
Predicting COVID-19 Vaccination Intention: The Determinants of Vaccine Hesitancy


Abstract
:1. Introduction
2. Parental Vaccination Intention
3. Method
3.1. Participants
3.2. Materials
3.3. Ethics
3.4. Procedure
4. Data Analysis
5. Results
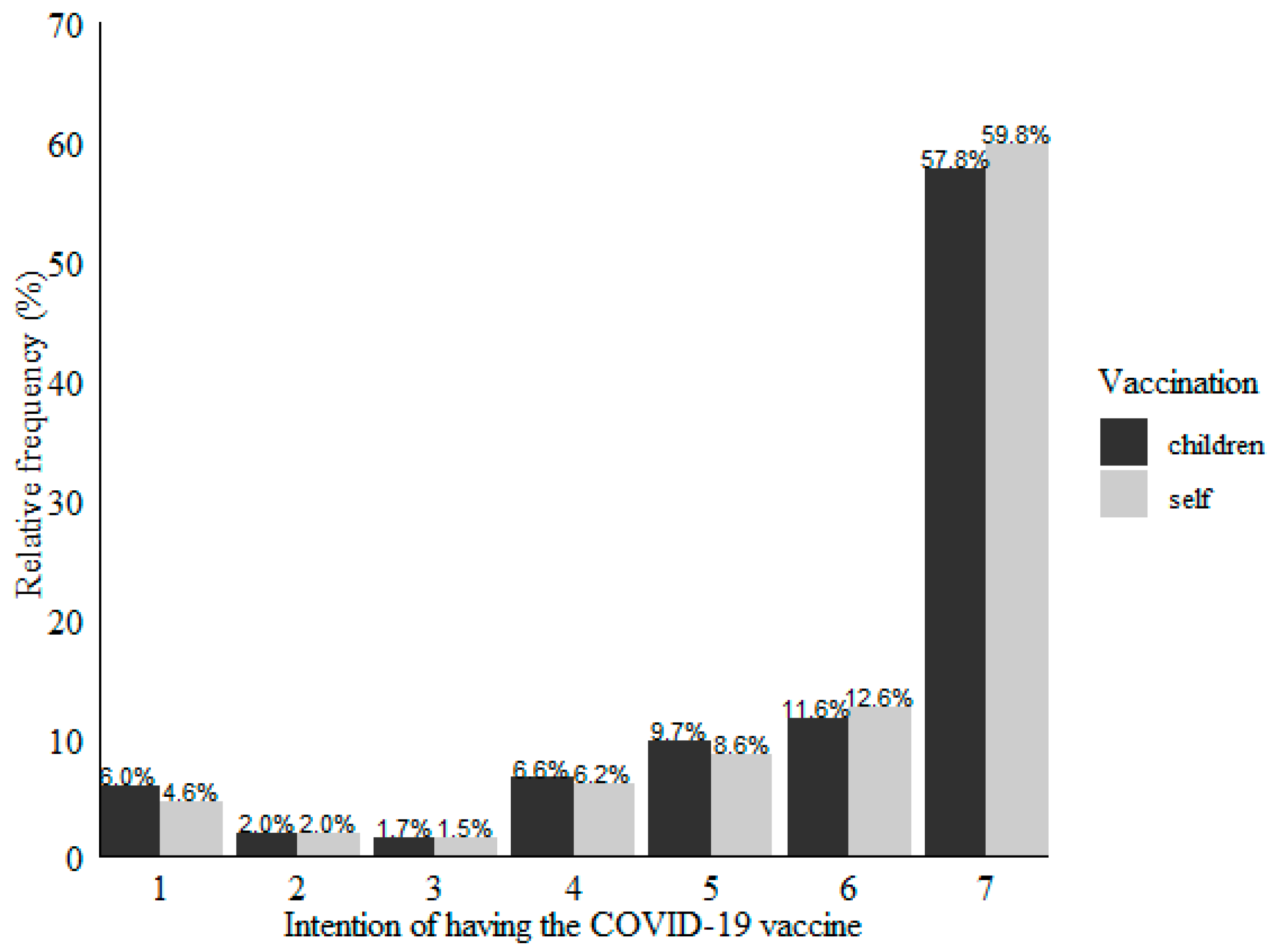
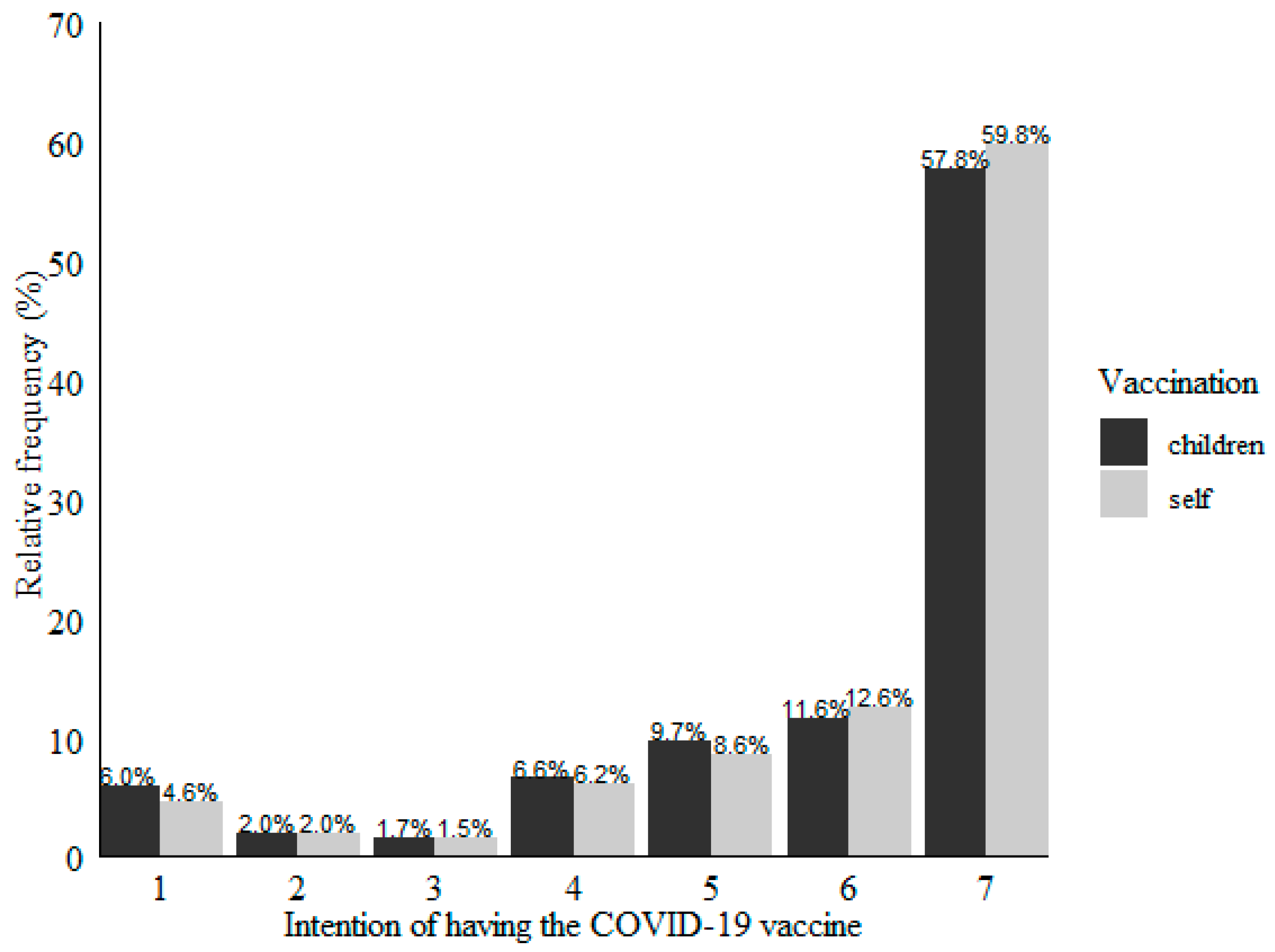
5.1. Self and Children Vaccination Intention
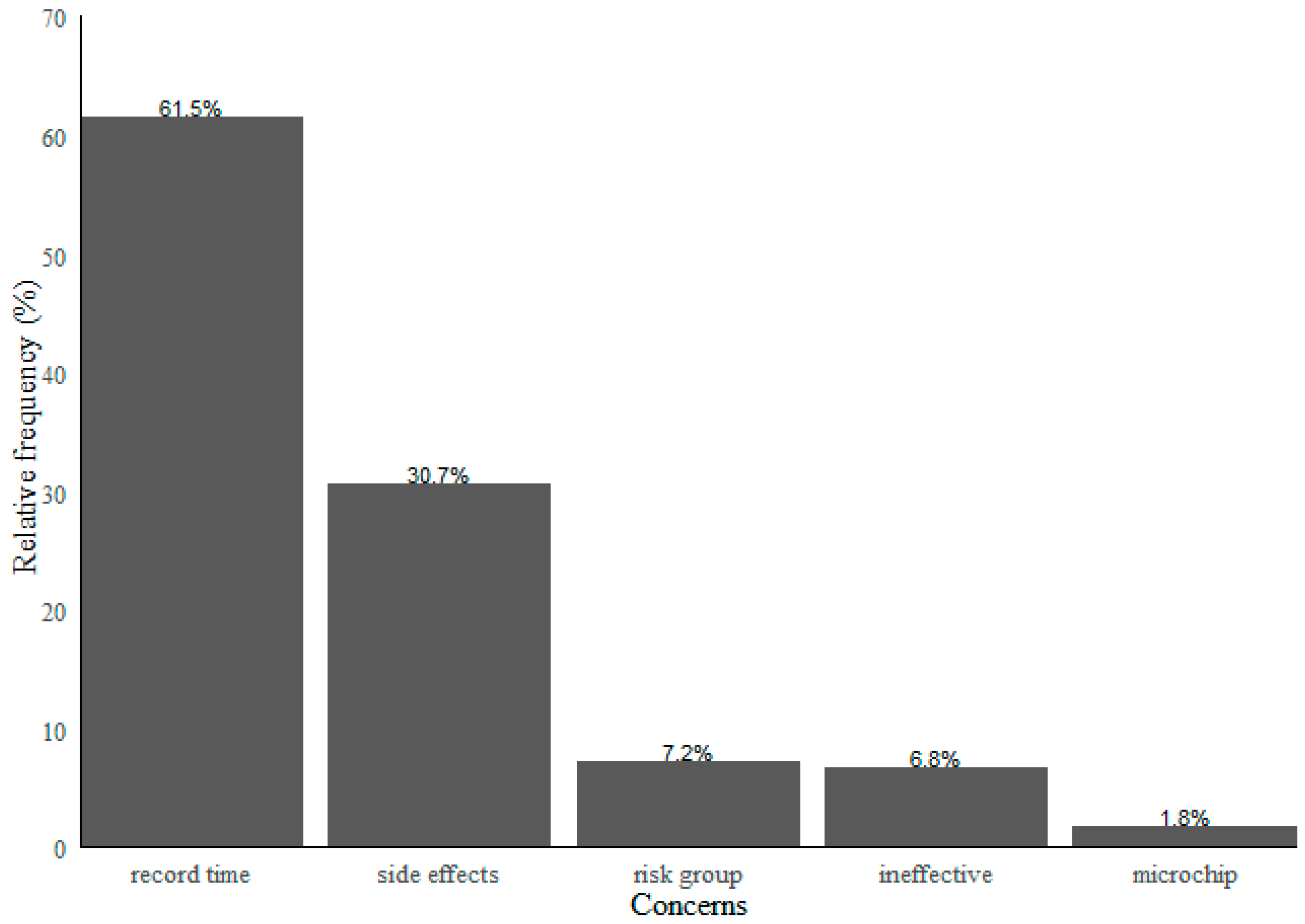
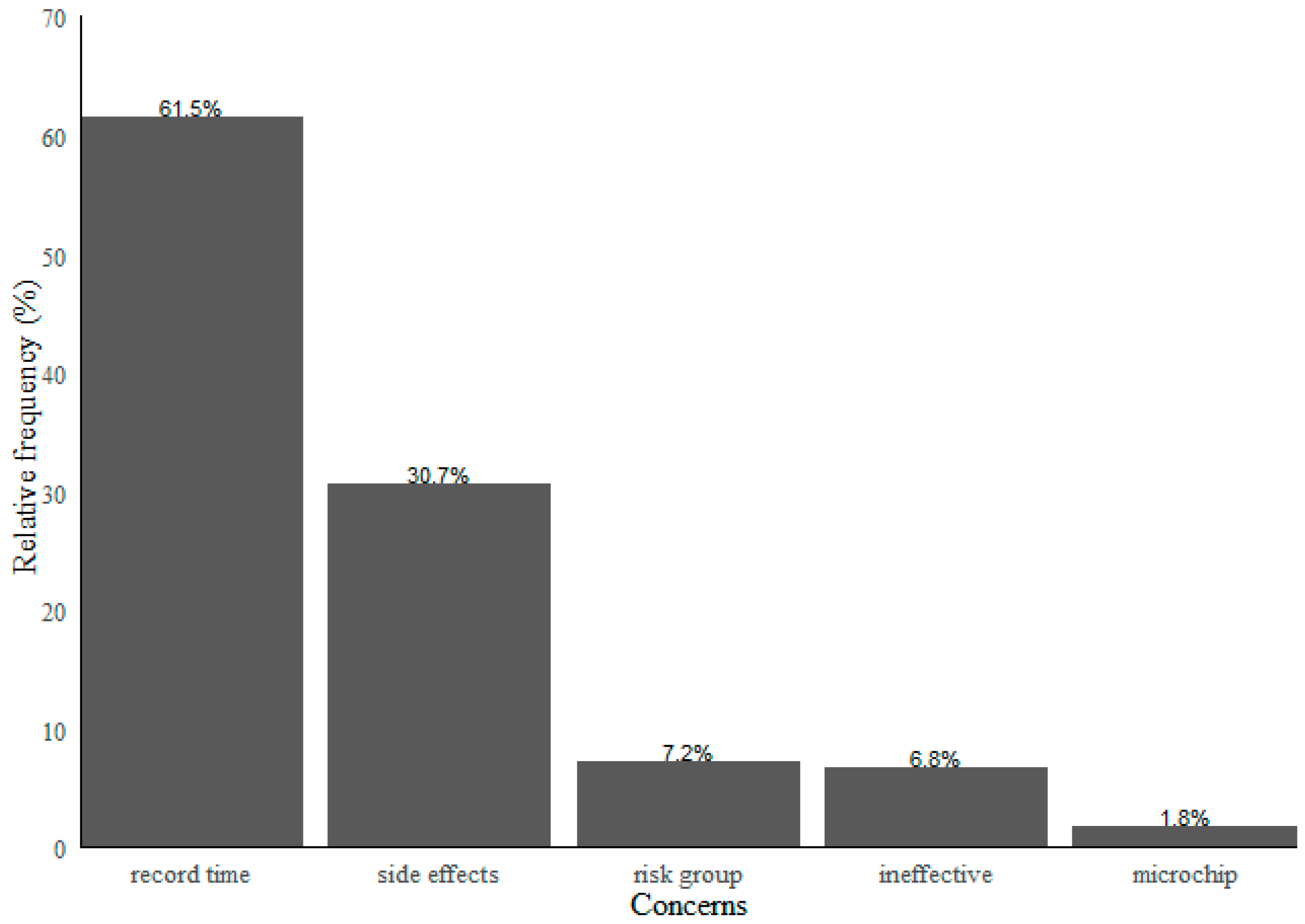
5.2. Vaccination Concerns
5.3. Dimensionality Reduction from the COVID-19 Attitudes and Beliefs Scale
5.4. Dimensionality Reduction from the COVID-19 Vaccine Attitudes and Beliefs Scale
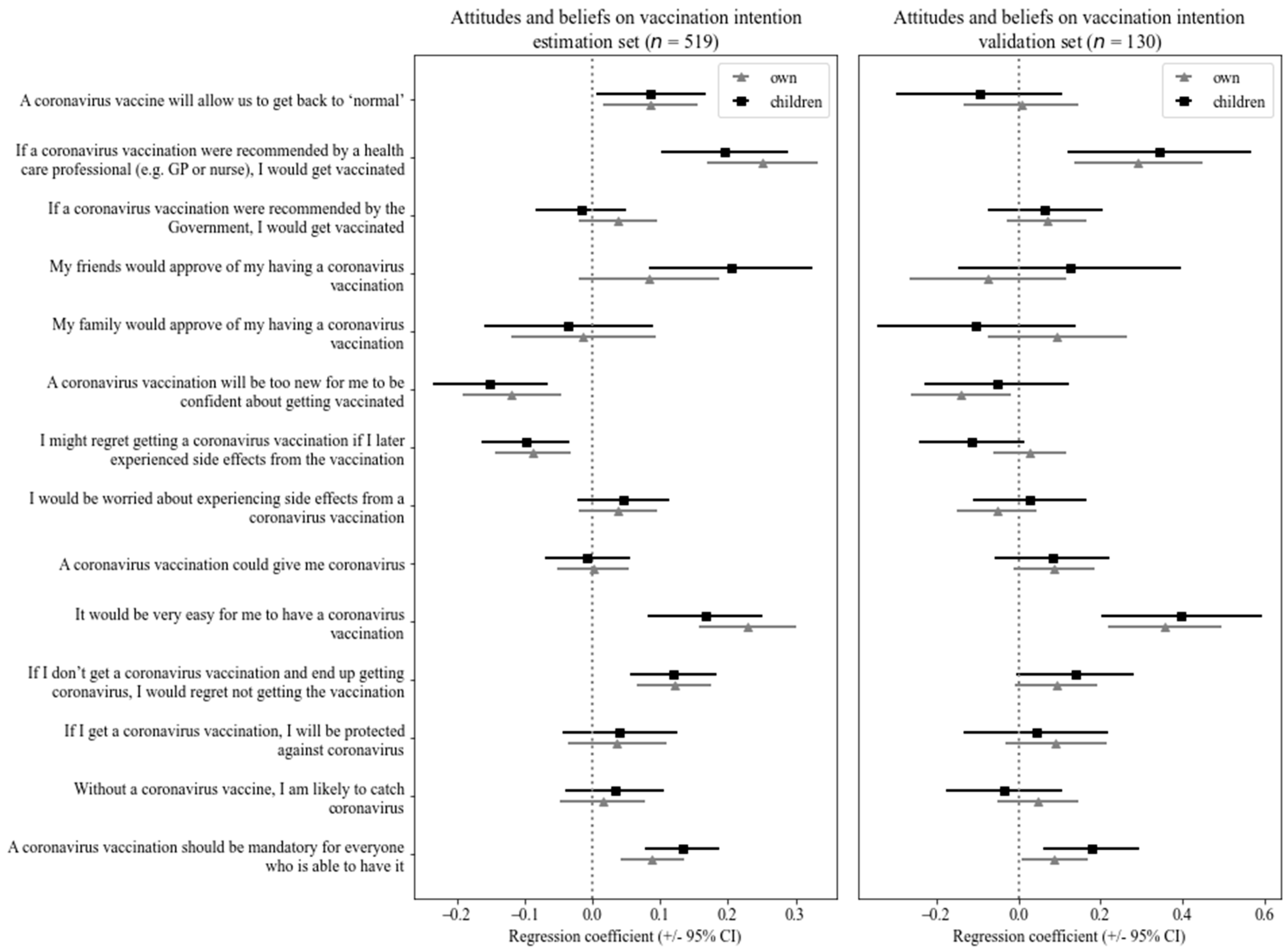
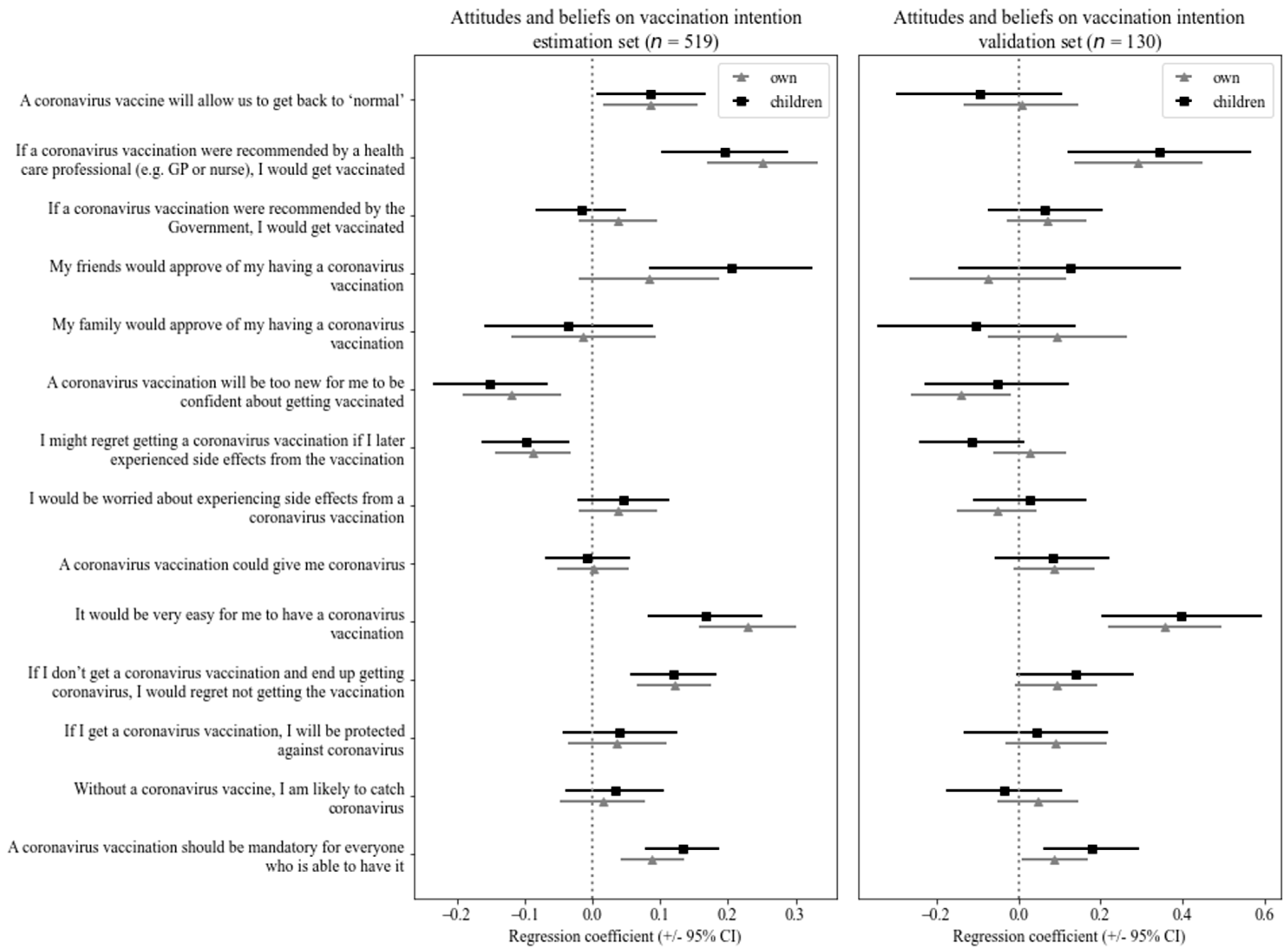
5.5. Multiple Regression Models of Self and Children Vaccination Intention
5.6. The Predictive Power of the General Beliefs and Attitudes towards the Vaccine
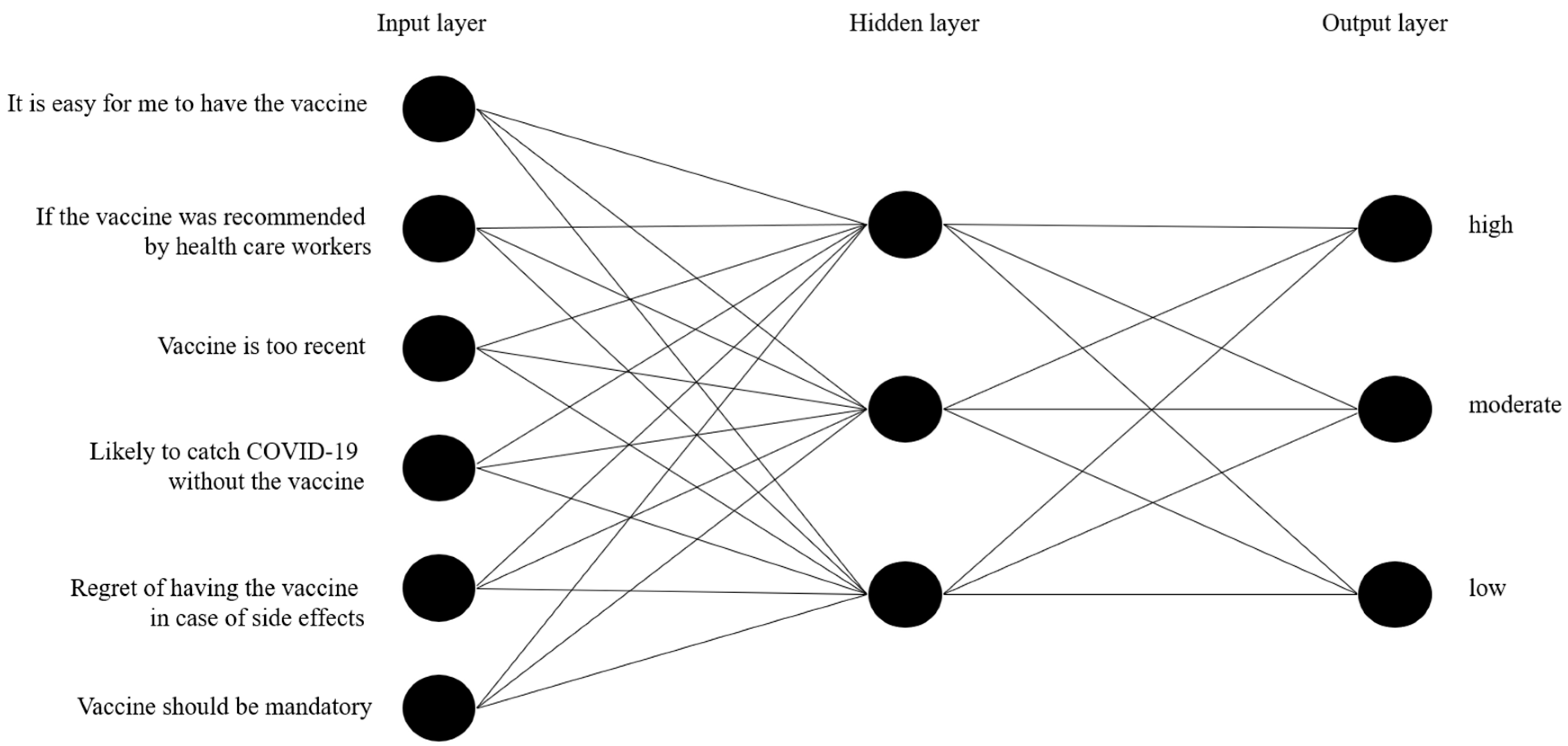
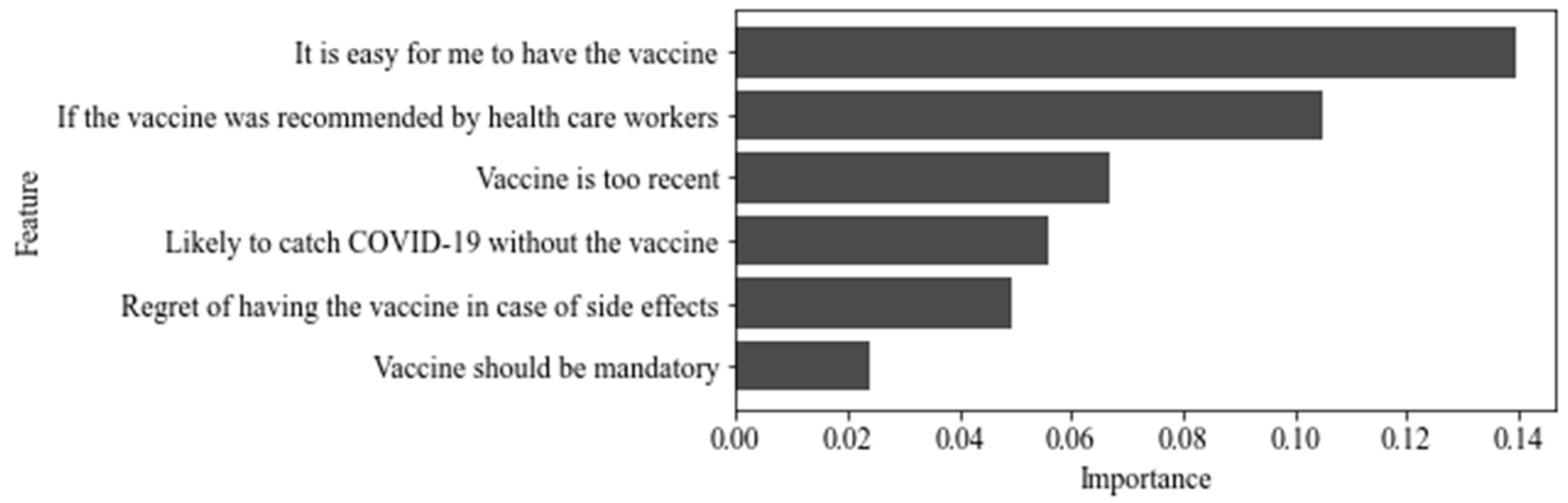
5.7. Machine Learning (ML)
6. Discussion
6.1. Theoretical Implications
6.2. Practical Implications
6.3. Limitations and Further Studies
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Personal Characteristics | Level | n (%) |
|---|---|---|
| Sex | Male | 152 (23.4) |
| Female | 495 (76.3) | |
| Other | 2 (0.3) | |
| Nationality | Portuguese | 616 (94.9) |
| Brazilian | 30 (4.6) | |
| Chinese | 1 (0.15) | |
| Colombian | 1 (0.15) | |
| French | 1 (0.15) | |
| Religion | No religion | 302 (46.5) |
| Christian | 278 (42.7) | |
| Buddhism | 2 (0.3) | |
| Asatru | 1 (0.2) | |
| Spiritualist | 5 (0.8) | |
| Evangelist | 5 (0.8) | |
| Jehovah’s Witness | 1 (0.2) | |
| Protestant | 1 (0.2) | |
| Any other religion | 49 (7.5) | |
| Prefer not to say | 5 (0.8) | |
| Highest qualification | Primary | 2 (0.3) |
| Basic | 21 (3.2) | |
| Secondary | 179 (27.6) | |
| Bachelor | 258 (39.8) | |
| Master | 172 (26.5) | |
| Doctorate | 11 (1.7) | |
| Other technical, professional, or higher qualification | 6 (0.9) | |
| Socioeconomic status | Low | 192 (29.5) |
| Medium | 380 (58.6) | |
| High | 77 (11.9) | |
| Employment status | Employed | 212 (32.7) |
| Student | 288 (44.4) | |
| Working student | 52 (8.0) | |
| Unemployed | 58 (8.9) | |
| Retired | 18 (2.8) | |
| Other | 21 (3.2) |
Appendix B
| Perceived Threat of COVID-19 | Trust in Management of COVID-19 | Impact of COVID-19 | |
|---|---|---|---|
| I am worried about catching coronavirus | −0.377 | ||
| I believe that coronavirus would be a mild illness for me | 0.514 | ||
| I believe I am immune to coronavirus | 0.493 | ||
| I trust the NHS to manage the coronavirus pandemic in Portugal | 0.693 | ||
| I trust the government to manage the coronavirus pandemic in Portugal | 0.650 | ||
| The coronavirus pandemic has had a big impact on my life | 0.91 |
Appendix C
| General COVID-19 Vaccination Beliefs and Attitudes | Others’ Intention | Perceived Knowledge Sufficiency | Return to Normal Life | |
|---|---|---|---|---|
| A coronavirus vaccination should be mandatory for everyone who is able to have it | 0.550 | |||
| Without a coronavirus vaccine, I am likely to catch coronavirus | 0.498 | |||
| If I get a coronavirus vaccination, I will be protected against coronavirus | 0.658 | |||
| If I don’t get a coronavirus vaccination and end up getting coronavirus, I would regret not getting the vaccination | 0.647 | |||
| It would be very easy for me to have a coronavirus vaccination | 0.753 | |||
| A coronavirus vaccination could give me coronavirus | −0.492 | |||
| I would be worried about experiencing side effects from a coronavirus vaccination | −0.557 | |||
| I might regret getting a coronavirus vaccination if I later experienced side effects from the vaccination | −0.583 | |||
| A coronavirus vaccination will be too new for me to be confident about getting vaccinated | −0.793 | |||
| Most people will get a coronavirus vaccination | - | 0.669 | ||
| Other people like me will get a coronavirus vaccination | - | 0.572 | ||
| If I were vaccinated, I think I would not need to follow social distancing and other restrictions for coronavirus | 0.574 | |||
| I know enough about the coronavirus illness to make an informed decision about whether or not to get vaccinated | 0.585 | |||
| I know enough about the coronavirus vaccine to make an informed decision about whether or not to get vaccinated | 0.569 | |||
| My family would approve of my having a coronavirus vaccination | 0.665 | |||
| My friends would approve of my having a coronavirus vaccination | 0.646 | |||
| If a coronavirus vaccination were recommended by the government, I would get vaccinated | 0.621 | |||
| If a coronavirus vaccination were recommended by a health care professional (e.g., doctor), I would get vaccinated | 0.788 | |||
| A coronavirus vaccine will allow us to get back to normal | 0.663 | |||
| There would be no point in having the coronavirus vaccination unless I could go back to my normal life | 0.604 |
Appendix D
Appendix E
Appendix F
| Predicted | |||
|---|---|---|---|
| Low | Moderate | High | |
| Low | 11 | 3 | 0 |
| Moderate | 0 | 24 | 10 |
| High | 0 | 7 | 75 |
| Class | Precision | Recall | F1 Score |
|---|---|---|---|
| Low | 100% | 79% | 88% |
| Moderate | 71% | 71% | 71% |
| High | 88% | 91% | 90% |
References
- Chriscaden, K. Impact of COVID-19 on People’s Livelihoods, Their Health and Our Food Systems. WHO, 2020. Available online: https://www.who.int/news/item/13-10-2020-impact-of-covid-19-on-people’s-livelihoods-their-health-and-our-food-systems (accessed on 13 May 2021).
- Dong, E.; Du, H.; Gardner, L. An interactive web-based dashboard to track COVID-19 in real time. Lancet. Infect. Dis. 2020, 20, 533–534. [Google Scholar] [CrossRef]
- Kim, Y.C.; Dema, B.; Reyes-Sandoval, A. COVID-19 vaccines: Breaking record times to first-in-human trials. NPJ Vaccines 2020, 5, 1–3. [Google Scholar] [CrossRef]
- Chou, W.S.; Budenz, A. Considering emotion in COVID-19 vaccine communication: Addressing vaccine hesitancy and fostering vaccine confidence. Health Commun. 2020, 35, 1718–1722. [Google Scholar] [CrossRef]
- Thunstrom, L.; Ashworth, M.; Finnoff, D.; Newbold, S. Hesitancy towards a COVID-19 vaccine and prospects for herd immunity. SSRN 2020, 1–51. [Google Scholar] [CrossRef]
- Neumann-Böhme, S.; Varghese, N.E.; Sabat, I.; Barros, P.P.; Brouwer, W.; Exel, J.V.; Schreyögg, J.; Stargardt, T. Once we have it, will we use it? A European survey on willingness to be vaccinated against COVID-19. Eur. J. Health Econ. 2020, 21, 977–982. [Google Scholar] [CrossRef] [PubMed]
- de Loomba, F.A.; Piatek, S.J.; de Graff, K.; Larson, H.J. Measuring the impact of COVID-19 vaccine misinformation on vaccination intent in the UK and USA. Nat. Hum. Behav. 2021, 5, 337–348. [Google Scholar] [CrossRef]
- Vogel, G.; Kupferschmidt, K. Side effect worry grows for AstraZeneca vaccine. Science 2021, 372, 14–15. [Google Scholar] [CrossRef] [PubMed]
- Larson, H.J.; Broniatowski, D.A. Volatility of vaccine confidence. Science 2021, 371, 1289. [Google Scholar] [CrossRef]
- Jarrett, C.; Wilson, R.; O’Leary, M.; Eckersberger, E.; Larson, H.J. Strategies for addressing vaccine hesitancy—A systematic review. Vaccine 2015, 33, 4180–4190. [Google Scholar] [CrossRef] [Green Version]
- Wilson, S.L.; Wiysonge, C. Social media and vaccine hesitancy. BMJ Glob. Health 2020, 5, 1–7. [Google Scholar] [CrossRef]
- Detoc, M.; Bruel, S.; Frappe, P.; Tardy, B.; Botelho-Nevers, E.; Gagneux-Brunon, A. Intention to participate in a COVID-19 vaccine clinical trial and to get vaccinated against COVID-19 in France during the pandemic. Vaccine 2020, 38, 7002–7006. [Google Scholar] [CrossRef]
- Sherman, S.M.; Smith, L.E.; Sim, J.; Amlôt, R.; Cutts, M.; Dasch, H.; Rubin, G.J.; Sevdalis, N. COVID-19 vaccination intention in the UK: Results from the COVID-19 vaccination acceptability study (CoVAccS), a nationally representative cross-sectional survey. Hum. Vaccin. Immunother. 2021, 17, 1612–1621. [Google Scholar] [CrossRef] [PubMed]
- Kahneman, D.; Tversky, A. Prospect theory: An analysis of decision under risk. Econometrica 1979, 47, 263–292. [Google Scholar] [CrossRef] [Green Version]
- Callaghan, T.; Moghtaderi, A.; Lueck, J.A.; Hotez, P.; Strych, U.; Dor, A.; Fowler, E.F.; Motta, M. Correlates and disparities of COVID-19 vaccine hesitancy. Soc. Sci. Med. 2021, 272, 113642. [Google Scholar] [CrossRef]
- Crainich, D.; Eeckhoudt, L.; Menegatti, M. Vaccination as a trade-off between risks. Ital. Econ. J. 2019, 5, 455–472. [Google Scholar] [CrossRef]
- Palm, R.; Bolsen, T.; Kingsland, J.T. The effect of frames on COVID-19 vaccine hesitancy. MedRxiv 2021, 3, 3. [Google Scholar] [CrossRef]
- Ajzen, I. The theory of planned behavior. Organ. Behav. Hum. Decis. Process. 1991, 50, 179–211. [Google Scholar] [CrossRef]
- Cialdini, R.B.; Trost, M.R. Social Influence: Social Norms, Conformity and Compliance. In The Handbook of Social Psychology, 4th ed.; Gilbert, D.T., Fiske, S.T., Gardner, L., Eds.; McGraw-Hill: New York, NY, USA, 1998; Volume 2, pp. 151–192. [Google Scholar]
- Tversky, A.; Kahneman, D. Availability: A heuristic for judging frequency and probability. Cogn. Psychol. 1973, 5, 207–232. [Google Scholar] [CrossRef]
- Anderson, E.J.; Campbell, J.D.; Creech, C.B.; Frenck, R.; Kamidani, S.; Munoz, F.M.; Nachman, S.; Spearman, P. Warp speed for COVID-19 vaccines: Why are children stuck in neutral? Clin. Infect. Dis. 2020, 73, 336–340. [Google Scholar] [CrossRef]
- Meszaros, J.R.; Asch, D.A.; Baron, J.; Hershey, J.C.; Kunreuther, H.; Schwartz-Buzaglo, J. Cognitive processes and the decisions of some parents to forego pertussis vaccination for their children. J. Clin. Epidemiol. 1996, 49, 697–703. [Google Scholar] [CrossRef]
- Bell, S.; Clarke, R.; Mounier-Jack, S.; Walker, J.L.; Paterson, P. Parents’ and guardians’ views on the acceptability of a future COVID-19 vaccine: A multi-methods study in England. Vaccine 2020, 38, 7789–7798. [Google Scholar] [CrossRef] [PubMed]
- Blais, A.; Weber, E.U. A Domain-Specific Risk-Taking (DOSPERT) scale for adult populations. Judgm. Decis. Mak. 2006, 1, 33–47. [Google Scholar] [CrossRef]
- Silva, R. Risk Profiling and the DOSPERT Scale: An Approach Using Prospect Theory. Master’s Thesis, Universidade Técnica de Lisboa, Lisboa, Portugal, 2012. Available online: http://hdl.handle.net/10400.5/10351 (accessed on 15 January 2021).
- Qualtrics. Qualtrics, Provo, UT, USA. 2021. Available online: https://www.qualtrics.com (accessed on 7 January 2021).
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2020. Available online: https://www.R-project.org/ (accessed on 5 September 2021).
- RStudio Team. RStudio: Integrated Development Environment for R. RStudio, PBC, Boston, MA, USA. 2021. Available online: http://www.rstudio.com/ (accessed on 5 September 2021).
- Pedregosa, F.; Varoquaux, G.; Gramfort, A.; Michel, V.; Thirion, B.; Grisel, O.; Blondel, M.; Prettenhofer, P.; Weiss, R.; Dubourg, V.; et al. Scikit-learn: Machine learning in Python. J. Mach. Learn. Res. 2011, 12, 2825–2830. [Google Scholar]
- Wise, T.; Zbozinek, D.T.; Michelini, G.; Hagan, C.C.; Mobbs, D. Changes in risk perception and self-reported protective behaviour during the first week of the COVID-19 pandemic in the United States. R. Soc. Open. Sci. 2020, 7, 200742. [Google Scholar] [CrossRef]
- Ripley, B.D. Pattern Recognition and Neural Networks; Cambridge University Press: Cambridge, UK, 1996. [Google Scholar] [CrossRef]
- Niazkar, H.R.; Niazkar, M. Application of artificial neural networks to predict the COVID-19 outbreak. Glob. Health Res. Policy 2020, 5, 1–11. [Google Scholar] [CrossRef]
- Tamang, S.K.; Singh, P.D.; Datta, B. Forecasting of Covid-19 cases based on prediction using artificial neural network curve fitting technique. Glob. J. Environ. Sci. Manag. 2020, 6, 53–64. [Google Scholar] [CrossRef]
- Soares, P.; Rocha, J.V.; Moniz, M.; Gama, A.; Laires, P.A.; Pedro, A.R.; Dias, S.; Leite, A.; Nunes, C. Factors associated with COVID-19 vaccine hesitancy. Vaccines 2021, 9, 300. [Google Scholar] [CrossRef]
- Ribas, A.; Sengupta, R.; Locke, T.; Zaidi, S.K.; Campbell, K.M.; Carethers, J.M.; Jaffee, E.M.; Wherry, E.J.; Soria, J.; D’Souza, G. Priority COVID-19 vaccination for patients with cancer while vaccine supply is limited. Cancer Discov. 2021, 11, 233–236. [Google Scholar] [CrossRef]
- Kelkar, A.H.; Blake, A.J.; Cherabuddi, K.; Cornett, H.; McKee, B.L.; Cogle, C.R. Vaccine enthusiasm and hesitancy in cancer patients and the impact of a webinar. Healthcare 2020, 9, 351. [Google Scholar] [CrossRef]
- Bavel, J.J.V.; Baicker, K.; Boggio, P.S.; Capraro, V.; Cichocka, A.; Cikara, M.; Crockett, M.J.; Crum, A.J.; Douglas, K.M.; Druckman, J.N.; et al. Using social and behavioural science to support COVID-19 pandemic response. Nat. Hum. Behav. 2020, 4, 460–471. [Google Scholar] [CrossRef] [PubMed]
- Scott, G.; Abdallah, D.A.; Lee, C.M. Social norms and vaccine uptake: College students’ COVID vaccination intentions, attitudes, and estimated peer norms and comparisons with influenza vaccine. Vaccine 2021, 39, 2060–2067. [Google Scholar] [CrossRef]
- van der Linden, S.; Roozenbeek, J.; Compton, J. Inoculating against fake news about COVID-19. Front. Psychol. 2020, 11, 2928–2935. [Google Scholar] [CrossRef]
- Fridman, A.; Gershon, R.; Gneezy, A. COVID-19 and vaccine hesitancy: A longitudinal study. PLoS ONE 2021, 16, e0250123. [Google Scholar] [CrossRef]
- DGS. Ponto de Situação Atual em Portugal. Available online: https://covid19.min-saude.pt/ponto-de-situacao-atual-em-portugal/ (accessed on 29 May 2021).
- Binder, S.; Nuscheler, R. Risk-taking in vaccination, surgery, and gambling environments: Evidence from a framed laboratory experiment. Health Econ. 2017, 26, 76–96. [Google Scholar] [CrossRef]
- Guo, N.; Wang, J.; Nicholas, S.; Maitland, E.; Zhu, D. Behavioral differences in the preference for hepatitis B virus vaccination: A discrete choice experiment. Vaccines 2020, 8, 527. [Google Scholar] [CrossRef]
- West, P.M.; Brockett, P.L.; Golden, L.L. A comparative analysis of neural networks and statistical methods for predicting consumer choice. Mark. Sci. 1997, 16, 295–391. [Google Scholar] [CrossRef]
- Gu, Y. COVID-19 Projections Using Machine Learning. Available online: https://covid19-projections.com (accessed on 5 October 2020).
- Lewin, K. Frontiers in group dynamics: Concept, method and reality in social science; social equilibria and social change. Hum. Relat. 1947, 1, 5–41. [Google Scholar] [CrossRef]
- Xiao, X.; Borah, P. Do norms matter? Examining norm-based messages in HPV vaccination promotion. Health Commun. 2020, 25, 843–858. [Google Scholar] [CrossRef] [PubMed]
- Cialdini, R.B.; Goldstein, N.J. The science and practice of persuasion. Cornell Hosp. Q. 2002, 43, 40–50. [Google Scholar] [CrossRef]
- Mahase, E. Covid-19: What have we learnt about the new variant in the UK? BMJ 2020, 371, m4944. [Google Scholar] [CrossRef]
- Hawkins, D.M. The problem of overfitting. J. Chem. Inf. Comput. Sci. 2004, 44, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Sáez, C.; Romero, N.; Conejero, J.A.; García-Gómez, J.M. Potential limitations in COVID-19 machine learning due to data source variability: A case study in the nCov2019 dataset. J. Am. Med. Inform. Assoc. 2020, 28, 360–364. [Google Scholar] [CrossRef] [PubMed]
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fernandes, N.; Costa, D.; Costa, D.; Keating, J.; Arantes, J. Predicting COVID-19 Vaccination Intention: The Determinants of Vaccine Hesitancy. Vaccines 2021, 9, 1161. https://doi.org/10.3390/vaccines9101161
Fernandes N, Costa D, Costa D, Keating J, Arantes J. Predicting COVID-19 Vaccination Intention: The Determinants of Vaccine Hesitancy. Vaccines. 2021; 9(10):1161. https://doi.org/10.3390/vaccines9101161
Chicago/Turabian StyleFernandes, Nuno, Daniela Costa, Diogo Costa, José Keating, and Joana Arantes. 2021. "Predicting COVID-19 Vaccination Intention: The Determinants of Vaccine Hesitancy" Vaccines 9, no. 10: 1161. https://doi.org/10.3390/vaccines9101161
APA StyleFernandes, N., Costa, D., Costa, D., Keating, J., & Arantes, J. (2021). Predicting COVID-19 Vaccination Intention: The Determinants of Vaccine Hesitancy. Vaccines, 9(10), 1161. https://doi.org/10.3390/vaccines9101161