1. Introduction
The practice of spiritual care in health has included the goal of addressing the spiritual needs of healthcare staff. Spiritual-care practitioners have had some difficulty in fulfilling this goal, which has created the need for innovative approaches. Two approaches designed to address the spiritual and existential needs of staff are Value-Based Reflective Practice (VBRP) and Schwartz Rounds. Schwartz Rounds are a regular whole-hospital meeting where staff are invited to share and discuss the social and emotional aspects of their work. They are an evidence-based intervention to reduce psychological distress and improve staff wellbeing. This paper seeks to explore the role of spiritual-care practitioners in addressing the spiritual and existential needs of staff. It then explores the synergy of these roles with the theory and practice of the above approaches with a particular emphasis on Schwartz Rounds. The paper is grounded in the experience of the authors collaborating to establish Schwartz Rounds in a large and culturally diverse hospital, while also playing a leadership role in the establishment and sustainability of Schwartz programmes in other settings.
A letter to the editor of the
Journal of Public Health written during the Covid-19 pandemic highlighted how rarely the spiritual needs of healthcare staff are addressed, and the scarcity of literature that addresses the extent of spiritual distress experienced by staff in the course of their work. The letter emphasises that healthcare staff are expected to provide compassionate care to others at great personal cost to themselves, yet as they emptied themselves for others, the same compassionate care was not always extended to them. The letter advocated keenly for ‘multifaith/non-faith chaplaincy/spiritual-care teams’ to provide comprehensive spiritual care to health care staff, ‘particularly those struggling with decisions made and their results’ (
Sarmiento 2021). Megan Best and colleagues note that spiritual care is important not only for patients and families/caregivers but also for healthcare worker (
Jones et al. 2023).
There is a significant need for the spiritual care of healthcare staff (
Sarmiento 2021;
Best et al. 2023). Most hospital spiritual-care departments have, as a core aim, the provision of religious or spiritual care to staff, patients, and their families/caregivers (
Keogh et al. 2017). And yet, spiritual-care departments struggle to connect with healthcare staff. Several reasons for this exist, including a lack of clarity about their role with staff, their place in the hospital system and staff wellbeing services, a conflation of religious care with spiritual care, and not wanting to deprive patients of spiritual-care services (
Jones et al. 2021). A significant barrier is the difficulty in a clearly articulated definition of spiritual care and the specific skills that practitioners can provide (
Best et al. 2020).
Before moving to address the spiritual care of staff there is a need to clarify several points, which include, first, terminology; second, providing more clarity around the relationship and differentiation between spiritual and religious care; third, what spiritual care actually is and where it fits into broader models of psychosocial care; fourth, the relationship of spiritual-care practitioners to the multidisciplinary team; and last, where the discipline of spiritual care fits within institutional healthcare.
2. Relationship between Spiritual Care and Religious Care
Several overlapping and related terms are used concerning the provision of spiritual and religious care. These include chaplains, pastoral care staff, or spiritual-care providers. These people provide differing religious and spiritual-care blends, and terminology varies between healthcare providers, organisations, and traditions. This article focuses on the spiritual care aspect of the role, rather than religious care. For this reason, the terms spirituality, spiritual-care department, and spiritual-care practitioner will be used as general terms without intending to diminish the distinctions and differences between the roles and traditions.
A current working definition of spirituality developed by the European Association of Palliative Care (EAPC) in their
White Paper (
Best et al. 2020) is as follows:
Spirituality is the dynamic dimension of human life that relates to the way persons (individual and community) experience, express and/or seek meaning, purpose and transcendence, and the way they connect to the moment, to self, to others, to nature, to the significant and/or the sacred.
This definition contains religious and non-religious elements which tap directly into a considerable discussion about how the concepts of religion and spirituality relate to each other (
Barker 2004). Various views have been advanced, including seeing religiosity as a more specific expression of a broader concept of spirituality (
Cottingham 2012), and, conversely, seeing spirituality as a non-religious expression of broader categories of mystical tenets found in all major religions (
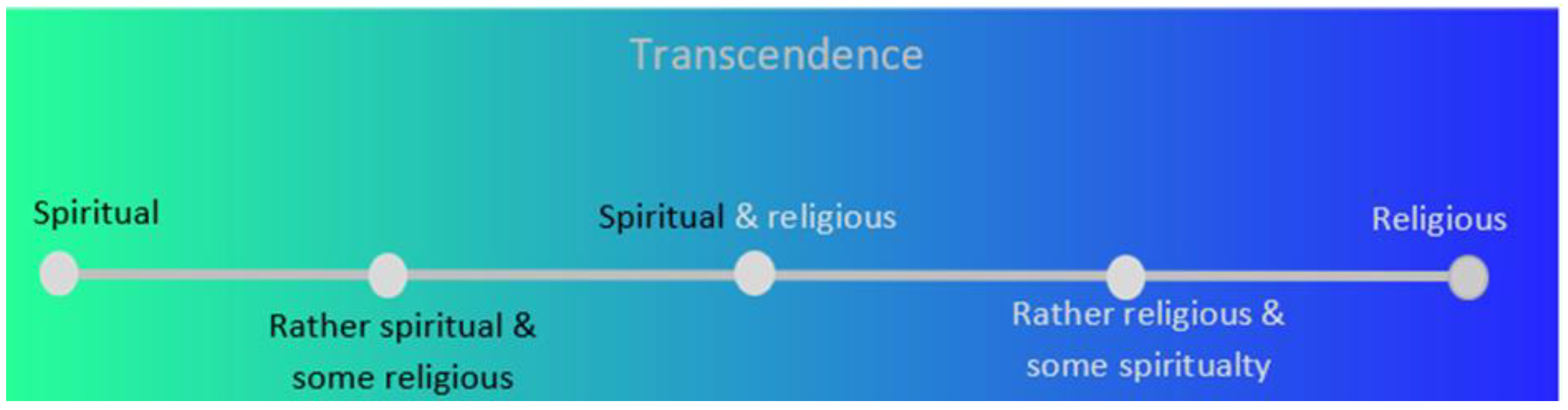
Frisk 2009). Others see the terms as broadly synonymous, while others see no congruence, and still others see the concepts as an overlapping Venn diagram. Heinz Streib and Constantin Klein offer another perspective, which neither conflates nor confuses spirituality with religion but rather places them at either end of a continuum that describes human phenomena with spiritual-but-not-religious, or existential expressions at one end and highly religious expressions at the other end. The continuum, see
Figure 1, moves from non-religious or existential spiritual positions through to a religious position connected to beliefs, institutions, and practices of a specific religious tradition with any number of more eclectic religious beliefs and religious/spiritual phenomena experienced in between. (
Streib and Klein 2016;
Jeserich et al. 2023).
3. The Practice of Spiritual Care
The provision of religious and spiritual care depends upon a similar set of insights and skills that are employed along the whole continuum. Simon Peng-Keller identified two predominant modes of providing spiritual care in chaplaincy literature (
Peng-Keller 2024):
Compassionate presence, through which connectedness, closeness, and acceptance can be experienced, and
Processes of reframing through which horizons of meaning and new life connections open up.
There is a significant overlap between providing compassionate presence and processes of reframing. Both depend on the spiritual awareness of the practitioner, (
Miller 2011) their training, and their spiritual formation. Simon Peng-Keller quotes McLaren, saying that pastoral care practitioners, similarly to psychotherapists, practise in a particular modality (
Peng-Keller 2024):
Competence in working within one’s core modality is a prerequisite for practice […] having no ‘spiritual modality’ is not an option […] a chaplain is precisely someone who has been formed within a particular wisdom tradition (Jewish, Buddhist, Sikh, Humanist, and so forth), and has developed the critical skills to be able to draw upon the resources of that tradition, and to critique its weaknesses. […] it is this rootedness in the spirituality of one or more concrete, historical, wisdom traditions that makes chaplains distinctive and constitutes their ‘unique selling point’..
When working with compassionate presence, spiritual-care practitioners provide structure and containment around what may feel like very strong emotions. Working from a basis of person-centred care, embodied practices include being a non-anxious presence, holding space, and working with pauses and silences. When working with processes of reframing, spiritual-care practitioners are drawing on ancient wisdom traditions, co-creating new possibilities through the use of metaphors and narratives that speak to experience. Such insight and skills include understanding the way in which ritual, liturgy, ancient wisdom texts, and tradition function. Such practices are underpinned by understanding the way in which people change, grow, and mature, fostering agency and holding open spaces where transformative moments can occur and insights of transcendence can form. At this point there is significant borrowing from the psychoanalytic and psychotherapeutic disciplines. Peng-Keller observes that the difference between spiritual care and other disciplines (e.g., psychology or psychotherapy) is the horizons of meaning within which each profession listens, dignifies, and resonates (
Peng-Keller 2024), which vary between medical, physical, psychological, psychiatric, and social concerns. The horizon of meaning within which spiritual care works is that of transcendence or the ‘sacred,’ even when not explicitly mentioned (
Peng-Keller 2024); it is the lens through which salient features are rendered visible, viable, and valuable. It is this lens which will vary between disciplines.
Just as it can be demonstrated that there is significant overlap between broad spiritual care and narrower religious care, there is also considerable overlap between general spiritual care, which involves all the multidisciplinary team, and specialist spiritual care, shown by the 2 × 2 Spiritual Care Matrix, see
Figure 2, included below (
Bradford et al. 2024).
4. Relationship between Religious Care and Spiritual Care and the Multidisciplinary Team
The 2 × 2 Spiritual Care Matrix delineates the relationship between spiritual care and religious care. The two quadrants on the right of the document represent narrower intentional religious care offered by an authorised religious representative of a particular faith or religion to people of similar religious tradition or faith groups. Spiritual care at a more general level is shown in the upper quadrant, and more specialised spiritual care is in the lower quadrant. The left-hand quadrants relate to broad spiritual care; the upper is more general, applying to each member of the multidisciplinary team. As with religious care, there is also a more specialised layer of spiritual care provided by spiritual-care practitioners, represented by the lower quadrant. The lower quadrant works with spiritual distress and existential and personal questions about meaning, purpose, and belonging, with significant skills overlap with the psychosocial disciplines.
At a broad level, spiritual-care practitioners work with existential challenges and value-based considerations, spiritual concerns. They are those things that are part of human life that are not considered diseases, disabilities, and disorders but nonetheless can cause deep distress if not given voice to and acknowledged. Spiritual care tends to focus on spiritual and existential needs and distress, in as much as they are normal responses to ‘abnormal’ events and encounters. As noted above, the similarities between spiritual care and other disciplines (e.g., psychology or psychotherapy) are differentiated against the horizons of meaning within which each works.
The overlap between spiritual care and programs such as the Schwartz Centre Rounds© and Value-Based Reflective Practice© sits comfortably within the upper left-hand quadrant of the spiritual-care matrix of broad general spiritual care. This quadrant focuses on compassionate presence with an emphasis on connecting and understanding others by attending and accompanying them through particular events, with a concern for their meaning, purpose, and belonging. The spiritual-care practitioner brings their specialist skills of compassionate presence and processes of reframing while refraining from guiding the conversation into spiritual depth or transcendence. Similarly, psychotherapists may find that Schwartz facilitation techniques are similar to the ‘common factors’ that are shared by equally effective psychotherapeutic modalities while noting that Schwartz Rounds are distinct from group psychotherapy (
Wampold 2015). Nevertheless, spiritual insight and transcendence may occur, as may the alleviation of psychological distress (
Leung et al. 2024).
5. Spiritual Care within the Healthcare Institution
Simon Peng-Keller highlights the liminality of the healthcare spiritual-care practitioner at an institutional level. The healthcare spiritual-care practitioner is held in tension between faith communities and the healthcare system and by being both inside and outside of the multidisciplinary care team. This liminal state necessitates a need for clear articulation of the restorative and beneficial goals at the individual and the organisational level. However, as Peng-Keller notes, when the spiritual-care practitioner’s responsibility is limited to bedside conversations without being involved at an institutional level, they have no leverage to be able to ‘exert a transformative influence in the health institution’. (
Peng-Keller 2024).
To be part of an institution requires more than occupying the same building. More is needed for connection than simply being in the same place at the same time; there is a need to enter a shared ‘third space’. A third space is a different way of forming a community, as described by Edward Sojo. The third space is differentiated from the first space or the physical environment, and the second space’s intended social use of the environment. A hospital ward is a physical space (first space) for the treatment of patients by various members of healthcare staff within strict roles and hierarchies (second space). Religious scholars Abdullahi Ahmed An-Na’im and Bonnie Miller McLemore describe a third space as a liminal space on the boundaries in-between forms of difference, which is revealed as a place where overwhelming narratives can be displaced (
An-Na’im and Miller-McLemore 2020). A third space is a hybrid space where professional roles and identities can be held at a distance allowing people to connect as equals beyond the usual hierarchies where experiences can be processed through new horizons of meaning.
6. Embracing Liminal Third Spaces
For consideration in this paper are two reflective-practice programs that open out ‘third spaces,’ providing different avenues for spiritual care by spiritual-care practitioners. These programs open new avenues for compassionate presence and processes of reframing for individual staff and at organisational levels. The two programs chosen both operate within the broad generalist domain of spiritual care and have spiritual-care practitioners integrated within their model. The Schwartz Centre Rounds®, developed by the Schwartz Centre for Compassionate Care at Massachusetts General Hospital, will be the primary focus of this paper, a program where spiritual-care practitioners can make a significant contribution. The second program to briefly mention is the hospital-wide chaplaincy-led program, Value-Based Reflective Practice VBRP®, developed by chaplains with the National Health Service (NHS) of Scotland.
The multidisciplinary Schwartz Centre Rounds® (Rounds), first convened in 2002, are named after oncology patient Kenneth Schwartz. In his last days, Ken Schwartz established a charitable foundation, The Schwartz Centre for Compassionate Care. The Schwartz Centre aimed to foster compassion in healthcare to enhance the human connection in healthcare, with concern for the spirit and soul of patients and caregivers.
The aim of the Schwartz Centre Rounds® (Rounds) is to
…support healthcare staff to re-connect with their values through peer reflection, and to promote more compassionate patient care (
Maben et al. 2021). …through organisation wide forums that prompt reflection and discussion of the emotional, social and ethical challenges of health-care work, with the aim of improving staff well-being and patient care (
Maben et al. 2018).
The Rounds are an organisation-wide project facilitated by a clinical leader, with a multidisciplinary planning committee that includes clinical and non-clinical staff: physicians, nurses, social workers, case managers, patient safety officers, spiritual-care practitioners, porters, security staff, administration staff, and management. Schwartz Rounds are conducted across hundreds of health facilities in the United States, Canada, the United Kingdom, Ireland, Australia, and New Zealand. The program and training are administered through licensed agreements with the Schwartz Centre in Boston, MA. Rounds are run by a leadership team across large health organisations and in smaller facilities such as hospices or as unit-based rounds.
Similar to Rounds, VBRP was developed as a form of reflective practice and support for staff where a facilitator leads the group through a set of reflective questions to explore and discuss through a series of reflective prompts, followed by a reflection on new insights that may have arisen.
VBRP was developed in Scotland by NHS chaplains for supervising reflective practice groups of chaplains from different theological and religious traditions. Initially, the chaplains sought to facilitate a shared reflective practice space for chaplains from different religious and theological perspectives. In VBRP, each person reflects on their work from the perspective of their own values framework. From the perspective of spiritual care, values underpin a sense of identity and belonging. Values can be viewed through personal, professional, or organisational lenses and connect to spiritual beliefs (
Kennedy and Kennedy 2022). It was realised that these same broad spiritual-care principles could be applied beyond spiritual care and used to facilitate multidisciplinary reflective practice groups.
The aim of VBRP® is that,
…staff have a regular opportunity to reconnect with their core values and motivations, reflect on their attitudes and behaviors, enhance their person-centered practice, deepen their relationship with colleagues, and develop their resilience and well-being.
From the inception, the Rounds have differed in size from VBRP, which involves small groups facilitated by a trained spiritual-care practitioner. Similarly to the Rounds, VBRP has the aim of helping staff remember the motivations and values that drew them to healthcare and to enhance person-centred care by engaging the head and heart of the participants together. The Rounds differ subtly in format from VBRP, as they tap directly and experientially into participants’ outcomes, feelings, and emotions in a sustained way before drawing new insights. Staff experience compassion and extend compassionate support to others; then, toward the end, they reframe their experiences against new horizons, which in turn supports healthcare staff in reconnecting with their values in a new way through the reflective process of the Rounds.
Our Rounds included spiritual-care practitioners in its inception (
Leung et al. 2024), although the focus was always compassionate care rather than spiritual care. Palliative-care physician and spiritual-care advocate Christina Puchalski has argued convincingly that compassionate presence is the essence of general spiritual care, where compassionate presence is the accompaniment of another through their suffering, alleviating the aloneness of isolation and deep pain. The practice of compassionate presence is to be present, listen deeply, and commit to caring while the person finds healing from their suffering (
Puchalski 2020,
2021).
The synergy between spiritual care and programs such as the Rounds or VBRP is the shared aim of modelling and providing compassionate presence and facilitating a shared third space where challenging encounters and experiences can be reframed in the context of community against new horizons of significance. The synergy happens first at the level of individual staff members and then at the organisational level.
7. Finding the Synergy
When spiritual care is limited to only the care of patients, spiritual-care practitioners have limited influence within the organisation or healthcare workforce. In our experience, the Rounds has created a third space where healthcare staff and spiritual-care practitioners connect on an equal footing as colleagues, focusing on similarities rather than differences. Through the Schwartz Rounds, staff experiences compassionate care that attends to the spirit and soul of staff and patients. From a synergetic point of view, spiritual-care practitioners work closely with members of multidisciplinary teams for patients’ care and collaborate to establish programs that open up leadership roles in the wider organisation such as Schwartz Rounds.
1 The Rounds, from another perspective, depend upon facilitators and members of the multidisciplinary leadership team with a range of skills and practices, particularly those with high-level skills in the areas of reflective practice, holding space, and accompanying people into a narrative space, which we have found provide a natural fit for specialist spiritual-care practitioners.
Spiritual care and the Rounds work from a person-centred model that fosters agency at a number of places; participation in the Rounds is voluntary, and there is an emphasis on allowing space for the exploration of dilemmas rather than problem solving. The Rounds seek to create safe spaces where healthcare professionals can be vulnerable, engage with their full humanity, including their spiritual and religious selves, and connect with themselves and others. Compassionate care neither conflicts with nor precludes a person’s religious beliefs. As shown by the 2 × 2 Spiritual Care Matrix, specialist spiritual care, while closely connected to specialist religious care, focuses on the meaning, purpose, and belonging that a person discovers in their specific situations.
The Rounds are designed to support staff in remaining emotionally engaged with their work and compassionate towards patients, their families, and colleagues, as well as improving the well-being of staff, the effectiveness of communication and engagement, and, ultimately the care of patients. These aspects resonate with the broad generalist quadrant of the 2 × 2 Spiritual Care Matrix, envisioning all staff offering general spiritual care in the form of compassionate presence and accompanying individuals through life events and circumstances.
Our initial studies of the Rounds in an urban Australian setting demonstrated benefits for the staff. In the shared experience of the Rounds, staff reported that they felt connected and not alone, and they were more able to understand other people’s roles. Participating in the Rounds normalised and validated their experiences, providing a safe space for vulnerability and authentic conversation. We observed that some of the optimism expressed to the Rounds was in response to the highly structured Schwartz process, active facilitation, consolidation of the safe space, and panellist preparation. This paper provides further perspectives and reflections on theoretical synergy and practical elements that we believe underpin the positive assessment of our Rounds by the participants (
Leung et al. 2024).
7.1. Theoretical Synergy
The Rounds, like spiritual care, are not outcome-driven but rather take place within a framework of certain objectives such as being supportive and helpful and orientating themselves towards participants’ needs. Such programs need to critically assess the way in which they have been experienced by recipients or participants and to what extent perceived as supportive and helpful through documentation, evaluation, and empirical research (
Peng-Keller 2024). In order to evaluate such programs they must be very clear about their goals and communicate them transparently, and each encounter should be evaluated in light of the extent to which it was beneficial and ‘healing’ (
Peng-Keller 2024). The work by Jill Maben and colleagues in the United Kingdom sought to identify the program theory and mechanism using a realist evaluation method, which takes account of the interplay between context and social processes and underlying causal mechanisms using a realist evaluation method (
Maben et al. 2018).
The realist evaluation identified four distinct stages in each presentation, illustrated by
Figure 3, each having a cumulative impact on the next stage; in sites with well-established rounds, there was a further cumulative effect as regular participants became ‘Schwartz savvy,’ understanding the purpose of the Rounds and contributing appropriately.
The four cumulative stages are as follows:
This in-depth iterative process of the realist evaluation revealed a simultaneous collection of nine interlinked programme theories that work in concert with a four-stage cycle for each Round, explaining how and why Rounds produce outcomes:
- (i)
The importance of trust, psychological safety, and containment;
- (ii)
Group interaction enhances reflection and sharing of stories;
- (iii)
Rounds provide a counter-cultural space for staff;
- (iv)
Rounds create an environment where staff are willing to self-disclose;
- (v)
Storytelling provides a vehicle for staff to talk about their experiences at work;
- (vi)
Staff role modelling vulnerability, courage, and bravery reveals their humanity;
- (vii)
Stories provide greater context to patient and staff experiences;
- (viii)
Stories shine a spotlight on hidden stories and roles;
- (ix)
Rounds facilitate experiences to be shared through storytelling that resonate and trigger reflection (
Maben and Taylor 2020).
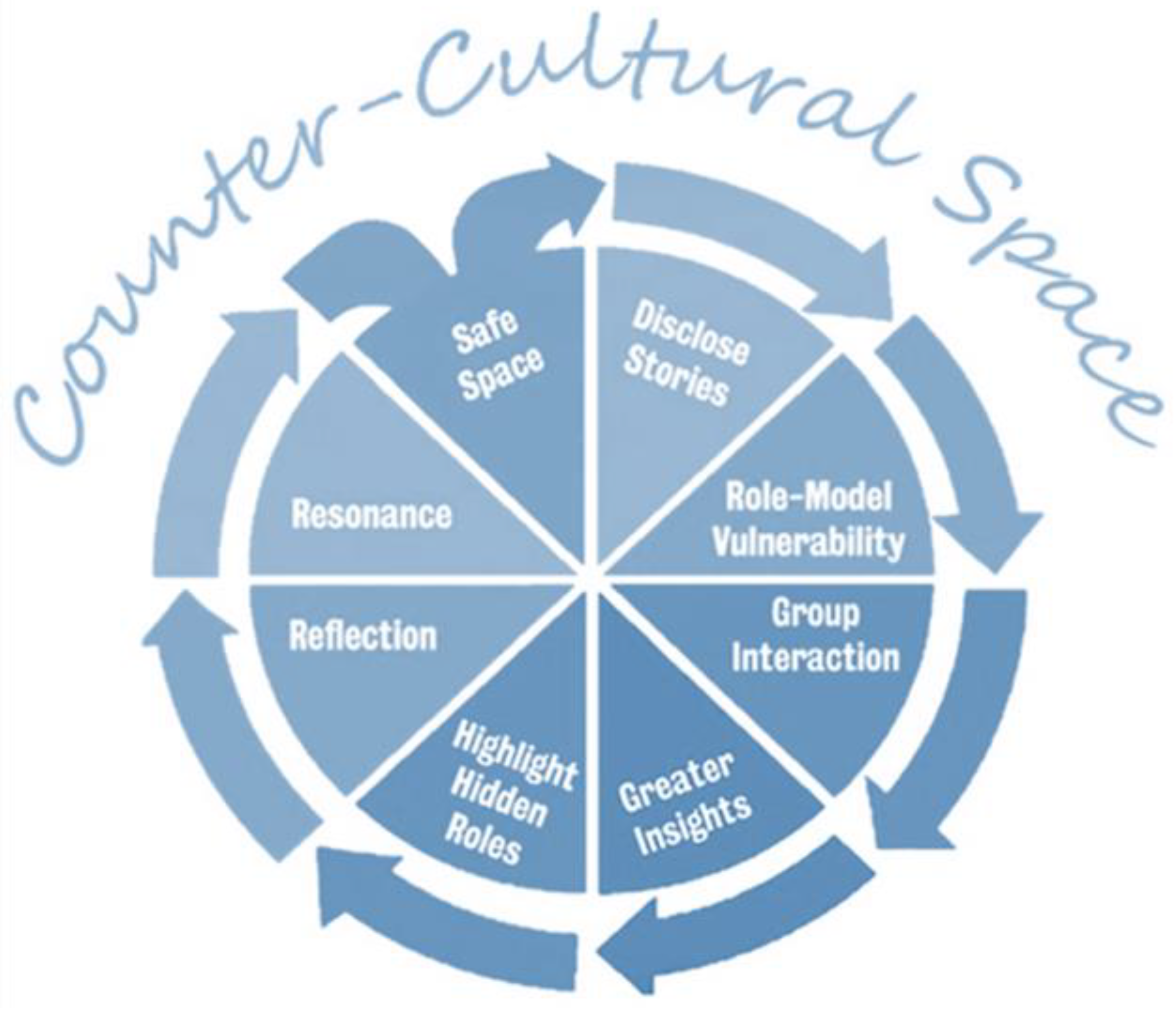
The nine interlinked program theories listed, see
Figure 4, correlate closely with central aspects of the theory and practice of spiritual care outlined below.
7.1.1. Trust, Psychological Safety, and Containment
An essential aspect of the Rounds and spiritual care is trust, safety, and containment, and the demonstratable skills of facilitators and practitioners to ensure this. For both, there is a need for implicit and explicit assent and clear guidelines for the visit or gathering. For the Rounds, this includes pre-Rounds safety checks and ground rules on confidentiality. This safety and containment also includes the reminder that the Rounds do not seek to problem solve or provide an outcome other than provide a safe place where stories can be shared, reflected upon, and resonated with, and that participants feel accepted, respected, and valued. As mentioned above, the approach is non-judgmental and the model itself provides structured support ‘through the use of the Schwartz model to provide a bounded and established time and through the use of the routine and rituals of Rounds’ (
Maben et al. 2018). An understanding and use of ritual is a foundational component of any spiritual care, of which the essential components can transfer to other settings such as the Rounds (
Peng-Keller 2024;
Best et al. 2020). Mabel et al. describe an ‘unsafe’ Round as including, ‘panellists and audience members experiencing embarrassment, rejection, reprisal or blame, or experiencing bullying and punishment for speaking out’ (
Maben et al. 2018). Underlying the trust, psychological safety, and containment are principles of trauma-informed care. The Schwartz Center uses a trauma-informed approach in their facilitation training, basing their unit on Hobfoll et al., and evidence-based factors that people need to recover from adversity and stress, mirroring concerns that also underlie spiritual care practices (
Streets 2015;
Kimberg and Wheeler 2019;
Hobfoll et al. 2007).
7.1.2. Group Interaction
The central dynamic of the Rounds is a group interaction. The Rounds itself is a ritual, following a carefully designed liturgy with stable patterns and rituals, beginning with a welcome, citing the ground rules, and explaining a little of the history and philosophy of the Rounds. The familiarity of the consistency helps create safety for the participants. This scaffolds healthcare staff through some of the psychological difficulties of their work. The mechanism by which such benefits might be derived is to liken Rounds to some of the benefits of group psychotherapy, as defined by Yalom (
Leung et al. 2024).
Structured group interactions such as Rounds correlate closely to the role of a spiritual-care practitioner. The role of the spiritual-care practitioner goes beyond formal notions of ritual or religious practice to encompass the unique capacity of each individual, but this is not to forget that contained within the role is conducting religious services and civil services such as memorial and remembrance services (
Best et al. 2020), as well as less formal roles of leading reflective practice groups. As such, they are well placed to lead Value-Based Reflective Practice groups of healthcare workers across different disciplines in the NHS in Scotland.
Each of the nine interlinked program theories of the Rounds listed above correlates closely with central aspects of the theory and practice of spiritual care with skills in providing a trustworthy counter-cultural third space. In this space, there is psychological safety and containment, where individual needs are contextualised within a group. These program theories provide the baseline for a spiritual or compassionate interaction where vulnerability and self-disclosure are modelled and hidden stories are shared, creating the conditions for resonance and reflection, and narratives as yet unsaid, to well up into speech.
7.1.3. Counter-Cultural Third Space
Rounds, like spiritual care, host a conversation by opening up a creative space where people have the freedom to ‘turn-over’ an event, thought, or emotion in an imaginative manner, remaining open to new emergent possibilities. Holding space for another person is a foundational concept in spiritual care, and the practice is often underpinned by the practice of Paul Tournier’s person-centred care and Carl Rogers’ non-directive, non-judgemental counselling techniques (
Peng-Keller 2024). Both the Rounds and spiritual-care theory draw on concepts of the third space, which is a ‘liminal space on the boundaries in-between forms of difference,’ where overwhelming narrative can be explored from different perspectives (
An-Na’im and Miller-McLemore 2020), or where staff can, for a time, be moved away from ‘their default position of urgent action, reaction and problem-solving to an hour of stillness and slowness’ (
Maben et al. 2018). A third space, or counter-cultural space, allows clinical and non-clinical staff to come together as a truly multidisciplinary group gathering in a flattened hierarchy, allowing for unique possibilities to think together and learn from each other (
Maben et al. 2018). Anita Atwal noted that healthcare spiritual-care practitioners who are skilled in reflective practice already occupy a liminal third space. Spiritual-care practitioners are outside line management systems, trained in offering multifaith and multicultural spiritual care for people, either religious or secular, and are well placed to care for staff as well as patients (
Atwal 2022). A further observation made by Maben et al. was the provision of food at the Rounds ‘and the way in which this forms a symbolic community and ‘breaking bread together’,’ (
Maben et al. 2018) drawing deeply on ancient images of spiritual symbolism and religious ritual.
7.1.4. Self-Disclosure through the I–Thou
To elaborate on this idea, the spiritual-care practitioner seeks to engage in an I–Thou relationship as described by
Buber (
1970). By bringing the self of the practitioner to a ‘meeting’ with another, a free conversation can emerge. The aim is first to meet, and only then to move together with a sense of resonance. Rather than seeking to understand ‘the facts’ of an object, the practitioner brings their whole selves to an interaction to create a sense of mutual discovery. There is a sense of play rather than of investigation. This character of relationship is also developed in psychotherapy. Schwartz Rounds seeks this resonance on a much larger scale. As Buber initially noted, this often cannot be measured, but it is nonetheless perceived. The expert spiritual-care practitioner can guide the cultivation of this relationship; a particularly difficult task with a non-Schwartz savvy audience and within an environment and culture more accustomed to factual understanding is what Buber would call the I–it relationship.
7.1.5. The Power of Narrative
Narratives and metaphors redescribe events by placing new interpretive grids over reality. Narrative, along with metaphors, provides new semantic innovations where a ‘new thing—the as yet unsaid, the unwritten springs up in language,’ a new insight is born or a new sequencing of events, or a ‘new congruence in the organizing of events’ (
Ricoeur et al. 1990). When a spiritual-care practitioner creates space for another, they are holding space for a new congruence in the organising of events formed into a new story. Spiritual-care practitioners have been described as ‘story catchers’ (
Best et al. 2023). From a narrative perspective, A.W. Frank observed that people arrange events into narratives that follow predominantly three narratives: first, narratives where chaos represents narrative circumstances where all hope has been lost; second, restitution narratives represent a hope that life will return to normal; and third, quest narratives are adopted by those who meet suffering embarking on journeys of hope and discovery (
Frank 1998). At a deeper philosophical level, the works of Irvin Yalom and Victor Frankl provided underpinnings of existential-psychotherapeutic approaches where they theorised that people have a ‘will to meaning’ and ‘existential givens,’ which provide horizons of meaning that are the horizon against which people seek meaning (
Hartog 2021).
Seeking and finding meaning are crucial to people’s everyday lives, particularly when coping with adversity (
Paloutzian and Park 2005). People go through life with a set of views about themselves, others, the world, and where they fit. Each person has a unique meaning system through which they categorise and comprehend events and circumstances and plan for the future (
Paloutzian and Park 2005). When confronted with an event or circumstance for which they have no working category, their meaning system is challenged, which has been called ‘contingency’. An experience of contingency occurs when something that is technically possible but will not necessarily happen, happens. For example, it is quite possible to get cancer, be involved in a car accident, or be betrayed by someone close, but if or when these things happen ‘to me’ or ‘to you’ when it is also possible that they might not happen, they can precipitate a sense of shock, an existential crisis or a sense of groundlessness. There is an inability to grasp or understand the event. An experience of contingency conflicts with a person’s worldview or sense of purpose, creating biographical disruption. This disruption is experienced as a breach of trust where there is an inability to make sense, conflicting with a ‘fundamental human need for understanding, coherence, and meaning’ (
Hartog 2021). It is the need for narrative integration ‘that urges a person to reinterpret one’s own life story, including the [new] life event that is part of it’ (
Hartog 2021).
An idea called narrative ethics is providing people with the opportunity to hear and retell their stories until they find a version they can live with, at best, a version worth living with (
Frank 2014). In finding a version worth living with, a person may find that although they move from chaos, there is no return to normal. Likewise, there is little victory in meeting the challenge head-on; rather, there exists the possibility of quietly embracing stories of transcendence, peacefulness, vulnerability, and even hopefulness where there are few or no changes in the material reality. John Swinton observed that even creative resignation may meet needs more than images of striving and overcoming (
Swinton 2014). Living with less-than-ideal outcomes, in a place of in-betweenness and complexity, is negotiated differently by each person (
Bruce et al. 2011).
Bruce notes, drawing on Yalom, ‘that it is a compelling quest to make sense and reconstruct one’s sense of self and life when it has been unravelled’ (
Bruce et al. 2011). Jill Maben et al. also drew on therapeutic factors that help scaffold this process of reframing, which include ‘universality, altruism, instillation of hope, cohesiveness, catharsis, interpersonal learning and self-understanding’. From a psychospiritual perspective, Lisa Miller, with similarity to Maben et al. and Yalom, articulated five observable traits or phenotypes associated with increased spiritual awareness and practice across ethnicity and culture: altruism, love of neighbour, interconnectedness—a sense of oneness, contemplative practice, and commitment to Religion/spirituality which correlate with ‘pronounced shifts in perception and buffer the effects of stress on mental health’ (
Maben et al. 2018;
Miller et al. 2019). Miller et al. demonstrated that the neuroprotective factors of spirituality corresponded more closely with the ability to reflect and reorientate than adhering to a religious belief. It was not the religious belief per se that was protective but the ability to reflect upon it.
The powerful benefit of narrative in the Schwartz Rounds is that it provides a process by which people can transform painful or disruptive events and find new resolutions on a transcendent or spiritual plane that draws on concepts such as universality, altruism, interconnectedness, hope, and love of others.
7.1.6. Role-Model Vulnerability
Many Schwartz panellists and participants, when interviewed, suggested that skilful facilitation was key to a successful Round (
Maben et al. 2021). This observation confirms Leung et al’.s observation that there is a need for a facilitator to actively role model a way of being through acknowledgement, validation, and offering insight (
Leung et al. 2024), which from a spiritual-care perspective depends upon the facilitator having particular skills. Such skills would include reflective practice mediated through genuine vulnerability where vulnerability is recognition of shared humanity, and ‘represents an important initial step in cultivating a compassionate presence’ (
Sinclair and Chochinov 2012). Existential conversations, such as those encountered in spiritual care, likewise programs such as the Rounds or VBRP, are complicated by overlapping personal and existential needs. For these reasons, ‘providing spiritual care, requires spiritual self-reflection, self-awareness, introspection, and vulnerability’ to mitigate an ever-present risk of miscommunication (
Chahrour et al. 2021).
The recognition of a shared humanity has close parallels with a shared human spirituality. Capturing an idea with similarities to compassionate presence, psychologist Carl Rogers observed that ‘the success of his non-directive counselling theory did not happen for the most part at a mental level, but at a spiritual level’ (
Peng-Keller 2024). Lisa Miller noted that psychotherapists working with client’s spirituality ‘must engage their own spiritual path if they are to accompany clients through a process of spiritual awareness,’ and this evolves through a process of direct experience (
Miller 2011).
Clinicians often directly experience vulnerability and inadequacy when witnessing a patient’s existential despair, which may be an intrinsic human response to another’s suffering, and paradoxically, as observed by Bruce et al. when discussing death, ‘this sense of a profound vulnerability evoked in caregivers, far from presenting an impediment to (re)connecting with a dying person, provides an opening for meaningful and authentic connection’. (
Bruce et al. 2011). Simon Lasair makes a similar point when chaplains meet ‘patients in times of deep vulnerability manifested by physical and perhaps emotional and spiritual poverty, chaplains who engage patients in their fullness as persons’ can facilitate spiritual restoration (
Lasair 2017).
Spiritual-care practitioners have much to contribute to Schwartz Rounds’ facilitation that role models vulnerability, as this ties in closely with their commitment to compassionate presence, spiritual self-reflection, self-awareness, introspection, and vulnerability.
7.1.7. Contextualising
Contextualising is an essential aspect of working with spirituality and understanding that ‘spirituality is constructed in different ways between various religious traditions, spiritual movements, belief systems, cultures, and contexts, and not least by particular individuals in specific circumstances. All may use the terms ‘spirituality’, but each may well be using it in quite different ways’ (
Swinton and Pattison 2010). Swinton and Pattison describe spirituality as a somewhat thin and vague term that has the advantage of sensitising the hearer to listen for issues such as meaning, purpose, value, and transcendence, and to be working within the context of the other person (
Swinton and Pattison 2010).
Spiritual-care practitioners have been described as working among three intersecting systems: between spiritual care and the different health disciplines, patients as the primary clients of healthcare and their relatives, and between languages of belief and values in multifaith and pluralistic contexts (
Peng-Keller 2024). Spiritual-care practitioners engage in a type of code-switching, moving back and forth between different languages of health and faith, religiously neutral language and language of belief, and working with the indeterminacies and ambiguities between the differing perspectives of staff, patients, and families (
Peng-Keller 2024;
Cadge and Sigalow 2013). Simon Peng-Keller describes this ‘ability to code-switch consciously…is the communicative competence needed to be able to provide healing chaplaincy support in complex and often ambivalent situations’ (
Peng-Keller 2024). Schwartz Round facilitation, like the practice of spiritual care, depends on contextualisation and adaptive communication strategies such as code-switching.
7.1.8. Spotlighting Hidden Stories
An integral aspect of the Rounds is shining a spotlight on those whose roles and hidden stories were less well known or understood in the organisation, with the effect of making staff more visible, enhancing teamwork, and helping staff appreciate and know more about each other’s roles (
Maben et al. 2018). A second aspect to spotlighting hidden stories is bringing these ‘hidden stories’ to light, stories deeply tethered to hidden parts of ourselves that invoke feelings of pain, shame, guilt, and regret that lie beneath the personal stories we tell each other about ourselves. Such hidden stories only come to light through processes of accompaniment and emotional resonance in a safe and trustworthy environment (
Pritzker 2012).
Spiritual-care practitioners have trained extensively in eliciting and working with hidden stories, through the reflective study of verbatims and pastoral encounters. Central to spiritual care is holding space and supporting people as they reflect upon their specific circumstances. They hold the dignity and worth of the person and their story through compassionate presence, a process of reframing and helping the emergence of new possibilities.
The process of hidden stories being brought to light creates possibilities for a third possible story to emerge, which is at the heart of much narrative work in Schwartz Rounds. A spiritual-care practitioner has a particular contribution in noticing and bringing to light very precious but hidden stories and valuing them.
7.1.9. Refection and Resonance
Chaplains have been described as providing people with a ‘resonance chamber in which the power of imagination can unfold and deepen’ (
Peng-Keller 2024). The Rounds seek to be a resonance chamber where stories shared by the panellists elicit an unfolding and deepening narrative experience whereby participants can imagine new futures and possibilities. Resonance depends on several factors, including trust, safety, and containment provided by skilled preparation, facilitation, and ritual.
Resonance provides circumstances where perceptions are altered, not through teaching, but through a shared and lived experience where the participants are brought alongside another person and together reflect on experiences resembling their own; there is a focus on ‘us’ creating an experience of emotional resonance in safety and feeling understood. This experience allows for new evaluations of events through an interpersonal resonance in which feeling understood precedes understanding (
Shulgina 2023). As VBRP has shown, resonance happens across one’s own profession and horizons of meaning at the level of shared humanity and is resonated through one’s own deep value system (
VBRP 2023). In addition to trust and vulnerability, two further aspects are needed to create the circumstances for resonance—rituals and rhythms. Rituals and liturgies follow patterns and rhythms, creating an experience of resonance between and within the inner world of the self, which begins to oscillate with another person or in a religious ritual with the Sacred or Divine (
Büssing 2019,
2021).
As the Rounds participants become more Schwartz savvy, our rounds often begin with music. We wonder if this promotes the creation of the third space and the resonance chamber as the dynamics of the Rounds’ rhythm and rituals become more familiar and internalised.
7.2. Outcome Synergy
From our experience of organising Schwartz Rounds in a large Australian tertiary hospital, four themes of the benefits of the Rounds were identified from the feedback of our participants (
Leung et al. 2024):
- (a)
Not feeling alone, connectedness, and shared experience;
- (b)
Understanding other health professionals and disciplines;
- (c)
Normalisation, validation, and safe space for vulnerability;
- (d)
Emotions generated foster authenticity and humanitarian aspect of healthcare (
Leung et al. 2024).
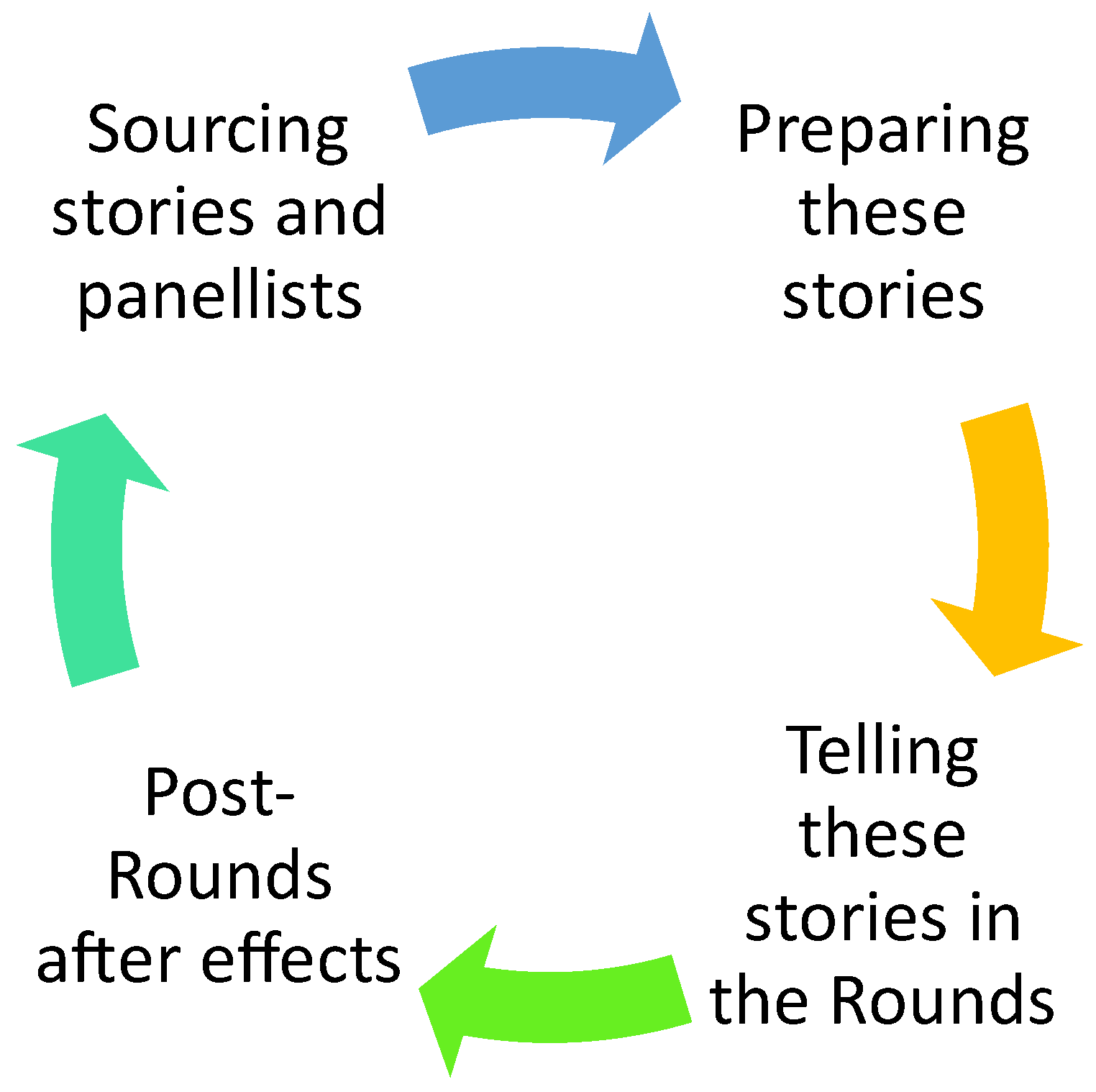
The outcome of our surveys demonstrates results consistent with fidelity to the nine interlinked programs. Our Rounds Leadership Team focused on having enough trained facilitators skilled in reflective practice to deliver a regular Rounds program of a consistently high standard. This facilitation includes allocating enough time and attention to sourcing panellists, preparing them and their stories, facilitating the Rounds, and reviewing afterwards. Our interdisciplinary team included a spiritual-care practitioner and other interdisciplinary staff. The contributions from the spiritual care map closely onto the in-depth iterative process of the nine interlinked programme theories outlined above. In our experience, spiritual-care practitioners have contributed to panellist preparation and facilitation. Each of these themes is consistent with broad spiritual care illustrated by the 2 × 2 Spiritual Care Matrix (above), focusing on connectedness or belonging, with the normalisation and validation related to meaning and purpose.
Spiritual care offers a lens beyond the medical model. From a spiritual-care perspective, change happens at different levels of explanation (chemical, physical, psychological, social, and spiritual), and such spiritual changes are viewed through a theological or philosophical lens with similarities to psychotherapeutic insights (
Leung et al. 2024). The spiritual-care practitioner, like all staff, remains grounded in their own faith, beliefs, and wisdom framework, with the skills to code-switch to a language of values to facilitate other people to speak of what is important to them. The value of the theological or philosophical lens is that, as demonstrated by VBRP, spiritual needs are almost universally experienced, and these are expressed through either religious or non-religious existential frameworks (
Bunniss 2021).
Central to spiritual care and related fields is
making the unbearable bearable, especially when there is little change in the material reality or circumstances (
van Deusen Hunsinger 2015). However, when endeavouring to meet a person’s deepest spiritual and existential needs, it is important to appreciate that spirituality and religion are complex, multivalent constructs that may or may not materially alter the health outcome for a person. However, attempting to meet a person’s deepest needs, and to accompany them through their suffering, are acts of compassion that honour the dignity and humanity of the whole person, a task for which the spiritual-care practitioner is well equipped or foster, in the words of Ken Schwartz, ‘small acts of kindness make the unbearable bearable’ (
Pepper et al. 2012).
7.3. Further Synergies
As showcased in our paper so far, the role of spiritual care may extend beyond individual spiritual support to involve systemic healthcare interventions, as seen in our partnership, and more importantly, having spiritual-care professionals involved in the leadership team of our Schwartz Rounds since inception. In our experience, we see the parallels between spiritual care and Schwartz Rounds in attempting to address the existential concerns of staff, both clinical and non-clinical, at the Rounds where matters are articulated and reflected upon in a safe manner, encouraging meaningful interactions and a deeper understanding of the shared human experience. Such an integration (for spiritual care to be embedded in a systemic health intervention) thereby proves instrumental in amplifying the essence of compassionate care, reinforcing the significance of spiritual care as an integral part of systemic interventions within hospitals.
There is a compelling argument for the ongoing complimentary relationship between spiritual care and Schwartz Rounds, ultimately justifying the necessity and value of such synergistic efforts.
Despite movements towards person-centred care and the biopsychosocial model, healthcare systems have faced competing pressures toward economisation and technical super specialisation. Hierarchical decision-making, treating illnesses rather than people, and sacrificing the psychosocial for aspects of care that are more conducive to quantitative measurement are the results. These aspects are enculturated in the medical model, and despite the best efforts of many, they have been difficult to shift. Diversity of perspectives from outside this model, such as spiritual care, is helpful in breaking down some of these problematic aspects and fostering more equal relationships between colleagues and, ultimately, between clinician and patient.
8. Moving Forward
The synergy between spiritual care and Schwartz Rounds may give valuable insight into holistic and compassionate care and the multifaceted human experience within healthcare settings. This is grounded in the understanding that individuals navigating healthcare systems have complex needs, not only including physical, but also emotional, social, and spiritual needs. As Antoine et al. have explored in their initial analysis, in response to the pandemic, there is a critical role of spiritual-care programmes in enhancing the overall quality of healthcare, rendering executives and chaplain leaders and managers to recognise their indispensable contributions to the quality of healthcare reliability and responsivity, and clinical training within a complex environment for their staff alike (
Antoine et al. 2022).
For a spiritual-care practitioner to have a ministry to staff, it is critical for staff to meet spiritual-care practitioners in a third space that is separate from the patient-facing roles that staff usually perform. Initiatives such as Schwartz Rounds and VBRP provide a countercultural third space away from patient-facing roles.
Another aspect of the I–Thou relationship is referred to by psychotherapists as a feeling of ‘mutuality’. A core component of the healing process from psychological suffering is the slow dissolving of isolation and shame, summed up well by the aphorisms ‘we are all in this together,’ and ‘the whole is greater than the sum of its parts’. Spiritual-care practitioners can utilise their relational skills in not only partnering with patients as they navigate their own suffering but also in recruiting a spiritual community, real or metaphorical. Allusion to the sacred or divine may also create a sense of not being alone. Schwartz Rounds also refers to this sense of ‘mutuality’ as a core component of ‘how it works’. Spiritual-care practitioners may have unique skills not only in fostering a sense of wholeness in Schwartz Rounds but also in partnering with staff through their suffering and being in a unique position to provide an ongoing relationship of care after the rounds. Staff benefit greatly from feeling less alone, both within the rounds and after, and spiritual-care services may also benefit through forming new connections with staff and the health organisation.
9. Conclusions
This paper seeks to demonstrate the significance of the synergy between spiritual care and Schwartz Rounds. A synergy creates something greater than the sum of the parts, which has occurred in our experience. Schwartz Rounds has contributed to spiritual care by providing a third-space encounter between spiritual-care practitioners and healthcare staff and being part of a multidisciplinary network working at an institutional level. The nine interlinked programs give language to spiritual-care practitioners and demonstrate evidenced-based theories that underpin much of general spiritual-care practice. The interlinked programs bring spiritual-care practice into conversation with other healthcare disciplines, employing reflective practice and training with close parallels to general spiritual care.
Despite movements towards person-centred care and the biopsychosocial-spiritual model, healthcare systems have faced competing pressures toward economisation and technical super specialisation. Hierarchical decision-making and treating people as illnesses sacrifice the psychosocial-spiritual for aspects of care that are more conducive to quantitative measurement than the quality of care. These aspects are enculturated in the medical model, and, despite the best efforts of many, they have been difficult to shift. Diverse perspectives from outside of this model are helpful to break down some of these problematic aspects. To foster more equal relationships between colleagues and ultimately between clinician and patient, spiritual care reminds us that there is much more to being human than a body, and neglecting a person’s spirituality can lead to harm. In our experience, Schwartz Rounds benefits greatly from spiritual-care practitioners who have expertise in relationships of care yet sit firmly outside of the medical model.
Our experience shows that the contribution of spiritual care to the leadership and facilitation of the Schwartz Rounds has enriched the texture of the multidisciplinary collaboration while at the same time embedding spiritual care more deeply in the fabric of the hospital.



{kind=link}
{kind=link}
{kind=link}
{kind=link}