The Contribution of New Areas to the Total Hirsutism Scores in Basrah Hirsute Women


Abstract
:1. Introduction
2. Patients and Methods
2.1. Design and Participants
2.1.1. Inclusion Criteria
2.1.2. Exclusion Criteria
- Premenarchal or postmenopausal patients
- Patients with drugs history that might interfere with the results e.g., anabolic steroid, metoclopramide, methyldopa, phenothiazine
- Patients who received oral contraceptive pills or/and other anti-androgen drugs in previous three months
- Those who failed to report follow-up visit will be excluded from the study
- Patients with m-FG scoring ˂8
- Pregnancy
- Breastfeeding
2.2. Physical Evaluation
2.3. Laboratory Tests
2.3.1. Basal Hormone Measurement
2.3.2. Metabolic Profile
2.4. Imaging
2.4.1. Ovarian Ultrasonography
2.4.2. Computed Tomography (CT) or Magnetic Resonance Imaging (MRI)
2.5. Statistical Analysis
3. Results
4. Discussion
5. Limitation
6. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Azziz, R. The evaluation and management of hirsutism. Obstet. Gynecol. 2003, 101, 995–1007. [Google Scholar] [PubMed]
- Rittmaster, R.S.; Loriaux, D.L. Hirsutism. Ann. Intern. Med. 1987, 106, 95–107. [Google Scholar] [CrossRef] [PubMed]
- Ferriman, D.; Gallwey, J. Clinical assessment of body hair growth in women. J. Clin. Endocrinol. Metab. 1961, 21, 1440–1447. [Google Scholar] [CrossRef] [PubMed]
- Hatch, R.; Rosenfield, R.L.; Kim, M.H.; Tredway, D. Hirsutism: Implications, etiology, and management. Am. J. Obstet. Gynecol. 1981, 140, 815–830. [Google Scholar] [CrossRef]
- Hassa, H.; Tanir, H.M.; Yildirim, A.; Senses, T.; Eskalen, M.; Mutlu, F.S. The hirsutism scoring system should be population specific. Fertil. Steril. 2005, 84, 778–780. [Google Scholar] [CrossRef] [PubMed]
- Redmond, G. Clinical Evaluation of the Woman with an Androgenic Disorder; Androgenic Disorders Raven Press: New York, NY, USA, 1995; pp. 1–20. [Google Scholar]
- Harrison, S.; Somani, N.; Bergfeld, W.F. Update on the management of hirsutism. Clevel. Clin. J. Med. 2010, 77, 388–398. [Google Scholar] [CrossRef] [PubMed]
- Somani, N.; Harrison, S.; Bergfeld, W.F. The clinical evaluation of hirsutism. Dermatol. Ther. 2008, 21, 376–391. [Google Scholar] [CrossRef] [PubMed]
- Camacho-Martίnez, F.M. Hirsutism. Hair Growth and Disorders; Blume-Peytavi, U., Tosti, A., Trüeb, R.M., Eds.; Springer: Berlin/Heidelberg, Germany, 2008; p. 365. [Google Scholar]
- Brodell, L.A.; Mercurio, M.G. Hirsutism: Diagnosis and management. Gend. Med. 2010, 7, 79–87. [Google Scholar] [CrossRef] [PubMed]
- Eshre, T.R. Group A-SPCW. Revised 2003 consensus on diagnostic criteria and long-term health risks related to polycystic ovary syndrome. Fertil. Steril. 2004, 81, 19–25. [Google Scholar]
- Azziz, R.; Carmina, E.; Sawaya, M.E. Idiopathic hirsutism. Endocr. Rev. 2000, 21, 347–362. [Google Scholar] [CrossRef] [PubMed]
- Rashidi, H.; Tehrani, F.R.; Khomami, M.B.; Tohidi, M.; Azizi, F. To what extent does the use of the Rotterdam criteria affect the prevalence of polycystic ovary syndrome? A community-based study from the Southwest of Iran. Eur. J. Obstet. Gynecol. Reprod. Biol. 2014, 174, 100–105. [Google Scholar] [CrossRef] [PubMed]
- American Diabetes Association. 2. Classification and Diagnosis of Diabetes. Diabetes Care 2016, 39 (Suppl. 1), S13–S22. [Google Scholar]
- Malik, L.M.; Ahmad, T.J. A diagnostic approach towards patients with hirsutism-screening for sinister causes. J. Pak. Assoc. Dermatol. 2005, 15, 320–322. [Google Scholar]
- Practice Committee of the American Society for Reproductive Medicine. The evaluation and treatment of androgen excess. Fertil. Steril. 2006, 86 (Suppl. 1), S241–S247. [Google Scholar]
- Apridonidze, T.; Essah, P.A.; Iuorno, M.J.; Nestler, J.E. Prevalence and characteristics of the metabolic syndrome in women with polycystic ovary syndrome. J. Clin. Endocrinol. Metab. 2005, 90, 1929–1935. [Google Scholar] [CrossRef] [PubMed]
- Derksen, J.; Moolenaar, A.J.; Van Seters, A.P.; Kock, D.F.M. Semiquantitative assessment of hirsutism in Dutch women. Br. J. Dermatol. 1993, 128, 259–263. [Google Scholar] [CrossRef] [PubMed]
- DÖNer, N.; EkmekçI, T.R. Criticising Modified Ferriman-Gallwey Scroring System in the Evaluation of Hirsutism in 1034 Turkish Women. Turk. Klin. J. Med. Sci. 2013, 33, 314–320. [Google Scholar] [CrossRef]
- Malik, L.M.; Khursheed, K.; Haroon, T.S.; Malik, M.A. An aetiological study of moderate to severe hirsutism. Pak. J. Med. Sci. 2007, 23, 167. [Google Scholar]
- Sharma, D.; Shanker, V.; Tegta, G.; Gupta, M.; Verma, G. Clinico-investigative profile of patients of hirsutism in a tertiary level institution. Int. J. Trichol. 2012, 4, 69–74. [Google Scholar] [CrossRef] [PubMed]
- Li, R.; Qiao, J.; Yang, D.; Li, S.; Lu, S.; Wu, X.; Wei, Z. Epidemiology of hirsutism among women of reproductive age in the community: A simplified scoring system. Eur. J. Obstet. Gynecol. Reprod. Biol. 2012, 163, 165–169. [Google Scholar] [CrossRef] [PubMed]
- Cook, H.; Brennan, K.; Azziz, R. Reanalyzing the modified Ferriman-Gallwey score: Is there a simpler method for assessing the extent of hirsutism? Fertil. Steril. 2011, 96, 1266–1270. [Google Scholar] [CrossRef] [PubMed]
- Rashidi, H.; Parizi, Z.T.; Mohammadi, M. Evaluation of only the chin or lower abdomen for predicting hirsutism. Indian J. Endocrinol. Metab. 2013, 17, 896. [Google Scholar] [CrossRef] [PubMed]
- Yildiz, B.O.; Bolour, S.; Woods, K.; Moore, A.; Azziz, R. Visually scoring hirsutism. Hum. Reprod. Update 2010, 16, 51–64. [Google Scholar] [CrossRef] [PubMed]
- DeUgarte, C.M.; Woods, K.; Bartolucci, A.A.; Azziz, R. Degree of facial and body terminal hair growth in unselected black and white women: Toward a populational definition of hirsutism. J. Clin. Endocrinol. Metab. 2006, 91, 1345–1350. [Google Scholar] [CrossRef] [PubMed]
- Knochenhauer, E.S.; Hines, G.; Conway-Myers, B.A.; Azziz, R. Examination of the chin or lower abdomen only for the prediction of hirsutism. Fertil. Steril. 2000, 74, 980–983. [Google Scholar] [CrossRef]
- Zhao, J.L.; Chen, Z.J.; Shi, Y.H.; Geng, L.; Ma, Z.X.; Li, Y.; Tang, R. Investigation of body hair assessment of Chinese women in Shandong region and its preliminary application in polycystic ovary syndrome patients. Zhonghua Fu Chan Ke Za Zhi 2007, 42, 590–594. [Google Scholar] [PubMed]
- Ansarin, H.; Aziz-Jalali, M.-H.; Rasi, A.; Soltani-Arabshahi, R. Clinical presentation and etiologic factors of hirsutism in premenopausal Iranian women. Arch. Iran. Med. 2007, 10, 7–13. [Google Scholar] [PubMed]

{kind=link}
| Body Area | Mean | Std. Error | 95% Confidence Interval for Mean |
|---|---|---|---|
| Upper lip | 2.3 | 0.12 | 2.2–2.4 |
| Chin | 2.6 | 0.11 | 2.5–2.8 |
| Upper back | 1.0 | 0.10 | 0.9–1.1 |
| Lower back | 1.4 | 0.13 | 1.2–1.5 |
| Upper arm | 0.7 | 0.04 | 0.6–0.8 |
| Thigh | 2.6 | 0.18 | 2.5–2.7 |
| Chest | 0.7 | 0.05 | 0.6–0.8 |
| Upper abdomen | 1.6 | 0.10 | 1.5–1.8 |
| Lower abdomen | 3.7 | 0.09 | 3.6–3.8 |
| Sideburn | 2.4 | 0.16 | 2.3–2.6 |
| Jaw and neck | 1.1 | 0.04 | 0.9–1.2 |
| Buttock and perineum | 1.4 | 0.09 | 1.2–1.5 |
| Total | 1.8 | 0.13 | 1.7–1.88 |
| Total Score for Three New Areas vs. Total Score for Nine Areas | |
|---|---|
| z statistic | 0.599 |
| p value | p = 0.5490 |
| Total Score for Three New Areas vs. Total for 12 Areas | |
| z statistic | 2.376 |
| p value | p = 0.0175 |
| Total Score for Nine Areas vs. Total Score for 12 Areas | |
| z statistic | 0.998 |
| p value | p = 0.3184 |
| Body Area | Area under the Curve | 95% CI | |
|---|---|---|---|
| Lower Limit | Upper Limit | ||
| Chest | 0.938 | 0.879 | 0.996 |
| Lower back | 0.911 | 0.833 | 0.988 |
| Sideburn | 0.904 | 0.806 | 1.000 |
| Upper arm | 0.901 | 0.803 | 0.997 |
| Upper abdomen | 0.898 | 0.820 | 0.975 |
| Lower jaw/neck | 0.884 | 0.770 | 0.995 |
| Upper back | 0.879 | 0.757 | 0.998 |
| Thighs | 0.837 | 0.700 | 0.971 |
| Chin | 0.829 | 0.662 | 0.992 |
| Buttock/perineum | 0.815 | 0.627 | 0.999 |
| Upper lip | 0.769 | 0.534 | 0.999 |
| Lower abdomen | 0.602 | 0.406 | 0.794 |
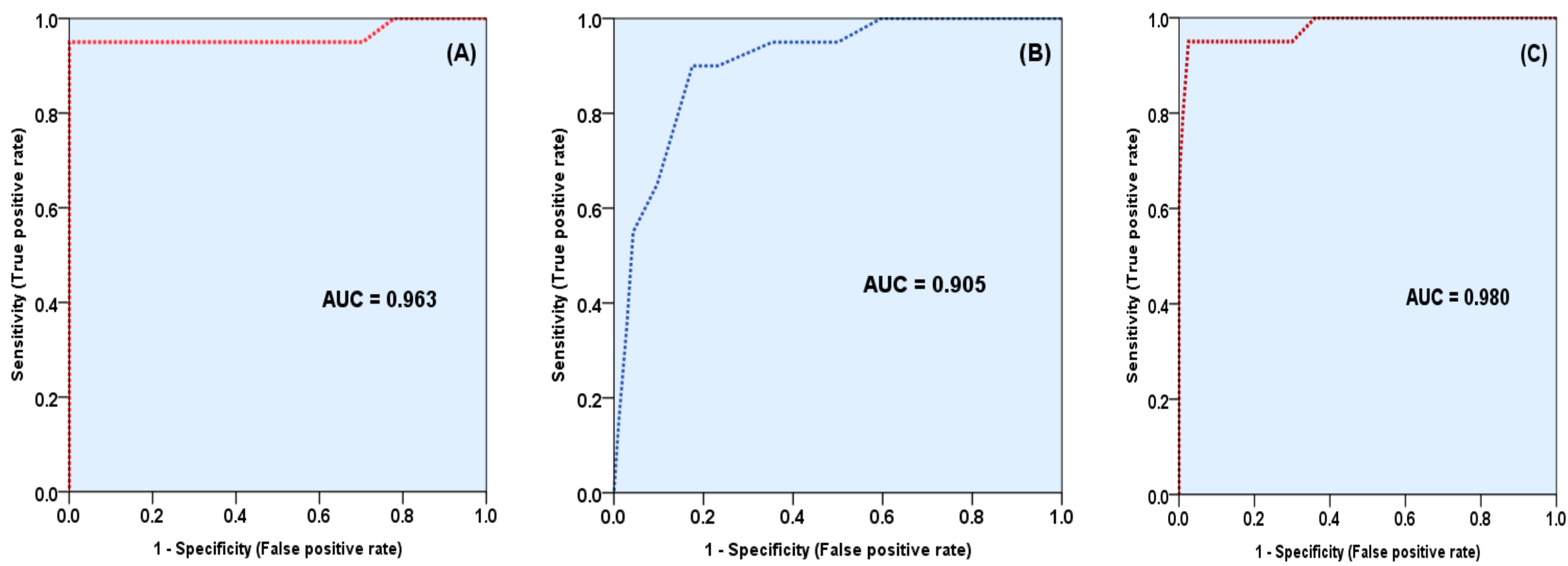
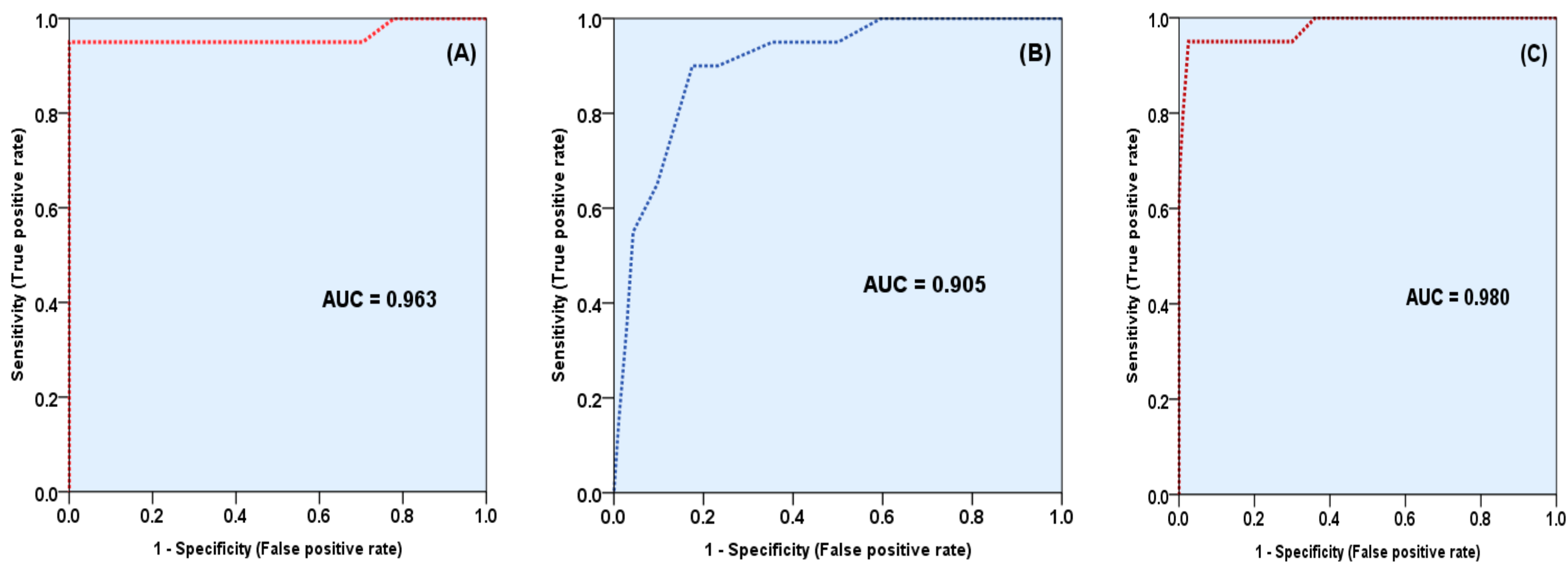
| Total score for all 12 areas | 0.986 | 0.960 | 0.999 |
| Total m-FG score 9 areas | 0.963 | 0.934 | 0.992 |
| Total score for 3 new areas | 0.905 | 0.811 | 0.997 |
| Body Areas | Severity of Hirsutism | p | |||||
|---|---|---|---|---|---|---|---|
| Mild | Moderate | Severe | |||||
| Mean | SE * | Mean | SE | Mean | SE | ||
| Upper lip | 1.99 | 0.07 | 2.60 | 0.07 | 3.10 | 0.22 | <0.001 |
| Chin | 2.07 | 0.11 | 3.16 | 0.10 | 3.95 | 0.05 | <0.001 |
| Upper back | 0.53 | 0.05 | 1.30 | 0.09 | 2.55 | 0.23 | <0.001 |
| Lower back | 0.64 | 0.06 | 2.08 | 0.11 | 3.40 | 0.17 | <0.001 |
| Upper arm | 0.25 | 0.04 | 1.01 | 0.10 | 2.75 | 0.26 | <0.001 |
| Thighs | 2.07 | 0.07 | 3.13 | 0.07 | 3.70 | 0.11 | <0.001 |
| Chest | 0.30 | 0.05 | 0.96 | 0.09 | 2.60 | 0.21 | <0.001 |
| Upper abdomen | 1.01 | 0.07 | 2.22 | 0.08 | 3.25 | 0.16 | <0.001 |
| Lower abdomen | 3.48 | 0.08 | 3.88 | 0.04 | 4.00 | 0.00 | <0.001 |
| Sideburn | 1.33 | 0.07 | 2.91 | 0.10 | 3.90 | 0.07 | <0.001 |
| Lower jaw/neck | 0.66 | 0.08 | 1.34 | 0.11 | 3.00 | 0.23 | <0.001 |
| Buttock/perineum | 0.67 | 0.08 | 1.92 | 0.12 | 2.90 | 0.27 | <0.001 |
| Total m-FG score 9 areas | 12.33 | 0.20 | 20.34 | 0.22 | 28.10 | 0.47 | <0.001 |
| Total score for 3 new areas | 3.33 | 0.21 | 6.17 | 0.23 | 9.40 | 1.00 | <0.001 |
| Total score for all 12 areas | 15.67 | 0.33 | 26.51 | 0.40 | 37.85 | 1.07 | <0.001 |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hussein, R.N.; Hamdi, K.I.A.; Mansour, A.A. The Contribution of New Areas to the Total Hirsutism Scores in Basrah Hirsute Women. Diseases 2017, 5, 32. https://doi.org/10.3390/diseases5040032
Hussein RN, Hamdi KIA, Mansour AA. The Contribution of New Areas to the Total Hirsutism Scores in Basrah Hirsute Women. Diseases. 2017; 5(4):32. https://doi.org/10.3390/diseases5040032
Chicago/Turabian StyleHussein, Rudha Naser, Khalil Ismail Al Hamdi, and Abbas Ali Mansour. 2017. "The Contribution of New Areas to the Total Hirsutism Scores in Basrah Hirsute Women" Diseases 5, no. 4: 32. https://doi.org/10.3390/diseases5040032
APA StyleHussein, R. N., Hamdi, K. I. A., & Mansour, A. A. (2017). The Contribution of New Areas to the Total Hirsutism Scores in Basrah Hirsute Women. Diseases, 5(4), 32. https://doi.org/10.3390/diseases5040032