
Atypical Rapid Onset of Olmesartan-Induced Enteropathy with Recurrence After Rechallenging

 , ,
, ,
Abstract
1. Introduction
2. Case Presentation
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| AKI | Acute kidney injury |
| ARB | Angiotensin II receptors blocker |
| AT | Angiotensin II receptor type 1 |
| CKD | Chronic kidney disease |
| GI | Gastrointestinal |
| OIE | Angiotensin II receptor type 1 (AT1 receptor) |
References
- Rubio-Tapia, A.; Herman, M.L.; Ludvigsson, J.F.; Kelly, D.G.; Mangan, T.F.; Wu, T.T.; Murray, J.A. Severe spruelike enteropathy associated with olmesartan. Mayo Clin. Proc. 2012, 87, 732–738. [Google Scholar] [CrossRef] [PubMed]
- Kamal, A.; Fain, C.; Park, A.; Wang, P.; Gonzalez-Velez, E.; Leffler, D.A.; Hutfless, S.M. Angiotensin II receptor blockers and gastrointestinal adverse events of resembling sprue-like enteropathy: A systematic review. Gastroenterol. Rep. 2019, 7, 162–167. [Google Scholar] [CrossRef] [PubMed]
- Van Horebeek, N.; Croes, R.; Vonck, A.; Colpaert, E. Olmesart0061n induced enteropathy affecting the entire gastrointestinal tract: A case report. Acta. Gastro-Enterol. Belg. 2023, 86, 95–97. [Google Scholar] [CrossRef] [PubMed]
- Storozuk, T.; Brown, I.; Lagana, S.; Westerhoff, M.; Setia, N.; Hart, J.; Alpert, L. The histological spectrum of ARB-induced gastritis. Histopathology 2022, 81, 653–660. [Google Scholar] [CrossRef] [PubMed]
- Ianiro, G.; Bibbò, S.; Montalto, M.; Ricci, R.; Gasbarrini, A.; Cammarota, G. Systematic review: Sprue-like enteropathy associated with olmesartan. Aliment. Pharmacol. Ther. 2014, 40, 16–23. [Google Scholar] [CrossRef] [PubMed]
- Burbure, N.; Lebwohl, B.; Arguelles-Grande, C.; Green, P.H.R.; Bhagat, G.; Lagana, S. Olmesartan-associated sprue-like enteropathy: A systematic review with emphasis on histopathology. Hum. Pathol. 2016, 50, 127–134. [Google Scholar] [CrossRef] [PubMed]
- Alexander, D.; Abdelazeem, B.; Alnounou, M. Olmesartan-Induced Ischemic Enteritis Complicated With Bowel Perforation: A Case Report and Literature Review. Cureus 2023, 15, e36660. [Google Scholar] [CrossRef] [PubMed]
- Holtgrewe, L.M.L.; Dippel, H.; Weckauf, H.; Linnemüller, S.; Schuppert, F. Candesartan-Induced Enteropathy That Mimics Celiac Disease in a 90-Year-Old Patient. Case Rep. Gastroenterol. 2023, 17, 185–191. [Google Scholar] [CrossRef] [PubMed]
- Kulai, T.; Arnason, T.; MacIntosh, D.; Igoe, J. Duodenal Villous Atrophy in a TTG-Negative Patient Taking Olmesartan: A Case Report and Review of the Literature. Can. J. Gastroenterol. Hepatol. 2016, 2016, 6091571. [Google Scholar] [CrossRef] [PubMed]
- Kang, M.J.; Min, K.H.; Kim, H.W.; Park, S.B.; Kang, D.H.; Choi, C.W. Olmesartan-associated Enteropathy with Acute Kidney Injury. Korean J. Gastroenterol. Taehan Sohwagi Hakhoe Chi. 2022, 79, 130–134. [Google Scholar] [CrossRef] [PubMed]
- Mehta, R.L.; Kellum, J.A.; Shah, S.V.; Molitoris, B.A.; Ronco, C.; Warnock, D.G.; Levin, A.; the Acute Kidney Injury Network. Acute Kidney Injury Network: Report of an initiative to improve outcomes in acute kidney injury. Crit. Care 2007, 11, R31. [Google Scholar] [CrossRef] [PubMed]
- Roca-Argente, L.; Diaz-Jaime, F.C.; López-Romero, L.C.; Manzur-Aguilar, Y.; Moll-Guillem, J.L.; Del Val-Antoñana, A.; Hernandez-Jaras, J. Acute kidney injury secondary to diarrhea caused by « sprue-like » enteropathy associated with olmesartan. Nefrol Publ. Soc. Esp. Nefrol. 2017, 37, 461–562. [Google Scholar]
- Mauloni, P.A.; Capuani, F.; Paone, C.; Marasco, G.; Bellacosa, L.; Cogliandro, R.F.; Cremon, C.; Barbara, G.; Vasuri, F.; Stanghellini, V. An unusual cause of diarrhoea: Case report and literature review of olmesartan-associated enteropathy. Eur. J. Gastroenterol. Hepatol. 2021, 33 (Suppl. 1), e1060–e1066. [Google Scholar] [CrossRef] [PubMed]
- Kodama, E.; Kawata, Y.; Yamazaki, S.; Igarashi, T.; Kojima, Y.; Tominaga, K.; Yokoyama, J.; Honma, T.; Terai, S. Diagnosis and resolution of olmesartan-associated sprue-like enteropathy confirmed by capsule endoscopy: A case report and literature review. Clin. J. Gastroenterol. 2024, 17, 891–898. [Google Scholar] [CrossRef] [PubMed]
- Briongos-Figuero, L.S.; Cuevas-González, J. Olmesartan-associated sprue-like enteropathy. Lancet 2023, 402, 1660. [Google Scholar] [CrossRef] [PubMed]
- Tran, T.H.; Li, H. Olmesartan and Drug-Induced Enteropathy. Pharm. Ther. 2014, 39, 47–50. [Google Scholar]
- Dong, Y.H.; Jin, Y.; Tsacogianis, T.N.; He, M.; Hsieh, P.H.; Gagne, J.J. Use of olmesartan and enteropathy outcomes: A multi-database study. Aliment. Pharmacol. Ther. 2018, 47, 792–800. [Google Scholar] [CrossRef] [PubMed]
- DeGaetani, M.; Tennyson, C.A.; Lebwohl, B.; Lewis, S.K.; Abu Daya, H.; Arguelles-Grande, C.; Bhagat, G.; Green, P.H.R. Villous atrophy and negative celiac serology: A diagnostic and therapeutic dilemma. Am. J. Gastroenterol. 2013, 108, 647–653. [Google Scholar] [CrossRef] [PubMed]
- Daines, B.S.; Kankam, A.; Tanami, S.; Nambiar, R. A Case Report of Olmesartan-Induced Enteropathy. Cureus 2021, 13, e20722. [Google Scholar] [CrossRef] [PubMed]
- Gamelas, V.; Borges, V.; Santos, S.; Santos, J.; Silva, M.; Bernardes, C.; Ramos, J. Gastrointestinal: Olmesartan-induced enterocolopathy: A new presentation of a known entity. J. Gastroenterol. Hepatol. 2021, 36, 1150. [Google Scholar] [CrossRef] [PubMed]
- Bashari, D.R. Severe Sprue-Like Enteropathy and Colitis due to Olmesartan: Lessons Learned From a Rare Entity. Gastroenterol. Res. 2020, 13, 150–154. [Google Scholar] [CrossRef] [PubMed]
- Scialom, S.; Malamut, G.; Meresse, B.; Guegan, N.; Brousse, N.; Verkarre, V.; Derrieux, C.; Macintyre, E.; Seksik, P.; Savoye, G.; et al. Gastrointestinal Disorder Associated with Olmesartan Mimics Autoimmune Enteropathy. PLoS ONE 2015, 10, e0125024. [Google Scholar] [CrossRef] [PubMed]
- Choi, E.Y.K.; McKenna, B.J. Olmesartan-Associated Enteropathy: A Review of Clinical and Histologic Findings. Arch. Pathol. Lab. Med. 2015, 139, 1242–1247. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
| 1st Admission Values | 2nd Admission Values | Normal Values | |
|---|---|---|---|
| BLOOD | |||
| Hemoglobin (g/dL) | 14.3 | 15.6 | 13–18 |
| MCV (fL) | 90 | 93 | 80–100 |
| Thrombocytes ×103/µL | 387 | 553 | 150–440 |
| Leucocytes ×103/µL | 10.68 | 15.56 | 3.5–11 |
| CRP (mg/dL) | 32 | 24 | <5 |
| Urea (mg/dL) | 437 | 127 | 17–48 |
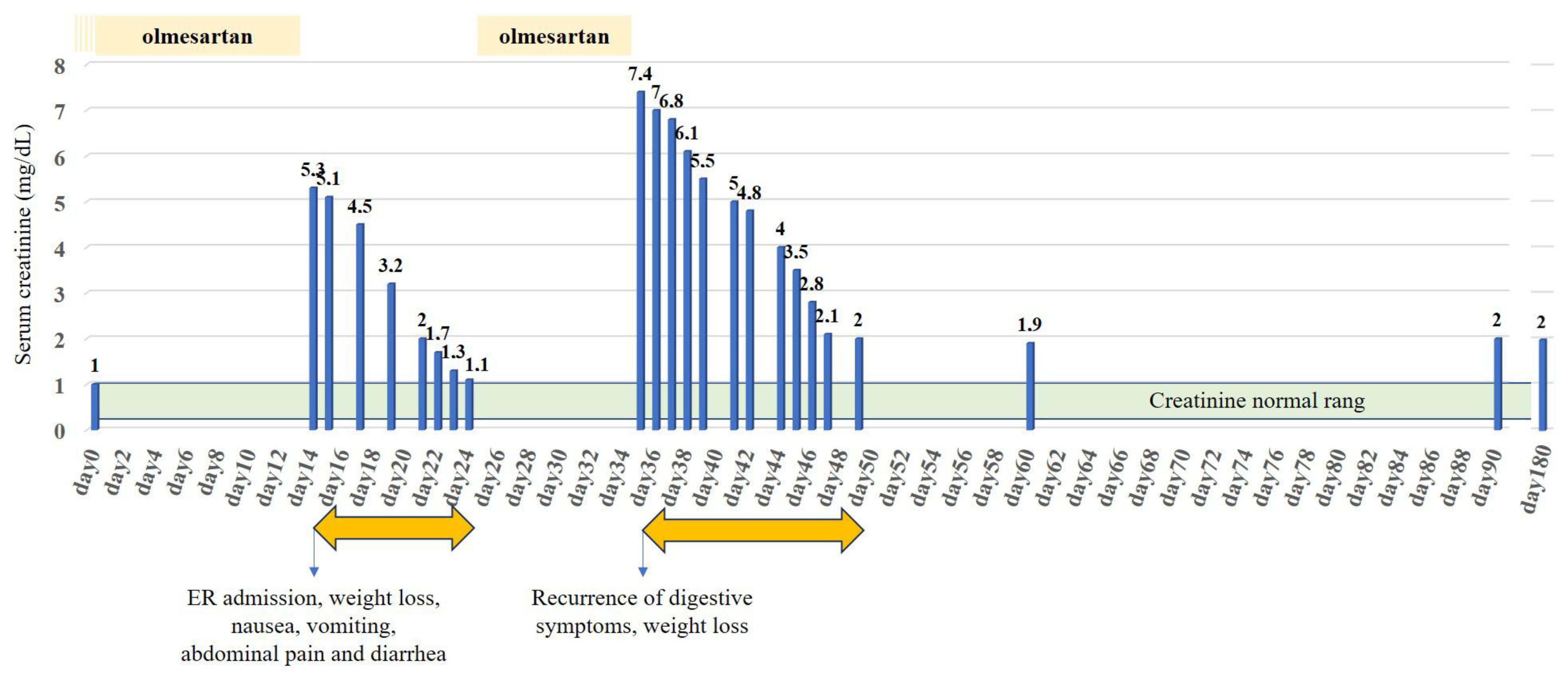
| Creatinine (mg/dL) | 5.30 | 7.44 | 0.7–1.2 |
| K/ HCO3 (mmol/L) | 3.3/12 | 3.4/8 | 3.5–4.5/23–29 |
| URINE | |||
| Erythrocytes /µL | 34 | <12 | <12 |
| Leucocytes /µL | 359 | 50 | <10 |
| Pathological cylinders | Absence | Presence (>6/2.25 µL) | Absence |
| Fractional excretion of urea (%) | 11.9 | 13.2 | |
| Fractional excretion of Sodium (%) | 0.2 | 0.1 | |
| Potassium (mmol/L) | 9 | 40 | <20 |
| - Rarity and underlooked disease [2] |
| - Heterogeneous clinical presentation, with a variety of symptoms ranging from mild enteropathy to severe diarrhea and malabsorption [4,5] |
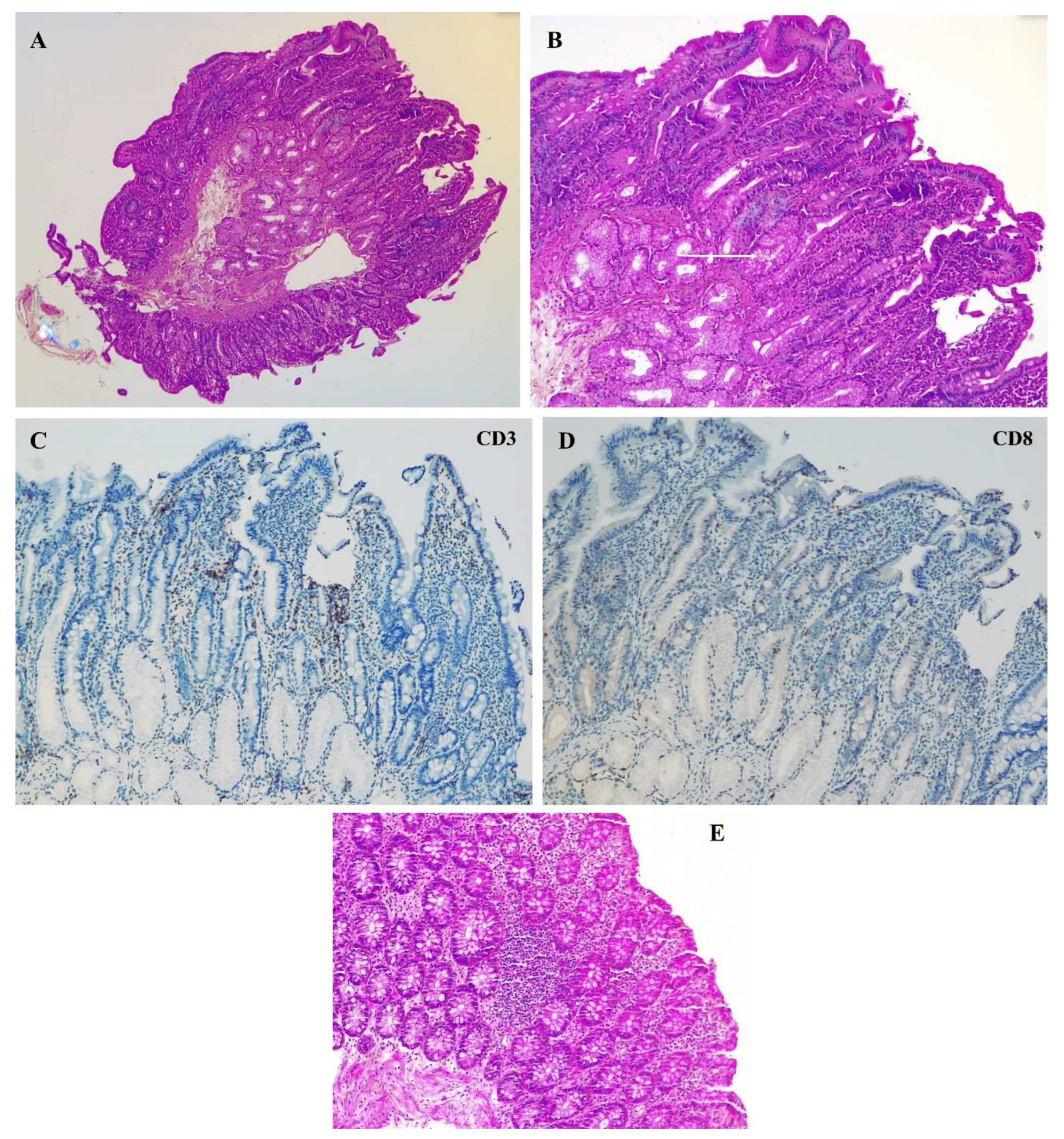
| - Heterogeneous histological presentation, ranging from unremarkable intestinal biopsy to classical “sprue like enteropathy” with villous atrophy and intraepithelial lymphocyte infiltrate [6] |
| - Patchy distribution of histological lesions, requiring multiple biopsies from various gastrointestinal [4,18,20] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bekkai, L.; Ibn Majah, A.; Verset, L.; Jacobs, L.; Danneel, C.; Elkilic, O.; Collart, F.; Nortier, J.; Taghavi, M. Atypical Rapid Onset of Olmesartan-Induced Enteropathy with Recurrence After Rechallenging. Diseases 2025, 13, 223. https://doi.org/10.3390/diseases13070223
Bekkai L, Ibn Majah A, Verset L, Jacobs L, Danneel C, Elkilic O, Collart F, Nortier J, Taghavi M. Atypical Rapid Onset of Olmesartan-Induced Enteropathy with Recurrence After Rechallenging. Diseases. 2025; 13(7):223. https://doi.org/10.3390/diseases13070223
Chicago/Turabian StyleBekkai, Lila, Aymen Ibn Majah, Laurine Verset, Lucas Jacobs, Charline Danneel, Okyay Elkilic, Frédéric Collart, Joëlle Nortier, and Maxime Taghavi. 2025. "Atypical Rapid Onset of Olmesartan-Induced Enteropathy with Recurrence After Rechallenging" Diseases 13, no. 7: 223. https://doi.org/10.3390/diseases13070223
APA StyleBekkai, L., Ibn Majah, A., Verset, L., Jacobs, L., Danneel, C., Elkilic, O., Collart, F., Nortier, J., & Taghavi, M. (2025). Atypical Rapid Onset of Olmesartan-Induced Enteropathy with Recurrence After Rechallenging. Diseases, 13(7), 223. https://doi.org/10.3390/diseases13070223