
Developing Complexity-Informed COVID-19 Responses to Optimize Community Well-Being: A Systems Thinking Approach


Abstract
:1. Introduction
“cause and effect are subtle, and where the effects over time of interventions are not obvious…. When the same action has dramatically different effects in the short run and the long run, there is dynamic complexity. When an action has one set of consequences locally and a different set of consequences in another part of the system, there is dynamic complexity. When obvious interventions produce non-obvious consequences, there is dynamic complexity.”[8] (p. 71)
Description of Setting
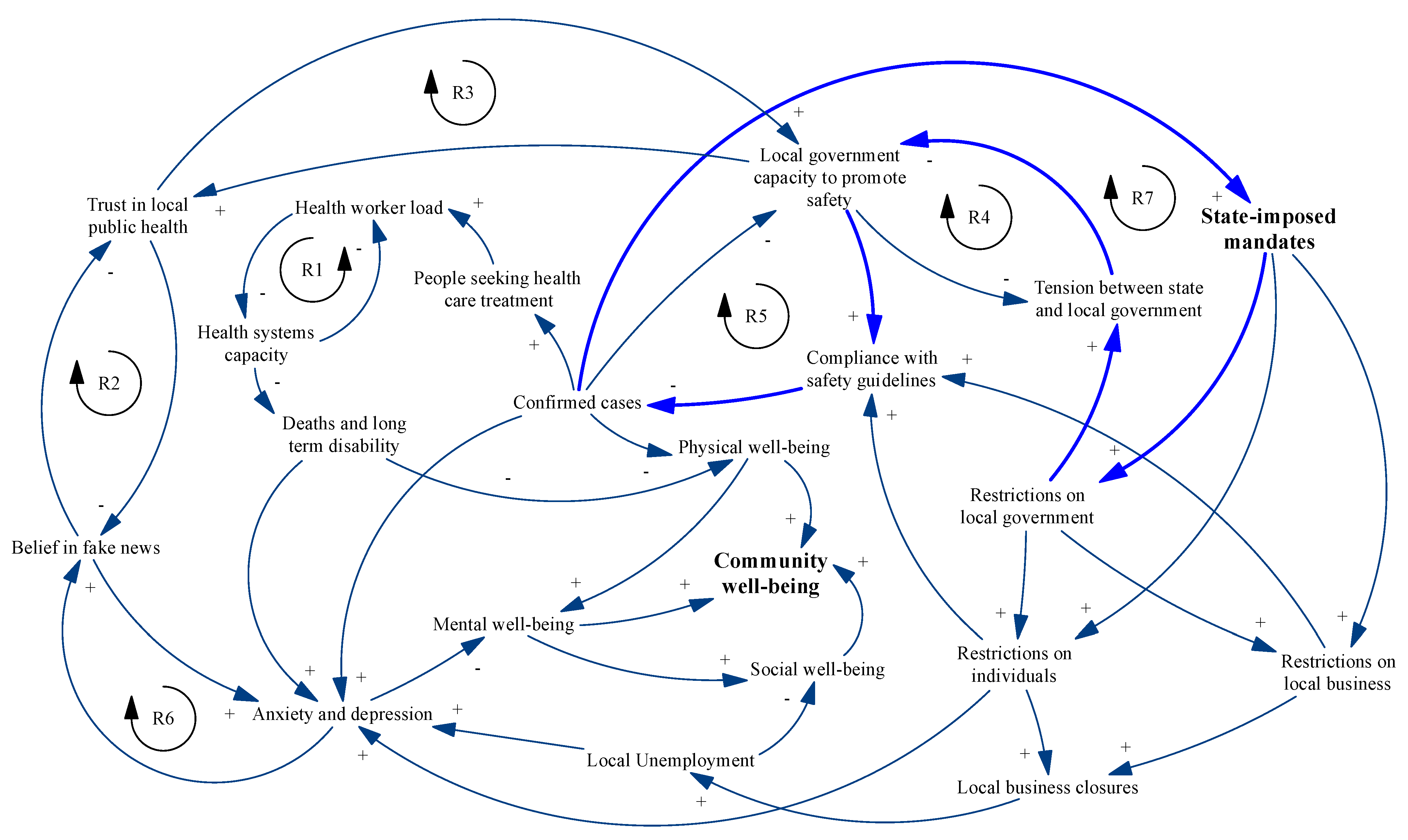
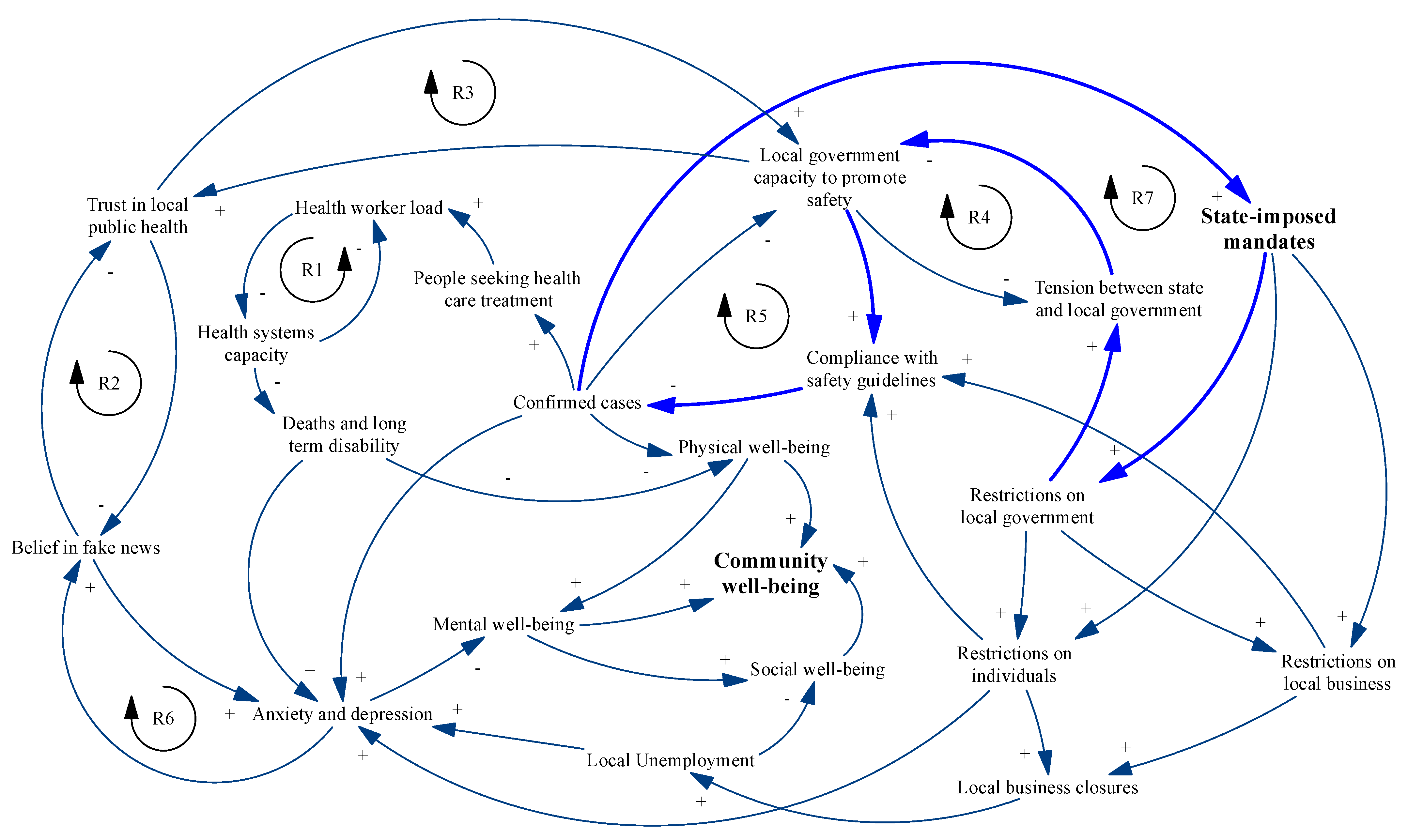
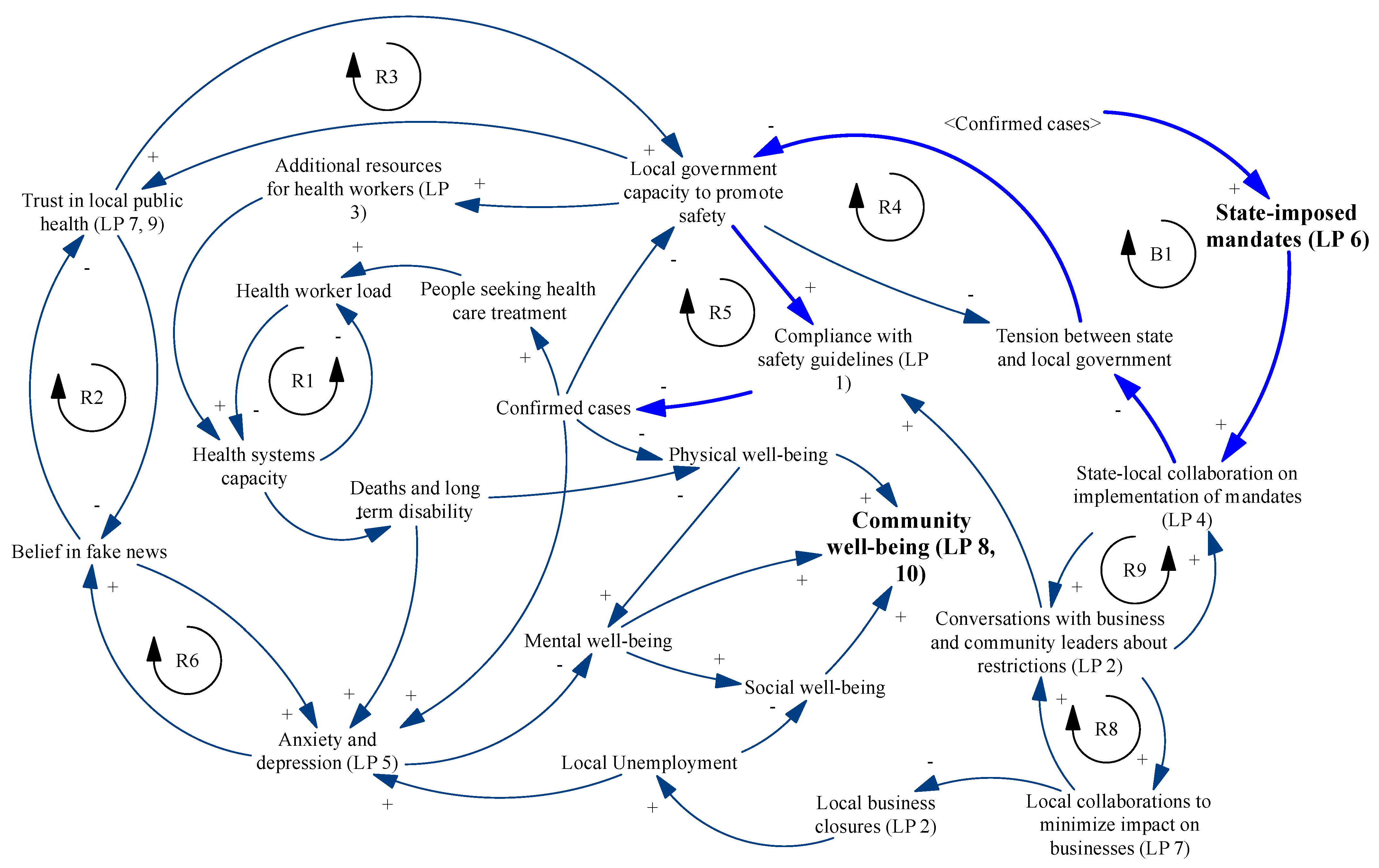
2. County-Level COVID-19 Dynamics
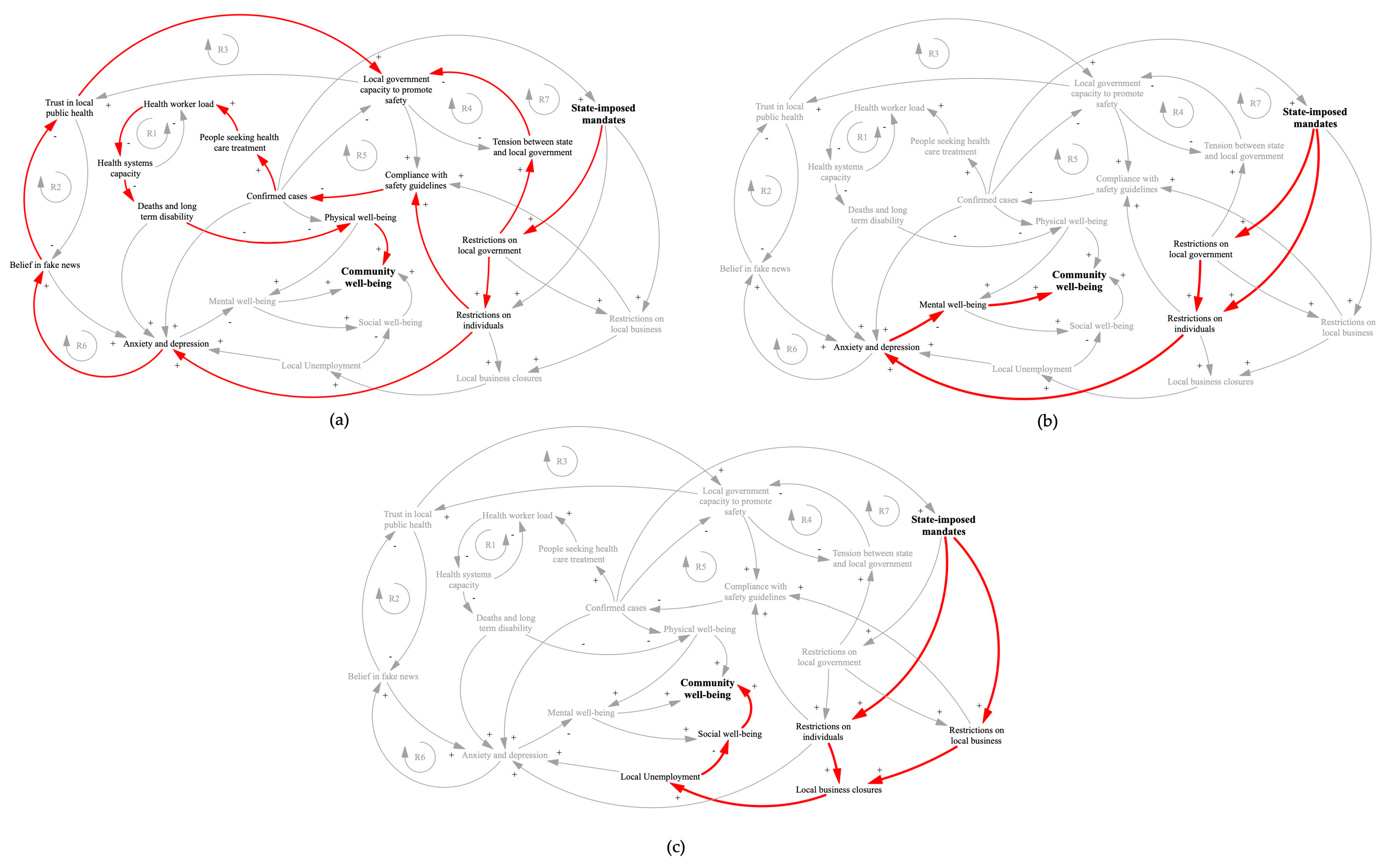
2.1. Impact of State Mandates on Community Physical Well-Being
2.2. Impact of State Mandates on Community Mental Well-Being
2.3. Impact of State Mandates on Community Social Well-Being
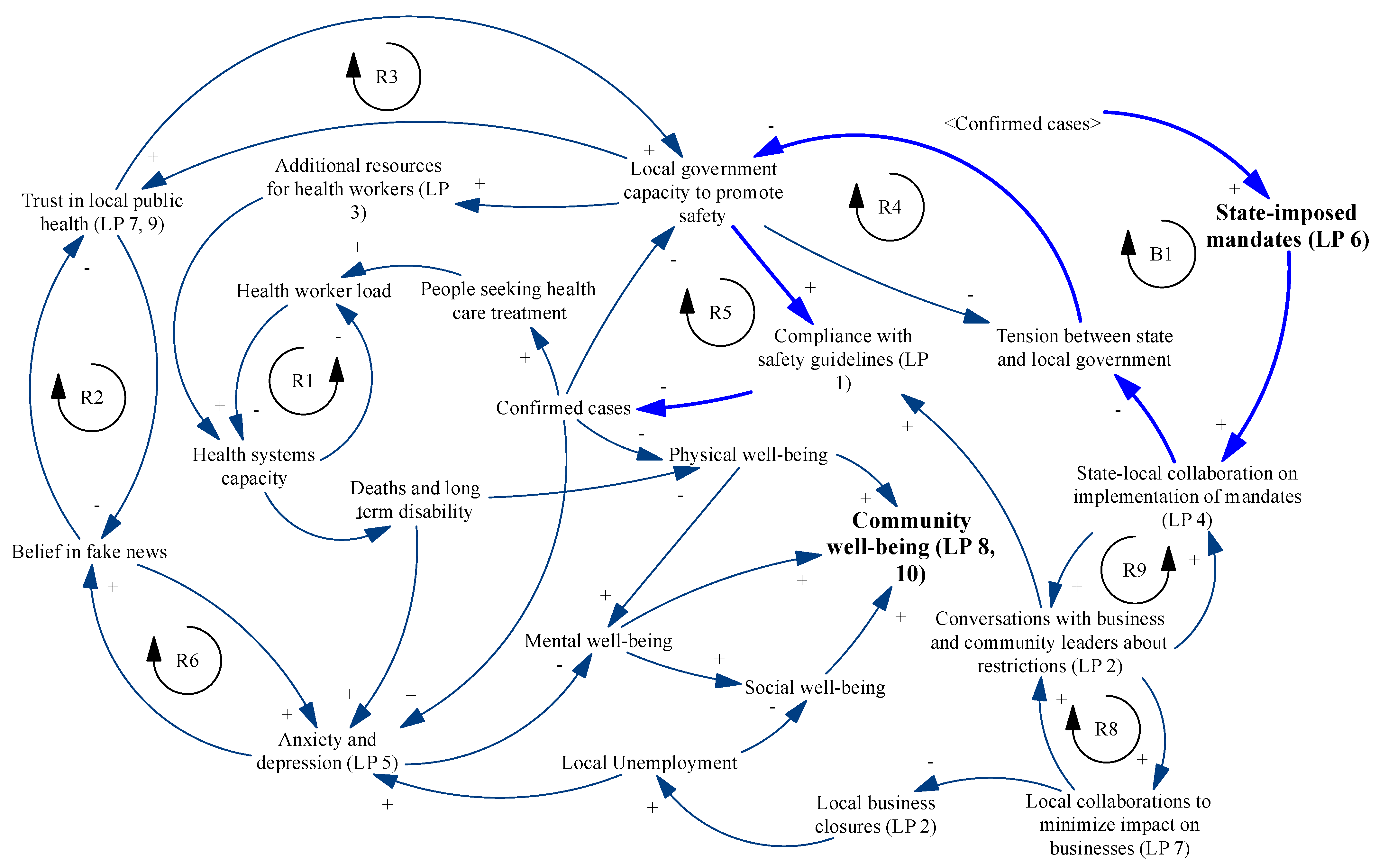
3. Changing the Dynamics: Identifying Leverage Points
4. Using Leverage Points to Transform the System: A Thought Experiment
4.1. Increasing Collaboration between State and Local Leaders
4.2. Increasing Local Multi-Stakeholder Community Partnerships
5. Conclusions: A Call to Action
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Center for Systems Science Engineering at Johns Hopkins University. COVID-19 Dashboard. Available online: https://coronavirus.jhu.edu/map.html (accessed on 1 July 2021).
- Engler, J.O.; Abson, D.J.; von Wehrden, H. The coronavirus pandemic as an analogy for future sustainability challenges. Sustain. Sci. 2021, 16, 317–319. [Google Scholar] [CrossRef] [PubMed]
- Qualls, N.; Levitt, A.; Kanade, N.; Wright-Jegede, N.; Dopson, S.; Biggerstaff, M.; Reed, C.; Uzicanin, A. Community Mitigation Guidelines to Prevent Pandemic Influenza: United States; Center for Surveillance, Epidemiology, and Laboratory Services, Centers for Disease Control and Prevention, U.S. Department of Health and Human Services: Atlanta, GA, USA, 2017.
- Hatchett, R.J.; Mecher, C.E.; Lipsitch, M. Public health interventions and epidemic intensity during the 1918 influenza pandemic. Proc. Natl. Acad. Sci. USA 2007, 104, 7582–7587. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Markel, H.; Lipman, H.B.; Navarro, A. Nonpharmaceutical interventions implemented by US cities during the 1918-1919 influenza pandemic. JAMA 2007, 298, 644–654. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ferguson, N.M.; Cummings, D.A.; Fraser, C.; Cajka, J.C.; Cooley, P.C.; Burke, D.S. Strategies for mitigating an influenza pandemic. Nature 2006, 442, 448–452. [Google Scholar] [CrossRef] [PubMed]
- Institute of Medicine. Modeling Community Containment for Pandemic Influenza: A Letter Report; Report No.: 978-0-309-10411-1; The National Academies Press: Washington, DC, USA, 2006. [Google Scholar]
- Senge, P.M. The Fifth Discipline: The Art and Practice of the Learning Organization; Doubleday/Currency: New York, NY, USA, 1990. [Google Scholar]
- Desmet, K.; Wacziarg, R. Understanding spatial variation in COVID-19 across the United States. Natl. Bur. Econ. Res. Work. Pap. Ser. 2020, 118. [Google Scholar] [CrossRef]
- Peters, D.H. The application of systems thinking in health: Why use systems thinking? Health Res. Policy Syst. 2014, 12, 51. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Meadows, D. Leverage Points: Places to Intervene in a System; The Sustainability Institute: Hartland, VT, USA, 1999. [Google Scholar]
- Sahin, O.; Salim, H.; Suprun, E.; Richards, R.; Macaskill, S.; Heilgeist, S.; Rutherford, S.; Stewart, R.A.; Beal, C.D. Developing a preliminary causal loop diagram for understanding the wicked complexity of the COVID-19 pandemic. Systems 2020, 8, 20. [Google Scholar] [CrossRef]
- Ratcliffe, M.; Burd, C.; Holder, K.; Fields, A. Defining Rural at the U.S. Censusu Bureau: American Community Survey and Geography Brief. 2016. Available online: https://www2.census.gov/geo/pdfs/reference/ua/Defining_Rural.pdf (accessed on 20 February 2021).
- United Statues Census Bureau. QuickFacts United States. Available online: https://www.census.gov/quickfacts/fact/table/US/PST045219 (accessed on 20 February 2021).
- United States Census Bureau. City and Town Population Tools: 2010–2019. 2020. Available online: https://www.census.gov/data/datasets/time-series/demo/popest/2010s-total-cities-and-towns.html#ds (accessed on 20 February 2021).
- United States Bureau of Labor Statistics. Quarterly Census of Employmeny and Wages. Available online: https://data.bls.gov/cew/apps/data_views/data_views.htm#tab=Tables (accessed on 27 March 2021).
- Politico. Presidental Election Results. Available online: https://www.politico.com/2020-election/results/president/ (accessed on 20 February 2021).
- United States Census Bureau. 2010 Census Urban and Rural Classification and Urban Area Criteria. Available online: https://www.census.gov/programs-surveys/geography/guidance/geo-areas/urban-rural/2010-urban-rural.html (accessed on 20 February 2021).
- Grad, F.P. The Preamble of the Constitution of the World Health Organization. Bull. World Health Organ. 2002, 80, 981–984. [Google Scholar]
- Slotnik, D.E. Mixed Virus Data Has Some Experts Questioning pace of NYC Reopening. The New York Times. 2021. Available online: https://apps.who.int/iris/bitstream/handle/10665/268691/PMC2567708.pdf?sequence=1&isAllowed=y (accessed on 20 February 2021).
- National Center for Health Statistics. Early Release of Selected Mental Health Estiamtes Based on Data from the January–June 2019 National Health Interview Survey; National Center for Health Statistics: Hyattsville, MD, USA, 2020.
- United States Census Bureau. Indicators of Anxiety or Depression Based on Reported Frequency of Symptoms during Last 7 Days. Available online: https://data.cdc.gov/NCHS/Indicators-of-Anxiety-or-Depression-Based-on-Repor/8pt5-q6wp (accessed on 27 March 2021).
- Pollack, J.; Helm, J.; Adler, D. What is the Iron Triangle, and how has it changed? Int. J. Manag. Proj. Bus. 2018, 11, 527–547. [Google Scholar] [CrossRef]
- Ehrlichman, D. Identifying Leverage Points in a System. Available online: https://medium.com/converge-perspectives/identifying-leverage-points-in-a-system-3b917f70ab13 (accessed on 1 April 2021).
- Vest, J.R.; Blackburn, J.; Yeager, V.A. Challenges in Translating National and State Reopening Plans Into Local Reopening Policies During the COVID-19 Pandemic. Public Health Rep. 2021, 136, 127–131. [Google Scholar] [CrossRef] [PubMed]
- Agrawal, V.; Cantor, J.H.; Sood, N.; Whaley, C.M. The Impact of the COVID-19 Pandemic and Policy Responses on Excess Mortality; National Bureau of Economic Research: Cambridge, MA, USA, 2021. [Google Scholar]
- Chetty, R.; Friedman, J.N.; Hendren, N.; Stepner, M.; The Opportunity Insights Team. Economic Tracker. Available online: https://tracktherecovery.org (accessed on 10 March 2021).
- Grusky, D.B.; Carenter, A.; Graves, E.; Kallschmidt, A.; Mitnik, P.; Nichols, B.; Snipp, C.M. The Rise of the Noxious Contract: Job Safety in the Covid-19 Crisis. 2021. Available online: https://inequality.stanford.edu/covid/noxious-contract (accessed on 27 March 2021).
- U.S. Census Bureau. Household Pulse Survey. Available online: https://www.cdc.gov/nchs/covid19/pulse/mental-health.htm (accessed on 28 May 2021).
- Liu, L.; Hu, T.; Bao, S.; Wu, H.; Peng, Z.; Wang, R. The Spatiotemporal Interaction Effect of COVID-19 Transmission in the United States. ISPRS Int. J. Geo-Inf. 2021, 10, 387. [Google Scholar] [CrossRef]
- Savage, A.; Brune, S.; Hovis, M.; Spencer, S.E.; Dinan, M.; Seekamp, E. Working Together: A Guide to Collaboration in Rural Revitalization; North Carolina State University: Raleigh, NC, USA, 2018. [Google Scholar]
- Roussos, S.T.; Fawcett, S.B. A review of collaborative partnerships as a strategy for improving community health. Annu. Rev. Public Health 2000, 21, 369–402. [Google Scholar] [CrossRef] [Green Version]
- Emerson, K.; Nabatchi, T.; Balogh, S. An Integrative Framework for Collaborative Governance. J. Public Adm. Res. Theory 2011, 22, 1–29. [Google Scholar] [CrossRef] [Green Version]
- Kania, J.; Kramer, M. Collective Impact. Stanford Social Innovation Review. 2011. Available online: https://ssir.org/articles/entry/collective_impact# (accessed on 26 June 2021).
- Tolentino, J. What Mutual Aid Can Do during a Pandemic. The New Yorker. 18 May 2020. Available online: https://www.newyorker.com/magazine/2020/05/18/what-mutual-aid-can-do-during-a-pandemic (accessed on 13 June 2021).

{kind=link}
{kind=link}
{kind=link}
| County | State | Country | |
|---|---|---|---|
| Rural population | 28.6% [13] | 33.9% [18] | 19.3% [18] |
| Median income [14] | $49,688 | $54,602 | $62,843 |
| Race [14] | |||
| White | 73.6% | 70.6% | 76.3% |
| Black or African American | 20.9% | 22.2% | 13.4% |
| American Indian or Alaska Native | 1.5% | 1.6% | 1.3% |
| Asian | 1.7% | 3.2% | 5.9% |
| Native Hawaiian or Other Pacific Islander | 0.1% | 0.1% | 0.2% |
| Two or more races | 2.3% | 2.3% | 2.8% |
| Education [14] | |||
| High school graduate or higher | 86.3% | 87.8% | 88.0% |
| Bachelor’s degree or higher | 24.8% | 31.3% | 32.1% |
| COVID-19 cases per 100,000 [1] | 5468 | 4257 | 5041 |
| COVID-19 case fatality rate [1] | 1.4% | 1.3% | 1.8% |
| Leverage Point | Location in Figure 1 | Descriptions | |
|---|---|---|---|
| Changes to System Infrastructure | |||
| 1 | Adding constraints | Compliance with safety guidelines | Enforcing restrictions on super spreader events |
| 2 | Changing rates | Local business closures | Reducing rates of local business closures by creating safe opportunities for businesses to interact with customers |
| 3 | Increasing buffers | Health worker load | Adding health worker resources to act as a buffer to increased patient volume |
| Modifying Information Flows | |||
| 4 | Modifying feedback loops | R7 (Figure 1) to B1 (Figure 3) | Converting “state–county tension” to “state–county collaboration” |
| 5 | Expanding communication systems | Anxiety and depression | Increasing public communication channels through faith communities, community activists, local radio stations, and other trusted networks |
| Redefining Organizing Principles | |||
| 6 | Changing the rules that govern the system | State-imposed mandates | Seeking to transfer authority for safety mandates to the county level stakeholders |
| 7 | Enhancing the organization of the system | Trust in local public health | Creating community partnerships to develop multifaceted response to COVID-19 |
| 8 | Aligning shared goals of the system | Community well-being | Acknowledging the need to simultaneously optimize physical, mental, and social well-being |
| Altering Mindsets | |||
| 9 | Modifying the beliefs that guide behaviors in the system | Trust in local public health | Building community trust in local multi-stakeholder partnerships through communication and dialogue |
| 10 | Expanding the system’s ability to transcend paradigms altogether | Community well-being | Creating opportunities for all stakeholders to engage in transparent dialogue about how to continually learn and adapt |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bogdewic, S.; Ramaswamy, R. Developing Complexity-Informed COVID-19 Responses to Optimize Community Well-Being: A Systems Thinking Approach. Systems 2021, 9, 68. https://doi.org/10.3390/systems9030068
Bogdewic S, Ramaswamy R. Developing Complexity-Informed COVID-19 Responses to Optimize Community Well-Being: A Systems Thinking Approach. Systems. 2021; 9(3):68. https://doi.org/10.3390/systems9030068
Chicago/Turabian StyleBogdewic, Stephanie, and Rohit Ramaswamy. 2021. "Developing Complexity-Informed COVID-19 Responses to Optimize Community Well-Being: A Systems Thinking Approach" Systems 9, no. 3: 68. https://doi.org/10.3390/systems9030068
APA StyleBogdewic, S., & Ramaswamy, R. (2021). Developing Complexity-Informed COVID-19 Responses to Optimize Community Well-Being: A Systems Thinking Approach. Systems, 9(3), 68. https://doi.org/10.3390/systems9030068