
Clinical Heterogeneity of Early-Onset Autoimmune Gastritis: From the Evidence to a Pediatric Tailored Algorithm

 ,
,  ,
,  , , , ,
, , , ,
Abstract
1. Introduction
2. Methods
3. Clinical Case Description
3.1. Case 1
3.2. Case 2
4. Evidence from the Literature Review
5. Discussion
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Adamu, M.A.; Weck, M.N.; Gao, L.; Brenner, H. Incidence of chronic atrophic gastritis: Systematic review and meta-analysis of follow-up studies. Eur. J. Epidemiol. 2010, 25, 439–448. [Google Scholar] [CrossRef] [PubMed]
- Saglietti, C.; Sciarra, A.; Abdelrahman, K.; Schneider, V.; Karpate, A.; Nydegger, A.; Sempoux, C. Autoimmune Gastritis in the Pediatric Age: An Underestimated Condition Report of Two Cases and Review. Front. Pediatr. 2018, 6, 123. [Google Scholar] [CrossRef]
- Neumann, W.L.; Coss, E.; Rugge, M.; Genta, R.M. Autoimmune atrophic gastritis—Pathogenesis, pathology, and management. Nat. Rev. Gastroenterol. Hepatol. 2013, 10, 529–541. [Google Scholar] [CrossRef] [PubMed]
- Lenti, M.V.; Facciotti, F.; Miceli, E.; Vanoli, A.; Fornasa, G.; Lahner, E.; Spadoni, I.; Giuffrida, P.; Arpa, G.; Pasini, A.; et al. Mucosal Overexpression of Thymic Stromal Lymphopoietin and Proinflammatory Cytokines in Patients with Autoimmune Atrophic Gastritis. Clin. Transl. Gastroenterol. 2022, 13, e00510. [Google Scholar] [CrossRef]
- Lenti, M.V.; Rossi, C.M.; Melazzini, F.; Gastaldi, M.; Bugatti, S.; Rotondi, M.; Bianchi, P.I.; Gentile, A.; Chiovato, L.; Montecucco, C.; et al. Seronegative autoimmune diseases: A challenging diagnosis. Autoimmun. Rev. 2022, 21, 103143. [Google Scholar] [CrossRef]
- Toh, B.H.; van Driel, I.R.; Gleeson, P.A. Pernicious Anemia. N. Engl. J. Med. 1997, 337, 1441–1448. [Google Scholar] [CrossRef]
- Taylor, K.B.; Roitt, I.M.; Doniach, D.; Couchman, K.G.; Shapland, C. Autoimmune Phenomena in Pernicious Anaemia: Gastric Antibodies. Br. Med. J. 1962, 2, 1347–1352. [Google Scholar] [CrossRef]
- Taylor, K.B. Inhibition of intrinsic factor by pernicious anæmia sera. Lancet 1959, 2, 106–108. [Google Scholar] [CrossRef] [PubMed]
- Faller, G.; Kirchner, T. Immunological and morphogenic basis of gastric mucosa atrophy and metaplasia. Virchows Arch. 2005, 446, 1–9. [Google Scholar] [CrossRef]
- Hogan, T.V.; Ang, D.K.Y.; Gleeson, P.A.; van Driel, I.R. Extrathymic mechanisms of T cell tolerance: Lessons from autoimmune gastritis. J. Autoimmun. 2008, 31, 268–273. [Google Scholar] [CrossRef]
- Lehy, T.; Roucayrol, A.M.; Mignon, M. Histomorphological characteristics of gastric mucosa in patients with Zollinger-Ellison syndrome or autoimmune gastric atrophy: Role of gastrin and atrophying gastritis. Microsc. Res. Tech. 2000, 48, 327–338. [Google Scholar] [CrossRef]
- Gonçalves, C.; Oliveira, M.E.; Palha, A.M.; Ferrão, A.; Morais, A.; Lopes, A.I. Autoimmune gastritis presenting as iron deficiency anemia in childhood. World J. Gastroenterol. 2014, 20, 15780–15786. [Google Scholar] [CrossRef] [PubMed]
- Mitsinikos, T.; Shillingford, N.; Cynamon, H.; Bhardwaj, V. Autoimmune Gastritis in Pediatrics: A Review of 3 Cases. J. Pediatr. Gastroenterol. Nutr. 2020, 70, 252–257. [Google Scholar] [CrossRef]
- Segni, M.; Borrelli, O.; Pucarelli, I.; Delle Fave, G.; Pasquino, A.M.; Annibale, B. Early manifestations of gastric autoimmunity in patients with juvenile autoimmune thyroid diseases. J. Clin. Endocrinol. Metab. 2004, 89, 4944–4948. [Google Scholar] [CrossRef]
- Lahner, E.; Zagari, R.M.; Zullo, A.; Di Sabatino, A.; Meggio, A.; Cesaro, P.; Lenti, M.V.; Annibale, B.; Corazza, G.R. Chronic atrophic gastritis: Natural history, diagnosis and therapeutic management. A position paper by the Italian Society of Hospital Gastroenterologists and Digestive Endoscopists [AIGO], the Italian Society of Digestive Endoscopy [SIED], the Italian Society of Gastroenterology [SIGE], and the Italian Society of Internal Medicine [SIMI]. Dig. Liver Dis. 2019, 51, 1621–1632. [Google Scholar] [CrossRef] [PubMed]
- Miguel, N.; Costa, E.; Santalha, M., Jr.; Lima, R.; Vizcaino, J.R.; Pereira, F.; Barbot, J. Refractory iron-deficiency anemia and autoimmune atrophic gastritis in pediatric age group: Analysis of 8 clinical cases. J. Pediatr. Hematol. Oncol. 2014, 36, 134–139. [Google Scholar] [CrossRef]
- Moreira-Silva, H.; Silva, G.; Costa, E.; Guerra, I.; Santos-Silva, E.; Tavares, M.; Cleto, E.; Lima, R. Insights into Pediatric Autoimmune Gastritis: Is There a Role for Helicobacter pylori Infection? J. Pediatr. Gastroenterol. Nutr. 2019, 68, e99–e104. [Google Scholar] [CrossRef]
- Kirsaclioglu, C.T.; Kuloglu, Z.; Kansu, A.; Ensari, A.; Siklar, Z.; Berberoğlu, M.; Ocal, G. Gastric carcinoid tumor in a 14-year-old girl. Scand. J. Gastroenterol. 2014, 49, 1391–1393. [Google Scholar] [CrossRef]
- Katz, S.; Berernheim, J.; Kaufman, Z.; Lazar, L.; Erez, I.; Wolach, B. Pernicious anemia and adenocarcinoma of the stomach in an adolescent: Clinical presentation and histopathology. J. Pediatr. Surg. 1997, 32, 1384–1385. [Google Scholar] [CrossRef]
- Greenwood, D.L.; Crock, P.; Braye, S.; Davidson, P.; Sentry, J.W. Autoimmune gastritis and parietal cell reactivity in two children with abnormal intestinal permeability. Eur. J. Pediatr. 2008, 167, 917–925. [Google Scholar] [CrossRef]
- Fröhlich-Reiterer, E.E.; Huber, J.; Katz, H.; Suppan, E.; Obermayer-Pietsch, B.; Deutschmann, A.; Demel, U.; Acham-Roschitz, B.; Weinhandl, G.; Ambros-Rudolph, C.M.; et al. Do children and adolescents with type 1 diabetes mellitus have a higher frequency of parietal cell antibodies than healthy controls? J. Pediatr. Gastroenterol. Nutr. 2011, 52, 558–562. [Google Scholar] [CrossRef] [PubMed]
- Russell, A.C.; Black, J.O.; Schwartz, D.A.; Correa, H.; Rosen, M.J. 15-year-old Girl with Metaplastic Atrophic Gastritis and Enterochromaffin-like Cell Hyperplasia. J. Pediatr. Gastroenterol. Nutr. 2012, 55, e148–e151. [Google Scholar] [CrossRef]
- Pogoriler, J.; Kamin, D.; Goldsmith, J.D. Pediatric non-Helicobacter pylori atrophic gastritis: A case series. Am. J. Surg. Pathol. 2015, 39, 786–792. [Google Scholar] [CrossRef]
- Koca, T.; Dereci, S.; Karahan, N.; Akcam, M. Gastrointestinal Neuroendocrine Tumors in Two Children. Indian. Pediatr. 2016, 53, 70–72. [Google Scholar]
- Besançon, A.; Michaud, B.; Beltrand, J.; Goncalves, T.; Jais, J.P.; Polak, M.; Chatenoud, L.; Robert, J.J. Revisiting autoimmune gastritis in children and adolescents with type 1 diabetes. Pediatr. Diabetes 2017, 18, 772–776. [Google Scholar] [CrossRef]
- Calcaterra, V.; Montalbano, C.; Miceli, E.; Luinetti, O.; Albertini, R.; Vinci, F.; Regalbuto, C.; Larizza, D. Anti-gastric parietal cell antibodies for autoimmune gastritis screening in juvenile autoimmune thyroid disease. J. Endocrinol. Investig. 2020, 43, 81–86. [Google Scholar] [CrossRef] [PubMed]
- Kulak, O.; Gurram, B.; Montgomery, E.A.; Park, J.Y. Pediatric autoimmune gastritis: Clinical correlates and histologic features. Hum. Pathol. 2021, 116, 31–38. [Google Scholar] [CrossRef] [PubMed]
- Granot, M.; Beinvogl, B.C.; Schvimer, M.; Goldsmith, J.D.; Matar, M.; Ben Tov, A.; Feler, A.Y.; Nachum, N.; Morgenstern, S.; Mayer, C.; et al. Clinical characteristics and outcomes of pediatric patients with autoimmune gastritis. J. Pediatr. Gastroenterol. Nutr. 2024, 79, 501–509. [Google Scholar] [CrossRef] [PubMed]
- Demir, A.M.; Berberoğlu Ateş, B.; Hızal, G.; Yaman, A.; Tuna Kırsaçlıoğlu, C.; Oğuz, A.S.; Karakuş, E.; Yaralı, N.; Özbek, N.Y. Autoimmune atrophic gastritis: The role of Helicobacter pylori infection in children. Helicobacter 2020, 25, e12716. [Google Scholar] [CrossRef]
- Conti, L.; Lenti, M.V.; Di Sabatino, A.; Miceli, E.; Galli, G.; Cazzato, M.; Falangone, F.; Annibale, B.; Lahner, E. Seronegative autoimmune atrophic gastritis is more common in elderly patients. Dig. Liver Dis. 2020, 52, 1310–1314. [Google Scholar] [CrossRef]
- Daniels, J.A.; Lederman, H.M.; Maitra, A.; Montgomery, E.A. Gastrointestinal Tract Pathology in Patients with Common Variable Immunodeficiency (CVID): A Clinicopathologic Study and Review. Am. J. Surg. Pathol. 2007, 31, 1800–1812. [Google Scholar] [CrossRef] [PubMed]
- Rugge, M.; Genta, R.M.; Malfertheiner, P.; Dinis-Ribeiro, M.; El-Serag, H.; Graham, D.Y.; Kuipers, E.J.; Leung, W.K.; Park, J.Y.; Rokkas, T.; et al. RE.GA.IN.: The Real-world Gastritis Initiative-updating the updates. Gut 2024, 73, 407–441. [Google Scholar] [CrossRef] [PubMed]
- Samuelsson, J.; Bertilsson, R.; Bülow, E.; Carlsson, S.; Åkesson, S.; Eliasson, B.; Hanas, R.; Åkesson, K. Autoimmune comorbidity in type 1 diabetes and its association with metabolic control and mortality risk in young people: A population-based study. Diabetologia 2024, 67, 679–689. [Google Scholar] [CrossRef] [PubMed]
- Ayaki, M.; Manabe, N.; Fujita, M.; Nakamura, J.; Sunago, A.; Kamada, T.; Haruma, K. A case of eosinophilic esophagitis with autoimmune polyendocrine syndrome type 2, including autoimmune gastritis. Clin. J. Gastroenterol. 2021, 14, 460–465. [Google Scholar] [CrossRef]
- Srivastava, A.; Lauwers, G.Y. Pathology of non-infective gastritis. Histopathology 2007, 50, 15–29. [Google Scholar] [CrossRef]
- Miceli, E.; Lenti, M.V.; Gentile, A.; Gambini, G.; Petrucci, C.; Pitotti, L.; Mengoli, C.; Di Stefano, M.; Vanoli, A.; Luinetti, O.; et al. Long-Term Natural History of Autoimmune Gastritis: Results from a Prospective Monocentric Series. Am. J. Gastroenterol. 2024, 119, 837–845. [Google Scholar] [CrossRef]
- Rugge, M.; Fassan, M.; Pizzi, M.; Graham, D.Y. Letter: Gastric cancer and pernicious anaemia--often Helicobacter pylori in disguise. Aliment. Pharmacol. Ther. 2013, 37, 764–765. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| CASE 1 | Main Findings |
|---|---|
| Symptoms | Asthenia and weight loss. Severe IDA. |
| Laboratory findings | Hb 7 g/dL †, MCV 59.1 fl †, transferrin saturation 1% †, ferritin 1 ng/mL †. Vit. B12 serum levels: 266 pg/mL; folate serum levels: 8.10 ng/mL. IgA 56 mg/dL †, IgG 348 mg/dL †, IgM 66 mg/dL, IgG1 287.3 mg/dL †, IgG2 83 mg/dL †, IgG3 21.5 mg/dL, IgG4 50.2 mg/dL. CD3+ cells 1751/mm3, CD4+ 1.009/mm3, CD8+ 536/mm3, CD19+ 185/mm3 †. Anti-HBsAg: 24.4 mIU/mL (presence of immunity); IgG anti-measles: 144 AU/mL presence of immunity); IgG anti-tetanus: 0.440 IU (vaccine protection); IgG anti-diphtheria: 0.142 IU (vaccine protection). ANA: < 1:80; ENA test: negative; ASCA: IgA 0.4 IU/mL, IgG 0.6 IU/mL. ANCA: IIF < 1:20; anti-MPO: 0.2 IU/mL, anti-PR3: 0.2 IU/mL. anti-TPO: 13.1 mIU/mL, anti-TG: <20 mIU/, ATTA-reflex test: negative. APCA: < 1:40. Anti-IF: not present. Anti-insulin ab: 1.6 IU/mL; anti-pancreatic islet ab: <1:4 IU/mL. H. pylori fecal antigen: negative. Fecal occult blood test: positive. Fecal calprotectin: 144.7 mg/kg † (0–50 mg/kg). Stool culture for BK: negative. IGRA: negative. Ab anti-Strongyloides (ELISA): negative. Ab anti-Toxocara (ELISA and Immunoblotting): negative. Ab anti-Trichinella (immunoblotting): negative. Ova and parasite stool exam: negative. Graham test: negative. |
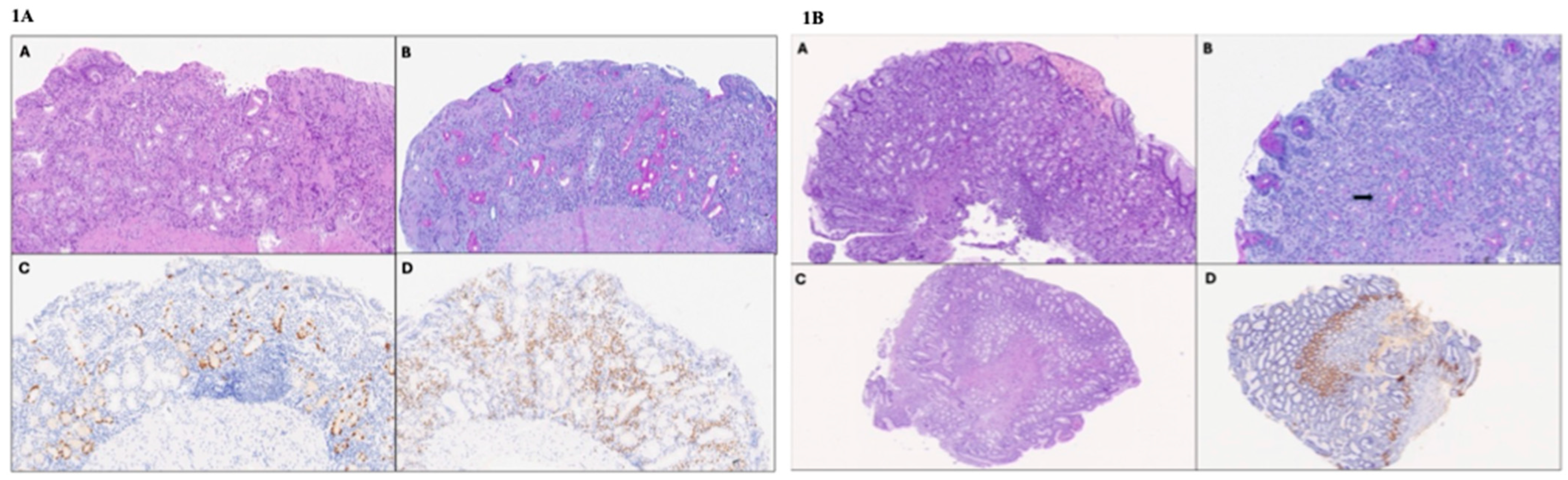
| Endoscopy and histological findings | Diffuse atrophic gastric mucosa without the normal folds. Antral gastric mucosa with mild chronic inflammation, and severe atrophy of the oxyntic mucosa with sclerosis, pseudo-pyloric metaplasia, and simple and linear hyperplasia of ECL cells. Nodular lymphoid hypertrophy of the last tract of the ileum. VCE: diffuse inflammation of the small intestine with epithelial erosion, multiple vascular ectasias, and blood vessel fragility. |
| Treatment | Iron and vitamin B12 supplementation. |
| CASE 2 | Main findings |
| Symptoms | Incidental finding during upper GI endoscopy for PPI non-responsive nausea, dyspepsia, heartburn, and severe food impaction episodes. |
| Laboratory findings | Hb 12.5 g/dL, MCV 82.9 fl, transferrin saturation 14%, ferritin 18.8 ng/mL. Vitamin B12 serum levels: 381 pg/mL; folate serum levels: 6.20 ng/mL. IgA 226 mg/dL, IgG 1115 mg/dL, IgM 136 mg/dL, IgG1 566.3 mg/dL, IgG2 285.3 mg/dL, IgG3 96.9 mg/dL, IgG4 19.9 mg/dL. APCA: 1:320 †. Anti-IF: not present. ANA: <1:80; ENA screening test: negative; anti-TPO: 13.1 mIU/, anti-TG: 20 mIU/mL, ATTA-reflex test: negative. Gastrin: 15.2 pg/mL [<108 pg/mL]. Chromogranin A: 100 ng/mL [19.4–98 ng/mL]. H. pylori fecal antigen: negative. |
| Endoscopy and histological findings | Regular esophageal mucosa and hyperemic gastric antral mucosa. Esophagus: intraepithelial eosinophilic granulocytes (>100 eos/hpf). Giemsa-stained special coloration for H. pylori and immunohistochemical staining with anti-H. pylori search negative. |
| Treatment | Topical corticosteroid (swallowed fluticasone; starting dose 875 μg/die with progressive decalage) |
| Author, Year | Type of Study | N°, Sex | Mean Age at the Diagnosis | Comorbidities | Iron Deficiency | B12 Deficiency | Hyper-Gastrinemia | APCA | Anti-IF | Macroscopic and Histologic Findings | HP Infection | Metaplasia | ECL Cell Hyperplasia | Therapy |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Katz et al., 1997 [19] | Case report | M | 15 | No | Yes | Yes | / | / | / | Atrophic gastric mucosa with antrum polyp. CSP | / | Yes (intestinal). Adenoma and poorly differentiated adenocarcinoma. | No | Oral iron supplementation + IM vitamin B12 Surgery. |
| Segni et al., 2004 [14] | Case series | 7 F (2) M (5) | 13 | CLT (5/7), GD (2/7), T1DM (1/7) | / | / | Yes (6/7) | + (7/7) | / | CSP (3/7), CPAG (4/7) | Yes (4/7) | / | / | / |
| Greenwood et al., 2008 [20] | Case series | 2 M (1) F (1) | 8.5 | AD (1/2), CLT (2/2), and alopecia (1/2). | Yes (2/2) | Yes (1/2) | Yes (1/2) | + (2/2) | + (1/2) | Mucosal erythema (1/2). Gland distortion and nodular lymphoid aggregate (1/2). Chronic inflammatory cell infiltration (lymphocytes with occasional PC and Eos) (1/2). | No (2/2) | Yes (intestinal) (1/2) | No | Oral iron and vitamin B12 supplementation (2/2) |
| Frohlich-Reiterer et al., 2011 [21] | Cross-sectional | 3 F (3/3) | 15.7 | T1DM (3/3), CLT (3/3) | Yes (3/3) | No | Yes (2/3) | + (3/3) | / (3/3) | Mild atrophic gastritis (1/3); mild CSP (2/3). | Yes (2/3) | No (3/3) | No (3/3) | / |
| Russell et al., 2012 [22] | Case report | F | 15 | No | No | No | / | - | - | Macroscopic nodules. Multifocal atrophic gastritis. | No | Yes (focal, intestinal) | Yes | / |
| Gonçalves et al., 2014 [12] | Case series | 5 M (2) F (3) | 13.6 | T1DM (1/5), CLT (1/5) | Yes (5/5) | No (3/5); / (2/5) | Yes (3/5) | + (5/5) | / (5/5) | Fold softening (2/5). CPAG [5/5; mild (1/5), moderate to severe (4/5)]. | No | Yes [4/5; intestinal (1/5); pseudopyloric (3/5)] | Yes
| / |
| Pogoriler et al., 2015 [23] | Case series | 12 M (6) F (6) | 11.6 | T1DM (4/12), AI hepatitis (1/12), AI cytopenia (2/12), CeD (1/12), CLT (2/12), CVID (1/12), T-cell PID (1/12) | Yes (6/12) | Yes (1/9); / (3/12) | Yes (2/2); / (10/12) | + (3/7) *; / (5/12). | + (2/5); / (7/12) | Not specific (12/12). Chronic inflammation:
| No | Yes [8/12; intestinal (3/8); pseudopyloric (4/8); squamous-mucinous (1/8)]. One patient developed gastric adenocarcinoma. | Yes (5/12) | / |
| Kirsaclioglu et al., 2014 [18] | Case report | F | 14 | No | Yes | / | Yes | + | / | Corpus polyp. Chronic atrophic gastritis. | / | Yes (intestinal) | Type 1 GCT | EMR |
| Miguel et al., 2014 [16] | Case series | 8 M (2) F (6) | 12.3 | ANA positivity (1/8) | Yes (8/8) | No (5/5); / (3/8) | Yes (8/8) | + (8/8) | / (8/8) | Chronic atrophic gastritis:
| Yes (4/8) | Yes [1/8 (intestinal)] | / (8/8) | Oral iron supplementation (8/8) |
| Koca et al., 2016 [24] | Case report | F | 15 | No | / | / | Yes | + | / | Nodules. Multifocal atrophic gastritis | Yes | Yes (intestinal) | Yes | / |
| Besançon et al., 2017 [25] | Case series | 2 M (1), F (1) | 12 | T1DM (2/2), CLT (1/2), | Yes (1/2) | / | / | + (2/2) | / | Chronic lymphocytic gastritis of the fundus (1/2). Gastritis of the antrum and fundus (1/2). | Yes (1/2) | / | / | Oral iron supplementation |
| Saglietti et al., 2018 [2] | Case series | 2 F (2/2) | 14.5 | No | Yes (2/2) | Yes (1/2); / (1/2) | / (2/2) | + (2/2) | / (2/2) | Normal aspect (2/2). Multifocal atrophic gastritis (2/2). | No | Yes (2/2) Intestinal (1/2) Pseudopyloric (1/2) | Yes (2/2) | / |
| Moreira-Silva et al., 2019 [17] | Case series | 20 M (9) F (11) | 12.3 | CLT (5/20), T1DM (4/20), CeD (1/20), ITP (1/20), FSGS (1/20), IgAGN (1/20) | Yes (18/20) | / (20/20) | Yes (19/20) | + (20/20) | / (20/20) | Chronic inflammation of the gastric mucosa in the corpus | Yes (11/20) | Yes (4/20, intestinal) | / | / |
| Calcaterra et al., 2020 [26] | Single-center retrospective study | 1 (F) | 16 | CLT | Yes | No | No | + | / | Foveolar hyperplasia | No | / | / | / |
| Mitsinikos et al., 2020 [13] | Case series | 3 F (3/3) | 14 | T1DM (2/3), AD (1/3), CLT (1/3), crescentic GN (1/3). | Yes (3/3) | Yes (1 */3) * pancytopenia | Yes (1/3) | + (3/3) | + (1/3) | Normal aspect (1/3), linear furrowing (1/3), erythema (1/3). Oxyntic mucosa mononuclear cells infiltration and gland damage, and decreased parietal cell mass (3/3) | No | Yes [2/3: pseudopyloric (1/2), intestinal (1/2)]. | Yes [2/3: Linear (2/3)]. | Oral iron (2/3) and vitamin B12 supplementation (1/3). |
| Demir et al., 2020 [29] | Single-center retrospective-observational study | 10 F (4) M (6) | 15 | CLT (1/10), CeD (1/10) | Yes (5/10) | / | / | + (10/10) | / | Hyperemic gastric corpus (5/10) or antrum (5/10). Gastric inflammation (7/10) | No | Yes (4/10, intestinal) | Yes (1/10) | / |
| Kulak et al., 2021 [27] | Single-center retrospective study | 22 F (15) M (7) | 10.9 | CLT (3/22), GD (2/22), T1DM (3/22), CVID and IPEX (1/22), IgA deficiency (1/22), AI hepatitis (1/22), CeD (1/22), Crohn’s disease (1/22), JIA (1/22) | Yes (4/22) | Yes (1/22) | Yes (8/10 tested) | + (6/12 tested) | + (0/7 tested) | CPAG (22/22), antral atrophy (4/22) | Yes (3/5 tested) | Yes [4/22: pseudopyloric (3/4), intestinal (1/4)] | Yes (22/22) | / |
| Granot et al., 2024 [28] | Multicenter retrospective study | 33 F (23) M (10) | 12 [median; IQR 7.0–15.1] | CeD (3/33), AITD (6/33), T1DM (4/33), AI hepatitis (2/33), AD (1/33) | Yes (25/33) | Yes (2/33) | Yes (23/27 tested) | + (16/33) | + (6/33) | Active inflammation: gastric body (5/28 tested), gastric antrum (19/31); Chronic inflammation: gastric body (18/30 tested), gastric antrum (27/28); | Yes (1/33) | Yes (8/32 gastric antrum: Pseudo pyloric 5/8; intestinal 1/8; both 2/8) | Yes (20/34) | Iron supplementation: oral (17/33) and IV (6/33); vit. B12 oral supplementation (5/33) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Taietti, I.; Votto, M.; Castagnoli, R.; Bertozzi, M.; De Filippo, M.; Di Sabatino, A.; Luinetti, O.; Raffaele, A.; Vanoli, A.; Lenti, M.V.; et al. Clinical Heterogeneity of Early-Onset Autoimmune Gastritis: From the Evidence to a Pediatric Tailored Algorithm. Diseases 2025, 13, 133. https://doi.org/10.3390/diseases13050133
Taietti I, Votto M, Castagnoli R, Bertozzi M, De Filippo M, Di Sabatino A, Luinetti O, Raffaele A, Vanoli A, Lenti MV, et al. Clinical Heterogeneity of Early-Onset Autoimmune Gastritis: From the Evidence to a Pediatric Tailored Algorithm. Diseases. 2025; 13(5):133. https://doi.org/10.3390/diseases13050133
Chicago/Turabian StyleTaietti, Ivan, Martina Votto, Riccardo Castagnoli, Mirko Bertozzi, Maria De Filippo, Antonio Di Sabatino, Ombretta Luinetti, Alessandro Raffaele, Alessandro Vanoli, Marco Vincenzo Lenti, and et al. 2025. "Clinical Heterogeneity of Early-Onset Autoimmune Gastritis: From the Evidence to a Pediatric Tailored Algorithm" Diseases 13, no. 5: 133. https://doi.org/10.3390/diseases13050133
APA StyleTaietti, I., Votto, M., Castagnoli, R., Bertozzi, M., De Filippo, M., Di Sabatino, A., Luinetti, O., Raffaele, A., Vanoli, A., Lenti, M. V., Marseglia, G. L., & Licari, A. (2025). Clinical Heterogeneity of Early-Onset Autoimmune Gastritis: From the Evidence to a Pediatric Tailored Algorithm. Diseases, 13(5), 133. https://doi.org/10.3390/diseases13050133