


Prayer and Healing: A Study of 83 Healing Reports in the Netherlands


Abstract
1. Introduction
2. Theoretical Background
3. Methods
3.1. Recruitment, Initial Assessment and Selection
- -
- Likelihood when compared to the Lambertine criteria (outlined below).
- -
- Completeness of medical data.
- -
- Duration of healing to assess if a recovery is ongoing, in serious chronic diseases or malignancies preferably at least five years.
- -
- Healings before 1990 were excluded because of difficulty in finding medical data (there was one exception in this study).
3.2. Medical Assessment
- The disease has to be serious.
- The disease is known under medical classifications, and the diagnosis should be correct.
- It must be possible to verify the healing with reference to medical data, such as medical history, physical examination, laboratory and radiology investigations.
- The cure cannot be explained by medical treatment in the past or present, nor by the natural course of the disease, such as spontaneous improvements or temporary remissions.
- The cure is unexpected and instantaneous. Although the recovery may take some time, its onset should be instantaneous and related to prayer.
- The cure is either complete or partial with substantial improvement. The individual is fully or largely returned to his or her original state of health.
- The cure is permanent (by the scope of the study time).
3.3. Qualitative Research, In-Depth Interviews
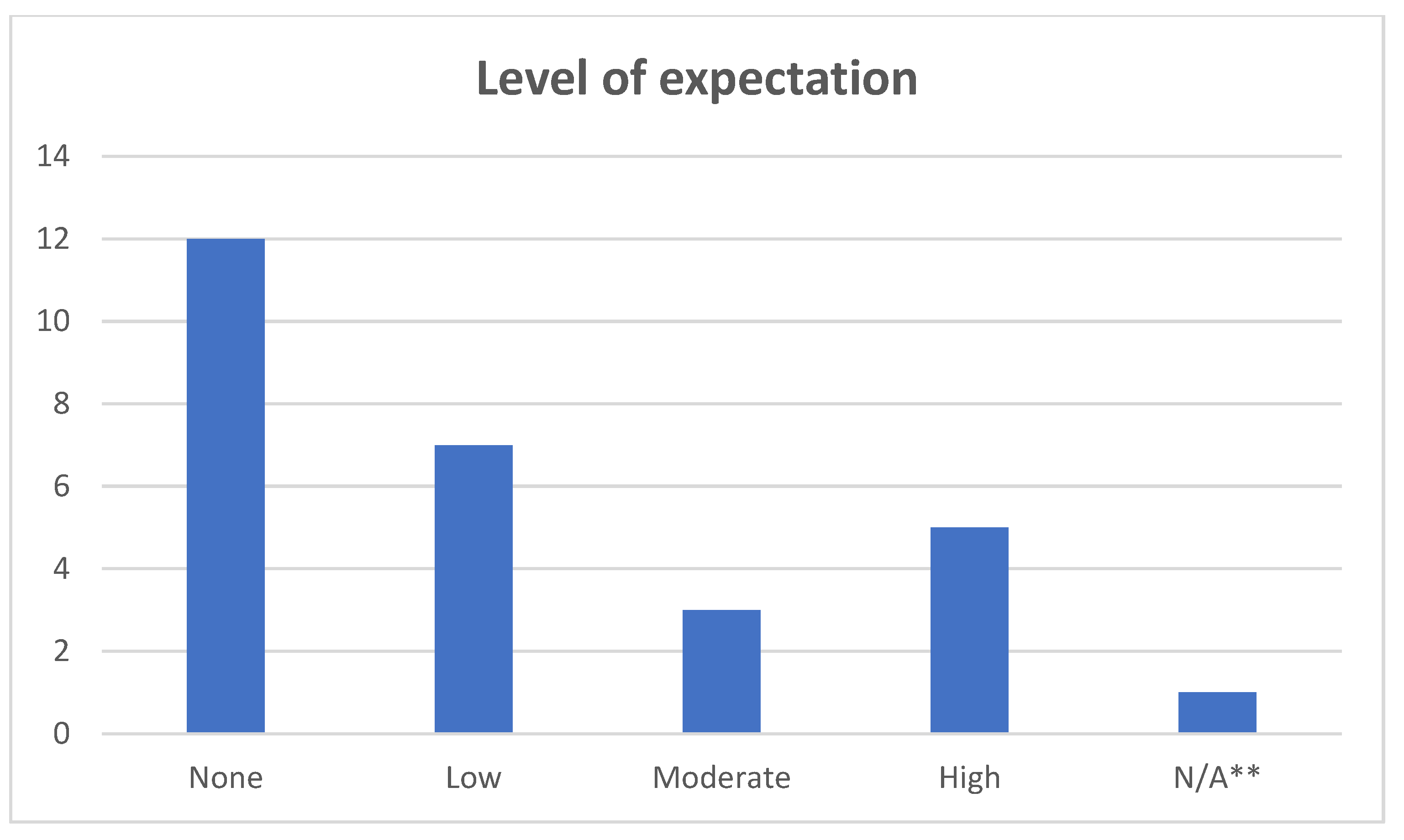
3.4. Level of Expectancy
3.5. Follow-Up
4. Results
4.1. Highlights
- Crohn’s disease
- Acute leukemia (temporary healing)
- Chronic herpetic keratitis one eye with low vision
- Iatrogenic aortic dissection
- Psoriasis with chronic arthritis + ulcerative colitis
- Multiple sclerosis
- Anorexia nervosa
- Parkinson’s disease (90% healing, partial relapse after 8–9 years)
- Drug induced hepatitis, Vanishing bile duct syndrome
- Multimorbidity: severe asthma, impaired hearing, inflammatory osteo-arthritis, incontinence
- Ulcerative colitis with debilitating diarrhea (40 times daily)
4.2. Results: Data Were Obtained until 2021
4.3. Results of Follow-Up in 2019 and 2021
4.4. A Secondary Result
5. Discussion
5.1. Major Observations
- When evaluating 27 selected cases out of 83 prayer healing reports, a medical assessment team concluded there were 11 ‘medically remarkable healings’, no ‘unexplained healings’.
- The study population was diverse.
- Diseases reported covered the entire medical spectrum.
- The setting of prayers varied considerably: personal prayers, group prayers, holy communion,
- liturgical prayers, prayer healing services, anointing of the sick, these could all lead to healing experiences.
- Healing experiences took place across all church denominations, and also when there was no church affiliation at all.
- Healing experiences were often unexpected. Expectancy does not seem to play a major role.
- A large majority of the participants reported an instantaneous onset of their healing, very often associated with physical and emotional manifestations at the same time.
- Manifestations varied a lot, but in all cases they were sensed as being positive and meaningful.
- Most healings had a multidimensional character, invariably interpreted as an act of God. Transforming people, often referred to as a healing of ‘mind, body and soul’.
- Due to the multidimensional aspects involved, the assessment team found it increasingly difficult to differentiate ‘medically remarkable’ from ‘a remarkability in a broader sense’.
- Pronounced mismatches were found repeatedly between ‘subjective’ data and ‘objective’ investigations.
- In our follow-up the majority of the participants were still healed 2 and 4 years afterwards with a lasting positive effect on their socio-religious quality of life. It had often triggered a life of benevolence.
- Participants were frequently confronted with negative reactions from outside, in particular from other Christians and from within their churches.
- These observations will now be taken as point of departure for our further discussion.
5.2. The Research Population
5.3. Spectrum of Diseases Reported
5.4. Modes of Presentation and Prayer Settings
5.5. Level of Expectation vs. Explanation
5.6. Course of Healing
5.7. Manifestations
5.8. Medical Assessment
5.9. ‘Mismatches’ and ‘Matches’
5.10. Follow-Up: Health Related and Socio-Religious Outcomes
5.11. A Pattern of a Healing Touch with a Spiritually Transformative Impact
5.12. An Explanatory Framework
5.13. Strengths and Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Abma, Tineke. 2020. Ethics work for good participatory action research, engaging in a commitment to epistemic justice. Beleidsonderzoek Online. [Google Scholar] [CrossRef]
- Abma, Tineke A., and Robert E. Stake. 2014. Science of the Particular: An Advocacy of Naturalistic Case Study in Health Research. Qualitative Health Research 24: 1150–61. [Google Scholar] [CrossRef] [PubMed]
- Anonym. 2011. Expliquez Moi: Les Miracles. En Complement du Guide Officiel des Sanctuaires de Lourdes. Lourdes: Imprimerie de la Grotte. [Google Scholar]
- Augustine St. n.d. The City of God. Book XXII Ch 8. Floyd: SMK Books.
- Austad, Anne, Marianne Rodriguez Nygaard, and Tormod Kleiven. 2020. Reinscribing the Lived Body: A Qualitative Study of Extraordinary Religious Healing Experiences in Norwegian Contexts. Religions 11: 563. [Google Scholar] [CrossRef]
- Barbour, Ian G. 2000. When Science Meets Religion. New York: Harper Collins. [Google Scholar]
- Baumert, Norbert. 2001. Charisma-Taufe-Geisttaufe 1/2. Wurzburg: Echter Verlag. [Google Scholar]
- Bendien, Elena, Dirk J. Kruijthoff, Cornelis van der Kooi, Gerrit Glas, Tineke A. Abma, and Peter C. Huijgens. 2022. A Dutch study of remarkable recoveries after prayer: How to deal with uncertainties of explanation. Journal of Religion and Health. Under review. [Google Scholar]
- Brown, Candy Gunther. 2012. Testing Prayer. Cambridge: Harvard University Press, pp. 182–84. [Google Scholar]
- Brown, Candy Gunther. 2015. Pentecostal Healing Prayer in an Age of Evidence-Based Medicine. Transformation 32: 1–16. [Google Scholar] [CrossRef]
- De Aguiar, Paulo Rogério Dalla Colletta, Tiago Pires Tatton-Ramos, and Letícia Oliveira Alminhana. 2017. Research on Intercessory Prayer: Theoretical and Methodological Considerations. Journal of Religion and Health 56: 1930–36. [Google Scholar] [CrossRef]
- Doodkorte, Corlien. 2016. Geen Grappen God. Aalten: Stichting Vrij Zijn, pp. 118–44. [Google Scholar]
- Dowling, St John. 1984. Lourdes cures and their medical assessment. Journal of the Royal Society of Medicine 77: 634–8. [Google Scholar] [CrossRef]
- Duffin, Jacalyn. 2007. The doctor was surprised; or, how to diagnose a miracle. Bulletin of the History of Medicine 81: 699–729. [Google Scholar] [CrossRef]
- Duffin, Jacalyn. 2009. Medical Miracles. Doctors, Saints and Healing in the Modern World. New York: Oxford University Press. [Google Scholar]
- Duffin, Jacalyn. 2013. Medical Saints. Cosmas and Damian in a Postmodern World. New York: Oxford University Press. [Google Scholar]
- Evers, Andrea W. M., Danielle J. P. Bartels, and Antoinette I. M. van Laarhoven. 2014. Placebo and Nocebo Effects in Itch and Pain. In Placebo. Handbook of Experimental Pharmacology. Edited by Benedetti Fabrizio, Paul Enck, Elisa Frisaldi and Manfred Schedlowski. Berlin and Heidelberg: Springer, vol. 225. [Google Scholar] [CrossRef]
- Finniss, Damien G., Ted J. Kaptchuk, Franklin Miller, and Fabrizio Benedetti. 2010. Biological, clinical, and ethical advances of placebo effects. The Lancet 375: 686–95. [Google Scholar] [CrossRef]
- François, Bernard, Esther M. Sternberg, and Elizabeth Fee. 2014. The Lourdes medical cures revisited. Journal of the History of Medicine and Allied Sciences 69: 135–62. [Google Scholar] [CrossRef]
- Glas, Gerrit. 2019. Person-Centered Care in Psychiatry. Self-Relational, Contextual and Normative Pespectives. Abingdon and New York: Routledge, pp. 8–9. [Google Scholar]
- Green, Judith, and Nicki Thorogood. 2018. Qualitative Methods for Health Research. London: Sage Publishers. [Google Scholar]
- Gutierrez, Ian A., Amy E. Hale, and Crystal L. Park. 2018. Life-Changing Religious and Spiritual Experiences: A Cross-Faith Comparison in the United States. Psychology of Religion and Spirituality 10: 334–44. [Google Scholar] [CrossRef]
- Hakkenes, Emiel. 2009. De dokter wil wonderen gaan toetsen. Trouw, October 30. [Google Scholar]
- Helming, Mary Blaszko. 2011. Healing through prayer: A qualitative study. Holistic Nursing Practice 25: 33–44. [Google Scholar] [CrossRef]
- Huber, Machteld, Marja van Vliet, M. Giezenberg, B. Winkens, Y. Heerkens, P. C. Dagnelie, and J. A. Knottnerus. 2016. Towards a ‘patient-centred’ operationalisation of the new dynamic concept of health: A mixed methods study. BMJ Open 6: e010091. [Google Scholar] [CrossRef] [PubMed]
- Jørgensen, Karsten Juhl, Asbjørn Hróbjartsson, and Peter C. Gøtzsche. 2009. Divine intervention? A Cochrane review on intercessory prayer gone beyond science and reason. Journal of Negative Results in Biomedicine 8: 7. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Koelsch, Lori E. 2013. Reconceptualizing the member check interview. International Journal of Qualitative Methods 12: 168–79. [Google Scholar] [CrossRef]
- Kruijthoff, Dirk J., Cornelis van der Kooi, Gerrit Glas, and Tineke A. Abma. 2017. Prayer Healing: A Case Study Research Protocol. Advances in Mind-Body Medicin 31: 17–22. [Google Scholar]
- Kruijthoff, Dirk J., Elena Bendien, Corlien Doodkorte, Cornelis van der Kooi, Gerrit Glas, and Tineke A. Abma. 2021. “My Body Does Not Fit in Your Medical Textbooks”: A Physically Turbulent Life With an Unexpected Recovery From Advanced Parkinson Disease After Prayer. Advances in Mind-Body Medicine 35: 4–13. [Google Scholar]
- Kruijthoff, Dirk J., Elena Bendien, Cornelis van der Kooi, Gerrit Glas, Tineke A. Abma, and Peter C. Huijgens. 2022a. Three cases of hearing impairment with surprising subjective improvements after prayer. What can we say when analyzing them? Explore 18: 475–82. [Google Scholar] [CrossRef]
- Kruijthoff, Dirk J., Elena Bendien, Cornelis van der Kooi, Gerrit Glas, and Tineke A. Abma. 2022b. Can you be cured if the doctor disagrees? A case study of 27 prayer healing reports evaluated by a medical assessment team in the Netherlands. Explore. Epub ahead of print. [Google Scholar] [CrossRef]
- Kuhlman, Kathryn. 1992. I Believe in Miracles. Gainesville: Bridge-Logos. [Google Scholar]
- Kuhlman, Kathryn. 1993. God Can Do It Again. Gainesville: Bridge-Logos. [Google Scholar]
- Kuhlman, Kathryn. 1999. Nothing Is Impossible with God. Gainesville: Bridge-Logos. [Google Scholar]
- Lee, Matthew T., Margaret M. Poloma, and Stephen G. Post. 2013. The Heart of Religion. Spiritual Empowerment, Benevolence, and the Experience of God’s Love. New York: Oxford University Press. [Google Scholar]
- Levin, Jeff. 2016. Prevalence and Religious Predictors of Healing Prayer Use in the USA: Findings from the Baylor Religion Survey. Journal of Religion and Health 55: 1136–58, Erratum in Journal of Religion and Health 55: 1159. [Google Scholar] [CrossRef]
- Levin, Jeffrey S. 1996. How prayer heals: A theoretical model. Alternative Therapies in Health and Medicine 2: 66–73. [Google Scholar] [PubMed]
- Levin, Jeff, and Lea Steele. 2005. The transcendent experience: Conceptual, theoretical, and epidemiologic perspectives. Explore 1: 89–101. [Google Scholar] [CrossRef] [PubMed]
- Lundmark, Mikael. 2010. When Mrs B Met Jesus during Radiotherapy A Single Case Study of a Christic Vision: Psychological Prerequisites and Functions and Considerations on Narrative Methodology. Archive for the Psychology of Religion 32: 27–68. [Google Scholar] [CrossRef]
- Maselko, Joanna, and Laura D. Kubzansky. 2006. Gender differences in religious practices, spiritual experiences and health: Results from the US General Social Survey. Social Science & Medicine 62: 2848–60. [Google Scholar] [CrossRef]
- McCaffrey, Anne M., David M. Eisenberg, Anna T. R. Legedza, Roger B. Davis, and Russell S. Phillips. 2004. Prayer for health concerns: Results of a national survey on prevalence and patterns of use. Archives of Internal Medicine 164: 858–62. [Google Scholar] [CrossRef]
- Merleau-Ponty, Maurice. 1968. The Visible and the Invisible. Evanston: Northwestern University Press, pp. 130–55. [Google Scholar]
- Nikchevich, Vesna, and Ana Smylyanich. 2017. Life and Miracles of Saint Basil of Ostrog (with Brief History of the Ostrog Monastery). Cetinje: Svetigora Press. [Google Scholar]
- Ouweneel, Willem Johannes. 2003. Geneest de Zieken! Over de Bijbelse Leer van Ziekte, Genezing en Bevrijding. Vaassen: Uitg Miedema. [Google Scholar]
- Paul, Mart Jan. 1997. Vergeving en Genezing. Ziekenzalving in de Christelijke Gemeente. Zoetermeer: Uitgeverij Boekencentrum. [Google Scholar]
- Poloma, Margaret M., and Matthew T. Lee. 2011. From Prayer Activities to Receptive Prayer: Godly Love and The Knowledge that Surpasses Understanding. Journal of Psychology and Theology 39: 143–54. [Google Scholar] [CrossRef]
- Radin, Dean. 2021. The future of spontaneous remissions. Explore (NY) 17: 483–4. [Google Scholar] [CrossRef]
- Roberts, Leanne, Irshad Ahmed, and Andrew Davison. 2009. Intercessory prayer for the alleviation of ill health. Cochrane Database of Systematic Reviews 2009: CD000368. [Google Scholar] [CrossRef]
- Romez, Clarissa, David Zaritzky, and Joshua W. Brown. 2019. Case Report of gastroparesis healing: 16 years of a chronic syndrome resolved after proximal intercessory prayer. Complementary Therapies in Medicine 43: 289–94. [Google Scholar] [CrossRef]
- Romez, Clarissa, Kenn Freedman, David Zaritzky, and Joshua W. Brown. 2021. Case report of instantaneous resolution of juvenile macular degeneration blindness after proximal intercessory prayer. Explore 17: 79–83. [Google Scholar] [CrossRef] [PubMed]
- Roukema, Riemer. 1989. Van wonderen gesproken. Bulletin voor Charismatische Theologie 24: 2–13. [Google Scholar]
- Salmon, Michel-Marie. 2000. The Cure of Vittorio Micheli. Sarcoma of the Pelvis. Lourdes: Imprimerie de la Grotte. [Google Scholar]
- Sloan, Richard P., and Rajasekhar Ramakrishnan. 2006. Science, medicine, and intercessory prayer. Perspectives in Biology and Medicine 49: 504–14. [Google Scholar] [CrossRef]
- Smith, Jonathan A. 2011. Evaluating the contribution of interpretative phenomenological analysis: A reply to the commentaries and further development of criteria. Health Psychology Review 5: 55–61. [Google Scholar] [CrossRef]
- Turner, Derek D. 2006. Just another drug? A philosophical assessment of randomised controlled studies on intercessory prayer. Journal of Medical Ethics 32: 487–90. [Google Scholar] [CrossRef] [PubMed]
- van Saane, Joke. 2008. Gebedsgenezing. Boerenbedrog of Serieus Alternatief? Kampen: Ten Have. [Google Scholar]
- Watson, Jean. 1999. Postmodern Nursing and Beyond. Edinburgh: Churchill Livingstone. [Google Scholar]



{kind=link}
{kind=link}
| Category | Stage | n= |
|---|---|---|
| All healing reports | After written entry | 83 |
| Subgroup ‘healings evaluated’ | After selection | 27 |
| Subgroup with in-depth interviews | After initial (primary) evaluation | 14 |
| Subgroup ‘medically remarkable’ | After full (secondary) evaluation/assessment | 11 |
| Participants | n = 83 | |
|---|---|---|
| Gender | Male | 30 |
| Female | 52 | |
| Family * | 1 | |
| Religious affiliation ** | No affiliation | 9 |
| Reformed | 23 | |
| Roman Catholic | 5 | |
| Evangelical | 9 | |
| Baptist | 2 | |
| Pentecostal | 2 | |
| Unknown | 33 |
| Reason | ||
|---|---|---|
| Loss to further follow-up * | n = 24 | |
| Healing before 1990 ** | 6 | |
| Death | 5 | |
| No more contact since initial report | 4 | |
| Other medical circumstances | 3 | |
| Personal reasons | 3 | |
| Relapse of the disease reported | 2 | |
| Emigration | 1 | |
| Specific reasons for limited data | n = 7 | |
| Temporary loss of contact | 4 | |
| Language barrier | 1 | |
| Living abroad | 1 | |
| Privacy reasons | 1 |
| Origin of Reports | n = 83 | |
|---|---|---|
| Self-report, articles in newspapers or via other media | 45 | |
| Via a prayer healer | 21 | |
| Via a friend or a relative | 7 | |
| Via a medical doctor | 7 | |
| Self-report, other modes | 3 | |
| Prayer Setting * | n = 90 ** | |
| Prayer healing service | 31 | |
| Prayer(s) by others | 20 | |
| Personal prayer(s) | 10 | |
| Anointing of the sick | 6 | |
| Church service/-members | 6 | |
| Prayer(s) in a group/team | 5 | |
| Christian conference | 4 | |
| Liturgical prayer (monastery, holy communion) | 2 | |
| Bathing (at pilgrimage site) | 1 | |
| Healing rooms | 1 | |
| Unknown | 4 |
| Classification | n * | Disease/Illness |
|---|---|---|
| Musculoskeletal disorders | 13 | Pelvic instability 3; Leg length difference 2; Recurrent backache 3 (post spondylodesis once, S-scoliosis once); Cuff rupture; Whiplash syndrome; C2 abnormality cervical column (impending spinal cord injury); Post traumatic dystrophy; Hip complaints not specified |
| ENT (Ear Nose Throat) | 9 | Hearing impairment 5; Recurrent otitis media; Tinnitus; One-sided vocal cord paralysis; Sinusitis |
| Oncology (malignancies) | 9 | Breast cancer 3 (in situ 1); Renal cell carcinoma; Prostate carcinoma; Carcinoma floor of the mouth; Pancreatic carcinoma; Stomach cancer; Cervical cancer in situ |
| Hematology | 4 | Acute leukemia; Vitamin B12 deficiency; Non Hodgkin lymphoma; Chronic leukemia |
| Neurology | 9 | Multiple sclerosis 2; Paralysis 2 (unspecified); Gullain-Barré disease; Encephalitis; Parkinson’s disease; Spasticity from cerebro-vascular accident (CVA); Coma after resuscitation |
| Ophthalmology | 5 | Descemet membrane rupture (in keratoconus); Chronic herpes keratitis; Retinal vein thrombosis; One-sided low vision (unspecified); Congenital nystagmus |
| Lung diseases | 6 | Asthma 4; Pneumonia; Pleural thickening |
| Traumatology | 4 | Ankle fracture; Leg injury (muscular); Wound finger; Arm fracture |
| Rheumatology | 9 | Fibromyalgia 6; Inflammatory osteo-arthritis; Chronic arthritis (psoriatic); Rheumatoid arthritis |
| Urogynecology | 5 | Incontinence; Nocturnal enuresis; Primary infertility; Hemorrhage with shock after stillbirth; Uterine prolapse |
| Gastro-enterology | 10 | Ulcerative colitis 2; Crohn’s disease; Complications after appendectomy; Chronic gastritis/ulcer; Gall stones; Chronic abdominal pain (adhesions); Gluten intolerance; Hirschsprung disease; Medication induced hepatitis/Vanishing bile duct syndrome |
| Cardiology | 3 | Pulmonary hypertension (in newborn with trisomy 8p); Endocarditis; Coronary sclerosis |
| Endocrinology | 3 | Hyperthyroidism (Graves); Thyroid tumor; Diabetes |
| Psychiatry | 10 | Depression 3; Anorexia nervosa 2; Psychosis 2 (in OCD; postnatal); Addiction 2 (alcohol; heroine); Borderline syndrome |
| Orthopedics | 5 | Knee complaints 2 (cartilage deficiency, meniscus lesion); Snapping hip; Congenital hip dysplasia; ‘Dent in back’ |
| Vascular medicine | 2 | Aortic dissection (iatrogenic); Complications of MoyaMoya syndrome |
| Dermatology | 1 | Psoriasis |
| Pediatrics | 1 | Intra-uterine chromosomal disorder, at birth no abnormalities |
| Infectious diseases | 1 | Lyme disease |
| Miscellaneous | 2 | Chronic fatigue syndrome 2 |
| EV Nr/Sex/Age | Illness | Setting/Duration of Healing | Manifestations | Course | E | Evaluation by Assessment Team |
|---|---|---|---|---|---|---|
| EV 1 M 50–55 | Cuff rupture, planned for cuff surgery | Prayer healing service, Prophecy (12 years) | Internal fight good- bad sensed | Instantaneous healing, no relapse | LE | Cuff rupture partial, could explain healing, but surprisingly instantaneous. |
| EV 2 F 40–45 | Pelvic instability, one-sided impaired hearing | Liturgical prayer in Roman Catholic monastery (15 years) | Touch, current, strong emotion | Instantaneous healing pelvic instability and impaired hearing in two steps, no relapse | NE | Lack of objective investigations pelvic complaints. Audiometry was unchanged. Still surprisingly instantaneous healings. |
| EV 3 F 35–40 | Crohn’s disease | Two prayer healing services (15 years) | 1st: local touch, emotion. 2nd: fell in Spirit, lifted from floor, wind in hall. | Instantaneous healing in two steps, no relapse | LE | Medically remarkable: 13-year course with remissions and exacerbations suddenly stopped after prayer. |
| EV 4 F 45–50 | Pneumonia, lung cancer suspected | Two prayers + laying on of hands in hospital (6 years) | Warm feeling on chest | Recovery under antibiotics | HE | Pneumonia resolved on antibiotics in hospital. |
| EV 5 M 40–45 | Ankle fracture | Prayer in Pentecostal church (14 years) | Prayer: power surge leg, emotion 2 days later | Instant functional healing two days later, no relapse | HE | Fracture lines were not in joint surface, recovery surprisingly instantaneous. |
| EV 6 M 35–40 | Refractory acute leukemia, with multiple fatal complications | Anointing of the sick, Reformed church (one year) | Feeling of support | Sent home to die, but there was complete remission. Relapse after one year, passed away. | NE | Med remarkable: Remission, very unexpected because of disseminated fungal infections, bowel perforation, abdominal abscesses. |
| EV 7 M 50–55 | Carcinoma oral cavity Positive cytology contralateral cervical lymph nodes | Prayers in church, Reformed (5 years) | None | No cervical metastases were found at surgery despite posiitive cytology; no relapse | NE | When reviewing cytology was not found to be conclusive. |
| EV 8 F 60–65 | Multimorbidity and polypharmacy: severe asthma, disabilities + arthritis, impaired hearing, incontinence et al. | Own prayer before sleep while desperate, wishing to die (5 years) | Strong emotions, then a sensation of calm with a sense of being wrapped in a blanket, fell asleep | Stepwise healing of all complaints, all drugs stopped except for levothyroxineNo relapse, has age related hearing aids at present. | NE | Med remarkable: Gross functional improvement after prayer: powerful, addictive drugs (inhalations, prednisone, oxygen, hydroxychloroquine, oxycodone et al.) were stopped without symptoms of withdrawal. Spirometry, audiometry unchanged |
| EV 9 F 50–55 | Advanced Parkinson disease, maximum oral treatment | Prayer at Evangelical Easter conference (8–9 years) | Warm cloud, thick air, ‘tight net’ removed from brain Others also felt sensation. | Instantaneous 90% improvement Partial relapse after 8–9 years. | NE | Med remarkable: rapidly progressive Parkinson’s, largely wheelchair bound and cognitive problems changed to full functional capabilities. DaT-SPECT scanning still abnormal 3–4 years later. |
| EV 10 F 25–30 | Anorexia Nervosa, repeated admis-sions in clinic. | Desperate outcry to God while not religious (5 years) | Dreams, bright light, immediate return of appetite, wind in closed room. | Instantaneous improve-ment, weight gain to 50 kg. No relapse. | NE | Med remarkable: Sudden healing and subsequent weight gain after 8 years of severe anorexia with Body Mass Index fluctuating between 10 and 20. |
| EV 11 F 20–25 | Chronic rt herpes keratitis, low vision; failed corneatransplant | Prayer healing service, pastor had prophecy (10 years) | Bright light, fell on the floor | Instantaneous relief of pain, with vision doubled, 0.2 > 0.4. Loss to follow-up | NE | Med remarkable: Chronic herpetic keratitis right eye from the age of 4 years, she was planned for a 2nd cornea-transplant. |
| EV 12 M 45–50 | Type B aortic dissection, iatrogenic due to cardiac catherization | Multiple prayers in Reformed church, planning to go to healing service (18 years) | Warm hand at his back, gladness, urge to walk | Instantaneous relief of walking restriction, no relapse. | ME | Med remarkable: Blood flow to legs was diminished, could only walk short distances. MRI’s still showing the dissection with a double lumen, both having flow. |
| EV 13 M 35–40 | Recurrent psychosis, obsessive compulsive disorder, suicidality | Prayers alpha course and healing services (17 years) | Feeling of peace during one of the prayers | Gradual healing, full recovery, no relapse | NE | Gradual healing of all psychiatric problems during repeated prayers, simultaneously with regular treatment. |
| EV 14 F 50–55 | Multiple Sclerosis, partially wheel-chair bound (EDSS disability score 6.5) | Different prayers, while preparing for a healing service (12 years) | None | Instantaneous healing of all disabilities after an afternoon sleep; No relapse | LE | Med remarkable: Sudden healing 7-year course of MS, walking max 50 m with crutches, cognitive symptoms. MRI lesions unchanged after healing. |
| EV 15 F 45–50 | Thyroid tumor, solid node 3.7 by 2.1 cm. | Prayer by husband before sleep (9 years) | None | Tumor disappeared next morning, no relapse | LE | Cytology suggestive of subacute (lymphocytic) thyroiditis. Nodi can resolve, but surprisingly fast in this case. |
| EV 16 M 65–70 | Cerebro Vascular Accident right side 1992, one- sided partial spasticity | Prayer healing service with laying on of hands (4 years) | ‘War in his head before healing’, crying after healing | Instantaneous healing in 2 steps (first his arm, then his leg); passed away in 2020, reason unknown. | LE | CVA diagnosed by neurologist in 1992 In 2016 the healing was documented, but absence of neurological data between 1992 and 2016 hampered the evaluation. |
| EV 17 F 30–35 | Ulcerative colitis, psoriasis with arthritis, asthma | Prayer healing service, group of 3 people praying (7 years) | Warmth, sensation as if claws were removed her back. | Healed from colitis, arthritis, psoriasis, not from asthma Medications (prednisone, TNF-alfa blockade) discontinued. No relapse. | HE | Med remarkable: 14-year course of chronic remitting and relapsing colitis and 2–3 year course of psoriasis and polyarthritis stopped after prayer. Regained full capacities, restarted sports. |
| EV 18 F 50–55 | Chronic abdominal pains due to neuralgia and adhesions post appendectomy | Prayers and a bath in Lourdes pilgrimage site’, Roman Catholic (26 years) | Trembling and strong emotions (continuous crying) while taking the bath | Instantaneous healing, no relapse. Passed away in 2021 due to unrelated cause. | NE | Although she had an impressive and instantaneous healing experience, there were no conclusive data of relevant medical investigations to substantiate the healing. |
| EV 19 M 25–30 | Non Hodgkin lymphoma | Group prayers and prayer healing services (33 years) | Vision prior to healing, creating peace and confidence | Instantaneous after first chemotherapy course; had 3 more courses, then quit chemotherapy. No relapse. | ME | Sudden healing after longstanding prayers, simultaneously with start chemotherapy. No decision possible because of concurrent medical treatment. |
| EV 20 F 30–35 | Ulcerative colitis, about to undergo total colectomy | Prayer healing service (7 years) | Strong physical sensationsHusband had a vision | Instantaneous healing, gross reduc-tion of diarrhea, from 40 times daily, now up to 6 times daily | ME | Med remarkable: 7-year course of invalidating diarrhea turned to normal functioning Lesions still visible on follow-up coloscopy |
| EV 21 F 30–35 | Acute Disseminated EncephaloMyelitis (ADEM) and/or Multiple Sclerosis (MS) | Prayer by husband, laying on of hands, also using a cloth of the prayer healer (20 years) | Strong emotional experiences both husband and wife. | Rapid recovery of serious condition. Temporary relapse. First diagnosed ADEM, later MS. Now no complaints. | NE | Evaluation hampered by etiological uncertainties. Extraordinary course, medication for MS was stopped in 2017. |
| EV 22 M 55–60 | Angina pectoris, coronary sclerosis. Past history of 5 coronary bypasses and a small cardiac infarct. | Prayer healing service, prophecy (13 years) | Warmth. Strong pain at the left side and in the left arm. | Instantaneous healing longstanding chest pains and limited exercise tolerance. Since 2019 mild complaints again, controlled by medication | NE | Etiological uncertainty of complaints. Grafts were open when reviewing the angiogram prior to prayer. |
| EV 23 F 35–40 | Congenitalhearing impairment (from childhood) Bilateral hearing loss 45 dB. | Prayer healing service (8 years) | Little push in the back before prayer, ears ‘popped open’. | Instantaneous healing, at present mild complaints, not interfering with daily life. | HE | Sudden normal hearing, confirmed by family, friends and a validated questionnaire. Functioning at work much impro-ved. Audiometry unchanged. |
| EV 24 M 55–60 | Cancer of stomach, signet-ring cell carcinoma | Prayer healing service (10 years) | Strong experience, warmth in stomach region; sure to be healed | Healing, no tumor found on surgery 2 days later; no relapse | LE | The healing coincided with 3 courses of debul-king chemotherapy This is known to be curative in 1–3% of cases as a sole treatment. |
| EV 25 M 50–55 | 1. Alcohol and smoking addiction | Prayer with health worker in clinic (18 years) | Felt as if addiction was ‘pulled out’. | Instantaneous healing, no more craving, no relapse | NE | Expert opinion: in addiction such instantaneous changes can be observed, though in rare instances. |
| 2. Post-traumatic dystrophy+ nerve compression right leg | Anointing of the sick by elders Reformed church (21 years) | None | Instantaneous healing of 18-year course of pain and functional restrictions next day. No relapse. | HE | Surprising course. Evaluation hampered by etiological uncertainties due to two conditions of the leg and intermingling symptoms. | |
| EV 26 M 50–55 | Hypoxic encephalopathy after re-suscitation lasting 20 min with multiple defibrillations | Prayer by daughter at the bedside in the ICU (21 years) | Unknown (because of coma) | Woke up after prayer when he was 5 days in coma, gradual full cognitive recovery | N/A | Admission ICU: comatose (Glasgow coma scale E1M3 Vtube), respiratory insufficient. Poor prognosis, full recovery only in rare instances.Evaluation was hampered due to lack of data concerning depth and course of coma. |
| EV 27 M 50–55 | Medication induced hepatitis (amoxy-cillin/clavulanic acid) with Vanishing bile duct syndrome, impending liver- and kid-ney failure | Prayers by different prayer groups at the same time (6 years) | Feeling of calm and lifted from bed at night in hospital, as if a ‘good power’ was around; neighbor also had a sensation | Rapid improvement starting after the prayers, full recovery | LE | Med remarkable: Transplantation of liver was discussed, when there was sudden rapid recovery. He received treatment simultaneously (prednisone), but bilirubin levels decreased unusually fast, with full recovery afterwards. |
| Reasons for Not Listing as Medically Remarkable | n = 17 |
|---|---|
| Treatment could be explanatory | 4 |
| The assessment team came to a different conclusion when reviewing medical data, such as imaging studies, cytology | 4 |
| No corresponding changes in additional investigations (radiology, audiometry) | 3 |
| Relevant data was lacking in files | 3 |
| Uncertainty about diagnosis | 2 |
| The natural course of the disease could also be an explanation of recovery | 1 |
| Mismatch | Case no |
|---|---|
| Strong and lasting healing experience in impaired hearing without numerical changes in audiometry | 2, 8, 23 |
| Parkinson disease: DaT-SPECT scan showing clear abnormalities despite gross improvement of symptomatology | 9 |
| Aortic dissection: MRI still showing the same double lumen when all symptoms had spontaneously disappeared | 12 |
| Multiple sclerosis: instantaneous healing of debilitating MS, MRI lesions remaining the same | 14 |
| Ulcerative colitis: instantaneous improvement of severe diarrhea (40 times/daily), but lesions were still seen in follow-up coloscopy | 20 |
| Nr/Sex | Illness | Year of Healing, Prayer Setting | Medical Course | Manifestations During Healing |
|---|---|---|---|---|
| 1. F | Breast cancer in situ | 2009 anointing of the sick, Reformed church | Unknown | Strong sensation of God’s presence |
| 2. F | Complications of encephalitis | +/− 1950: prayers by her mother | Gradual improvement | Unknown |
| 3. F | Congenital nystagmus | 2013 prayer healing service | Instantaneous improvement; relapse after 2 years | Strong emotions |
| 4. M | Renal cell + prostate carcinoma | 2015 anointing of the sick, Reformedchurch | Improvement while having treatment; relapse, passed away | Feeling of support |
| 5. M | Leg injury from kickboxing | 2015 prayer in Full Gospel church | Pain flowed away, no relapse | Unknown |
| 6. M | Scoliosis, leg length difference | 1995, setting unknown | Legs became equal while seated; no relapse | Unknown |
| 7. M | Complications of appendicitis | 1978 prayer by his father, in hospital | Favorable rapid recovery | Unknown |
| 8. F | Moya Moya syndrome with brain complications | +/− 2015 own prayer | Neurosurgery was cancelled; further course unknown | Unknown (child) |
| 9. M | Pulmonary hypertension in chromosomal syndr (trisomy) | 2001 prayer with cloth from prayer healer at bedside in hospital | Life threatening pulmonary hypertension stopped (no data from hospital) | Neonate, impossible to establish |
| 10. F | Hyperthyroidism (Graves’ disease) | 2002 Holy Communion in a Reformed church | Instantaneous relief of persistent symptoms under treatment; no relapse | Tiredness suddenly gone, ‘filled by Spirit’ |
| 11. F | Chronic fatigue, Fibromyalgia | 2004 and 2005 Christian conferences | Instantaneous improvements in 2 steps, no relapse | Sense of touch, warm feeling in area with pains |
| 12. F | Rt Descemet membrane rupture with hydrops cornea in keratoconus | 2005 prayer by a pastoral worker twice with in stantaneous improvements | Could instantly read license plates again (she had corneal transplants inboth eyes, 2019) | A shock from top to toe both times |
| 13. F | 1. Finger wound 2. A ‘dent’ in her back due to childhood injury | 2015; 1: prayer by Christian group on street. 2: prayer Facebook contact | 1: rapid healing of wound 2: partially improved | 1: ‘dream’: she could forgive people 2: unknown |
| 14. F | Fibromyalgia/Early arthritis | 1992 prayer healing service | Instantaneous healing | Unknown |
| 15. F | Chronic back complaints. Leg length difference. | 2017 prayer in Healing rooms (USA) | Instantaneous healing, no relapse | Sensation of sparkling water in legs, radiating into both feet |
| 16. F | Cartilage deficiency, knee surgeries. Crut- ches, wheelchair | 2006 prayer healing service, prophecy | Instantaneous relief of pain, walking distances without crutches. No relapse. | Unknown |
| 17. F | Retinal vein thrombosis right eye | 1996 prayer group at work, she was not aware of these prayers. | Gradual improvement | None |
| 18. F | Duodenal ulcer | 2014 prayer healing service | Instantaneous healing Medication stopped | Unknown |
| 19. F | Congenital bilateral hip dysplasia, multiple surgeries | 2005 prayer by husband before visiting the specialist | Instantaneous relief of symptoms | Glowing and trembling legs after the prayer.Husband: gladness during prayer. |
| 20. F | Fibromyalgia | 2009 anointing of the Sick (Reformed church) | Instantaneous relief next day, no relapse | Feeling of heat twice in the night after the prayer |
| 21. F | Postnatal depression, Psychotic features | 2015 breakthrough prayer (long continuous group prayer) | Instantaneous healing | Prophecy, during prayer a vision of a pillar above her head |
| 22. M | Nocturnal enuresis from childhood | 1988 prayer when converting to Jesus in evangelism bus | Instantaneous healing No relapse until 2017 (at present unknown) | Unknown |
| 23. F | Disability, backache after spondylodesis | 2003 prayer healing service | Instantaneous healing, no relapse | None |
| 24. F | Guillain Barré disease | 2009 prayer healing service own church, Evangelical | Rapid recovery, not instantaneous. After 4 years limited relapse. | None |
| 25. M | Recurrent backache, very painful episodes | 2008 own prayer at home, reading the Bible | Instantaneous healing, no recurrence | Strong emotions, paresthesia. |
| 26. F | Pancreas carcinoma with metastases | +/− 1950 prayer services in different churches | Report from son: survived after prayers, while expected to die | Unknown |
| 27. M | Complaints of stomach since 1963 | 1968 prayer, laying on of hands during a conference | Healing after prayer, no recurrence | Intense gladness |
| 28. F | Endocarditis, no further data | 1991 distant prayers | No complaints, no recurrence | Experience of peace |
| 29. M | Recurrent ear infections | 1966 distant prayer by woman in village with gift of healing | Pain disappeared instantly, no recurrence | None |
| 30. M | Tinnitus 2015, all encompassing | 2016–2017 own prayer + diet | Gradual healing, complete | Unknown |
| 31. M | Gall stones, discovered after a colic in 1992 | 1992/1993 prayers, anointing with oil by elders | Gall stones gradually disappeared on ultrasounds | Unknown |
| 32. M | Severe depression: multiple ECT, lithium | 2014 own prayers, and together with others as well. | Healing after prayers, lithium stopped; relapse later on. | Unknown |
| 33. F | Couple, both with heroin addiction: wife one year, husband six years | 1987 desperate prayer by wife. Prayer by husband elsewhere. | Instantaneous healing wife and husband at the same moment, while at different locations. | Both of them felt heat waves going through body at that same moment. |
| 34. M | One sided vocal cord paralysis, after intubation | 1969 healed upon prayer (according to his parents) | Healed | Unknown |
| 35. F | Infertility and anorexia | Late seventies desperate prayers for fertility | Gained weight, had 3 children afterwards | Vision of Jesus on doorstep of room, thankfulness, knew she would become pregnant |
| 36. F | Stillbirth with life threatening hemorrhage | 1984 prayer of husband in adjacent room of hospital. He felt a touch. | Fluxus stopped | She also felt a touch at the moment of her husband’s prayer, and gladness. |
| 37. F | Whiplash | 1994 distant prayers in Brazil, prophecy. | Instantaneous healing | Unknown |
| 38. F | Breast cancer with bone metastases | 2000 prayer in own church (Evangelical) by missionary | Metastases stable since 20 years, no treatment (limited medical data) | Unknown |
| 39. F | Breast cancer: surgery, radio-/chemotherapy; bone metastases found (jawbone and skull) after treatment | 2016 prayer healing service | Healed, scans normal after prayer.(no medical data obtained) | Strong emotions, feeling as if walking on a cloud |
| 40. M | Deficiency Vit B12; gluten intolerance | 2016 prayer and baptism by his father at the beach | Instantaneous healing | Sense of certainty of being healed during baptism |
| 41. F | Fetus with chromosomal abnormalities in pregnancy, abortion was advised | Prayer healing service, date unknown | Normal child was born, no further data | Unknown |
| 42. M | Pleural thickening, suspicion of mesothelioma (not confirmed) | 2009 prayer healing service | Sudden improve-ment of complaints, restoration of relationships with relatives; no relapse | Experience of love and peace, sure to be healed |
| 43. M | Lyme disease | Prayer healing service, date unknown | Instantaneous healing; no further data | Unknown |
| 44. F | ‘Paralysis’, no further data | Prayer healing service, date unknown | Instantaneous healing | Unknown |
| 45. F | Borderline disorder (psychiatry) | Prayer healing service, date unknown | Instantaneous healing, no further data | Unknown |
| 46. F | Hirschsprung disease, diagnosed at age 27, multiple surgeries Note: no medical data obtained. | 2001 prayer healing service | Instantaneous healing, normal bowel movement; no relapse. | Felt a touch, especially in the abdomen, a beneficent healing power |
| 47. F | Neck- and backache, abnormality cervical vertebral column (aberrant position C2) with impending spinal cord injury. | 2008 prayer healing service | Instantaneous healing; no relapseNote: no medical data obtained. | Tingling from top to toe, dizziness, coldness, as if C2 was shifting position. |
| 48. F | One sided low vision (juvenile cataract) and one sided impaired hearing post ENT surgery | 2010 prayer healing service | Instantaneous healing, no relapse. Limited data, only patient history | Feeling of embrace and warmth |
| 49. F | Pelvic instability, in wheelchair | 2000 Prayer healing service | Instantaneous healing, no relapse | Overwhelming experience |
| 50. F | Pelvic instability, fibromyalgia | 2001 Prayer healing service | Instantaneous healing, no relapse | Feeling as if hands were laid on pelvis |
| 51. M | Fibromyalgia, chronic fatigue syndrome | 1. 2005 prayer with reverend 2. 2006 prayer healing service | Healing in 2 steps, instantaneous on both occasions.No relapse | 1. Feeling of rest, peace 2. Feeling of warmth, pain instantly gone |
| 52. F | Fibromyalgia since 42 years | +/− 2014 Prayer healing service | Instantaneous healing | Feeling of warmth in body, pain gone. |
| 53. Mother, son, daughter | Migrant family with multiple diseases: deaf, diabetes, asthma, depression, ‘broken’ arm (no medical data) | Prayer healing service, date unknown | Instantaneous healing of diseases in 3 family members at the same time. | Unknown |
| 54. F | Snapping/slipping hip, longstanding backache | 2009 Prayer healing service | Instantaneous healing when standing in the line before the prayer. No relapse. | Touch in the side of the body and the back, ‘moved in her soul’. |
| 55. F | Several diseases: Chronic leukemia, asthma, uterine prolapse and other problems | Prayer team; Dates unknown | Several healings. Passed away, reason unknown. Note: no medical data obtained. | Vision about wine and holy communion |
| 56. F | Cervical cancer (in situ?), other problems (sinusitis, meniscus). Note: no medical data obtained. | 1989–1991 prayer group | PAP smears became normal, other conditions healed | Visions of Jesus |
| Manifestations | n= |
|---|---|
| Strong emotions/incessant crying | 13 |
| A sensation of being touched * | 13 |
| A sensation of warmth | 12 |
| Experience of quiet/love/peace/support | 9 |
| A current or wave through the body/paresthesia | 8 |
| A vision or strong meaningful dreams | 7 |
| A bright light | 3 |
| Internal fight between good and bad | 2 |
| Strong sensation of God’s presence/angel | 2 |
| Falling (in the Spirit) | 2 |
| Levitation (being lifted from floor or bed) | 2 |
| Wind in a closed room | 2 |
| Others nearby having sensations as well | 2 |
| Feeling of intense gladness | 2 |
| Feeling as if sickness is pulled out of body | 2 |
| Shivering/trembling | 2 |
| A feeling of being liberated | 1 |
| Course of Healing | TOTAL | Manifestations Associated with Healing (Physical, Emotional) | ||||||
|---|---|---|---|---|---|---|---|---|
| YES | NO | UNKNOWN | ||||||
| EV n = 28 | ALL n = 84 | EV | ALL | EV | ALL | EV | ALL | |
| Instantaneous onset | 23 | 61 | 20 | 43 | 3 | 5 | 0 | 13 |
| Gradual recovery | 2 | 12 | 2 | 5 | 0 | 3 | 0 | 4 |
| Unknown | 3 | 11 | 1 | 3 | 2 | 2 | 0 | 6 |
| 28 * | 84 * | 23 | 51 | 5 | 10 | 0 | 23 | |
| Level of Expectation | All Healings (n = 84) * | Subgroup Evaluated Healings (n = 28) * |
|---|---|---|
| None | 25 | 12 |
| Low | 11 | 7 |
| Moderate | 7 | 3 |
| High | 10 | 5 |
| N/A (newborn, comatose) | 3 | 1 |
| Unknown | 28 | 0 |
| Explanation of Healing | All Cases (n = 83) | Subgroup Evaluated Cases (n = 27) |
|---|---|---|
| It was God | 48 | 25 |
| Higher power | 3 | 0 |
| God and/or a physical mechanism | 2 | 1 |
| God and a positive drive | 1 | 1 |
| God and/or Mary | 1 | 0 |
| Doubting (after relapse) | 2 | 0 |
| Unknown (no data) | 26 | 0 |
| Subject Investigated | Outcome | Follow-Up Study 2019 n = 56 * | Follow-Up Study 2021 n = 59 * |
|---|---|---|---|
| Health outcome | Complete healing | 43 | 50 ** |
| Incomplete healing | 11 | 2 | |
| (Partial) relapse | 2 | 7 | |
| Outcome of socio-religious quality of life (QOL) | QOL improved | 42 | 45 |
| QOL unchanged | 13 | 12 | |
| QOL decreased | 1 | 2 |
| Frequency of Reported Positive Effects on Socio-Religious Life | 2019 | 2021 |
|---|---|---|
| Sharing the healing experience, talking about faith more easily | 15 | 12 |
| Deepening of faith | 8 | 20 * |
| More active (or newly active) in church | 7 | 8 ** |
| Increased social activities, helping others | 6 | 10 ** |
| Closer to God, ‘permeated by his love’ | 4 | 3 |
| Deepening of prayer life/praying for sick people | 4 | 17 * |
| Strengthening (confirmation) of faith | 2 | 12 * |
| Writing books | 2 | 1 |
| Missionary activities | 2 | 6 ** |
| Increased activities in coaching/pastoral care | 2 | 4 ** |
| Restoration of relationships (relief of bitterness) | 2 | 5 ** |
| Bible school | 1 | 0 |
| Different view on healing | 1 | 0 |
| Self-confirmation (increased awareness of own strength) | 1 | 3 |
| Strong wish to know more about God/Bible | 0 | 5 |
| After healing it was more easy to empathize with people having a chronic disease | 0 | 1 |
| Frequency of Reported Negative Effects on Socio-Religious Life | 2019 | 2021 |
|---|---|---|
| (Partial) bitterness because of difficult life events in the years after healing | 0 | 3 |
| Bitterness after relapse | 1 | 0 |
| Negative experiences in church/with Christians after healing | 17 * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kruijthoff, D.; Bendien, E.; Kooi, K.v.d.; Glas, G.; Abma, T. Prayer and Healing: A Study of 83 Healing Reports in the Netherlands. Religions 2022, 13, 1056. https://doi.org/10.3390/rel13111056
Kruijthoff D, Bendien E, Kooi Kvd, Glas G, Abma T. Prayer and Healing: A Study of 83 Healing Reports in the Netherlands. Religions. 2022; 13(11):1056. https://doi.org/10.3390/rel13111056
Chicago/Turabian StyleKruijthoff, Dirk, Elena Bendien, Kees van der Kooi, Gerrit Glas, and Tineke Abma. 2022. "Prayer and Healing: A Study of 83 Healing Reports in the Netherlands" Religions 13, no. 11: 1056. https://doi.org/10.3390/rel13111056
APA StyleKruijthoff, D., Bendien, E., Kooi, K. v. d., Glas, G., & Abma, T. (2022). Prayer and Healing: A Study of 83 Healing Reports in the Netherlands. Religions, 13(11), 1056. https://doi.org/10.3390/rel13111056