Abstract
Dimensions of religion contribute in different ways to the in general protective effect of religiosity and spirituality (R/S) against suicidality. Few studies have included a substantial number of dimensions, and even fewer a follow-up, to clarify the stability and contribution of R/S over the course of psychopathology. In this follow-up study among 155 religiously affiliated in- and outpatients with major depression, religious service attendance, frequency of prayer, type of God representation, moral objections to suicide, and social support were re-assessed in 59 subjects. Diverse statistical analyses show a partial change in R/S parameters. Supportive R/S is persistently associated with lower suicidality. R/S at T0 or change in R/S is not associated with additional changes in suicidality over time. The results suggest that the most important change in suicidality can be understood as an effect of a decline in depressive symptomatology, not of changes in R/S. Despite the limited follow-up and sample size, these results emphasize the importance of longitudinal and dynamic evaluation of especially affective and supportive aspects of R/S in suicidal persons.
1. Introduction
Most studies on religion, spirituality and suicidality find that religiosity serves as a protective factor against suicide across all major religious denominations (Gearing and Alonzo 2018; Koenig et al. 2012; Lawrence et al. 2016). The growing body of research on the relationship between religiosity and suicidality demonstrates that multiple dimensions are involved: religious affiliation, religious salience, religious practices and coping (Kleiman and Liu 2014), moral objections to suicide (van den Brink et al. 2018), social support (Kleiman and Liu 2013; Lawrence et al. 2016), type of God representation (Jongkind et al. 2019), and religious struggle (Currier et al. 2019). Few studies on suicidality have included multiple aspects of religion and spirituality (R/S) in one cross-sectional design (Jongkind et al. 2019; McClintock et al. 2016). Even fewer have included multiple factors in a longitudinal design, and when they did, the number of factors were limited (Currier et al. 2019; Mosqueiro et al. 2021). In addition, few theories explain the protective influence of religion on suicidality, such as the moral community theory, moral objections theory, and religious integration, religious commitment, and religious networks perspectives (Jongkind et al. 2019; Koenig et al. 2012; Stack and Kposowa 2011). None of them integrates multiple aspects of R/S in one theory.
This leaves open several questions about the positive and negative effects of R/S and its different dimensions over time in relation to the course of suicidality. Are all R/S aspects subject to change over time? Is the impact of R/S on suicidality always the same over time? Mental illness is a risk factor for suicide, and many mental disorders are accompanied by suicidality, not in the least depressive disorders (Schechter and Goldblatt 2020). The influence of changes in psychiatric symptoms such as a depressive episode is important to examine. Does R/S at the beginning of, or changed R/S over the course of such an episode, also influence the course of suicidality?
This article reports a follow-up measurement (T1) to a previous study (T0) by Jongkind et al. (2019) of 155 religiously affiliated in- and outpatients with a major depressive episode as the primary diagnosis, including all dimensions mentioned above. In that study (T0), high moral objections to suicide (MOS) and a positive-supportive God representation were negatively correlated with suicidal ideation. MOS showed a negative correlation with lifetime suicide attempts. These correlations stayed significant when controlled for the severity of depressive symptoms and demographic factors.
In this sample at T0, two God representation types were identified (Jongkind et al. 2019; van Vliet et al. 2018): (1) a positive-supportive God representation; and (2) a passive-distressing God representation. The first cluster represents a type of God representation that is supportive as well as authoritative and powerful, with positive feelings being dominant in the perceived relationship with God, and with low anxiety. The second cluster is characterized by high anxiety and anger towards God, and the perceived distance of God.
R/S factors, specifically religious attendance, are also a main predictor of remission in a 6-month follow-up of depressed individuals (Mosqueiro et al. 2021). Supportive facets of religiosity are associated with lower levels of depressive symptoms in prospective studies (Braam and Koenig 2019). However, most of these studies do not include repetitive R/S assessment over time.
The aim of the current observational prospective study is to evaluate whether supportive R/S influences suicidality over the course of a depressive episode. Special focus is given to the previously identified factors of MOS and positive-supportive God representations. Therefore, the course of depressive symptoms, suicidality, and R/S over time is assessed, and associations of MOS and type of God representation with suicidality over the course of a psychopathological state are analyzed. Four hypotheses (H1–H4) are tested in a sample of religiously affiliated in- and outpatients with major depression.
H1.
Religious service attendance, frequency of prayer, God representations (QGR-scales and -cluster), moral objections to suicide (MOS), and experienced social support change over time between T0 and T1. Religious activities and experience of support increase with decreasing depressive symptoms.
H2.
QGR-cluster and MOS show a continuous and stable negative correlation with suicidality over time, at both T0 and T1.
H3.
Both MOS and positive-supportive God representations at T0 predict lower suicidal ideation at T1. These correlations persist when corrected for depressive symptoms at T0 (suicidality being excluded).
H4.
When MOS or positive-supportive God representations increase from T0 to T1, suicidal ideation decreases. This effect persists after correction for changes in depressive symptoms (suicidality being excluded) and demographic factors.
2. Methods
2.1. Procedure
This study is a follow-up to a study performed at Eleos, a Christian institute for mental health care with a clinical location and several outpatient departments in the Netherlands. In the first measurement, reported and described in detail by Jongkind et al. (2019), 155 religious (mainly protestant Christian) in- and outpatients were included, all adults with a primary diagnosis of a major depressive episode who participated in a standard diagnostic procedure after they started treatment, in the period between February 2015 and August 2015. Patients signed informed consent and were asked to participate in a follow-up measurement. Those who consented were approached for follow-up in the period between June 2016 and December 2016. Fifty-nine subjects received and returned the follow-up measurement-set and consent by mail, 15 (+/−1) months after their first assessment. This study was performed in accordance with the ethical standards set in the 1964 Declaration of Helsinki (World Medical Association 2013). The medical ethical committee of the University Medical Center Groningen decided that this study conformed to these standards and did not require further approval, under the scope of the Dutch Medical Research Involving Human Subjects Act (WMO).
2.2. Instruments
2.2.1. Psychopathology
Following the intake interview, the presence of a depressive episode was confirmed using the Structured Clinical Interview for DSM-IV TR (SCID; First et al. 2002) on depression at the first measurement (T0). The extent of general psychopathology was measured by the 24-item version of the Brief Psychiatric Rating Scale (BPRS; range 24–168), a detailed semi-structured clinical interview with questions for each symptom, scored on a seven-point Likert scale, ranging from (1) not present to (7) extremely severe (Cronbach’s α 0.78). The SCID and the BPRS were rated at T0 by trained and supervised psychologists with at least a master degree in clinical psychology. Depressive symptoms were assessed at both T0 and T1 using the Beck Depression Inventory (BDI-II-NL) (Beck et al. 1996), a 21-item self-report measure. A score between 0 and 13 reflects minimal depression, 14 and 19 mild depression, 20 and 28 moderate depression, and 29 and 63 severe depression. Cronbach’s α was 0.90 and 0.95 at T0 and T1, respectively. In the analyses in this study, we used the BDI total score excluding Item 9 about suicidality (from here on referred to as BDI-adjusted). The dependent variable is suicidality and inclusion of this item would make the BDI score redundant with the PSI score.
2.2.2. Suicidality
Suicidal ideation and attempt were assessed using the five-item Paykel Suicide Items (PSI; range 5–24) evaluating death wishes to suicidal plans in the previous month, and frequency of any previous attempts. It contains four 5-point (range: never—always) Likert scale items, such as: “During the past four weeks, have you reached a point where you seriously considered taking your life or perhaps made plans how you would go about doing it?”; and one 4-point (range: never—frequent) Likert scale item, “Did you ever in your life attempt suicide?” (Paykel et al. 1974). Cronbach’s α was 0.86 at T0 and 0.87 at T1. Participants were also asked about important risk factors for suicidal behavior, such as suicide attempts by relatives (Franklin et al. 2017).
2.2.3. Religion and Spirituality
The type of God representation was investigated using the Questionnaire God Representations (QGR) (Schaap-Jonker et al. 2008). The QGR 34-item version (including an item on feeling abandoned, in the scale Anger) was used. The first, affective, dimension of the QGR taps the feelings of someone in his or her relationship with God/the divine (e.g., “When I think of God, I experience security”) and includes three scales: Positive Feelings (POS, nine items, range 9–45, α = 0.95 at T0 and 0.94 at T1); Anger (ANG, four items, range 4–20, α = 0.80 at T0 and 0.84 at T1); and Anxiety (ANX, five items, α = 0.88 at T0 and 0.88 at T1). The second dimension concerns perceptions of God’s actions (e.g., “God rules”) and also consists of three scales: Supportive Actions (SUP, 10 items, range 10–50, α = 0.95 at T0 and 0.94 at T1); Ruling/Punishing Behavior (RULP, four items, range 4–20, α = 0.67 at T0 and 0.73 at T1); and Passivity (PAS, two items, range 2–10, α = 0.81 at T0 and 0.72 at T1). Answers are scored on a five-point Likert scale, ranging from (1), does not apply at all, to (5), does completely apply.
Moral and religious objections (MOS; range 4–24) against suicide were investigated with the four-item MOS scale, one of the six subscales of the Reason for Living Inventory (RFLI; Linehan et al. 1983), consisting of four statements considering MOS, such as “My religious beliefs forbid it” and “I am afraid of going to hell”. Answers were scored on a six-point Likert scale, ranging from (1), not at all important, to (6), extremely important. The Cronbach’s α was 0.84 at T0 and 0.85 at T1.
Perceived social support was assessed using the 17-item Social Support Questionnaire (Revenson et al. 1983), which measures positive as well as negative social interactions. This 17-item questionnaire focuses on the amount of social support received over the past seven days and has two scales. The first nine-item scale measures negative aspects of social support (e.g., not feeling understood; range 9–36, Cronbach’s α in this study = 0.79 at T0 and 0.77 at T1). The second eight-item scale measures positive aspects of social support (e.g., receiving warmth and friendliness; range 8–32, Cronbach’s α in this study = 0.81 at T0 and 0.91 at T1).
To measure the extent to which religion was significant in the participants’ daily lives, a four-item scale for religious salience was used, only at T0. Example items are as follows: “My faith is important to me” and “If I have to make important decisions my faith plays an important role.” Answers are scored on a five-point Likert scale, ranging from (1) does not apply at all to (5) does completely apply. In this study, Cronbach’s α was 0.89.
2.2.4. Sociodemographic Characteristics
Respondents also answered questions about their age, sex, marital status, level of education, employment status, religious denomination, medication, and substance use at T0, as well as questions on frequency of church attendance (range 1–5: once a year or less–once a week or more) and prayer at both measurements. The level of education was scored as low (minimum of 8 years), average (minimum of 12 years), or high (minimum of 18 years).
2.3. Statistical Analysis
2.3.1. H1: Change of BDI, PSI, and R/S Factors over Time within the T1-Subsample
First, the distribution of the variables in our sample was described by running descriptive statistics. To examine if the diverse religious dimensions change over time between T0 and T1, instability of the diverse variables for the T1-subsample was tested and the absolute rater agreement between T0 and T1 computed. The correlations of the different scales between T0 and T1 and reporting variances, Pearson’s correlation coefficients, and paired samples t-test values were calculated. A predictive regression analysis was performed to test if measures at T1 could be predicted based on T0 scores per individual measure. Statistically significant changes in outcomes from T0 to T1 were plotted in a diagram, with R/S variables combined in a ‘distressing’ and ‘supportive’ category, respectively.
The stability of the QGR-clusters over time was explored using k-means cluster analysis using the Hartigan and Wong implementation (Morissette and Chartier 2013), with 1000 random starts and a maximum of 10 iterations. This generates two or more sets of observations, named clusters, with a minimized within-cluster sum of squares (i.e., variance), thus providing two or more ‘prototypes’ of individual QGR-profiles, further named QGR-cluster. Estimations were performed at T0 and T1, using data at QGR-item as well as QGR-scale level. The variance ratio of between-cluster and within-cluster dispersion was checked using the Calinski–Harabasz index.
2.3.2. H2: Strength of Correlation of the QGR-Cluster, Respectively MOS, with Suicidality from T0 to T1
This was tested using a Repeated Measures ANOVA with the QGR-cluster, respectively MOS, and moment of measurement (T0, T1). To indicate the strength, direction, and eventual changes of correlations between T0 and T1, simple bivariate correlations between suicidality and, respectively, MOS and QGR-cluster were computed separately for T0 and T1.
2.3.3. H3, H4: Predictive Regression Analyses with (Delta) Suicidality as Outcome
Predictive modelling with internal cross-validation (Browne 2000) was used for the last two hypotheses. Internal cross-validation is an appropriate method to explore the value of different models that have not been tested previously. In the first predictive regression analysis, the predictive ability of diverse religious and spiritual variables (H3) from T0, controlled for the BDI-adjusted score at T0, for suicidal ideation at T1 was estimated. Similarly, in the next predictive regression analysis, the predictive ability (H4) of change in scores from T0 to T1 (delta-T) for the same predictors and BDI-adjusted was estimated. To assess their predictive abilities, a 60% training sample was used to fit the regression model. The predictive ability was evaluated by applying the just-fitted model to the remaining 40% as the validation sample. Performance of this procedure on at maximum three training and validation samples was evaluated through the Root Mean Squared Error (RMSE) and the Mean Absolute Percentage Error (MAPE). The RMSE can be interpreted as the standard deviation of the unexplained variance and is therefore on the same scale as the response variable. It quantifies how accurately the model predicts the response, and it is the most important criterion for the current purpose. As its range and evaluation depend on the outcome scale range, we use the MAPE to assess the prediction error in percentage (Lewis 1982). A MAPE value <10 indicates highly accurate prediction, a value between 10 and 20 is considered good, under 50 is considered reasonable, and above 50 is considered inaccurate. For robustness, the same associations were additionally assessed with a full-sample regression analysis.
All analyses were performed using R, version 4.0.2 (R Core Team 2020). Given the explorative, multidimensional design and limited number of subjects at T0, no power analysis was performed.
3. Results
3.1. Participants and General Characteristics
Fifty-nine subjects (38% response rate of the T0 sample) participated in the measurement at T1. Characteristics of all 155 subjects at T0 and of those 59 included in the follow-up were reported in Table 1. Comparison did not reveal noteworthy differences in general characteristics, and additional t-tests for reported variables in those 59 versus the other 96 subjects found no significant differences (available on request). Most of the participants (83%) were affiliated to Dutch reformed or protestant churches. These churches have been characterized by an emphasis on personally experienced faith, high service-attendance, and deeming suicide a sin (de Lely et al. 2019), where patients from some of their subgroups reported significantly more negative types of God representations (Schaap-Jonker et al. 2017). Two participants committed suicide between T0 and T1, as far as is known by the research team.

Table 1.
Demographic information, history of suicidality, religious affiliation, and salience, of all 155 patients (T0) and the subsample of 59 patients (T1); measured at T0.
3.2. H1: BDI, PSI, QGR-Scales, and Cluster of God Representations (QGR-Cluster) and Negative Social Support Changed Significantly over Time between T0 and T1, with Increasingly Supportive Religious Experiences Accompanying a Decrease in Depressive Symptoms and Suicidality
Mean scores on depressive symptoms and suicidality were more than 25% lower at T1. The mean BDI total score changed between T0 to T1 from 30 to 21 (paired t-test: t = 5.8, p < 0.001), with 32% being in remission (defined as a BDI total score below 14) at T1 versus 7% at T0. The mean PSI total score changed from 12 to 9 on a 24-point scale, with 24% reporting no suicidality (total score below 6) at T1, versus 10% at T0. All R/S factors within the T1-subsample changed less than 25% in absolute height from T0 to T1. All QGR-scales but two demonstrated statistically significant changes in paired t-tests. Scores on Anger and Anxiety decreased by 21% (p = 0.015) and 10% (p = 0.015) respectively. Scores on Positive Feelings and Supportive Actions increased by 2% (p < 0.001) and 8% (p < 0.001) respectively. The QGR-scales Passivity and Ruling/Punishing Behavior, religious service attendance, frequency of prayer, moral objections to suicide (MOS), and the positive subscale of social support did not show any significant (p < 0.05) changes in the paired t-test. The negative subscale of social support decreased between T0 and T1 with 8.5% (paired t-test p 0.035). Table 2 gives the exact means, variances, Pearson’s correlation coefficients, and paired samples t-test values.
Table 2.
Stability of measurements over time within the T1 subsample (n = 59).
In the predictive regression analysis, most measures at T1 could be predicted, with a small offset, based on T0 scores per individual measure (see Table 2). Only QGR-scale PAS, positive social support, and negative social support could not be predicted from T0 (p < 0.05). With adjustment for individual differences in sex, age, and educational level, only negative social support at T1 could not be predicted from scores at T0.
Figure 1 plots the means, rescaled and normalized to a scale from 0 to 1 (0 being the minimum and 1 the maximum of the scale range) for BDI, PSI, MOS, and distressing and supportive R/S aspects over time from T0 to T1. This plot combines only those R/S scales that showed significant change based on the paired samples t-tests: QGR scales Supportive Actions and Positive Feeling in ‘Supportive R/S aspects’, and QGR scales Anxiety and Anger in ‘Distressing R/S aspects’. Negative social support, although significantly changed, was not included because of its non-specific link with R/S. MOS, though stable over time, was separately added for its unique contribution and importance to suicidality.

Figure 1.
Plot of changes from T0 to T1, normalized and rescaled (range 0–1).
A two-cluster outcome for QGR-profiles fitted best for both T0 and T1, with some changes in cluster for individual persons. Exploration of the cluster structure of the QGR profiles on scale level with hierarchical clustering showed a clear ‘gap’ with two clusters, at both T0 and T1. This was supported by the Calinski–Harabasz index based on k-means estimation, which found the highest variance ratio at k = 2 clusters. A plot of both cluster profiles at scale-level at both T0 and T1 is presented in Figure 2. Cluster 1 was a ‘positive-supportive’ cluster, characterized by a combination of positive and supportive representations. Cluster 2 was a ‘passive-distressing’ cluster, characterized by experiences of anxiety and anger towards God, and a stronger experienced passivity of God than the other cluster. These two clusters were used in subsequent analyses. Six subjects were excluded from this specific analysis due to missing observations on one or more of the scales, resulting in the inclusion of 53 subjects for this analysis. Comparison through crosstabulation of the two-cluster solutions at T0 and T1 points indicated a change of cluster for nine persons from a passive-distressing God representation-cluster at T0 to a positive-supportive God representation-cluster at T1, and for four persons a change vice versa, combining to 15 (28%) changes among all 53 subjects. Cluster allocations and cluster transitions were equivalent when using individual items instead of scales.
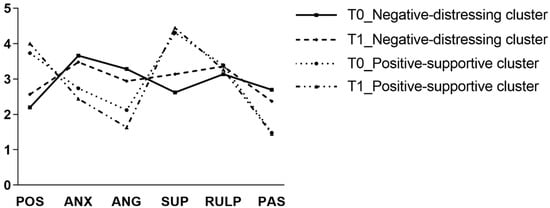
Figure 2.
Profile plot of two QGR-clusters at both T0 and T1.
3.3. H2: The Strength of Correlation of the QGR-Cluster, Respectively MOS, with Suicidality Differed Significantly between T0 and T1
To test for a difference in correlation between QGR-cluster, respectively MOS, and suicidality between T0 and T1, the interaction term from the RM ANOVA was computed. This outcome was statistically significant. The correlations differed statistically significantly between time points for both QGR-cluster (F (1, 197) = 23.17, p < 0.001) and MOS (F (1, 197) = 4.10, p = 0.044). Between T0 and T1, the simple bivariate correlations between suicidality and QGR-cluster changed from 0.40 to 0.48, and between suicidality and MOS from −0.47 to −0.29 (all p-values < 0.001; not reported in table). This implies that both the positive-supportive QGR-cluster and MOS exerted a continuous inhibiting effect on suicidality, but that the strength of this effect changed over time.
3.4. H3: Neither MOS nor Positive-Supportive God Representations at T0 Are Negatively Correlated to Suicidal Ideation at T1: This Persisted when Corrected for Depressive Symptoms at T0 (Suicidality Being Excluded)
Table 3 presents the results of the predictive linear regression analysis for a random 60% training sample, with correction for depressive symptoms at T0 (BDI-adjusted). Neither religious service attendance, frequency of prayer, nor cluster (or any specific scale) of God representation at T0 significantly (p < 0.05) predicted suicidal ideation at T1. MOS had a slightly significant correlation in the presented training sample, but no significant correlation in the two other training samples, indicating no predictive value either. The mean prediction error (MAPE) for this regression model varied between 42% and 65% for three random 60% training samples and their respective 40% validation samples. The same associations were also assessed in the additional full-sample regression analysis, with equivalent results. In a post-hoc analysis without correction for depressive symptoms (BDI-adjusted), no association yielded consistent significance over three random training and validation samples, with a MAPE varying between 41% and 49%. Although the individual R/S parameters at T0 did not predict lower suicidality at T1, additional post hoc analysis indicated a unique contribution of all R/S parameters together. The total model had a R2 of 0.43, and the model F statistics were repetitively significant.
Table 3.
Regression coefficients of different R/S factors and their Deltas (∆) on (Delta) suicidality, obtained from the predictive regression analysis at a random 60% of the sample, corrected for sex, age, and level of education, and for BDI.
3.5. H4: Neither Increase in MOS, nor Increase in Positive-Supportive God Representations from T0 to T1 Were Positively Correlated to an Additional Decrease in Suicidal Ideation When Corrected for Changes in Depressive Symptoms (Suicidality Being Excluded)
Repeated predictive linear regression analysis for change (delta) in suicidal ideation by a set of variables at T0, namely QGR-cluster allocation, MOS, BDI-adjusted, frequency of prayer, religious service attendance, social support, and sociodemographic factors (age, sex, and educational level), yielded no persistent significant R/S predictors in two random training samples. The results of one training sample are reported in Table 3. MOS was significant once, but not in the repeated analysis. The RMSE indicated 5.1 points misprediction, which was more than the actual difference between mean suicidal ideation at T0 and T1 (11.8 and 8.81 respectively). The model yielded a more than 100% misprediction (MAPE), indicating no accurate predictive value. Predictive linear regression for change (delta) in suicidal ideation by change (delta) of the same set of variables also yielded no R/S predictors significant in a training sample (Table 3), with a misprediction percentage (MAPE) above 100%, indicating no accurate predictive value. Equivalent conclusions were drawn from the additional full sample regression analyses. This means that, although MOS and QGR-cluster were consistently associated with lower suicidality over time, increases in these variables did not generate additional decreases in suicidality.
4. Discussion and Conclusions
The focus of this study is the question if supportive R/S, such as MOS and positive-supportive God representations, change over the course of a depressive episode, and if this influences suicidality or even predicts a better outcome.
In short, affective aspects of R/S prove to be dynamic, with continuous protective abilities for supportive R/S. The outcomes suggest that: (a) some R/S outcomes, mainly affective ones, display significant change over time; (b) supportive R/S outcomes show a structural positive association with lower suicidality; and (c) changes in suicidality are mainly correlated to changes in depressive symptoms.
Results show that, in the natural course of a depressive episode, both depressive symptoms in general and suicidality in particular (Kivelä et al. 2019; Richards 2011) decline substantially (>25%) and significantly over time in this population of depressed, religiously affiliated people. God representations, moral objections to suicide, positive and negative social support, prayer, and church attendance show a concomitant change when re-assessed after 15 (+/−1) months. This is a smaller change, both in absolute height and in order of magnitude. Several God-representation scales and negative social support change significantly over time in this study, with an on average 10% decline or increase. God-representation clusters are also moderately stable over this period; a quarter of all subjects change cluster over time. The other R/S factors show no significant changes (H1). This implies that at least some, especially affective, aspects of R/S, change over time, and that these changes are accompanied by changes in depressive symptomatology. The direction of change is as expected: distressing R/S parameters decline with declining depressive symptoms, while supportive R/S parameters increase (see Figure 1). R/S parameters of a behavioral nature, such as prayer or attendance of religious meetings, or convictions such as MOS, are more stable over time. Intermittent, short-lived substantial changes between T0 and T1 in these last factors cannot be ruled out based on the current results, but are less likely.
R/S parameters are frequently associated with lower suicidality, and MOS and QGR-cluster do so in this sample in cross-sectional correlations. Over time these correlations remain present, but change in strength (H2). No R/S parameters or their deltas are statistically significant negatively or positively correlated to the development of suicidality over time, after adjustment for changes in depressive symptoms (H3, H4). This suggests that the most important change in suicidality can be understood as a consequence of a decline in depressive symptomatology, not of changes in R/S.
These outcomes correspond with previous reports. Supportive facets of religiosity are generally associated with lower levels of depressive symptoms. Braam and Koenig (2019), reviewed all 152 available prospective studies on R/S and depression until 2017. Of these studies, 49% reported at least one significant association between supportive facets of R/S and a more favourable course of depression, whereas 10% indicated an association with more depression or mixed results. In addition, studies that focus more specifically on suicidality show that MOS and lower suicide acceptability are associated with less suicidality and a lower future risk of suicide (Phillips and Luth 2018; van den Brink et al. 2018). This fits the current finding that MOS and convictions such as MOS are stable and exert an ongoing influence during the depressive episode, not only during the less severe parts of a major depressive episode.
God representations comprise an affective dimension, capitalizing on the attachment system, and a cognitive dimension, involving the propositional knowledge about God/the divine acquired during religious socialization. Secure adult attachment representations in general, as data from cross-sectional studies suggest, are associated with less depressive symptoms than insecure attachment representations (Dagan et al. 2018). In line with this, the limited cross-sectional research on affective state and God representation shows a positive relation of secure God representations with positive affect (Schaap-Jonker et al. 2017; Stulp et al. 2019), and positive associations of divine struggles, especially in the context of distant or cruel conceptions of God, with mental health symptomatology, recent suicide ideation, and perceived likelihood of a future suicide attempt (Currier et al. 2020). Findings from the scarce longitudinal studies suggest that R/S struggles can act as both a cause and an effect of psychological problems (Pargament and Exline 2020), and that God representations improve during treatment (Tisdale et al. 1997).
With regard to God representations it is important to note that in the current study, the cluster profiles for God representations for both clusters at T1 are almost the same as those previously reported for the full sample at T0 as a ‘positive-supportive God representation’ and a ‘passive-distressing God representation’ (Jongkind et al. 2019; van Vliet et al. 2018). Persons with a positive-supportive profile of God representation experience high positive feelings towards God and perceive his behavior as more supportive; persons with a passive-distressing profile experience high negative feelings (distress) towards God and more passivity of God (see Figure 2). Overall, the same clusters are found at T1. The only difference between T0 and T1 is that at T1 both clusters differ less with regard to authoritative and passive representations. This indicates a relative robustness of cluster profiles over time.
Moreover, the QGR-cluster profiles found in this sample are in line with previous findings in other studies. Schaap-Jonker et al. (2017), who performed cluster analyses on the QGR in 297 individuals both with and without a psychiatric diagnosis, found three types of God representations: a positive-authoritative one, a passive-unemotional one, and, only among psychiatric patients, a negative-authoritarian. These last two clusters seem to combine in the current sample in a ‘passive-distressing’ cluster. From an attachment perspective, the ‘positive-supportive God representation’ could be associated with a secure/autonomous attachment style with God, and a ‘passive-distressing God representation’ with an insecure (anxious, avoidant, or disorganized) attachment style with God (e.g., Granqvist and Kirkpatrick 2016; Schaap-Jonker et al. 2017).
The switching of individuals between clusters is noteworthy. This could be interpreted as an indication that these profiles of God representation are valid and naturally occurring (versus random grouping). In the current study, the changes in type of God representation over time are mainly based on changes in the affective dimension of God representation. This finding suggests that affective disorders bring about changes in the affective aspects of God representations, in contrast to the literature thus far which showed that attachment patterns in general are relatively stable over time (Chopik et al. 2019), and that state effects of affective disorders on personality traits in general are limited (Karsten et al. 2012). Consequently, God representations, especially feelings towards God, seem to be more susceptible to change than expected.
Both the general studies on attachment, and the specific studies on attachment to God, do not mention state-like changes in attachment to God, i.e., God representations, mainly because of missing longitudinal evaluation. A meta-analysis based on 123 samples with 348 effect sizes of in total 29,963 adolescent and adult religious participants yielded “mostly medium effect sizes (r = 0.25 to r = 0.30) for the associations of positive God representations with wellbeing, and for the associations of two out of three negative God representations with distress”, including depressive symptoms (Stulp et al. 2019). Furthermore, several studies have shown positive effects of a secure or supportive attachment style in general (not specifically attachment experienced in relation to God) on depression: in a thorough meta-analysis, Spruit et al. (2020) found, for 123 independent samples, 643 effect sizes, and a total of 54,598 subjects, a significant, moderate correlation of r = 0.31 between attachment and depression in young people, indicating that secure attachment is negatively and insecure attachment is positively associated with depression. For suicidality in particular, fewer studies are available. Miniati et al. (2017) reviewed the then-available literature and found 16 studies, most of them having a cross-sectional design, and suggest that “insecure attachment style, mostly anxious, and unresolved traumas are associated with an increased suicide risk”.
One of the key findings of this study is that R/S, and especially affective aspects of R/S, show some state-like variability and are subject to influences of other state-like parameters, such as severity of depression. Thus far, nearly all longitudinal research on the relationship between R/S and suicidality included only one assessment of R/S, treating it as a trait-like variable. However, assessment of R/S only at T0 underestimates changes in R/S, and leaves a relevant factor out of dynamic modelling. Even constructs thought to be trait-like still “exhibit nonnegligible state components” (Lance et al. 2021), and R/S is no exception. Affective aspects of R/S vary in strength, even during depressive episodes. These attachment-related aspects can be seen as the distress-regulating aspects of religion and spirituality (Granqvist and Kirkpatrick 2013), activated during stressful circumstances (van der Velde et al. 2021). Although suicidality can be seen and treated as a transdiagnostic phenomenon, the outcomes of this study emphasize the importance of both depression and R/S as contributors to suicide risk (cf. Schechter and Goldblatt 2020).
4.1. Limitations
This prospective observational study included 59 subjects, as a non-random subset selected by consent to follow-up, in a naturalistic design, with any usual guideline-concordant psychological and psychopharmacological interventions for depression. Some reasons for the low response rate at follow-up were the long interval and loss of contact or termination of treatment. A comparison of the basic characteristics with all 155 subjects at T0 does not reveal significant shifts that would indicate a selection bias. Unfortunately, it is not possible to find out if non-responders are those with more persistent and severe depression, or just those whose episode went into remission. Although R/S scores in the current sample had changed at follow-up, they were more stable over time than expected. Depressive symptoms and suicidality also remained present, but to a lower extent. These limited or moderate changes restricted the possibilities of this study to detect significant effects of (changes in) R/S on change in suicidality.
The two assessment points and small number of participants limit the power of this study. A mediation or moderation analysis was not possible in this sample given these limitations. In addition, follow-up intervals of months or longer, especially in subjects with a psychiatric disorder, as in the present study, create response biases due to reverse recall over a period of weeks, and loss of information.
4.2. Recommendations and Clinical Implications
For clinicians, these results highlight the importance of including R/S in a psychiatric assessment of depression and suicidality. R/S can be a stable buffer against suicidality during depressive episodes—and in some cases a crystallizing point or even booster of symptoms. This includes not only affiliation or active participation in a religious community. Assessment of the experienced meaning in life, of the significance of religion and spirituality to the individual client, and assessment of the potential benefit of strengthening the client’s religiosity and spirituality, and of participation in supportive R/S activities, are important elements in this approach (Gearing and Alonzo 2018). This study also gives evidence for the common clinical wisdom that R/S-experiences can get better once a depression goes into remission, and stresses the importance of treating a depression as the most important step to lower suicidality in the first place.
The outcomes of this study offer an invitation to do more intensive longitudinal research on the variability of different, especially affective, R/S aspects over time and their correlation to psychopathology. Inclusion of R/S factors in the follow-up of future (intensive) longitudinal research focusing on the prediction of change in clinical parameters and outcomes is advised. It is advisable to include God representations or other measures of attachment to God in such research on suicidality, and also broader daily spiritual experiences. Such intensive methods would further elucidate the natural variability of, for example, affective parameters, lend more insight into the dynamics of different R/S aspects, and enable a more personalized, detailed, and dynamic evaluation of interrelations of suicidality, psychopathology, religiosity, and spirituality.
Author Contributions
Conceptualization, B.v.d.B. and M.J.; methodology, B.v.d.B., M.J. and R.C.A.R.; software, B.v.d.B. and R.C.A.R.; validation, B.v.d.B., M.J. and R.C.A.R.; formal analysis, B.v.d.B., M.J. and R.C.A.R.; investigation, B.v.d.B. and M.J.; resources, B.v.d.B. and M.J.; data curation, B.v.d.B., M.J. and R.C.A.R.; writing—original draft preparation, B.v.d.B.; writing—review and editing, B.v.d.B., M.J., R.C.A.R., N.v.d.V., A.W.B. and H.S.-J.; visualization, B.v.d.B.; supervision, A.W.B. and H.S.-J.; project administration, B.v.d.B. and M.J. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approval was waived by the Ethics Committee of University Medical Center Groningen (2016-03), due to data-collection as a part of the standard diagnostical procedure and a minimal burden for participants in the follow-up measurement.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The data presented in this study are available on request from the corresponding author. The data are not publicly available due to privacy/ethical restrictions.
Acknowledgments
We thank Gerda Mosterd-Pol (Eleos) for her assistance in data collection.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Beck, Aaron T., Robert A. Steer, and Gregory Brown. 1996. Beck depression inventory–II. [Database record]. APA PsycTests. [Google Scholar] [CrossRef]
- Braam, Arjan W., and Harold G. Koenig. 2019. Religion, spirituality and depression in prospective studies: A systematic review. Journal of Affective Disorders 257: 428–38. [Google Scholar] [CrossRef] [PubMed]
- Browne, Michael W. 2000. Cross-Validation Methods. Journal of Mathematical Psychology 44: 108–32. [Google Scholar] [CrossRef] [PubMed]
- Chopik, William J., Robin S. Edelstein, and Kevin J. Grimm. 2019. Longitudinal changes in attachment orientation over a 59-year period. Journal of Personality and Social Psychology 116: 598–611. [Google Scholar] [CrossRef]
- Currier, Joseph M., Joshua D. Foster, Charlotte VanoyeWitvliet, Alexis D. Abernethy, Lindsey M. Root Luna, Sarah A. Schnitker, Karl VanHarn, and Janet Carter. 2019. Spiritual struggles and mental health outcomes in a spiritually integrated inpatient program. Journal of Affective Disorders 249: 127–35. [Google Scholar] [CrossRef]
- Currier, Joseph M., Nicholas Fadoir, Timothy D. Carroll, Shane Kuhlman, Laura Marie, Sarah E. Taylor, Tracey Smith, Steven L. Isaak, and Brook M. Sims. 2020. A cross-sectional investigation of divine struggles and suicide risk among men in early recovery from substance use disorders. Psychology of Religion and Spirituality 12: 324–33. [Google Scholar] [CrossRef]
- Dagan, Or, Christopher R. Facompré, and Kristin Bernard. 2018. Adult attachment representations and depressive symptoms: A meta-analysis. Journal of Affective Disorders 236: 274–90. [Google Scholar] [CrossRef]
- de Lely, Arie-Jan A., Hanneke Schaap-Jonker, and Arjan W. Braam. 2019. Reformed pietists: Higher risk for suicide? A retrospective cohort study on the incidence of suicides in a christian institute for mental health care. Tijdschrift Voor Psychiatrie 61: 837–44. [Google Scholar]
- First, Michael B., Robert L. Spitzer, Miriam Gibbon, and Janet B. Williams. 2002. Structured Clinical Interview for DSM-IV-TR Axis I Disorders, Research Version, Patient Edition. New York: SCID-I/P. [Google Scholar]
- Franklin, Joseph C., Jessica D. Ribeiro, Kathryn R. Fox, Kate H. Bentley, Evan M. Kleiman, Xieyining Huang, Katherine M. Musacchio, Adam C. Jaroszewski, Bernard P. Chang, and Matthew K. Nock. 2017. Risk factors for suicidal thoughts and behaviors: A meta-analysis of 50 years of research. Psychological Bulletin 143: 187–232. [Google Scholar] [CrossRef]
- Gearing, Robin Edward, and Dana Alonzo. 2018. Religion and Suicide: New Findings. Journal of Religion and Health 57: 2478–99. [Google Scholar] [CrossRef]
- Granqvist, Pehr, and Lee A. Kirkpatrick. 2013. Religion, spirituality, and attachment. In APA Handbook of Psychology, Religion, and Spirituality (Vol 1): Context, Theory, and Research. Edited by Kenneth I. Pargament, Julie J. Exline and James W. Jones. Washington, DC: American Psychological Association, pp. 139–55. [Google Scholar] [CrossRef]
- Granqvist, Pehr, and Lee A. Kirkpatrick. 2016. Attachment and religious representations and behavior. In Handbook of Attachment: Theory, Research, and Clinical Applications, 3rd ed. New York: Guilford Press, pp. 856–78. [Google Scholar]
- Jongkind, Matthias, Bart van den Brink, Hanneke Schaap-Jonker, Nathan van der Velde, and Arjan W. Braam. 2019. Dimensions of religion associated with 547 suicide attempt and suicide ideation in depressed, religiously affiliated patients. Suicide and Life-Threatening Behavior 49: 505–19. [Google Scholar] [CrossRef]
- Karsten, Julie, Brenda W. J. H. Penninx, Hariëtte Riese, Johan Ormel, Willem A. Nolen, and Catharina A. Hartman. 2012. The state effect of depressive and anxiety disorders on big five personality traits. Journal of Psychiatric Research 46: 644–50. [Google Scholar] [CrossRef]
- Kivelä, Liia, Annegret Krause-Utz, Joanne Mouthaan, Maartje Schoorl, Rianne de Kleine, Bernet Elzinga, Merijn Eikelenboom, Brenda Wjh Penninx, Willem van der Does, and Niki Antypa. 2019. Longitudinal course of suicidal ideation and predictors of its persistence—A NESDA study. Journal of Affective Disorders 257: 365–75. [Google Scholar] [CrossRef]
- Kleiman, Evan M., and Richard T. Liu. 2013. Social support as a protective factor in suicide: Findings from two nationally representative samples. Journal of Affective Disorders 150: 540–45. [Google Scholar] [CrossRef]
- Kleiman, Evan M., and Richard T. Liu. 2014. Prospective prediction of suicide in a nationally representative sample: Religious service attendance as a protective factor. The British Journal of Psychiatry: The Journal of Mental Science 204: 262–66. [Google Scholar] [CrossRef]
- Koenig, Harold George, Dana King, and Verna B. Carson. 2012. Handbook of Religion and Health, 2nd ed. New York: Oxford University Press. [Google Scholar]
- Lance, Charles E., Juliette Christie, and Gail M. Williamson. 2021. Do State and Trait Measures Measure States and Traits? The Case of Community-Dwelling Caregivers of Older Adults. Assessment 28: 829–44. [Google Scholar] [CrossRef]
- Lawrence, Ryan E., Maria A. Oquendo, and Barbara Stanley. 2016. Religion and Suicide Risk: A Systematic Review. Archives of Suicide Research 20: 1–21. [Google Scholar] [CrossRef]
- Lewis, Colin David. 1982. Industrial and Business Forecasting Methods: A Practical Guide to Exponential Smoothing and Curve Fitting. London: Butterworth Scientific, pp. 236–52. [Google Scholar]
- Linehan, Marsha M., Judith L. Goodstein, Stevan L. Nielsen, and John A. Chiles. 1983. Reasons for staying alive when you are thinking of killing yourself: The Reasons for Living Inventory. Journal of Consulting and Clinical Psychology 51: 276–86. [Google Scholar] [CrossRef]
- McClintock, Clayton H., Elsa Lau, and Lisa Miller. 2016. Phenotypic Dimensions of Spirituality: Implications for Mental Health in China, India, and the United States. Frontiers in Psychology 7: 1600. [Google Scholar] [CrossRef]
- Miniati, Mario, Antonio Callari, and Stefano Pini. 2017. Adult attachment style and suicidality. Psychiatria Danubina 29: 250–59. [Google Scholar] [CrossRef]
- Morissette, Laurence, and Sylvain Chartier. 2013. The k-means clustering technique: General considerations and implementation in Mathematica. Tutorials in Quantitative Methods for Psychology 9: 15–24. [Google Scholar] [CrossRef]
- Mosqueiro, Bruno Paz, Marco Antônio Caldieraro, Mateus Messinger, Felipe Bauer Pinto da Costa, John R. Peteet, and Marcelo P. Fleck. 2021. Religiosity, spirituality, suicide risk and remission of depressive symptoms: A 6-month prospective study of tertiary care Brazilian patients. Journal of Affective Disorders 279: 434–42. [Google Scholar] [CrossRef] [PubMed]
- Pargament, Kenneth I., and Julie J. Exline. 2020. Religious and Spiritual Struggles. Washington, DC: American Psychological Association. Available online: https://www.apa.org/topics/belief-systems-religion/spiritual-struggles (accessed on 26 April 2022).
- Paykel, Eugene S., Jerome K. Myers, Jacob J. Lindenthal, and Joanne Tanner. 1974. Suicidal feelings in the general population: A prevalence study. The British Journal of Psychiatry 124: 460–69. [Google Scholar] [CrossRef] [PubMed]
- Phillips, Julie A., and Elizabeth A. Luth. 2018. Beliefs About Suicide Acceptability in the United States: How Do They Affect Suicide Mortality? The Journals of Gerontology: Series B 75: 414–25. [Google Scholar] [CrossRef]
- R Core Team. 2020. R: A Language and Environment for Statistical Computing. Vienna: R Foundation for Statistical Computing. Available online: https://www.R-project.org/ (accessed on 1 January 2021).
- Revenson, Tracey A., Carol A. B. A. Wollman, and Barbara J. Felton. 1983. Social supports as stress buffers for adult cancer patients. Psychosomatic Medicine 45: 321–31. [Google Scholar] [CrossRef]
- Richards, Derek. 2011. Prevalence and clinical course of depression: A review. Clinical Psychology Review 31: 1117–25. [Google Scholar] [CrossRef]
- Schaap-Jonker, Hanneke, Elisabeth H. M. Eurelings-Bontekoe, Hetty Zock, and Evert R. Jonker. 2008. Development and validation of the Dutch Questionnaire God Image: Effects of mental health and religious culture. Mental Health, Religion & Culture 11: 501–15. [Google Scholar] [CrossRef]
- Schaap-Jonker, Hanneke, Nathan van der Velde, Elisabeth H. M. Eurelings-Bontekoe, and Jozef M. T. Corveleyn. 2017. Types of God Representations and Mental Health: A Person-Oriented Approach. The International Journal for the Psychology of Religion 27: 199–214. [Google Scholar] [CrossRef]
- Schechter, Mark A., and Mark J. Goldblatt. 2020. Suicide: A Transdiagnostic Phenomenon. Psychiatric Annals 50: 136–37. [Google Scholar] [CrossRef]
- Spruit, Anouk, Linda Goos, Nikki Weenink, Roos Rodenburg, Helen Niemeyer, Geert Jan Stams, and Cristina Colonnesi. 2020. The Relation Between Attachment and Depression in Children and Adolescents: A Multilevel Meta-Analysis. Clinical Child and Family Psychology Review 23: 54–69. [Google Scholar] [CrossRef]
- Stack, Steven, and Augustine J. Kposowa. 2011. Religion and Suicide: Integrating Four Theories Cross-nationally. In International Handbook of Suicide Prevention: Research, Policy and Practice. Hoboken: John Wiley & Sons, Ltd., pp. 236–52. [Google Scholar]
- Stulp, Henk P., Jurrijn Koelen, Annemiek Schep-Akkerman, Gerrit G. Glas, and Liesbeth Eurelings-Bontekoe. 2019. God representations and aspects of psychological functioning: A meta-analysis. Cogent Psychology 6: 1647926. [Google Scholar] [CrossRef]
- Tisdale, Theresa C., Teresa L. Key, Keith J. Edwards, Beth Fletcher Brokaw, Steven R. Kemperman, Henry Cloud, John Townsend, and Thomas Okamoto. 1997. Impact of 607 Treatment on God Image and Personal Adjustment, and Correlations of God Image to Personal Adjustment and Object Relations 608 Development. Journal of Psychology and Theology 25: 227–39. [Google Scholar] [CrossRef]
- van den Brink, Bart, Hanneke Schaap-Jonker, and Arjan W. Braam. 2018. Moral objections and fear of hell: An important barrier to suicidality. Journal of Religion and Health 57: 2301–12. [Google Scholar] [CrossRef]
- van der Velde, Nathan, Hanneke Schaap-Jonker, Elisabeth H. M. Eurelings-Bontekoe, and Jozef M. T. Corveleyn. 2021. God Representation Types Are Associated With Levels of Personality Organization and Christian Religious Orthodox Culture. Journal of Nervous & Mental Disease 209: 710–19. [Google Scholar] [CrossRef]
- van Vliet, Niels, Hanneke Schaap-Jonker, Matthias van der Jongkind, Nathan Velde, Bart van den Brink, and Arjan W. Braam. 2018. De relatie tussen godsrepresentaties en suïcidaliteit bij christelijke patiënten met een depressieve stoornis. Tijdschrift Voor Psychiatrie 60: 511–20. [Google Scholar]
- World Medical Association. 2013. World Medical Association Declaration of Helsinki: Ethical Principles for Medical Research Involving Human Subjects. JAMA 310: 2191–94. [Google Scholar] [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).