Impact of Islam-Based Caring Intervention on Spiritual Well-Being in Muslim Women with Breast Cancer Undergoing Chemotherapy



Abstract
1. Introduction
2. Methods
2.1. Study Design
2.2. Participants and Setting
2.3. Materials
2.4. Procedures
2.5. Data Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Aisyah, Popy Siti. 2017. The correlation between being deeply absorbed in shalat with adaptation to illness in breast cancer patients undergoing chemotherapy. Paper presented at International Nursing Workshop and Conference on Professional Nursing Practice in Free Trade Era: Threat and Challenge, Surabaya, Indonesia, December 6–8; pp. 1–10. [Google Scholar]
- Al-Natour, Ahlam, Sharaf Mohammed Al Momani, and Abeer MA Qandil. 2017. The relationship between spirituality and quality of life of Jordanian women diagnosed with breast cancer. Journal of Religion and Health 56: 2096–108. [Google Scholar] [CrossRef]
- Aranda, Sanchia, P. Schofield, Lea Weih, D. Milne, P. Yates, and R. Faulkner. 2006. Meeting the support and information needs of women with advanced breast cancer: A randomised controlled trial. The British Journal of Cancer 95: 667–73. [Google Scholar] [CrossRef]
- Bai, Mei, and Mark Lazenby. 2015. A systematic review of associations between spiritual well-being and quality of life at the scale and factor levels in studies among patients with cancer. Journal of Palliative Medicine 18: 286–98. [Google Scholar] [CrossRef] [PubMed]
- Balaguer, Albert, Cristina Monforte-Royo, Josep Porta-Sales, Alberto Alonso-Babarro, Rogelio Altisent, Amor Aradilla-Herrero, and Mercedes Bellido-Pérez. 2016. An international consensus definition of the wish to hasten death and its related factors. PLoS ONE 11: 0146184. [Google Scholar] [CrossRef]
- Battaglini, C. L., J. P. Mihalik, Martim Bottaro, C. Dennehy, M. A. Petschauer, L. S. Hairston, and E. W. Shields. 2008. Effect of exercise on the caloric intake of breast cancer patients undergoing treatment. Brazilian Journal of Medical and Biological Research 41: 709–15. [Google Scholar] [CrossRef] [PubMed]
- Caldeira, Sílvia, Fiona Timmins, Emília Campos de Carvalho, and Margarida Vieira. 2017. Spiritual well-being and spiritual distress in cancer patients undergoing chemotherapy: Utilizing the SWBQ as component of holistic nursing diagnosis. Journal of Religion and Health 56: 1489–502. [Google Scholar] [PubMed]
- Cella, David F., David S. Tulsky, George Gray, Bernie Sarafian, Elizabeth Linn, Amy Bonomi, and Margaret Silberman. 1993. The Functional Assessment of Cancer Therapy scale: Development and validation of the general measure. Journal of Clinical Oncology 11: 570–79. [Google Scholar] [CrossRef]
- Chimluang, Janya, Sureeporn Thanasilp, Lanchasak Akkayagorn, Ratchaneekorn Upasen, Noppamat Pudtong, and Wilailuck Tantitrakul. 2017. Effect of an intervention based on basic Buddhist principles on the spiritual well-being of patients with terminal cancer. European Journal of Oncology Nursing 31: 46–51. [Google Scholar] [CrossRef]
- Côté, Andréanne, and Serge Daneault. 2012. Effect of yoga on patients with cancer: Our current understanding. Canadian Family Physician 58: 475–9. [Google Scholar]
- Cramer, H., R. Lauche, A. Paul, and G. Dobos. 2012. Mindfulness-based stress reduction for breast cancer—A systematic review and meta-analysis. Current Oncology 19: 343–52. [Google Scholar] [CrossRef]
- crossroadshospice.com. 2020. Crossroads Hospice: End-of-Life Family Care Services. Available online: www.crossroadshospice.com (accessed on 29 June 2020).
- Delgado-Guay, Marvin O., David Hui, Henrique A. Parsons, Kathy Govan, Maxine De la Cruz, Steven Thorney, and Eduardo Bruera. 2011. Spirituality, religiosity, and spiritual pain in advanced cancer patients. Journal of Pain and Symptom Management 41: 986–94. [Google Scholar] [CrossRef]
- DeSantis, Carol E., Freddie Bray, Jacques Ferlay, Joannie Lortet-Tieulent, Benjamin O. Anderson, and Ahmedin Jemal. 2015. International variation in female breast cancer incidence and mortality rates. Cancer Epidemiology and Prevention Biomarkers 24: 1495–506. [Google Scholar] [CrossRef] [PubMed]
- Fallah, R., M. Golzari, M. Dastani, and M. E. Akbari. 2011. Integrating spirituality into a Group Psychotherapy Program for women surviving from breast cancer. Iranian Journal of Cancer Prevention 4: 141–47. [Google Scholar]
- Fjorback, Lone Overby, Mikkel Arendt, Eva Ørnbøl, Per Fink, and Harald Walach. 2011. Mindfulness-Based Stress Reduction and Mindfulness-Based Cognitive Therapy—A systematic review of randomized controlled trials. Acta Psychiatrica Scandinavica 124: 102–19. [Google Scholar] [CrossRef] [PubMed]
- Hassanzade, Ramezan, Ghasem Janbabaei, Mojgan Salavati, F. Moonesi, Sara Khaleghi, and Hasan Siamian. 2012. Evaluation of group-therapy efficacy by cognitive-behavioral therapy method for promoting general health among breast cancer patients. Health Med 6: 1541–46. [Google Scholar]
- Hosseini, Leili, Farah Lotfi Kashani, Somayeh Akbari, Mohammad Esmaeil Akbari, and Saeedeh Sarafraz Mehr. 2016. The Islamic perspective of spiritual intervention effectiveness on Bio-Psychological Health Displayed by gene expression in breast cancer patients. Iranian Journal of Cancer Prevention 9: 6360. [Google Scholar] [CrossRef]
- Ijaz, Shahid, Muhammad Tahir Khalily, and Irshad Ahmad. 2017. Mindfulness in salah prayer and its association with mental health. Journal of Religion and Health 56: 2297–307. [Google Scholar] [CrossRef] [PubMed]
- Imamoğlu, Osman, and Ahmet Naci Dilek. 2016. Common benefits of prayer and yoga on human organism. International Journal of Sport Culture and Science 4: 639–51. [Google Scholar] [CrossRef]
- Ismail, Suhartini, and Urai Hatthakit. 2018. Islam-Based Caring for the harmony of life among Moslem critically Ill patients. Evidence Based Care 8: 28–38. [Google Scholar]
- Jafari, Najmeh, Ziba Farajzadegan, Ahmadreza Zamani, Fatemeh Bahrami, Hamid Emami, Amir Loghmani, and Nooshin Jafari. 2013. Spiritual therapy to improve the spiritual well-being of Iranian women with breast cancer: A randomized controlled trial. Evidence-Based Complementary and Alternative Medicine 2013: 1–9. [Google Scholar] [CrossRef]
- Kabat-Zinn, Jon. 2003. Mindfulness-based stress reduction (MBSR). Constructivism in the Human Sciences 8: 73. [Google Scholar]
- Lengacher, Cecile A., Versie Johnson-Mallard, Janice Post-White, Manolete S. Moscoso, Paul B. Jacobsen, Thomas W. Klein, and Raymond H. Widen. 2009. Randomized controlled trial of mindfulness-based stress reduction (MBSR) for survivors of breast cancer. Psycho-Oncology 18: 1261–72. [Google Scholar] [CrossRef] [PubMed]
- Lewis, Shirley, Naveen Salins, M. Raghavendra Rao, and Amrit Kadam. 2014. Spiritual well-being and its influence on fatigue in patients undergoing active cancer directed treatment: A correlational study. Journal of Cancer Research and Therapeutics 10: 676–80. [Google Scholar] [CrossRef]
- Loh, Keng Yin. 2004. Spiritual distress in a terminally ill patient with breast cancer. International Journal of Palliative Nursing 10: 131–32. [Google Scholar] [CrossRef]
- Lötzke, Désirée, Florian Wiedemann, Daniela Rodrigues Recchia, Thomas Ostermann, Daniel Sattler, Johannes Ettl, Marion Kiechle, and Arndt Büssing. 2016. Iyengar-yoga compared to exercise as a therapeutic intervention during (neo) adjuvant therapy in women with stage I–III breast cancer: health-related quality of life, mindfulness, spirituality, life satisfaction, and cancer-related fatigue. Evidence-Based Complementary and Alternative Medicine 2016: 1–8. [Google Scholar] [CrossRef]
- Martins, Helga, and Sílvia Caldeira. 2018. Spiritual distress in cancer patients: A synthesis of qualitative studies. Religions 9: 285. [Google Scholar] [CrossRef]
- Martins, Helga, Tiago Dias Domingues, and Sílvia Caldeira. 2019. Spiritual well-being in cancer patients undergoing chemotherapy in an outpatient setting: A cross-sectional study. Journal of Holistic Nursing 38: 68–77. [Google Scholar] [CrossRef]
- Martoni, A. A., S. Varani, B. Peghetti, D. Roganti, E. Volpicella, R. Pannuti, and F. Pannuti. 2017. Spiritual well-being of Italian advanced cancer patients in the home palliative care setting. European Journal of Cancer Care 26. [Google Scholar] [CrossRef]
- Nawansih, Witria Sekar, and Setiyo Purwanto. 2012. Perbedaan kekhusyukan shalat ditinjau dari jenis kelamin jama’ah halaqah shalat khusyuk. [The difference in the solemnity of prayer in terms of the sex of the congregation halaqah solemn prayer]. Paper Presented at Seminar Nasional Psikologi Islami, Surakarta, Indonesia, April 21. [Google Scholar]
- Oemiati, Ratih, Ekowati Rahajeng, and Antonius Yudi Kristanto. 2011. Prevalensi tumor dan beberapa faktor yang mempengaruhinya di Indonesia. [The prevalence of tumors and several factors that influence it in Indonesia ]. Buletin Penelitian Kesehatan 39: 190–204. [Google Scholar]
- Phenwan, Tharin, Thanarpan Peerawong, and Kandawsri Tulathamkij. 2019. The meaning of spirituality and spiritual well-being among Thai breast cancer patients: A qualitative study. Indian Journal of Palliative Care 25: 119–23. [Google Scholar] [CrossRef]
- Pok-Ja Oh, R. N., and Soo Hyun Kim. 2014. The effects of spiritual interventions in patients with cancer: A meta-analysis. Oncology Nursing Forum 41: E290–E301. [Google Scholar] [CrossRef]
- Rosmani, Arifah Fasha, Noor Azura Zainuddin, Siti Zulaiha Ahmad, and Siti Zubaida Ramli. 2015. Bio Terapi Solat: 3D Integration in Solat Technique for Therapeutic Means. In Advanced Computer and Communication Engineering Technology. Cham: Springer, pp. 1001–11. [Google Scholar]
- Sajadi, Mahbobeh, Naimeh Niazi, Sharareh Khosravi, Abolghasem Yaghobi, Mahboubeh Rezaei, and Harold G. Koenig. 2018. Effect of spiritual counseling on spiritual well-being in Iranian women with cancer: A randomized clinical trial. Complementary Therapies in Clinical Practice 30: 79–84. [Google Scholar] [CrossRef] [PubMed]
- Sayeed, Shabbir Ahmed, and Anand Prakash. 2013. The Islamic prayer (Salah/Namaaz) and yoga togetherness in mental health. Indian Journal of Psychiatry 55: 224–30. [Google Scholar] [CrossRef] [PubMed]
- Sibeoni, Jordan, Camille Picard, Massimiliano Orri, Mathilde Labey, Guilhem Bousquet, Laurence Verneuil, and Anne Revah-Levy. 2018. Patients’ quality of life during active cancer treatment: A qualitative study. BMC Cancer 18: 1–8. [Google Scholar] [CrossRef] [PubMed]
- Speca, Michael, Linda E. Carlson, Eileen Goodey, and Maureen Angen. 2000. A randomized, wait-list controlled clinical trial: The effect of a Mindfulness Meditation-Based Stress Reduction Program on mood and symptoms of stress in cancer outpatients. Psychosomatic Medicine 62: 613–22. [Google Scholar] [CrossRef] [PubMed]
- Stutzman, Hannah, and Sam Abraham. 2017. A correlational study of spiritual well-being and depression in the adult cancer patient. The Health Care Manager 36: 164–72. [Google Scholar] [CrossRef]
- Suara, Eviwindha, Mardiyono Mardiyono, and Anggorowati Anggorowati. 2017. Relationship between demographic characteristics and spiritual wellbeing among cancer survivors. Belitung Nursing Journal 3: 405–11. [Google Scholar] [CrossRef]
- Thasaneesuwan, Samonnan, Wongchan Petpichetchian, and Tippamas Chinnawong. 2018. A randomized controlled trial of a Buddhist-based Nursing Program for women with breast cancer. Pacific Rim International Journal of Nursing Research 22: 58–73. [Google Scholar]
- Villagomeza, Liwliwa R. 2005. Spiritual distress in adult cancer patients: Toward conceptual clarity. Holistic Nursing Practice 19: 285–94. [Google Scholar] [CrossRef]
- Wahyuningsih, Fefi Eka, Muchlis Achsan Udji Sofro, and Meidiana Dwidiyanti. 2019. Spiritual well being of breast cancer patients undergoing chemotherapy through Mindfulness Based Spiritual. Media Keperawatan Indonesia 2: 83–89. [Google Scholar] [CrossRef]
- Wang, Yin-Chih, and Chia-Chin Lin. 2016. Spiritual well-being may reduce the negative impacts of cancer symptoms on the quality of life and the desire for hastened death in terminally ill cancer patients. Cancer Nursing 39: 43–50. [Google Scholar] [CrossRef]
- Werdani, Yesiana Dwi Wahyu. 2018. Effect of cancer related fatigue to the level of independence of cancer patients and caregiver stress level. Folia Medica Indonesiana 54: 108–12. [Google Scholar] [CrossRef]
- Zamaniyan, Sakineh, Jafar Bolhari, Ghasem Naziri, Majid Akrami, and Sara Hosseini. 2016. Effectiveness of Spiritual Group Therapy on quality of life and spiritual well-being among patients with breast cancer. Iranian Journal of Medical Sciences 41: 140–4. [Google Scholar] [PubMed]
- Zhang, Jun, Rui Xu, Bo Wang, and Jinxia Wang. 2016. Effects of mindfulness-based therapy for patients with breast cancer: A systematic review and meta-analysis. Complementary Therapy Medicine 26: 1–10. [Google Scholar] [CrossRef] [PubMed]
| 1 | Dhikr refers to divine remembrance, methodical repetitions of the divine name with prayer beads, and the repetition of devotional poems and Quranic formulas. |
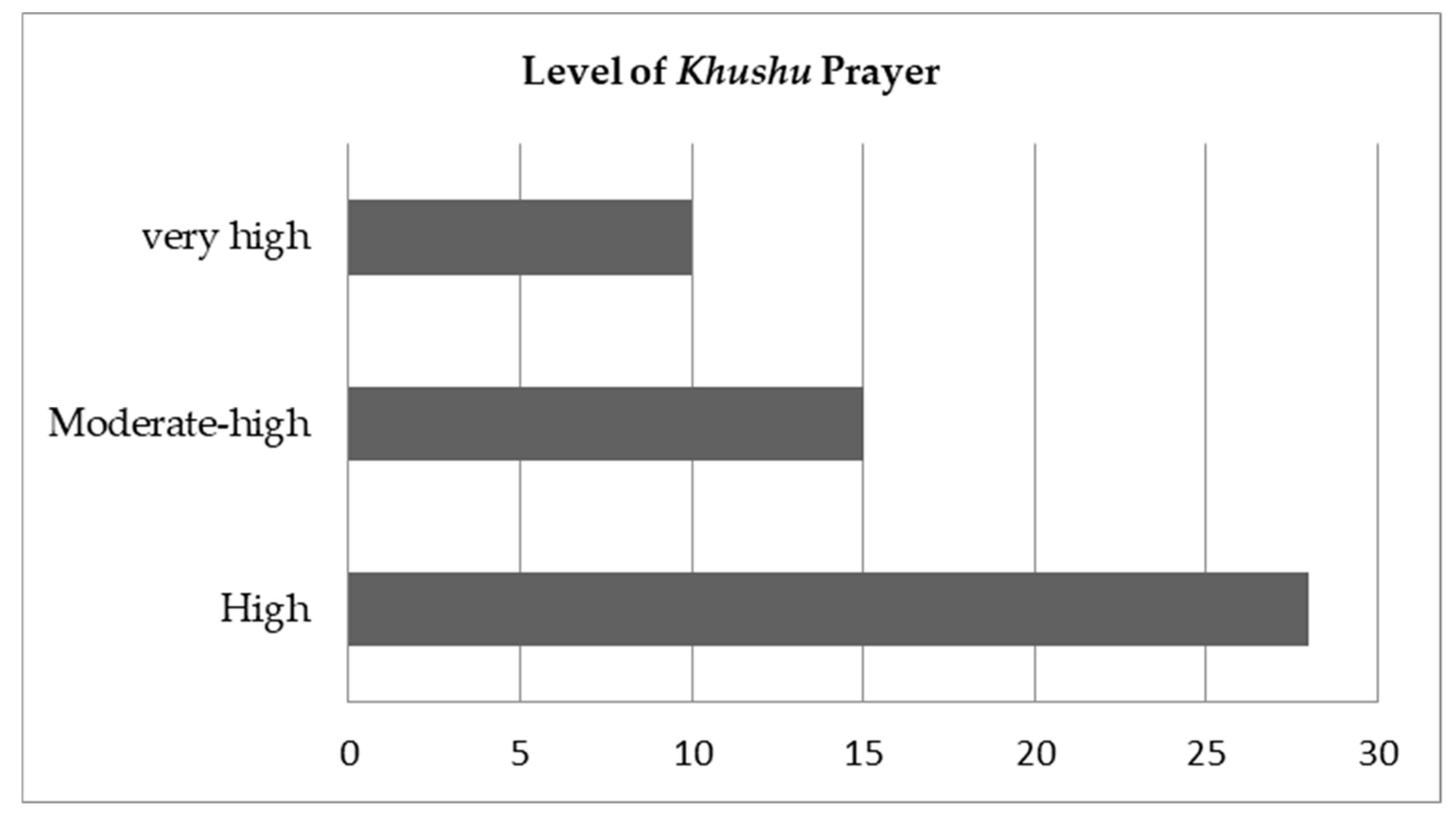
| 2 | Khushu refers to performing prayers quietly, focusing one’s mind only on God. |



{kind=link}
{kind=link}
| Variable | Intervention Group n = 53 | Control Group n = 59 | Statistics Test | p-Value |
|---|---|---|---|---|
| Age (Mean/SD) | 47.51(7.74) | 46.83(8.60) | −0.44 a | 0.66 |
| Education | ||||
| Primary | 28(52.8) | 34(57.6) | 0.26 | 0.88 c |
| High school | 21(39.6) | 21(35.6) | ||
| University | 4(7.6) | 4(6.8) | ||
| Occupation | ||||
| Unemployed | 35(66.0) | 39(66.1) | 0.00 | 1.00 b |
| Employed | 18(34.0) | 20(33.9) | ||
| Marital status | ||||
| Single | 3(5.7) | 1(1.7) | 1.33 | 0.52 c |
| Married | 41(77.3) | 48(81.4) | ||
| Widow | 9(17.0) | 10(16.9) | ||
| Number of children | ||||
| 0–2 | 34(64.2) | 31(52.5) | 1.55 | 0.21 b |
| 3–5 | 19(35.8) | 28(47.5) | ||
| Family income | ||||
| Adequate | 45(84.9) | 46(78.0) | 0.88 | 0.35 b |
| Inadequate | 8(15.1) | 13(22.0) | ||
| Medical History | ||||
| Breast cancer staging | ||||
| IIIa | 13(24.5) | 23(39.0) | 3.53 | 0.17 c |
| IIIb | 37(69.8) | 31(52.5) | ||
| IIIc | 3(5.7) | 5(4.5) | ||
| Surgical treatment | ||||
| No | 31(58.5) | 36(61.0) | 0.07 | 0.79 b |
| Yes | 22(41.5) | 23(39.0) | ||
| Chemotherapy treatment | ||||
| FAC | 43(81.1) | 47(79.7) | 0.05 | 0.98 c |
| TAC | 6(11.3) | 7(11.8) | ||
| AC + paclitaxel | 4(7.6) | 5(8.5) | ||
| Chemotherapy cycle | ||||
| 1 | 22(41.5) | 20(33.9) | 3.54 | 0.32 b |
| 2 | 12(22.6) | 23(39.0) | ||
| 3 | 9(17.0) | 7(11.9) | ||
| 4 | 10(18.9) | 9(15.2) | ||
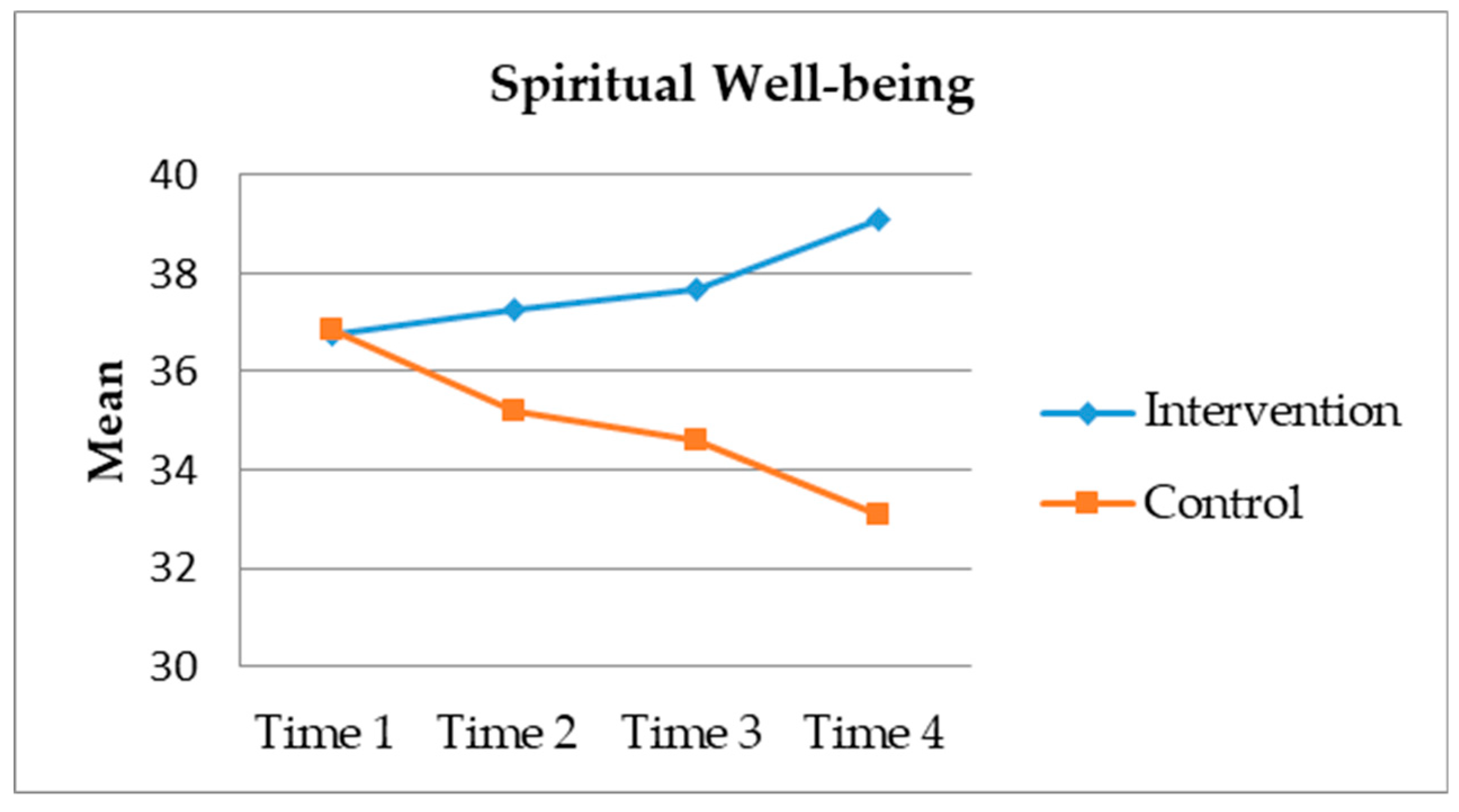
| Time | Group | p | |
|---|---|---|---|
| Intervention (n = 53) | Control (n = 59) | ||
| Mean (SD) | Mean (SD) | ||
| Time 1 | 36.77(3.67) | 36.86(5.57) | 0.918 |
| Time 2 | 37.25(5.22) | 35.19(5.80) | 0.042 * |
| Time 3 | 37.66(5.77) | 34.61(7.10) | 0.015 * |
| Time 4 | 39.09(4.81) | 33.08(7.24) | 0.000 ** |
| SWB | Gr | Time 1 | p | Time 2 | p | Time 3 | p | Time 4 | p |
|---|---|---|---|---|---|---|---|---|---|
| Mean (SD) | Mean (SD) | Mean (SD) | Mean (SD) | ||||||
| I feel peaceful. | In | 2.85(0.74) | 0.039 * | 2.70(0.93) | 0.194 | 2.75(0.90) | 0.048 * | 3.09(0.66) | 0.000 ** |
| Ct | 2.53(0.90) | 2.47(0.88) | 2.42(0.86) | 2.20(1.03) | |||||
| I have a reason for living. | In | 3.45(0.61) | 0.562 | 3.57(0.84) | 0.845 | 3.53(0.61) | 0.187 | 3.66(0.48) | 0.000 ** |
| Ct | 3.53(0.70) | 3.59(0.62) | 3.34(0.86) | 3.22(0.79) | |||||
| My life has been productive. | In | 2.81(0.81) | 0.072 | 2.58(0.99) | 0.143 | 2.64(0.86) | 0.048 * | 2.92(0.76) | 0.001 * |
| Ct | 2.51(0.95) | 2.32(0.90) | 2.64(0.86) | 2.37(0.87) | |||||
| I have trouble feeling peace of mind (reversed). | In | 2.91(0.97) | 0.466 | 2.96(0.98) | 0.138 | 2.83(1.07) | 0.803 | 3.11(0.99) | 0.001 * |
| Ct | 2.76(1.09) | 2.66(1.15) | 2.78(1.07) | 2.51(0.94) | |||||
| I feel a sense of purpose in my life. | In | 3.11(0.64) | 0.425 | 3.15(0.91) | 0.323 | 3.28(0.84) | 0.082 | 3.23(0.77) | 0.005 * |
| Ct | 3.00(0.83) | 2.98(0.88) | 2.98(0.96) | 2.81(0.75) | |||||
| I am able to reach down deep into myself for comfort. | In | 2.77(0.78) | 0.235 | 2.87(0.81) | 0.001 * | 2.98(0.82) | 0.040 * | 2.92(0.78) | 0.000 ** |
| Ct | 2.58(0.97) | 2.32(0.88) | 2.47(1.02) | 2.31(0.89) | |||||
| I feel a sense of harmony within myself. | In | 2.66(0.94) | 0.483 | 2.53(0.80) | 0.193 | 2.81(0.86) | 0.016 * | 2.94(0.66) | 0.000 ** |
| Ct | 2.53(1.09) | 2.32(0.86) | 2.41(0.89) | 2.34(0.84) | |||||
| My life lacks meaning and purpose (reversed). | In | 3.15(0.95) | 0.060 | 3.42(1.13) | 0.586 | 3.51(0.93) | 0.127 | 3.83(0.85) | 0.001 * |
| Ct | 3.53(1.12) | 3.53(1.01) | 3.19(1.28) | 3.15(1.19) | |||||
| I find comfort in my faith or spiritual beliefs. | In | 3.13(0.65) | 0.002 * | 3.30(0.88) | 0.576 | 3.28(0.66) | 0.205 | 3.30(0.72) | 0.022 * |
| Ct | 3.53(0.65) | 3.20(1.01) | 3.10(0.82) | 2.92(1.02) | |||||
| I find strength in my faith or spiritual beliefs. | In | 3.36(0.65) | 0.012 * | 3.34(0.73) | 0.421 | 3.36(0.56) | 0.177 | 3.30(0.75) | 0.127 |
| Ct | 3.53(0.68) | 3.20(1.01) | 3.19(0.75) | 3.05(0.95) | |||||
| My illness has strengthened my faith or spiritual beliefs. | In | 3.43(0.67) | 0.368 | 3.42(0.60) | 0.071 | 3.30(0.67) | 0.571 | 3.36(0.62) | 0.021 * |
| Ct | 3.44(0.84) | 3.14(0.99) | 3.22(0.83) | 3.00(0.95) | |||||
| I know that whatever happens with my illness, things will be okay. | In | 3.51(0.64) | 0.823 | 3.42(0.60) | 0.838 | 3.38(0.63) | 0.252 | 3.42(0.63) | 0.080 |
| Ct | 3.42(0.75) | 3.44(0.75) | 3.20(0.92) | 3.17(0.81) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Komariah, M.; Hatthakit, U.; Boonyoung, N. Impact of Islam-Based Caring Intervention on Spiritual Well-Being in Muslim Women with Breast Cancer Undergoing Chemotherapy. Religions 2020, 11, 361. https://doi.org/10.3390/rel11070361
Komariah M, Hatthakit U, Boonyoung N. Impact of Islam-Based Caring Intervention on Spiritual Well-Being in Muslim Women with Breast Cancer Undergoing Chemotherapy. Religions. 2020; 11(7):361. https://doi.org/10.3390/rel11070361
Chicago/Turabian StyleKomariah, Maria, Urai Hatthakit, and Nongnut Boonyoung. 2020. "Impact of Islam-Based Caring Intervention on Spiritual Well-Being in Muslim Women with Breast Cancer Undergoing Chemotherapy" Religions 11, no. 7: 361. https://doi.org/10.3390/rel11070361
APA StyleKomariah, M., Hatthakit, U., & Boonyoung, N. (2020). Impact of Islam-Based Caring Intervention on Spiritual Well-Being in Muslim Women with Breast Cancer Undergoing Chemotherapy. Religions, 11(7), 361. https://doi.org/10.3390/rel11070361