increase attention to novel objects in children with autism and comprehension-matched children with typical development. Autism 2006, 10, 288–301. [Google Scholar] [CrossRef] [PubMed]
- Joseph, R.M.; Tager-Flusberg, H. An investigation of attention and affect in children with autism and Down syndrome. J. Autism Dev. Disord. 1997, 27, 385–396. [Google Scholar] [CrossRef] [PubMed]
- Chevallier, C.; Parish-Morris, J.; McVey, A.; Rump, K.M.; Sasson, N.J.; Herrington, J.D.; Schultz, R.T. Measuring social attention and motivation in autism spectrum disorder using eye-tracking: Stimulus type matters. Autism Res. 2015, 8, 620–628. [Google Scholar] [CrossRef]
- Sidner, C.L.; Dzikovska, M. Human-robot interaction: Engagement between humans and robots for hosting activities. In Proceedings of the Fourth IEEE International Conference on Multimodal Interfaces ICMI-02, Pittsburgh, PA, USA, 16 October 2002; pp. 123–128. [Google Scholar]
- Perugia, G.; Van Berkel, R.; Díaz-Boladeras, M.; Català-Mallofré, A.; Rauterberg, M.; Barakova, E. Understanding Engagement in Dementia Through Behavior. The Ethographic and Laban-Inspired Coding System of Engagement (ELICSE) and the Evidence-Based Model of Engagement-Related Behavior (EMODEB). Front. Psychol. 2018, 9, 690. [Google Scholar] [CrossRef]
- Anzalone, S.M.; Boucenna, S.; Ivaldi, S.; Chetouani, M. Evaluating the Engagement with Social Robots. Int. J. Soc. Robot. 2015, 7, 465–478. [Google Scholar] [CrossRef]
- Sidner, C.L.; Lee, C.; Kidd, C.D.; Lesh, N.; Rich, C. Explorations in engagement for humans and robots. Artif. Intell. 2005, 166, 140–164. [Google Scholar] [CrossRef]
- Kort, W.; Schittekatte, M.; Dekker, P.; Verhaeghe, P.; Compaan, E.; Bosmans, M.; Vermeir, G. Wechsler intelligence scale for children (WISC-III NL). In Handleiding en Verantwoording, 3rd ed.; Harcourt Test Publishers, Instituut voor Psychologen: Amsterdam, The Netherlands, 2005. [Google Scholar]
- Hendriksen, J.; Hurks, P. WPPSI-III-NL Wechsler Preschool and Primary Scale of Intelligence; Nederlandse Bewerking; Pearson: Amsterdam, The Netherlands, 2009. [Google Scholar]
- Mullen, E.M. Mullen Scales of Early Learning; American Guidance; Service Inc.: Circle Pines, MN, USA, 1995. [Google Scholar]
- SoftBank Robotics. “NAO”. Available online: https://www.softbankrobotics.com/emea/en/nao (accessed on 6 May 2019).
- Barakova, E.I.; Gillesen, J.; Huskens, B.; Lourens, T. End-user programming architecture facilitates the uptake of robots in social therapies. Robot. Auton. Syst. 2013, 61, 704–713. [Google Scholar] [CrossRef]
- Kim, M.-G.; Oosterling, I.; Lourens, T.; Staal, W.; Buitelaar, J.; Glennon, J.; Smeekens, I.; Barakova, E.I. Designing robot-assisted Pivotal Response Training in game activity for children with autism. In Proceedings of the 2014 IEEE International Conference on Systems, Man, and Cybernetics (SMC), San Diego, CA, USA, 5–8 October 2014; pp. 1101–1106. [Google Scholar]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Child’s Behavior | Direction of Behavior | Affect |
|---|---|---|
| Gaze behavior | Gaze towards the robot Gaze towards the game Gaze towards the parent Gaze towards the therapist Non-directed gaze No gaze visible | Positive facial expression Neutral facial expression Negative facial expression |
| Arm/hand behavior | Arm/hand towards the robot Arm/hand towards the game Arm/hand towards the parent Arm/hand towards the therapist Non-directed arm/hand movement No Arm/hand movement | Positive gesture Neutral gesture Negative gesture |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
van Otterdijk, M.T.H.; de Korte, M.W.P.; van den Berk-Smeekens, I.; Hendrix, J.; van Dongen-Boomsma, M.; den Boer, J.C.; Buitelaar, J.K.; Lourens, T.; Glennon, J.C.; Staal, W.G.; et al. The Effects of Long-Term Child–Robot Interaction on the Attention and the Engagement of Children with Autism. Robotics 2020, 9, 79. https://doi.org/10.3390/robotics9040079
van Otterdijk MTH, de Korte MWP, van den Berk-Smeekens I, Hendrix J, van Dongen-Boomsma M, den Boer JC, Buitelaar JK, Lourens T, Glennon JC, Staal WG, et al. The Effects of Long-Term Child–Robot Interaction on the Attention and the Engagement of Children with Autism. Robotics. 2020; 9(4):79. https://doi.org/10.3390/robotics9040079
Chicago/Turabian Stylevan Otterdijk, Maria T. H., Manon W. P. de Korte, Iris van den Berk-Smeekens, Jorien Hendrix, Martine van Dongen-Boomsma, Jenny C. den Boer, Jan K. Buitelaar, Tino Lourens, Jeffrey C. Glennon, Wouter G. Staal, and et al. 2020. "The Effects of Long-Term Child–Robot Interaction on the Attention and the Engagement of Children with Autism" Robotics 9, no. 4: 79. https://doi.org/10.3390/robotics9040079
APA Stylevan Otterdijk, M. T. H., de Korte, M. W. P., van den Berk-Smeekens, I., Hendrix, J., van Dongen-Boomsma, M., den Boer, J. C., Buitelaar, J. K., Lourens, T., Glennon, J. C., Staal, W. G., & Barakova, E. I. (2020). The Effects of Long-Term Child–Robot Interaction on the Attention and the Engagement of Children with Autism. Robotics, 9(4), 79. https://doi.org/10.3390/robotics9040079