Implementing “Link Nurses” as Spiritual Care Support in a General Hospital


Abstract
1. Introduction
1.1. Background and Problem
1.2. Research Questions
- (1)
- What are patient and nurse perspectives on spiritual care before and after implementation of a multidimensional strategy to support spiritual care practice by nurses in a general hospital?
- (2)
- What is the spiritual care competence development of nurses and spiritual care link nurses after the same strategy?
- (3)
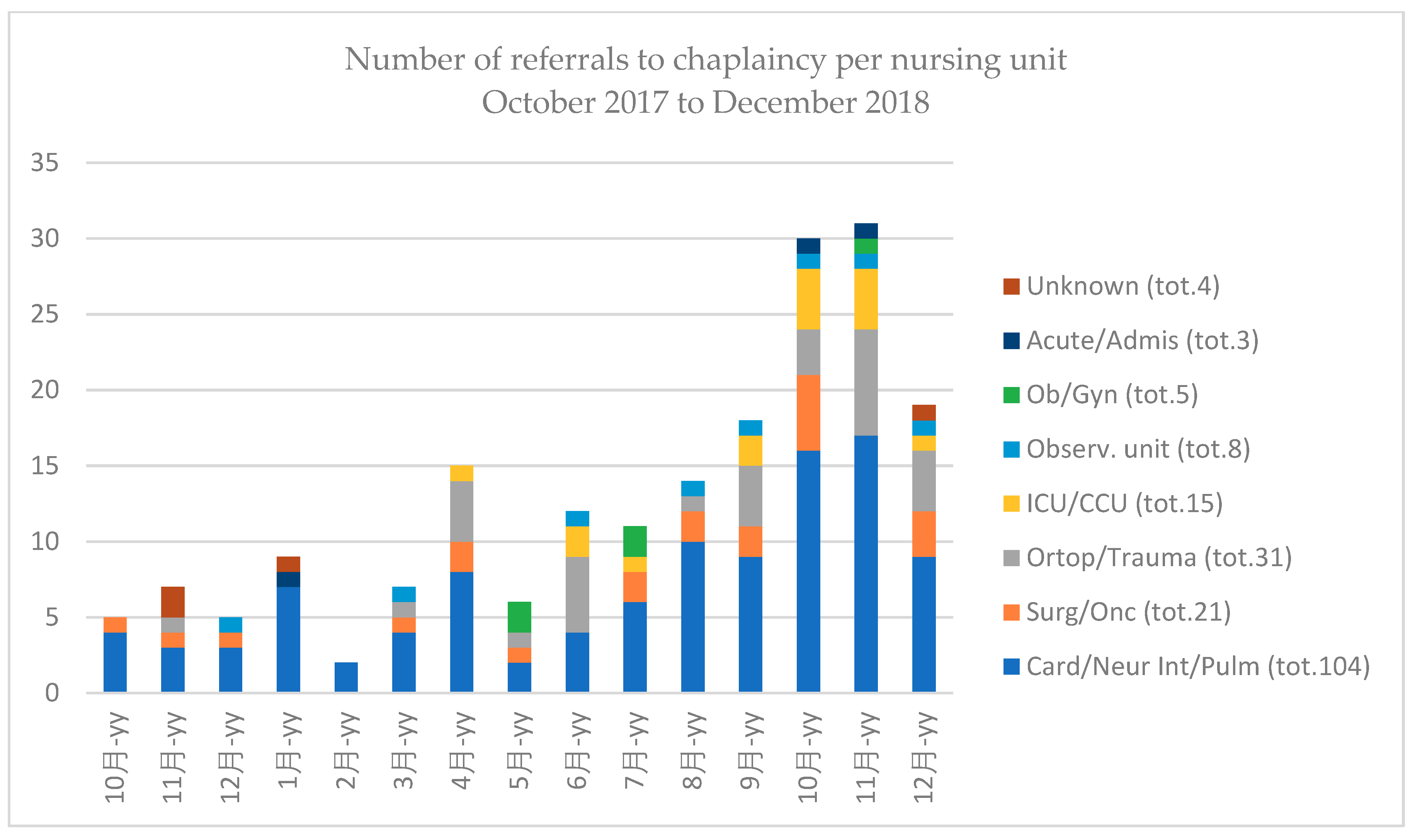
- What is the development in patient referral to chaplaincy after the same strategy?
1.3. Intervention
2. Method
2.1. Design and Samples
2.2. Data Collection
2.3. Analysis
2.4. Ethical Approval
3. Results
3.1. Patients
- -
- “They are friendly, professional and hardworking people”;
- -
- “I am grateful for the love that shows from the care they provide”;
- -
- “Nurses truly put their heart and soul into their work”;
- -
- “They do what they’re trained for and do it with kindness and an encouraging word. The same goes for the chaplain”.
- -
- “They’re very busy and rushed and seem understaffed”;
- -
- “Organization and communication in the unit leaves something to be desired”;
- -
- “Some should show more tact and manners. Some of them seem to be working too much on automatic pilot”;
- -
- “It wasn’t always made clear to me what was waiting for me, which made me anxious and irritable”.
3.2. Nurse Competence
3.3. Nurses: Follow-Up Focus Group
- -
- “What about continuity? If we do not keep bringing spiritual care to each other’s attention, if only in team meetings and evaluations every six months or so, then what? And why were the medical staff not involved?”;
- -
- “Case deliberation in our own team would be helpful. The link nurse could prepare this”;
- -
- “We need to make contact with the link nurse, familiarize ourselves with what she is doing”;
- -
- “Management/administration should make more time available for e-learning and make spiritual care part of the regular educational programs of the hospital. Also, this e-learning course it too long”;
- -
- “The objectives and content of education should be introduced much clearer beforehand”;
- -
- “Include more information of world religions and cultural differences”.
3.4. Link Nurses: Competency Scale
3.5. Link Nurses: Follow-Up Focus Group
- -
- “The whole project set something in motion; if the goal was to raise awareness, it succeeded. The topic is being addressed more openly now”;
- -
- “We became more aware of the need to really be there for the patient, it forced us to sit down and think how to put it into practice”;
- -
- “The chaplain was a positive factor in the spiritual care to both patients and nurses”;
- -
- “We now see more and better reports of patient–nurse interaction on spirituality. The use of model questions was a big help for intake as well as probing spirituality later on”.
- -
- “There was more than a little grumbling and opposition during the project, a hostile reception even”;
- -
- “It was required of us on top of everything else, and it cost a lot of time, it was burdensome”;
- -
- “We did not see the point, as we were in fact already doing it”;
- -
- “It was unclear if spirituality was seen as religious or as something broader”;
- -
- “The objectives of the project were communicated insufficiently, the hospital gave it too little support, was this what the board wanted with its Christian heritage?”.
- -
- “As LNSC, we should meet as a group at least twice a year, together with the steering group and the chaplain, to compare notes and develop expertise”;
- -
- “Continuity of the link nurse’s role should be secured in the unit’s policy, meaning when one resigns another is appointed. The head nurse and senior nurses obviously have to be behind it”;
- -
- “Continuing education for link nurses should be provided after the project”;
- -
- “Make educational strategies more interactive (attuned to the experiences and development to my own team), more customized (attuned to the medical specialty and patient category of my own unit), and even more practical (attuned to the needs of the individual patient)”;
- -
- “I want to motivate my colleagues in a natural way: how to do that?”;
- -
- “How am I supposed to move forward with the SWOT analysis and plan for improvement in the longer run? What are the objectives in the long run?”;
- -
- “It was important to ask the chaplain to join patient consultations. We need to formalize this way of working. It lowers the threshold to consult him”.
3.6. Chaplaincy
4. Discussion
4.1. Practice
4.2. Intervention
- -
- Anticipating resistance to change is key: management of expectations and sharing information on objectives and activities at all levels of the organization were not recognized by all nurses and link nurses.
- -
- Involving support staff (education, communication) and leadership is key: the role of head nurses and the PR department as well as communication was not recognized by all nurses and link nurses.
- -
- Repeating, fine-tuning and/or supplementing activities involved in the project is key: not all link nurses followed through on their own improvement plans by themselves, nor on liaising with the chaplaincy.
- -
- Participants indicated the need to feel part of a bigger whole: some nurses and link nurses felt that without involvement of all or most other health professionals in the hospital, such as midwives, social workers, and medical staff, they were not so much frontrunners but rather an odd exception in the development of professional practice.
- -
- A project like this is only possible when those formally responsible are explicitly behind it and “put their money where their mouth is”: not all nurses and link nurses recognized this as actually being the case.
4.3. Method
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Clarke, Janice, and Kath Baume. 2019. Embedding spiritual care into everyday nursing practice. Nursing Standard. [Google Scholar] [CrossRef]
- Cockell, Nell, and Wilfred McSherry. 2012. Spiritual care in nursing: An overview of published international research. Journal of Nursing Management 20: 958–69. [Google Scholar] [CrossRef] [PubMed]
- European Association of Palliative Care. 2020. Available online: https://www.eapcnet.eu/eapc-groups/reference/spiritual-care (accessed on 29 April 2020).
- EPICC. 2019. Available online: www.epicc-project.eu (accessed on 17 December 2019).
- Ferrell, Betty R., Marcia Grant, Kathie Jo Ritchey, Rebecca Ropchan, and Lynne M. Rivera. 1993. The pain resource nurse training program: A unique approach to pain management. Journal of Pain Symptom Management 8: 549–56. [Google Scholar] [CrossRef]
- Leget, Carlo. 2017. Art of Living, Art of Dying. London: Jessica Kingsley Publishers. [Google Scholar]
- Legg, Melanie, Anne Cleary, Joanne Shackelton, and Sylvie Hampton. 2017. P-288 Establishing Link Nurse roles to enhance leadership, knowledge and development. BMJ Supportive and Palliative Care 7 Suppl. S2: A113. [Google Scholar]
- Lo, Chung Kwan. 2018. Grounding the flipped classroom approach in the foundations of educational technology. Educational Technology Research and Development 66: 793–811. [Google Scholar] [CrossRef]
- McSherry, W., and L. Ross. 2012. Nursing. In Oxford Textbook of Spirituality in Healthcare. Edited by Mark Cobb, Christina Puchalski and Bruce Rumbold. New York: Oxford Press. [Google Scholar]
- NHS Scotland. 2010. Spiritual Care Matters: An Introductory Source for All NHS Scotland Staff. Available online: https://www.nes.scot.nhs.uk/media/3723/spiritualcaremattersfinal.pdf (accessed on 29 April 2020).
- Puchalski, Christina, Betty Ferrell, Rose Virani, Shirley Otis-Green, Pamela Baird, Janet Bull, Harvey Chochinov, George Handzo, Holly Nelson-Becker, Maryjo Prince-Paul, and et al. 2009. Improving the quality of spiritual care as a dimension of palliative care: The report of the consensus conference. Journal of Palliative Medicine 12: 885–904. [Google Scholar] [CrossRef] [PubMed]
- Raile Alligood, Martha Raile. 2017. Nursing Theorists and Their Work, 9th ed. Edinburgh, London and Oxford: Elsevier Health Europe. [Google Scholar]
- Rychen, Dominique Simone, and Laura Hersh Salganik. 2002. Definition and Selection of Competencies (DESECO): Theoretical and Conceptual Foundations. Strategy Paper. Neuchâtel: Organisation for Economic Co-operation and Development (OECD). [Google Scholar]
- Snowden, Austyn, and Iain Telfer. 2017. Patient Reported Outcome Measure of Spiritual Care as Delivered by Chaplains. Journal of Healthcare Chaplaincy 23: 131–55. [Google Scholar] [CrossRef] [PubMed]
- Van Leeuwen, René, Lucas J. Tiesinga, Berrie Middel, Doeke Post, and Henk Jochemsen. 2009. The validity and reliability of an instrument to assess nursing competencies in spiritual care. Journal of Clinical Nursing 18: 2857–69. [Google Scholar] [CrossRef] [PubMed]
- Vlasblom, Jan P. 2015. Spiritual Care by Nurses and the Role of the Chaplaincy in a General Hospital. Ph.D. Thesis, Vrije Universiteit Amsterdam, Amsterdam, The Netherlands. [Google Scholar]
- Vogel, Annemieke, and Annemiek E. Schep-Akkerman. 2018. Competence and frequency of provision of spiritual care by nurses in the Netherlands. Scandinavian Journal of Caring Sciences 32: 1314–21. [Google Scholar] [CrossRef] [PubMed]
- White, Carole L. 2011. Nurse champions: A key role in bridging the gap between research and practice. Journal of Emergency Nursing 37: 386–87. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| General Nursing Competencies for Spiritual Care | |
| A | Attitude towards patients’ spirituality |
| B | Communication |
| C | Personal support and patient counseling |
| D | Assessment and planning of spiritual care |
| E | Referral to other professionals |
| F | Professionalization and improving the quality of spiritual care |
| Additional Competencies for Link Nurses Spiritual Care | |
| G | Embedding spiritual care in the primary process on the unit |
| H | Supporting and coaching team members in spiritual care |
| I | Working and collaborating inside and outside the organization |
| J | Contributing to the profession |
| Time | Intervention | Participants * | Content | Modus Operandi | Monitoring |
|---|---|---|---|---|---|
| May 2017 | Explorative interviews | ||||
| Oct 2017 | Start of data collection referral | ||||
| Nov 2017 | Introduction to educational intervention | LNSC | Overview role, competencies, e-learning course and meetings | ||
| Jan 2018 | First workshop | LNSC | Being a champion: “dreaming, thinking and doing” | Teaching and assignment | Baseline measurement |
| Feb 2018 | First seminar | Nurses | Interpersonal and intrapersonal spirituality: “me, you and us” | Teaching and discussion | |
| Mar 2018 | Start of e-learning course | Nurses | Spiritual care competencies | ||
| Apr 2018 | Second workshop | LNSC | Acting as a champion: “practice development” | Teaching and assignment | |
| May 2018 | Second seminar | Nurses | Spiritual care: assessing, planning and supporting | Teaching and exercise | |
| Aug 2018 | End of e-learning course | Nurses | Follow-up measurement | ||
| Sept 2018 | Nurses | Concluding interviews | |||
| Nov 2018 | Final Symposium | Nurses | Learning outcomes | Pitches | |
| Dec 2018 | Finalize data collection referral |
| During My Stay * | Before (n = 131) | After (n = 122) | p-Value MW-Test |
|---|---|---|---|
| I was listened to | 95% ** (128) | 98% (121) | 0.89 |
| I was able to talk about what was on my mind | 95% (126) | 96% (121) | 0.32 |
| My situation was understood | 91% (127) | 95% (122) | 0.42 |
| My faith/beliefs were valued | 98% (114) | 92% (110) | 0.40 |
| SCCS, Mean Score * | LNSC | Nurses | ||||
|---|---|---|---|---|---|---|
| Before (n = 15) | After (n = 18) | p-Value MW-Test | Before (n = 123) | After (n = 86) | p-Value MW-Test | |
| Assessment and planning | 3.7 | 3.9 | 0.12 | 3.6 ** | 3.8 ** | 0.01 ** |
| Professionalization and quality assurance | 3.1 | 3.4 | 0.06 | 3.0 | 3.3 | 0.08 |
| Personal support and patient counseling | 3.7 | 4.0 | 0.11 | 3.6 ** | 3.9 ** | 0.00 ** |
| Referral to other professionals | 3.9 ** | 4.1 ** | 0.04 ** | 3.8 ** | 4.0 ** | 0.02 ** |
| Attitude towards patients’ spirituality | 4.1 | 4.3 | 0.16 | 4.3 | 4.3 | 0.70 |
| Communication | 4.3 | 4.3 | 0.63 | 4.3 | 4.3 | 0.90 |
| Nursing Competencies for Spiritual Care in Link Nurses, Mean Score Per Item * | Before (n = 15) | After (n = 18) | p-Value MW-Test |
|---|---|---|---|
| Professionalization and quality assurance in the role as a link nurse | |||
| I can contribute to the improvement of my colleagues’ expertise regarding spiritual care to patients | 3.0 ** | 3.8 ** | 0.01 ** |
| I can advise my team/unit on quality improvement regarding spiritual care to patients | 3.1 | 3.7 | 0.08 |
| I can develop an education program for my team/unit regarding spiritual care | 2.5 ** | 3.4 ** | 0.01 ** |
| Referral to other professionals in the role of link nurse | |||
| I can liaise with professionals in my organization with a special role in spiritual care (chaplains, link nurses, social workers, psychologists) | 3.4 | 4.1 | 0.07 |
| I can report and hand over spiritual care to professionals in my organization with a special role in spiritual care | 3.3 | 3.7 | 0.20 |
| I can refer patients and colleagues to professionals in my organization with a special role in spiritual care | 3.5 | 4.1 | 0.08 |
| I can act as an advocate for spiritual care within my team/on my unit (as a champion or resource person). | 3.3 | 3.6 | 0.40 |
| Collaboration in the role of link nurse | |||
| I can liaise on behalf of patients or colleagues with professionals, organizations, and communities outside my own organization with a special role in spiritual care | 2.4 | 3.0 | 0.22 |
| I know world religions and value systems important in my country | 2.5 | 2.8 | 0.68 |
| Advocating spiritual care in the role of link nurse | |||
| I am able to function as a role model in spiritual care for my team/unit | 3.1 | 3.6 | 0.13 |
| I can explain the role of link nurse to members of my profession | 2.7 | 3.4 | 0.06 |
| Professionalizing and organizing in the role of link nurse | |||
| I can organize an ethics meeting or moral case deliberation for my team/unit | 3.1 | 3.4 | 0.28 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cusveller, B.; Damsma-Bakker, A.; Streefkerk, T.; van Leeuwen, R. Implementing “Link Nurses” as Spiritual Care Support in a General Hospital. Religions 2020, 11, 308. https://doi.org/10.3390/rel11060308
Cusveller B, Damsma-Bakker A, Streefkerk T, van Leeuwen R. Implementing “Link Nurses” as Spiritual Care Support in a General Hospital. Religions. 2020; 11(6):308. https://doi.org/10.3390/rel11060308
Chicago/Turabian StyleCusveller, Bart, Aliza Damsma-Bakker, Theotimus Streefkerk, and René van Leeuwen. 2020. "Implementing “Link Nurses” as Spiritual Care Support in a General Hospital" Religions 11, no. 6: 308. https://doi.org/10.3390/rel11060308
APA StyleCusveller, B., Damsma-Bakker, A., Streefkerk, T., & van Leeuwen, R. (2020). Implementing “Link Nurses” as Spiritual Care Support in a General Hospital. Religions, 11(6), 308. https://doi.org/10.3390/rel11060308