Abstract
Introduction: An effective vaccination strategy requires monitoring serotype changes by geography and age. This study analyzed Streptococcus pneumoniae serotypes in healthy children under 6 years of age vaccinated with PCV10 in Bulgaria from October 2021 to May 2025. Methods: A total of 569 children were screened for the lytA and cpsA genes viareal-time polymerase chain reaction (real-time PCR). Positive samples were typed using relevant kits, and 76 serotypes/serogroups of S. pneumoniae were identified. Results: Nasopharyngeal swabs from 232 children (40.8%) were found to carry S. pneumoniae, and a total of 255 serotypes were detected, with 19B/19C (17.2%), 6C (10.7%), and 15B/15C (9.8%) being the most prevalent. Of these, 91 serotypes (15.9%) were included in at least one vaccine, while the remaining 164 serotypes (25.4%) were not. The carriage rate reduced to 22% in 2023 but increased to 47% in 2024. Overall, younger children had lower carriage rates (p < 0.05), with serotype 6C being more common in children under 12 months of age (25%). Approximately 9.1% of pneumococcal carriage cases involved co-detected serotypes, with significantly higher co-detection rates for 19B/19C, 15B/15C, 10B, 10F/C, 23B, 7C/40, 23A, and 24A compared with mono-detection rates (p < 0.05). Conclusions: 19B/19C, 6C, 15B/15C, and 19A were identified as the main serotypes. Children over 3 years of age were also more likely to carry multiple pneumococci. These findings emphasize the need to reassess childhood vaccination strategies to curb the spread of antibiotic-resistant serotypes.
1. Introduction
Streptococcus pneumoniae represents a significant public health challenge worldwide. It is one of the most common bacterial pathogens responsible for invasive disease in both children and adults [1]. According to the World Health Organization (WHO), an estimated 1.6 million people died from pneumococcal disease in 2011, with between 0.7 and 1 million of these deaths occurring in children under 5 years of age, predominantly in developing countries [2]. The high mortality rates can be explained by the wide global distribution of S. pneumoniae and its ability to colonize the nasopharynx without causing symptoms [3,4]. This bacterium can spread rapidly, especially in close-knit communities, through airborne transmission via droplets or direct contact with carriers [5].
S. pneumoniae has a complex relationship with its human host. These bacteria are highly adapted companions that primarily inhabit the mucosal surfaces of the upper respiratory tract of carriers, facilitating their transmission [1,6]. However, they can also cause severe disease when certain bacterial and host factors allow them to invade normally sterile areas such as the middle ear, lungs, bloodstream, and meninges [7]. S. pneumoniae can both evade and exploit host inflammatory and immune responses, which determine the processes of transmission, colonization, and invasion [1,8]. These features in pneumococcal pathogenesis make it an important target of epidemiological research aimed at developing strategies to reduce transmission and prevent complications associated with pneumococcal infections.
The polysaccharide capsule of this bacterium is its most important pathogenic factor [3]. It is a major virulence and antigenic component in S. pneumoniae and plays a crucial role in the bacterium’s ability to colonize hosts. Pneumococcal serotypes are classified based on variations in the structure of their polysaccharide capsules [9,10]. Since the introduction of pneumococcal conjugate vaccines, there has been a noticeable decrease in the asymptomatic carriage of vaccine-targeted serotypes of this pathogen [11]. Over 100 different pneumococcal serotypes have been identified, varying in frequency, disease manifestation, and antibiotic resistance [12,13]. Many factors, including the introduction of new pneumococcal conjugate vaccines (PCVs) and the use of antibiotics, may influence the spread of different S. pneumoniae serotypes [14]. These serotypes vary in frequency, clinical manifestations, and antibiotic resistance. The introduction of new conjugate vaccines and antibiotic usage can influence the replacement of these serotypes [15]. The first pneumococcal polysaccharide vaccine was tested in 1944 [16]. Interest in vaccines declined after the discovery of penicillin, but the need for prevention led to the introduction of the 23-valent pneumococcal polysaccharide vaccine (PPSV23), covering 23 serotypes, in 1983 [17]. PPSV23 primarily induces a B-cell-mediated immune response, making it ineffective for infants and toddlers at high risk of pneumococcal disease. To address this, pneumococcal conjugate vaccines (PCVs) were developed to elicit a T-cell-dependent immune response, inspired by the success of the Haemophilus influenzae type b vaccine [18]. The first pneumococcal conjugate vaccine (PCV), known as the 7-valent PCV (PCV7), was introduced in 2000 and demonstrated high effectiveness in children. This was followed by two additional higher-valency PCVs: the 10-valent PCV (PCV10), introduced in 2009, which included all the serotypes covered by PCV7 plus three additional serotypes (1, 5, and 7F); and the 13-valent PCV (PCV13), launched in 2010, which included all the serotypes in PCV10 plus three more (3, 6A, and 19A) [19]. These three vaccines—PCV7, PCV10, and PCV13—are part of national immunization programs (NIPs) for children in many countries worldwide.
In 2010, Bulgaria’s Ministry of Health approved and instituted mandatory vaccination with the 10-valent pneumococcal vaccine (PCV10) in children. Immunization against pneumococcal disease is administered in four doses, scheduled at 2, 3, 4, and 12 months after birth. From 2011 to 2023, vaccine coverage was reported to be around 90%, according to data from the National Center for Infectious and Parasitic Diseases [20]. Developing an effective vaccination strategy for each country requires monitoring changes in the serotypes that colonize the population and analyzing geographic and age-specific distribution patterns. Despite the critical need to select the right vaccination approach, the existing literature does not sufficiently address the epidemiology of emerging serotypes. To evaluate the long-term impact of vaccination, we aim to conduct an epidemiological analysis of the different S. pneumoniae serotypes carried by healthy children up to 6 years of age who have been vaccinated with PCV10.
2. Materials and Methods
2.1. Study Population
This study focused on vaccinated, healthy children aged 5 months to 6 years. It was conducted from October 2021 to May 2025, providing data on the carriage and distribution of S. pneumoniae serotypes in Bulgaria. Samples for this study were collected after obtaining informed consent from the parents.
Nasopharyngeal samples were collected using a flexible, sterile swab. The samples were collected by trained personnel during planned home visits. Sample collection occurred year-round, with secretions collected from children up to 6 years of age in kindergartens and by general practitioners across 15 of 28 districts in Bulgaria: Sofia, the Sofia region, Yambol, Pernik, Montana, Shumen, Burgas, Blagoevgrad, Gabrovo, Plovdiv, Kardzhali, Stara Zagora, Kyustendil, Pleven, and Vidin.
2.2. Participant Selection Criteria
- −
- Healthy children aged 2 to 6 years who attended childcare facilities, having completed a full vaccination course of PCV10 (3 + 1 doses).
- −
- Healthy children aged 5 months to 6 years who did not attend childcare facilities but had received at least one of the mandatory doses of PCV10.
2.3. Sample Collection
Nasopharyngeal secretions were collected using two swabs: one with eSwab transport medium (Copan, Italy) for microbiological examination on nutrient medium and one dry sterile swab for DNA isolation. The samples were transported to the National Reference Laboratory (NRL) for Molecular Microbiology at the National Centre of Infectious and Parasitic Diseases in Sofia, Bulgaria. Samples from children under 11 months were collected before administration of the fourth vaccine dose. No additional biological samples were included in this study, and the participating children remained anonymous; only data on year and month of birth, gender, kindergarten attendance, and vaccination status were used.
2.4. Exclusion Criteria
The study excluded patients who exhibited symptoms of respiratory infections and those older than 6 years of age, as well as individuals who were unwilling or unable to provide consent. Additionally, any samples received in the laboratory that did not comply with the specified criteria for the transportation and storage of nasopharyngeal samples were also excluded.
2.5. Detection of S. Pneumoniae
2.5.1. Classical Detection Method
The collected samples were cultured on Columbia CNA agar with 5% sheep blood, supplemented with an optochin disc to differentiate pneumococci from other flora, at 35 ± 2 °C for 18–24 h in an aerobic atmosphere enriched with carbon dioxide at an elevated concentration (8–10%). In the presence of S. pneumoniae, it was isolated, subcultured, and subsequently used for DNA extraction and strain storage [21].
2.5.2. Molecular Methods
For direct DNA isolation from swabs containing nasopharyngeal secretions, a protocol using 5% Chellex [22] ion exchange resin was followed, in accordance with the standard procedures of the National Laboratory of Molecular Microbiology. Samples were screened for the lytA (in Supplementary Table S1) and cpsA genes using real-time PCR [23]. Samples positive for both genes were further typed using PCR and subsequent allelic hybridization for 76 serotypes and serogroups. Samples positive only for lytA were classified as non-capsular, and pneumococcus typing was not performed for these samples.
2.5.3. Typing of S. Pneumoniae Isolates
Samples positive for both genes were typed using PCR and subsequent allelic hybridization using the commercial kit “S. PneumoStrip” from Operon, allowing easy and rapid single amplification identification of 76 serotypes/serogroups of S. pneumoniae. Among these serogroups are those included in the currently available vaccines.
The following serotypes/serogroups were included:
Band A: 1, 3, 4, 5, 6A, 6B, 6C, 6D, 7F/7A, 9A/9V, 14, 18A, 18B/18C, 18F, 19A, 19F, 23A, 23B, 23F.
Band B: 2, 8, 9N/9L, 10A, 10B, 10F/C, 11A/D, 11B, 11C, 11F, 12A/46, 12B/44, 12F, 15B/15C, 17F, 20, 22F/22A, 33F/33A, 37.
Band C: 7B, 7C/40, 15A, 15F, 16F, 19B/19C, 21, 25A/25F, 38, 24A, 24B/24F, 31, 32A/32F, 33B/33D, 33C, 35A, 35C, 35F, 47F, 41A, 41F.
LytA and cpsA were also identified as control genes during the hybrid analysis.
2.6. Statistical Analysis
We used a 2 × 2 contingency table to analyze the data, using the number of patients by two or more experimental factors, and dividing participants into appropriate categories. A Fisher’s exact test was used to analyze categorical variables in GraphPad (https://www.graphpad.com/quickcalcs/contingency1/, accessed on 10 June 2025). p-values less than 0.05 were deemed statistically significant.
3. Results
3.1. Characteristics of the Tested Group
This study was conducted over 4 years, during which 569 samples from children up to 6 years of age were tested for S. pneumoniae. The distribution of children by age group was as follows: under 12 months (73), 12–24 months (107), 36–59 years (220), and 5–6 years (169). PCR testing detected S. pneumoniae in nasopharyngeal swabs from 232 children, indicating a carrier rate of 40.8% in the study population. In comparison, the traditional microbiological method isolated S. pneumoniae from only 26 nasal secretions, representing only a 4.6% positivity rate (p = 0.0001). The carrier rates for both sexes were similar, with 128 males (42.2%) and 105 females (39.4%) testing positive for S. pneumoniae.
3.2. S. pneumoniae Serotypes
We conducted an analysis to differentiate between capsular and non-capsular strains of S. pneumoniae. Our findings revealed that capsular strains accounted for 214 (91.8%) of the samples, while only 18 (7.7%) were non-capsular strains. We then analyzed the capsular S. pneumoniae to identify their serogroups/serotypes. The kit we used for this analysis successfully differentiated S. pneumoniae in 168 samples (78.6%) from children under 6 years of age, with 46 samples (21.4%) remaining untyped. The following S. pneumoniae serotypes were present at the highest percentages: 19B/19C (n = 40; 17.2%), 6C (n = 25; 10.7%), 15B/15C (n = 23; 9.8%), 19A (n = 17; 7.3%), 23B (n = 16; 6.9%), 11A/D (n = 15; 6.4%) (Figure 1).
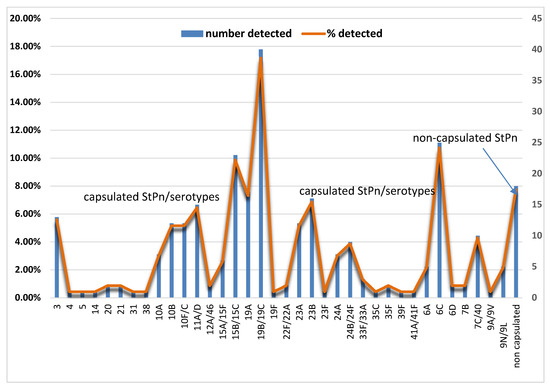
Figure 1.
The distribution of detected encapsulated and non-encapsulated Streptococcus pneumoniae. The distribution of the type, number, and percentage of non-encapsulated S. pneumoniae is presented, along with serotypes of encapsulated S. pneumoniae (StPn*).
3.3. Vaccine Serotypes
Out of the 255 serotypes detected, 91 (15.9%) were covered by at least one of the available vaccines: PCV7, PCV10, PCV13, PCV15, or PCV20. These 91 serotypes belonged to 14 different serotype/serogroup categories. However, 164 serotypes, representing 25.4% of 22 different categories, were not included in these vaccines. Specifically, 6% of the documented pneumococcal carriage was attributed to serotypes 3, 19A, and 6A, which are included as vaccine strains in PCV13 but not covered by PCV10. The carriage rate of the strains included in the PCV10 vaccine was only 1% (refer to Table 1 for further details).

Table 1.
The distribution of vaccine serotypes in different vaccine generations compared with Streptococcus pneumoniae serotypes detected in children under 6 years of age.
3.4. The Dynamics of the Spread of S. pneumoniae
In the first year of this study (2021), we found that the prevalence of S. pneumoniae carriage among children under 6 years of age was 34.3%. In the following year (2022), we observed a decrease in the frequency of this carriage (27%). The decrease was even more significant in 2023, with the carriage frequency reducing to 22%, a statistically significant change compared with the 2021 data (p < 0.05). In 2024, the presence of S. pneumoniae in the nasopharynx of children increased to 47% among those surveyed. This increase was statistically significant compared with the levels observed in 2022 and 2023 (p < 0.05). All 54 healthy children studied in the first 3 months of 2025 were found to be carriers of S. pneumoniae.
3.4.1. The Dynamics of the Spread of S. pneumoniae Serotypes
A total of 24 different S. pneumoniae serotypes were identified in 2021. By 2024, this number had decreased to 18. The years 2022 and 2023 showed less diversity, with 17 and 14 serotypes identified, respectively. In the first half of 2025, 16 different serotypes of S. pneumoniae were identified in children under 6 years of age. The predominant serotype from 2021 to 2024 was 19B/19C, with a detection rate of 7–9%. The most common serotype in 2025 was 19A, with a detection rate of 19%, followed by 6C, 15B/15C, and 11A/D, with detection rates of 17.6%, 17.6%, and 11.8%, respectively, among children tested for S. pneumoniae carriage (Figure 2).
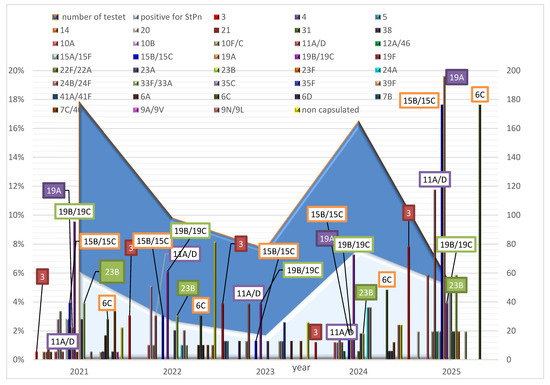
Figure 2.
The dynamics of the spread of non-capsular and capsular S. pneumoniae, along with their serotypes, for each year from 2021 to 2025 among healthy children under 6 years of age.
Analysis of the variation in the detected serotypes among the children tested was conducted in relation to their presence in previous years. In 2021, eight of the detected serotypes (14, 21, 31, 19F, 39F, 41A/41F, and 9A/9V) were unique, as they were not observed in children tested in previous years. In 2022, we detected serotypes 24A, 24B/24F, 33F/33A, 6D, and 9N/9L in this group of children, noting varying rates of detection in subsequent years. In 2023, newly identified serotypes included 4, 5, 38, 35C, and 35F. The newly identified serotype in 2024 was 22F/22A; this was also identified in the group of children tested in 2025.
3.4.2. Age Distribution of Detected S. pneumoniae Serotypes
Participants in this study were divided into four age groups to examine the relationship between age and S. pneumoniae carriage (Table 2). Children under 12 months of age were less likely to be carriers of S. pneumoniae (20.4%) compared with the other three age groups (12–35 months, 38.08%; 36–59 months, 71.89%; 5–6 years, 76.38%). Non-capsulated S. pneumoniae was significantly less common in children under 12 months of age (5.6%) compared with encapsulated S. pneumoniae in children aged 36 months to 6 years (36–59 months, 33%; 5–6 years, 43%; p < 0.05). Furthermore, the incidence of capsulated S. pneumoniae was significantly lower in children under 12 months of age (14.8%) compared with the incidence of non-encapsulated S. pneumoniae in children aged 36 months to 6 years (36–59 months, 38.9%; 5–6 years, 33.3%; p < 0.05).
Table 2.
Distribution of detected S. pneumoniae serotypes in different age groups: under 12 months, 12–35 months, 36–59 months, and 5–6 years.
Serotype 6C was detected more frequently in children under 12 months of age than in the other three age groups, with a prevalence of 25% compared with 15% in the 12–35 months group (n = 0.0996), 15% in the 36–59 months group (n = 0.2318), and 8.5% in the 5–6 years group (n = 0.0398) (see Table 1). Serogroup 10A also showed a higher detection rate in the youngest children, at 14.3%, compared with none detected in the 12–35 months group (n = 0.0267) and the 36–59 months group (n = 0.0088), and 5% in the 5–6 years group (n = 0.2051) (see Table 1). There was a predominance of S. pneumoniae serogroups 19B/19C and 7C/40 in the 36–59 months and 5–6 years age groups compared with the younger children. A significant difference was observed in the frequency of 19B/19C carriage in children over 36 months of age compared with children in the 12–35 months group (10.7%), with a prevalence of 26% in the 36–59 months group and 32.2% in the 5–6 years group (p < 0.05).
3.5. Mono- and Co-Detection of S. pneumoniae Serotypes
In this study involving 569 children under the age of 6 years, we observed both mono- and co-carriage of multiple serotypes of S. pneumoniae. Specifically, one serotype was detected in 116 children, accounting for 20.4% of the total number of children. In contrast, more than one serotype was identified in 52 children, representing 9.1% of the group. The distribution of detected serotypes among the patients was as follows: two serotypes were found in 30 (17.9%) children, three serotypes in 15 (8.9%) children, four serotypes in 5 (2.9%) children, five serotypes in 1 (0.6%) child, and six serotypes in 1 (0.6%) child. Figure 3 shows that, among children screened for S. pneumoniae carriage, some serotypes were more frequently detected together with other S. pneumoniae serotypes than alone. Serotypes 19B/19C, 15B/15C, 10B, 10F/C, 23B, 7C/40, 23A, and 24A had co-detection rates of 55.8%, 28.9%, 21.2%, 21.2%, 17.3%, 15.4%, and 13.4%, respectively. In contrast, the mono-detection rates of these serotypes were significantly lower: 9.5%, 6.9%, 0.9%, 0.9%, 4.3%, 0.9%, 3.5%, and 0.9%. The difference was statistically significant (p < 0.05). Serotypes 14, 20, 31, 38, 22F/22A, 23F, 33F/33A, and 39F were detected individually, with no accompanying serotypes.
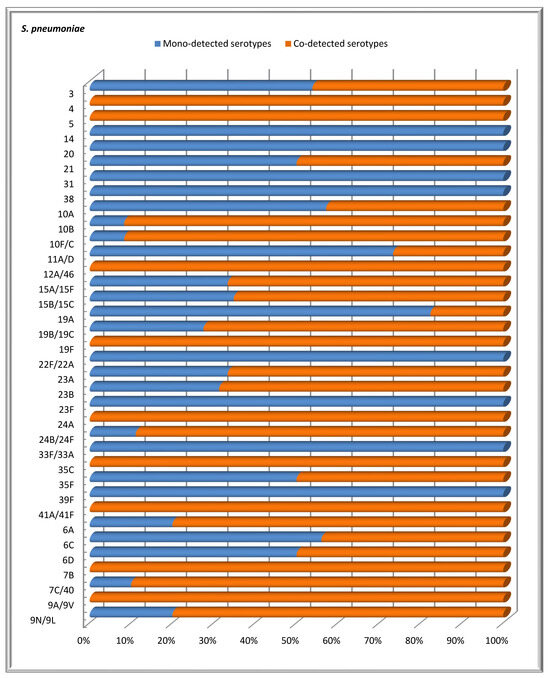
Figure 3.
The distribution of confirmed S. pneumoniae serotypes based on the proportions of mono- and co-detections among healthy children under 6 years of age.
This study found that the highest rate of co-carriage of multiple serotypes occurred in children aged 36 to 60 months, with a rate of 39.4%. In contrast, only 17.9% of children under 35 months had multiple serotypes; this difference was statistically significant (p = 0.0030). Among infants under 12 months of age, a small proportion (17.9%) were carriers of two serotypes, while in older age groups, the co-carriage of three, four, five, or even six serotypes of S. pneumoniae was observed (see Table 3).
Table 3.
The age distribution of co-detected serotypes of S. pneumoniae among healthy children in different age groups: under 12 months, 12–35 months, 36–59 months, and 5–6 years.
4. Discussion
Invasive pneumococcal disease continues to represent a significant global health challenge, even in developed countries, despite the introduction of the PCV vaccine. This study investigated the prevalence of S. pneumoniae over a 10-year period after the introduction of the PCV10 vaccine, which was added to the immunization schedule in Bulgaria. The results provide information on the effects of vaccination and other factors on nasopharyngeal colonization, changes in serotypes, and antimicrobial susceptibility of pneumococci.
S. pneumoniae is commonly found in the human nasopharynx, with prevalence ranging from 27% to 65% in children [24]. In our study, we observed a prevalence of 40.8%, which falls within this range. The high carriage rates may be due to the fact that many of the reported S. pneumoniae serotypes are not included in the PCV10 vaccine, leading to an increase in the total number of detected cases [25]. The predominant serotypes identified in our study include 19B/19C, 6C, 15B/15C, 19A, 23B, and 11A/D. A prospective study conducted in Marrakech, Morocco, between 2017 and 2018 followed healthy children attending vaccination centers. That study revealed an increased prevalence of serotypes 19B/19C and 15B/15C among these children [26]. The vaccination program implemented during this time is similar to that used in Bulgaria and involves the administration of PCV10. Additionally, a study conducted in infants in Belgium reported an increase in the prevalence of serotypes 6C and 19A during the transition period from PCV10 vaccination to PCV13 [27].
A Belgian study found that the increase in certain pneumococcal serotypes is linked to the vaccination strategy and the return to the use of the PCV10 vaccine [28]. This approach is similar to Bulgaria’s vaccination strategy, which also utilizes the PCV10 vaccine, despite it not covering specific serotypes. Notably, an increase in serotype 19A was observed after the switch to PCV10, particularly among children with invasive pneumococcal disease (IPD) [29]. This led to an increase in pediatric cases starting in 2017. By 2020, serotype 19A represented 19.3% of cases in Belgium, marking an increase of 3.8% compared with 2019 [27].
Recent studies have shown a worrying increase in the prevalence of serotype 6C in Bulgaria [30], mirroring findings from other countries [27,31]. In Belgium, for example, serotype 6C is implicated in 5.9% of IPD cases [29]. In our study, the prevalence of serotype 6C among children under 6 years of age was 10.7%. This increase was associated with the use of the pneumococcal conjugate vaccine PCV10 instead of PCV13 in Bulgaria. Although PCV13 does not directly target serotype 6C, its prevalence appears to be associated with serotype 6A, which is included in PCV13, possibly due to a presumed cross-protection between these two serotypes [32]. In addition, cases of tetracycline and erythromycin resistance have been documented alongside the increasing prevalence of serotype 6C [33,34].
In this follow-up study, lower levels of S. pneumoniae carriage were recorded in 2022 and 2023 compared with 2021 and 2024. This decrease may be due to non-pharmaceutical measures introduced during the COVID-19 pandemic, such as the closure of childcare facilities and the reduction in close contact between people [35]. A study in England reported that the overall incidence of invasive lung disease was lower in 2022–2023 than in 2019–2020 [36]. Therefore, after the lifting of these measures in 2022 and the official end of the pandemic in 2024, a significant increase in recorded carriage cases was observed. The diversity of identified serotypes reflects this pattern. While serotype diversity was noted in 2021, a slight decrease in diversity was observed in 2022 and 2023; however, we again observed an increase in the diversity of S. pneumoniae serotypes in 2024 and early 2025. There was no clear temporal relationship between serotypes, as they disappeared and then reappeared. For example, from 2013 to 2015, a predominance of serotypes 22F/22A was reported in Madrid [37]. However, these serotypes were not observed in Bulgaria until 2024. Thus, the distribution of the different serotypes shows different geographical characteristics. The prevalence of invasive serotypes of S. pneumoniae also varies geographically [38]. Colonization rates are higher among children during the fall and winter months, which coincides with an increase in colds and viral upper respiratory tract infections, often accompanied by nasal discharge [39].
S. pneumoniae shows age-related preferences in terms of carriage rates, influenced by geographic and seasonal factors. Studies have shown that children who are carriers play a key role in the transmission of pneumococci to the elderly. Approximately 10% of adults are asymptomatic carriers [40]. Noteworthily, children under 2 years of age have a lower rate of carriage compared to those aged 3 to 6 years. This difference may be due to the higher frequency of attendance at daycare and preschool compared with children under 3 years of age. Factors that increase the likelihood of asymptomatic carriage in children include attendance at daycare or school and the number of children living in the household [41]. While pneumococcal infections can affect people of all ages, children under two years of age and adults over 65 years of age are at significantly higher risk of developing complications [42]. A relationship has been established between the age group of the children and the prevalence of different serotypes. A study conducted in 2017 and 2018 found that serotypes 6C and 11A/D were more prevalent in children under 12 months of age [26], which aligns with our findings. However, we cannot confirm our conclusion that higher carriage of serotypes 19B/19C was observed in children over 36 months of age compared with younger children, as this is not supported by other studies.
Monitoring nasopharyngeal carriage in children hospitalized with clinical pneumonia revealed that half of the patients carried more than one serotype of S. pneumoniae simultaneously [43]. In contrast, our study found that only 9.1% of the examined healthy children carried multiple serotypes. This difference may be attributed to the fact that our study focused on healthy children, whereas the cited study concentrated on hospitalized patients. Thus, we can conclude that the carriage of multiple serotypes is more common among hospitalized children than among healthy children. Research has demonstrated that introducing vaccines with a higher number of vaccine serotypes leads to a reduction in the carriage of multiple serotypes [44]. We frequently detected serotypes 19B/19C together with other serotypes. Additionally, we identified other co-detected serotypes, including 10B, 10F/C, 23B, 7C/40, 23A, and 24A, that are not currently included in any of the available vaccines. This emphasizes the importance of creating new generations of vaccines that incorporate these co-detected serotypes. It is expected that addressing these serotypes will help reduce the incidence of pneumonia caused by non-vaccine pneumococcal serotypes.
The epidemiological results of this study show an increase in the simultaneous detection of more than two serotypes in children aged 5 to 6 years. This finding highlights the need to develop a vaccine that covers a greater percentage of non-vaccine serotypes. However, this study has some limitations, such as its narrow scope and including children from only 15 of the 28 regions in Bulgaria. Additionally, it is crucial to investigate the presence of S. pneumoniae in hospitalized patients of all ages to validate our findings regarding the effectiveness of the country’s vaccination strategy. We plan to conduct a future study focusing on hospitalized patients with respiratory symptoms to assess the carriage of S. pneumoniae. Furthermore, we did not analyze the antibiotic resistance of individual serotypes because we could not isolate them using conventional microbiological methods. To address this gap, we intend to conduct sequencing analysis in the future, which will help determine if any antibiotic resistance genes are present in the strains we encounter.
5. Conclusions
This review reveals a relatively high prevalence of S. pneumoniae carriage among healthy children up to 6 years of age who were vaccinated with PCV10. The study identified the predominant serotypes as 6C, 15B/15C, and 19A, while serotype 19B/19C was found to be the most common cause of both single and multiple nasopharyngeal colonization in children. Furthermore, children over 3 years of age were more likely to be colonized with more than two pneumococci. These findings highlight the need to review the childhood vaccination strategy. Such a change is essential to reduce the emergence and spread of antibiotic-resistant serotypes both in our country and in neighboring regions
Supplementary Materials
The following supporting information can be downloaded at: https://www.mdpi.com/article/10.3390/vaccines13060634/s1, Table S1 Sequence of primers and probes used in real-time PCR for detection of Streptococcus pneumoniae to the lytA gene. Thermal conditions for conducting the PCR reaction.
Author Contributions
I.T. and V.L., writing—review and editing, writing—original draft preparation, visualization, validation, and supervision; V.L., software, resources, project administration, methodology, formal analysis, data curation, and conceptualization; I.S., validation, resources, and formal analysis; M.I., validation and formal analysis; N.B. and T.K., validation, resources, data curation, investigation, and funding acquisition. All authors have read and agreed to the published version of the manuscript.
Funding
This study was supported by a grant from the Ministry of Education and Science, Bulgaria, Scientific Research Fund (contract project KP-06-H43/4-30.11.2020): “Molecular genetics identification and creation of an archival genomic bank of circulating S. pneumoniae in children, as well as analysis of common serotypes associated with the introduction of pneumococcal vaccines. in the Republic of Bulgaria”.
Institutional Review Board Statement
This study was conducted per the Declaration of Helsinki and the protocol was approved by the Ethics Committee of the National Centre of Infectious and Parasitic Diseases (00006384, protocol 2/2022: Bio-molecular identification and creation of an archival genomic bank of circulating S. pneumoniae in children, as well as epidemiological analysis of common serotypes associated with the introduction of pneumococcal vaccines in the Republic of Bulgaria).
Informed Consent Statement
All subjects gave their informed consent for inclusion before participating in this study.
Data Availability Statement
https://grippe.gateway.bg/page.php?category=77 accessed on 10 June 2025.
Acknowledgments
We would like to express our gratitude to the staff of the childcare facilities for their cooperation during sample collection. We also appreciate the efforts of our colleagues who participated in the sampling process. Finally, we are grateful to the parents who agreed to enroll their children in this study.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Weiser, J.N.; Ferreira, D.M.; Paton, J.C. Streptococcus pneumoniae: Transmission, colonization and invasion. Nat. Rev. Microbiol. 2018, 16, 355–367. [Google Scholar] [CrossRef]
- Ceyhan, M.; Ozsurekci, Y.; Aykac, K.; Hacibedel, B.; Ozbilgili, E. Economic burden of pneumococcal infections in children under 5 years of age. Hum. Vaccines Immunother. 2018, 14, 106–110. [Google Scholar] [CrossRef]
- Bogaert, D.; De Groot, R.; Hermans, P.W. Streptococcus pneumoniae colonisation: The key to pneumococcal disease. Lancet Infect. Dis. 2004, 4, 144–154. [Google Scholar] [CrossRef]
- Dekaj, E.; Gjini, E. Pneumococcus and the stress-gradient hypothesis: A trade-off links R0 and susceptibility to co-colonization across countries. Theor. Popul. Biol. 2024, 156, 77–92. [Google Scholar] [CrossRef]
- Brooks, L.R.K.; Mias, G.I. Streptococcus pneumoniae’s Virulence and Host Immunity: Aging, Diagnostics, and Prevention. Front. Immunol. 2018, 9, 1366. [Google Scholar] [CrossRef]
- Morimura, A.; Hamaguchi, S.; Akeda, Y.; Tomono, K. Mechanisms Underlying Pneumococcal Transmission and Factors Influencing Host-Pneumococcus Interaction: A Review. Front. Cell. Infect. Microbiol. 2021, 11, 639450. [Google Scholar] [CrossRef]
- Loughran, A.J.; Orihuela, C.J.; Tuomanen, E.I.; Fischetti, V.A.; Novick, R.P.; Ferretti, J.J.; Portnoy, D.A.; Braunstein, M.; Rood, J.I. Streptococcus pneumoniae: Invasion and Inflammation. Microbiol. Spectr. 2019, 7. [Google Scholar] [CrossRef]
- Ruiz-Ruiz, C.; Margüello, E.R. An immune system fighting against pneumococcus. Vacunas (Engl. Ed.) 2024, 25, 415–419. [Google Scholar] [CrossRef]
- Feemster, K.; Hausdorff, W.P.; Banniettis, N.; Platt, H.; Velentgas, P.; Esteves-Jaramillo, A.; Burton, R.L.; Nahm, M.H.; Buchwald, U.K. Implications of Cross-Reactivity and Cross-Protection for Pneumococcal Vaccine Development. Vaccines 2024, 12, 974. [Google Scholar] [CrossRef]
- Geno, K.A.; Gilbert, G.L.; Song, J.Y.; Skovsted, I.C.; Klugman, K.P.; Jones, C.; Konradsen, H.B.; Nahm, M.H. Pneumococcal Capsules and Their Types: Past, Present, and Future. Clin. Microbiol. Rev. 2015, 28, 871–899. [Google Scholar] [CrossRef]
- Wyllie, A.L.; Wijmenga-Monsuur, A.J.; van Houten, M.A.; Bosch, A.A.T.M.; Groot, J.A.; van Engelsdorp Gastelaars, J.; Bruin, J.P.; Bogaert, D.; Rots, N.Y.; Sanders, E.A.M.; et al. Molecular surveillance of nasopharyngeal carriage of Streptococcus pneumoniae in children vaccinated with conjugated polysaccharide pneumococcal vaccines. Sci. Rep. 2016, 6, 23809. [Google Scholar] [CrossRef]
- Ganaie, F.; Saad, J.S.; McGee, L.; van Tonder, A.J.; Bentley, S.D.; Lo, S.W.; Gladstone, R.A.; Turner, P.; Keenan, J.D.; Breiman, R.F.; et al. A New Pneumococcal Capsule Type, 10D, is the 100th Serotype and Has a Large cps Fragment from an Oral Streptococcus. mBio 2020, 11, e00937-20. [Google Scholar] [CrossRef]
- Johnson, C.N.; Wilde, S.; Tuomanen, E.; Rosch, J.W. Convergent impact of vaccination and antibiotic pressures on pneumococcal populations. Cell Chem. Biol. 2024, 31, 195–206. [Google Scholar] [CrossRef]
- Savrasova, L.; Villerusa, A.; Zeltina, I.; Krumina, A.; Cupeca, H.; Balasegaram, S.; Greve, M.; Savicka, O.; Selderina, S.; Galajeva, J.; et al. Streptococcus pneumoniae serotypes and factors associated with antimicrobial resistance in Invasive pneumococcal disease cases in Latvia, 2012–2022. Front. Public Health 2025, 13, 1501821. [Google Scholar] [CrossRef]
- Li, L.; Ma, J.; Yu, Z.; Li, M.; Zhang, W.; Sun, H. Epidemiological characteristics and antibiotic resistance mechanisms of Streptococcus pneumoniae: An updated review. Microbiol. Res. 2023, 266, 127221. [Google Scholar] [CrossRef]
- Musher, D.M.; Anderson, R.; Feldman, C. The remarkable history of pneumococcal vaccination: An ongoing challenge. Pneumonia (Nathan Qld.) 2022, 14, 5. [Google Scholar] [CrossRef]
- Aliberti, S.; Mantero, M.; Mirsaeidi, M.; Blasi, F. The role of vaccination in preventing pneumococcal disease in adults. Clin. Microbiol. Infect. 2014, 20, 52–58. [Google Scholar] [CrossRef]
- Rodgers, G.L.; Whitney, C.G.; Klugman, K.P. Triumph of Pneumococcal Conjugate Vaccines: Overcoming a Common Foe. J. Infect. Dis. 2021, 224 (Suppl. 2), S352–S359. [Google Scholar] [CrossRef]
- Bennett, J.C.; Deloria Knoll, M.; Kagucia, E.W.; Garcia Quesada, M.; Zeger, S.L.; Hetrich, M.K.; Yang, Y.; Herbert, C.; Ogyu, A.; Cohen, A.L.; et al. Global impact of ten-valent and 13-valent pneumococcal conjugate vaccines on invasive pneumococcal disease in all ages (the PSERENADE project): A global surveillance analysis. Lancet Infect. Dis. 2025s, 25, 457–470. [Google Scholar] [CrossRef]
- Malcheva, M. Streptococcus pneumoniae serotype distribution after the introduction of pneumococcal conjugate vaccines. Probl. Infect. Parasit. Dis. 2019, 47, 5–8. [Google Scholar] [CrossRef]
- Krieg Noel, R.; Holt John, G. Bergey’s Manual of Systematic Bacteriology; Yi Hsien Publishing Co.: Taipei, Taiwan, 1984. [Google Scholar]
- de Lamballerie, X.; Zandotti, C.; Vignoli, C.; Bollet, C.; de Micco, P. A one-step microbial DNA extraction method using “Chelex 100” suitable for gene amplification. Res. Microbiol. 1992, 143, 785–790. [Google Scholar] [CrossRef]
- Lang, A.L.S.; McNeil, S.A.; Hatchette, T.F.; Elsherif, M.; Martin, I.; LeBlanc, J.J. Detection and prediction of Streptococcus pneumoniae serotypes directly from nasopharyngeal swabs using PCR. J. Med. Microbiol. 2015, 64, 836–844. [Google Scholar] [CrossRef][Green Version]
- Zhao, W.; Pan, F.; Wang, B.; Wang, C.; Sun, Y.; Zhang, T.; Shi, Y.; Zhang, H. Epidemiology Characteristics of Streptococcus pneumoniae from Children with Pneumonia in Shanghai: A Retrospective Study. Front. Cell. Infect. Microbiol. 2019, 9, 258. [Google Scholar] [CrossRef]
- Candeias, C.; Almeida, S.T.; Paulo, A.C.; Simões, A.S.; Ferreira, B.; Cruz, A.R.; Queirós, M.; Touret, T.; Brito-Avô, A.; de Lencastre, H.; et al. Streptococcus pneumoniae carriage, serotypes, genotypes, and antimicrobial resistance trends among children in Portugal, after introduction of PCV13 in National Immunization Program: A cross-sectional study. Vaccine 2024, 42, 126219. [Google Scholar] [CrossRef]
- Warda, K.; Amari, S.; Boureddane, M.; Elkamouni, Y.; Arsalane, L.; Zouhair, S.; Bouskraoui, M. Changes in pneumococcal serotypes distribution and penicillin resistance in healthy children five years after generalization of PCV10. Heliyon 2024, 10, e25741. [Google Scholar] [CrossRef]
- Ekinci, E.; Van Heirstraeten, L.; Willen, L.; Desmet, S.; Wouters, I.; Vermeulen, H.; Lammens, C.; Goossens, H.; Van Damme, P.; Verhaegen, J.; et al. Serotype 19A and 6C Account for One-Third of Pneumococcal Carriage Among Belgian Day-Care Children Four Years After a Shift to a Lower-Valent, P.C.V. J. Pediatr. Infect. Dis. Soc. 2023, 12, 36–42. [Google Scholar] [CrossRef]
- Desmet, S.; Lagrou, K.; Wyndham-Thomas, C.; Braeye, T.; Verhaegen, J.; Maes, P.; Fieuws, S.; Peetermans, W.E.; Blumental, S. Dynamic changes in paediatric invasive pneumococcal disease after sequential switches of conjugate vaccine in Belgium: A national retrospective observational study. Lancet Infect. Dis. 2021, 21, 127–136. [Google Scholar] [CrossRef]
- Desmet, S.; Wouters, I.; Heirstraeten, L.V.; Beutels, P.; Van Damme, P.; Malhotra-Kumar, S.; Maes, P.; Verhaegen, J.; Peetermans, W.E.; Lagrou, K.; et al. In-depth analysis of pneumococcal serotypes in Belgian children (2015–2018): Diversity, invasive disease potential, and antimicrobial susceptibility in carriage and disease. Vaccine 2021, 39, 372–379. [Google Scholar] [CrossRef]
- Alexandrova, A.S.; Setchanova, L.P.; Pencheva, D.R.; Mitov, I.G. Phenotypic and genotypic characterization of serogroup 6 Streptococcus pneumoniae isolates collected during 10-valent pneumococcal conjugate vaccine era in Bulgaria. Acta Microbiol. Et Immunol. Hung. 2020, 67, 91–99. [Google Scholar] [CrossRef]
- lmeida, S.C.G.; Lemos, A.P.S.; Bierrenbach, A.L.; Moraes, J.C.; Brandileone, M.C.C. Serotype Distribution and Antimicrobial Susceptibility Pattern of Streptococcus pneumoniae in COVID-19 Pandemic Era in Brazil. Microorganisms 2024, 12, 401. [Google Scholar] [CrossRef]
- Naucler, P.; Galanis, I.; Morfeldt, E.; Darenberg, J.; Örtqvist, Å.; Henriques-Normark, B. Comparison of the Impact of Pneumococcal Conjugate Vaccine 10 or Pneumococcal Conjugate Vaccine 13 on Invasive Pneumococcal Disease in Equivalent Populations. Clin. Infect. Dis. 2017, 65, 1780–1789. [Google Scholar] [CrossRef]
- Gabarrot, G.G.; Vega, M.L.; Giffoni, G.P.; Hortal, M.; Camou, T. Antibiotic Resistance and Clonal Spread. Pneumonia 2014, 3, 204–221. [Google Scholar] [CrossRef]
- Neves, F.P.G.; Cardoso, N.T.; Souza, A.R.V.; Snyder, R.E.; Marlow, M.M.; Pinto, T.C.A.; Teixeira, L.M.; Riley, L.W. Population structure of Streptococcus pneumoniae colonizing children before and after universal use of pneumococcal conjugate vaccines in Brazil: Emergence and expansion of the MDR serotype 6C-CC386 lineage. J. Antimicrob. Chemother. 2018, 73, 1206–1212. [Google Scholar] [CrossRef]
- Duval, D.; Evans, B.; Sanders, A.; Hill, J.; Simbo, A.; Kavoi, T.; Lyell, I.; Simmons, Z.; Qureshi, M.; Pearce-Smith, N.; et al. Non-pharmaceutical interventions to reduce COVID-19 transmission in the UK: A rapid mapping review and interactive evidence gap map. J. Public Health (Oxf. Engl.) 2024, 46, e279–e293. [Google Scholar] [CrossRef]
- Bertran, M.; D’Aeth, J.C.; Abdullahi, F.; Eletu, S.; Andrews, N.J.; Ramsay, M.E.; Litt, D.J.; Ladhani, S.N. Invasive pneumococcal disease 3 years after introduction of a reduced 1 + 1 infant 13-valent pneumococcal conjugate vaccine immunisation schedule in England: A prospective national observational surveillance study. Lancet Infect. Dis. 2024, 24, 546–556. [Google Scholar] [CrossRef]
- Sanz, J.C.; de Luis, R.; Del Río, S.; Gamen, S.; Cercenado, E.; Orellana, M.A.; Yuste, J. Direct identification of pneumococcal serotypes in blood cultures by a PCR-reverse-hybridisation technique. Enfermedades Infecc. Microbiol. Clin. (Engl. Ed.) 2020, 38, 170–173. [Google Scholar] [CrossRef]
- Maeda, H.; Morimoto, K. Global distribution and characteristics of pneumococcal serotypes in adults. Hum. Vaccines Immunother. 2025, 21, 2469424. [Google Scholar] [CrossRef]
- Korona-Glowniak, I.; Malm, A. Characteristics of Streptococcus pneumoniae strains colonizing upper respiratory tract of healthy preschool children in Poland. Sci. World J. 2012, 732901. [Google Scholar] [CrossRef]
- Torén, K.; Albin, M.; Alderling, M.; Schiöler, L.; Åberg, M. Transmission factors and exposure to infections at work and invasive pneumococcal disease. Am. J. Ind. Med. 2023, 66, 65–74. [Google Scholar] [CrossRef]
- Parker, A.M.; Jackson, N.; Awasthi, S.; Kim, H.; Alwan, T.; Wyllie, A.L.; Kogut, K.; Holland, N.; Mora, A.M.; Eskenazi, B.; et al. Upper respiratory Streptococcus pneumoniae colonization among working-age adults with prevalent exposure to overcrowding. Microbiol. Spectr. 2024, 12, e0087924. [Google Scholar] [CrossRef]
- Tan Tina, Q. Pediatric invasive pneumococcal disease in the United States in the era of pneumococcal conjugate vaccines. Clin. Microbiol. Rev. 2012, 25, 409–419. [Google Scholar] [CrossRef]
- Jullien, S.; Sharma, R.; Lhamu Mynak, M.; Henares, D.; Muñoz-Almagro, C.; Bassat, Q. Pneumococcal nasopharyngeal carriage among Bhutanese children hospitalized with clinical pneumonia: Serotypes and viral co-infection. BMC Infect. Dis. 2020, 20, 940. [Google Scholar] [CrossRef]
- Dhoubhadel, B.G.; Suzuki, M.; Ishifuji, T.; Yaegashi, M.; Asoh, N.; Ishida, M.; Hamaguchi, S.; Aoshima, M.; Yasunami, M.; Ariyoshi, K.; et al. High prevalence of multiple serotypes of pneumococci in patients with pneumonia and their associated risk factors. Thorax 2022, 77, 1121–1130. [Google Scholar] [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).