

Changes in Confidence, Feelings, and Perceived Necessity Concerning COVID-19 Booster

Abstract
1. Introduction
2. Methods
2.1. Participants and Data Collection
2.2. Measures
- Confidence (“How confident are you with the COVID-19 vaccines (including the updated booster in 2022) available in the U.S.”? from very to not at all confident).
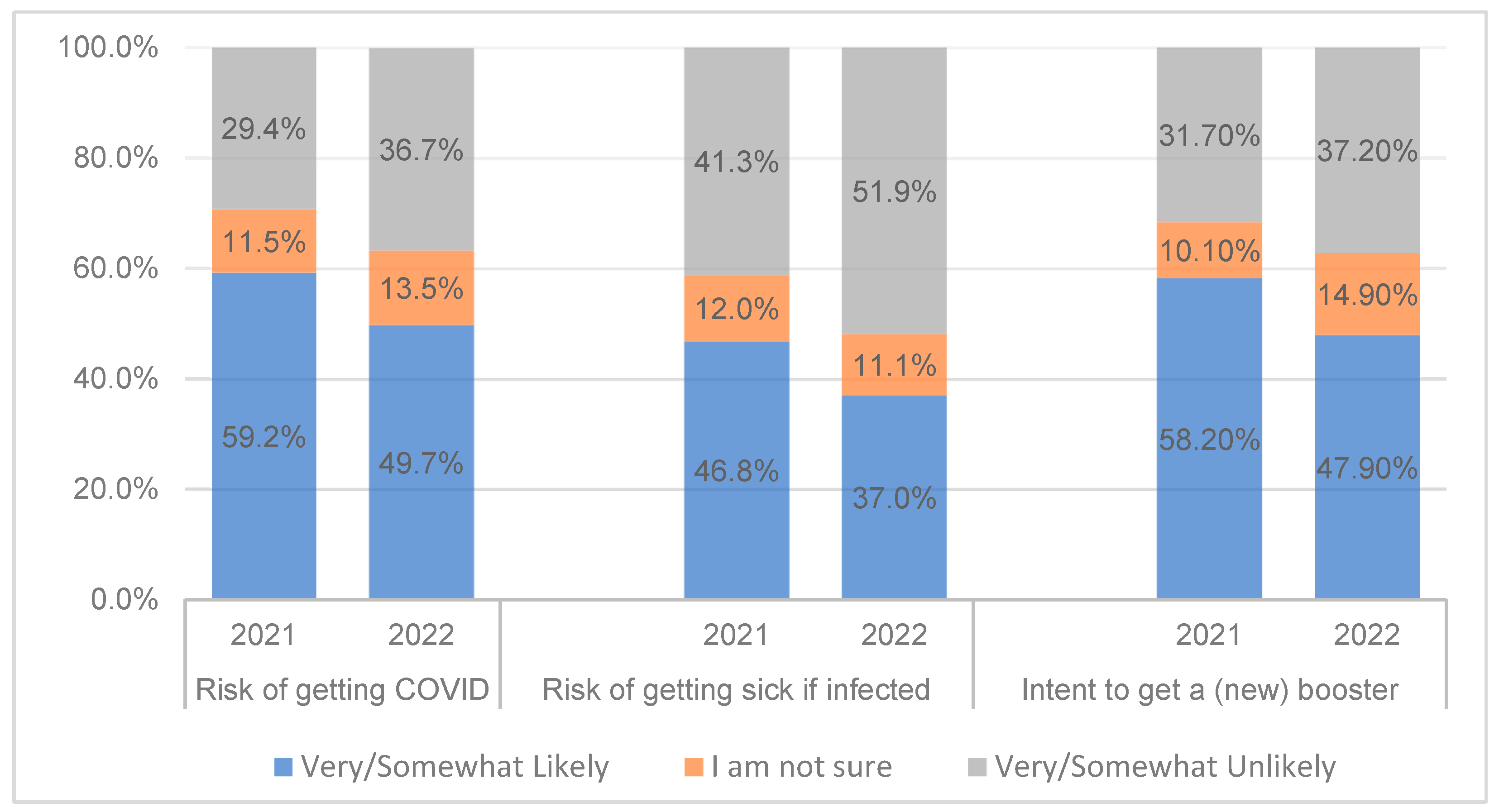
- Perceived vaccine necessity, according to perceived risk of infection (“How likely do you think you would get COVID-19”? and “If you contracted COVID, how likely is it that you would get very sick”?), experienced risk (“Did you ever get COVID-19”?), and perceived pandemic seriousness (“From what you know, how serious is the current COVID-19 situation”?).
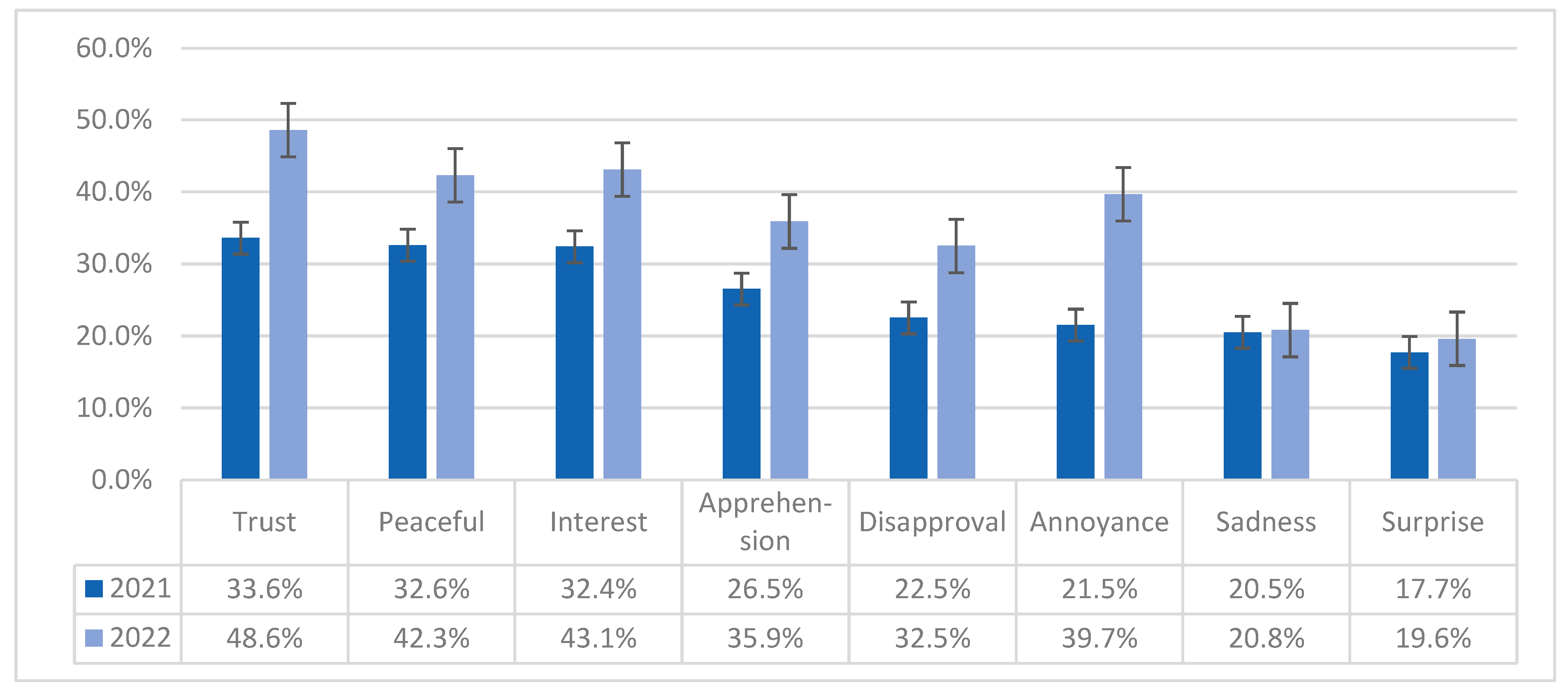
- Prevalent emotions regarding the COVID booster: emotions were first assessed in 2021 by asking participants whether the booster made them feel any of the 24 common emotions (shown in random order) under the eight dimensions described in Plutchik’s Wheel of Emotions [34,38] with a yes/no response. The most prevalent emotion in each of the eight dimensions (annoyance, disapproval, apprehension, sadness, interest, peaceful, surprise, and trust) observed in 2021 were again assessed in our 2022 survey for comparison. Participants in both surveys also were asked how well the words hope and frustrated described how the booster made them feel (on a scale of 1–10).
2.3. Data Analysis
3. Results
3.1. Vaccination Acceptance and Refusal
3.2. Booster Uptake and Intention
3.3. Perceived and Experienced Risk of COVID-19
3.4. Confidence and Hope
3.5. Emotions Elicited by the Booster
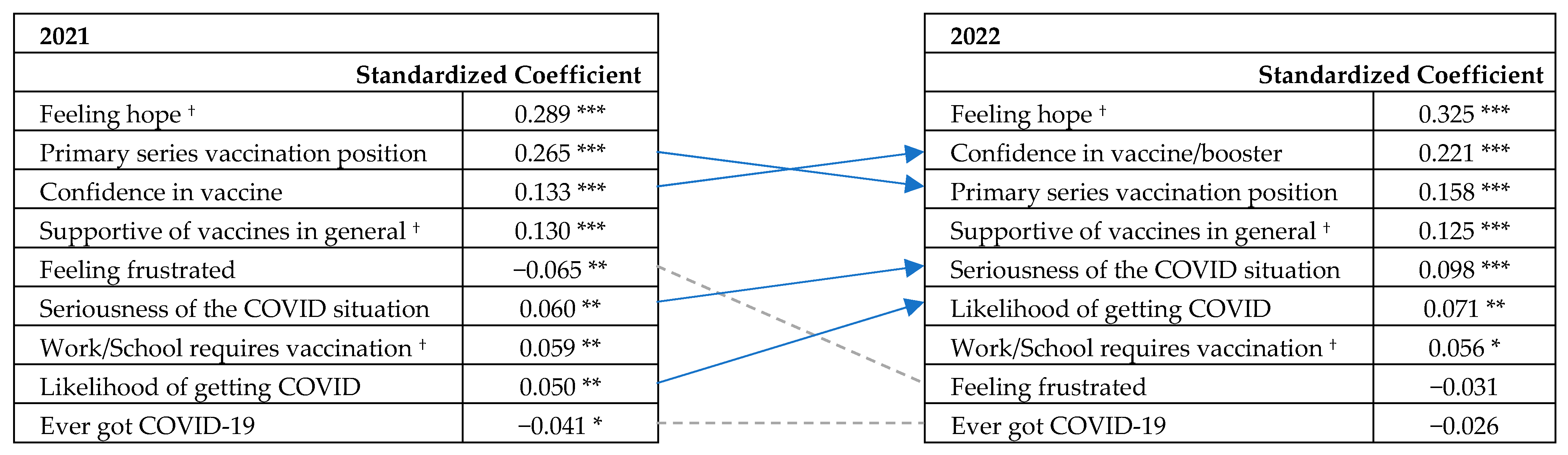
3.6. The Significance of Feeling Hope, Confidence, and Vaccination History
4. Discussion
Limitations and Future Research
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- CDC. CDC Strengthens Recommendations and Expands Eligibility for COVID-19 Booster Shots. Available online: https://www.cdc.gov/media/releases/2022/s0519-covid-booster-acip.html (accessed on 2 January 2023).
- CDC. COVID Data Tracker—Vaccination and Case Trends of COVID-19 in the US. Available online: https://covid.cdc.gov/covid-data-tracker/#vaccinations-cases-trends (accessed on 16 May 2023).
- CDC. CDC Recommends the First Updated COVID-19 Booster. Available online: https://www.cdc.gov/media/releases/2022/s0901-covid-19-booster.html (accessed on 24 March 2023).
- Bendix, A. Less than 4% of Eligible People Have Gotten Updated Covid Booster Shots, One Month into the Rollout. NBC News, 23 September 2022. Available online: https://www.nbcnews.com/health/health-news/updated-covid-booster-shots-doses-administered-cdc-rcna48960 (accessed on 26 October 2022).
- Wouters, O.J.; Shadlen, K.C.; Salcher-Konrad, M.; Pollard, A.J.; Larson, H.J.; Teerawattananon, Y.; Jit, M. Challenges in Ensuring Global Access to COVID-19 Vaccines: Production, Affordability, Allocation, and Deployment. Lancet 2021, 397, 1023–1034. [Google Scholar] [CrossRef] [PubMed]
- Lai, X.; Zhu, H.; Wang, J.; Huang, Y.; Jing, R.; Lyu, Y.; Zhang, H.; Feng, H.; Guo, J.; Fang, H. Public Perceptions and Acceptance of COVID-19 Booster Vaccination in China: A Cross-Sectional Study. Vaccines 2021, 9, 1461. [Google Scholar] [CrossRef] [PubMed]
- Rzymski, P.; Poniedziałek, B.; Fal, A. Willingness to Receive the Booster COVID-19 Vaccine Dose in Poland. Vaccines 2021, 9, 1286. [Google Scholar] [CrossRef] [PubMed]
- Paul, E.; Fancourt, D. Predictors of Uncertainty and Unwillingness to Receive the COVID-19 Booster Vaccine: An Observational Study of 22,139 Fully Vaccinated Adults in the UK. Lancet Reg. Health—Eur. 2022, 14, 100317. [Google Scholar] [CrossRef] [PubMed]
- Neely, S.R.; Scacco, J.M. Receptiveness of American Adults to COVID-19 Vaccine Boosters: A Survey Analysis. PEC Innov. 2022, 1, 100019. [Google Scholar] [CrossRef] [PubMed]
- Ouyang, H.; Ma, X.; Wu, X. The Prevalence and Determinants of COVID-19 Vaccine Hesitancy in the Age of Infodemic. Hum. Vaccines Immunother. 2022, 18, 2013694. [Google Scholar] [CrossRef]
- Lorini, C.; Collini, F.; Gasparini, F.; Paolini, D.; Grazzini, M.; Ierardi, F.; Galletti, G.; Zanobini, P.; Gemmi, F.; Bonaccorsi, G. Health Literacy, Vaccine Confidence and Influenza Vaccination Uptake among Nursing Home Staff: A Cross-Sectional Study Conducted in Tuscany. Vaccines 2020, 8, 154. [Google Scholar] [CrossRef]
- Wang, P.-W.; Ahorsu, D.K.; Lin, C.-Y.; Chen, I.-H.; Yen, C.-F.; Kuo, Y.-J.; Griffiths, M.D.; Pakpour, A.H. Motivation to Have COVID-19 Vaccination Explained Using an Extended Protection Motivation Theory among University Students in China: The Role of Information Sources. Vaccines 2021, 9, 380. [Google Scholar] [CrossRef]
- Ezati Rad, R.; Mohseni, S.; Kamalzadeh Takhti, H.; Hassani Azad, M.; Shahabi, N.; Aghamolaei, T.; Norozian, F. Application of the Protection Motivation Theory for Predicting COVID-19 Preventive Behaviors in Hormozgan, Iran: A Cross-Sectional Study. BMC Public Health 2021, 21, 466. [Google Scholar] [CrossRef]
- Corace, K.; Prematunge, C.; McCarthy, A.; Nair, R.C.; Roth, V.; Hayes, T.; Suh, K.N.; Balfour, L.; Garber, G. Predicting Influenza Vaccination Uptake among Health Care Workers: What Are the Key Motivators? Am. J. Infect. Control 2013, 41, 679–684. [Google Scholar] [CrossRef]
- Luk, T.T.; Lui, J.H.T.; Wang, M.P. Efficacy, Usability, and Acceptability of a Chatbot for Promoting COVID-19 Vaccination in Unvaccinated or Booster-Hesitant Young Adults: Pre-Post Pilot Study. J. Med. Internet Res. 2022, 24, e39063. [Google Scholar] [CrossRef]
- Batra, K.; Sharma, M.; Dai, C.-L.; Khubchandani, J. COVID-19 Booster Vaccination Hesitancy in the United States: A Multi-Theory-Model (MTM)-Based National Assessment. Vaccines 2022, 10, 758. [Google Scholar] [CrossRef] [PubMed]
- CDC. CDC’s State of Vaccine Confidence Insights Report; CDC: Atlanta, GA, USA, 2022. [Google Scholar]
- Lin, C.; Bier, B.; Tu, R.; Paat, J.J.; Tu, P. Vaccinated Yet Booster-Hesitant: Perspectives from Boosted, Non-Boosted, and Unvaccinated Individuals. Vaccines 2023, 11, 550. [Google Scholar] [CrossRef]
- Prater, E. Many Americans Are Shunning the Omicron COVID Booster. What It Means for the Coming Season as the Virus Mutates. Available online: https://fortune.com/well/2022/10/09/americans-hesitant-omicron-covid-booster-shot-vaccine-coroanvirus-forecast-fall-winter/ (accessed on 6 February 2023).
- Herper, M. Pfizer Seeks Authorization for Updated Covid Vaccine, without Fresh Clinical Trial Data. Available online: https://www.statnews.com/2022/08/22/pfizer-seeks-authorization-for-updated-covid-vaccine-without-fresh-clinical-trial-data/ (accessed on 6 February 2023).
- Aboulenein, A.; Kahn, C. Most Vaccinated Americans Want COVID-19 Booster Shots—Reuters/Ipsos Poll. Available online: https://www.reuters.com/business/healthcare-pharmaceuticals/most-vaccinated-americans-want-covid-19-booster-shots-reutersipsos-poll-2021-09-01/ (accessed on 15 January 2022).
- Yadete, T.; Batra, K.; Netski, D.M.; Antonio, S.; Patros, M.J.; Bester, J.C. Assessing Acceptability of COVID-19 Vaccine Booster Dose among Adult Americans: A Cross-Sectional Study. Vaccines 2021, 9, 1424. [Google Scholar] [CrossRef] [PubMed]
- Ipsos. Global Attitudes on COVID-19 Vaccine Booster Shots; Game Changers; Ipsos: Singapore, 2021. [Google Scholar]
- Sønderskov, K.M.; Vistisen, H.T.; Dinesen, P.T.; Østergaard, S.D. COVID-19 Booster Vaccine Willingness. Dan. Med. J. 2022, 69, A10210765. [Google Scholar]
- Pal, S.; Shekhar, R.; Kottewar, S.; Upadhyay, S.; Singh, M.; Pathak, D.; Kapuria, D.; Barrett, E.; Sheikh, A.B. COVID-19 Vaccine Hesitancy and Attitude toward Booster Doses among US Healthcare Workers. Vaccines 2021, 9, 1358. [Google Scholar] [CrossRef] [PubMed]
- Mellers, B.A.; Schwartz, A.; Ho, K.; Ritov, I. Decision Affect Theory: Emotional Reactions to the Outcomes of Risky Options. Psychol. Sci. 1997, 8, 423–429. [Google Scholar] [CrossRef]
- Conner, M.; Norman, P. Understanding the Intention-Behavior Gap: The Role of Intention Strength. Front. Psychol. 2022, 13, 923464. [Google Scholar] [CrossRef] [PubMed]
- Chou, W.-Y.S.; Budenz, A. Considering Emotion in COVID-19 Vaccine Communication: Addressing Vaccine Hesitancy and Fostering Vaccine Confidence. Health Commun. 2020, 35, 1718–1722. [Google Scholar] [CrossRef]
- Betsch, C.; Ulshöfer, C.; Renkewitz, F.; Betsch, T. The Influence of Narrative v. Statistical Information on Perceiving Vaccination Risks. Med. Decis. Mak. 2011, 31, 742–753. [Google Scholar] [CrossRef]
- Jordan, J.; Yoeli, E.; Rand, D.G. Don’t Get It or Don’t Spread It: Comparing Self-Interested versus Prosocial Motivations for COVID-19 Prevention Behaviors. Sci. Rep. 2021, 11, 20222. [Google Scholar] [CrossRef]
- Heffner, J.; Vives, M.-L.; FeldmanHall, O. Emotional Responses to Prosocial Messages Increase Willingness to Self-Isolate during the COVID-19 Pandemic. Pers. Individ Dif. 2021, 170, 110420. [Google Scholar] [CrossRef]
- Hensley, S. An FDA Committee Votes to Roll out a New COVID Vaccination Strategy. Available online: https://www.npr.org/sections/health-shots/2023/01/26/1151810765/fda-committee-votes-to-roll-out-new-covid-vaccination-strategy (accessed on 29 January 2023).
- Office of the FDA Commissioner FDA Authorizes Moderna, Pfizer-BioNTech Bivalent COVID-19 Vaccines for Use as a Booster Dose. Available online: https://www.fda.gov/news-events/press-announcements/coronavirus-covid-19-update-fda-authorizes-moderna-pfizer-biontech-bivalent-covid-19-vaccines-use (accessed on 5 April 2023).
- Plutchik, R. The Nature of Emotions: Human Emotions Have Deep Evolutionary Roots, a Fact That May Explain Their Complexity and Provide Tools for Clinical Practice. Am. Sci. 2001, 89, 344–350. [Google Scholar] [CrossRef]
- Plutchik, R. Emotions and Life: Perspectives From Psychology, Biology, and Evolution; American Psychological Association: Washington, DC, USA, 2002; ISBN 978-1-55798-949-9. [Google Scholar]
- CDC. CDC Expands Eligibility for COVID-19 Booster Shots to All Adults. Available online: https://www.cdc.gov/media/releases/2021/s1119-booster-shots.html (accessed on 23 November 2021).
- Federal Trade Commission. Children’s Online Privacy Protection Rule; Federal Trade Commission: Washington, DC, USA, 2013. [Google Scholar]
- Plutchik, R. A Psychoevolutionary Theory of Emotions. Soc. Sci. Inf. 1982, 21, 529–553. [Google Scholar] [CrossRef]
- R Core Team. R: A Language and Environment for Statistical Computing; R Core Team: Vienna, Austria, 2020. [Google Scholar]
- Mbaeyi, S. The Advisory Committee on Immunization Practices’ Interim Recommendations for Additional Primary and Booster Doses of COVID-19 Vaccines—United States, 2021. MMWR Morb. Mortal. Wkly. Rep. 2021, 70, 1545–1552. [Google Scholar] [CrossRef]
- Kim, J.H. Multicollinearity and Misleading Statistical Results. Korean J. Anesthesiol. 2019, 72, 558–569. [Google Scholar] [CrossRef]
- COVID-19: Cancellation of Public Events and Gatherings. Available online: https://ourworldindata.org/covid-cancel-public-events (accessed on 30 March 2023).
- Yang, L.; Grenfell, B.T.; Mina, M.J. Waning Immunity and Re-Emergence of Measles and Mumps in the Vaccine Era. Curr. Opin. Virol. 2020, 40, 48–54. [Google Scholar] [CrossRef]
- CDC Global Measles Outbreaks. Available online: https://www.cdc.gov/globalhealth/measles/data/global-measles-outbreaks.html (accessed on 22 May 2023).
- Half the, U.S. Population Has Had COVID, but Many Cases Are Going Unreported. Available online: https://www.hks.harvard.edu/faculty-research/policy-topics/health/half-us-population-has-had-covid-many-cases-are-going (accessed on 30 March 2023).
- Institute for Health Metrics and Evaluation. COVID-19 Results Briefing; Institute for Health Metrics and Evaluation: Seattle, WA, USA, 2022. [Google Scholar]
- Galanis, P.; Vraka, I.; Katsiroumpa, A.; Siskou, O.; Konstantakopoulou, O.; Katsoulas, T.; Mariolis-Sapsakos, T.; Kaitelidou, D. First COVID-19 Booster Dose in the General Population: A Systematic Review and Meta-Analysis of Willingness and Its Predictors. Vaccines 2022, 10, 1097. [Google Scholar] [CrossRef]
- Quinn, S.C.; Jamison, A.M.; An, J.; Hancock, G.R.; Freimuth, V.S. Measuring Vaccine Hesitancy, Confidence, Trust and Flu Vaccine Uptake: Results of a National Survey of White and African American Adults. Vaccine 2019, 37, 1168–1173. [Google Scholar] [CrossRef]
- Lin, C.; Tu, P.; Beitsch, L.M. Confidence and Receptivity for COVID-19 Vaccines: A Rapid Systematic Review. Vaccines 2020, 9, 16. [Google Scholar] [CrossRef]
- McGinley, L.; Sun, L. FDA to Okay Second Omicron-Targeting Booster for Some, Officials Say. Washington Post. Available online: https://www.washingtonpost.com/health/2023/04/03/covid-booster-shot/ (accessed on 5 May 2023).




{kind=link}
{kind=link}
{kind=link}
| Demographics | Survey 1 (2021) n = 1889 | Survey 2 (2022) n = 1319 | |
|---|---|---|---|
| Age | 13–15 | 179 (9.5%) | 125 (9.5%) |
| 16–17 | 262 (13.9%) | 149 (11.3%) | |
| 18–29 | 343 (18.2%) | 252 (19.1%) | |
| 30–39 | 288 (15.2%) | 174 (13.2%) | |
| 40–49 | 414 (21.9%) | 199 (15.1%) | |
| 50–64 | 272 (14.4%) | 228 (17.3%) | |
| 65 and above | 131 (6.9%) | 192 (14.6%) | |
| Gender most closely identifies with | Female | 966 (46.5%) | 691 (52.3%) |
| Male | 879 (51.1%) | 610 (46.2%) | |
| Other/Prefer not to answer | 44 (2.3%) | 18 (1.4%) | |
| Race/ethnicity best describes you | American Indian/Native American | 30 (1.6%) | 27 (2.1%) |
| Asian/Pacific Islander | 110 (5.8%) | 57 (4.3%) | |
| Black/African American | 235 (12.4%) | 185 (14.0%) | |
| Hispanic/Latino | 167 (8.8%) | 209 (15.6%) | |
| White | 1280 (67.8%) | 803 (60.9%) | |
| Other/Prefer not to answer | 67 (3.5%) | 38 (2.9%) | |
| Educational level | Some high school or less | 399 (21.2%) | 288 (21.8%) |
| High school or equivalent | 465 (24.6%) | 380 (28.8%) | |
| Some college or trade school | 378 (20.0%) | 270 (20.5%) | |
| College degree | 416 (22.0%) | 259 (19.6%) | |
| Graduate/professional degree | 225 (11.9%) | 100 (7.6%) | |
| Other/Prefer not to answer | 6 (0.3%) | 22 (1.7%) | |
| Annual household income (US$) * | <$25,000 | 251 (21.2%) | 336 (32.2%) |
| $25,000–$49,999 | 305 (25.7%) | 305 (29.1%) | |
| $50,000–$99,999 | 338 (28.5%) | 247 (23.6%) | |
| $100,000–$199,999 | 209 (17.6%) | 99 (9.5%) | |
| >$200,000 | 44 (3.7%) | 20 (1.9%) | |
| Prefer not to answer | 39 (3.3%) | 38 (3.6%) |
| Survey 1 (2021) n = 1889 | Survey 2 (2022) n = 1319 | |
|---|---|---|
| Primary series vaccination status | ||
| Fully vaccinated (2 doses of Pfizer/Moderna or 1 dose of J&J) | 1099 (58.1%) | 861 (65.3%) |
| Partially vaccinated (1 dose of Pfizer/Moderna) | 84 (4.5%) | 47 (3.6%) |
| Planned to get vaccinated | 144 (7.6%) | -- |
| Did not plan to get it †/not vaccinated ‡ | 380 (20.1%) | 389 (29.5%) |
| Not sure † (still undecided) | 182 (9.6%) | -- |
| Unsure ‡ (of my vaccination status) | -- | 22 (1.7%) |
| Booster status ‡ | ||
| Non-boosted: did not plan to get boosted | 467 (35.4%) | |
| planned to get boosted | 137 (10.4%) | |
| Boosted: received 1 booster | 255 (19.3%) | |
| received 2 boosters | 251 (19.0%) | |
| received 3 or more boosters | 159 (12.1%) | |
| Was not sure (of the status) | 50 (3.8%) | |
| Booster intention | ||
| “If and when a (new ‡) COVID-19 booster becomes available to you, would you get it”? | ||
| I already got a booster shot † | 172 (9.1%) | -- |
| Very likely | 673 (35.6%) | 405 (30.7%) |
| Somewhat likely | 255 (13.5%) | 227 (17.2%) |
| Not very likely | 174 (9.2%) | 194 (14.7%) |
| Not at all likely | 425 (22.5%) | 297 (22.5%) |
| I am not sure | 190 (10.1%) | 196 (14.9%) |
| Primary Series Position | Vaccinated | Uncommitted * | Did Not Plan to Get Vaccinated | |||
|---|---|---|---|---|---|---|
| 2021 n = 1149 (60.8%) | 2022 n = 861 (65.3%) | 2021 n = 360 (19.1%) | 2022 n = 69 (5.2%) | 2021 n = 380 (20.1%) | 2022 n = 389 (29.5%) | |
| Booster intention † | ||||||
| Very/somewhat likely to get a booster | 82.8% | 67.1% | 38.6% | 29.0% | 2.6% | 8.7% |
| Unlikely to get a booster/not sure | 7.2% | 25.1% | 24.2% | 43.5% | 5.3% | 37.0% |
| Not getting a booster | 10.0% | 7.8% | 37.2% | 27.5% | 92.1% | 54.2% |
| Primary Series Uptake | Booster Intention | Booster Uptake | |||
|---|---|---|---|---|---|
| 2021 | 2022 | 2021 | 2022 | 2022 | |
| Primary series vaccination uptake | 1 | 1 | 0.728 *** | 0.617 *** | 0.610 *** |
| Booster Intention | 0.728 *** | 0.617 *** | 1 | 1 | 0.637 *** |
| Confidence in COVID-19 vaccine (and booster ‡) | 0.670 *** | 0.650 *** | 0.712 *** | 0.710 *** | 0.562 *** |
| Emotions toward the booster | |||||
| Feeling hope | 0.619 *** | 0.550 *** | 0.731 *** | 0.696 *** | 0.548 *** |
| Feeling frustrated | −0.474 *** | −0.237 *** | −0.538 *** | −0.325 *** | −0.217 *** |
| Supportive of vaccine in general | 0.615 *** | 0.582 *** | 0.655 *** | 0.631 *** | 0.473 *** |
| Usually get the annual flu shot | 0.401 *** | 0.417 *** | 0.441 *** | 0.506 *** | 0.402 *** |
| Work or school requires COVID-19 vaccination | 0.325 *** | 0.463 *** | 0.330 *** | 0.446 *** | 0.428 *** |
| Perceived necessity and risk | |||||
| Likelihood of getting COVID-19 without vaccine † / booster ‡ | 0.448 *** | 0.409 *** | 0.456 *** | 0.391 *** | 0.301 *** |
| Likelihood of getting very sick if infected | 0.193 *** | 0.084 ** | 0.260 *** | 0.183 *** | 0.100 *** |
| Seriousness of the pandemic | 0.332 *** | 0.256 *** | 0.414 *** | 0.428 *** | 0.306 *** |
| Ever got COVID-19 | −0.081 ** | −0.003 | −0.091 *** | −0.041 | −0.013 |
| Education level | 0.221 *** | 0.163 *** | 0.174 *** | 0.165 *** | 0.228 *** |
| Household income | 0.232 *** | 0.148 *** | 0.171 *** | 0.129 *** | 0.233 *** |
| Survey 1 (2021) n = 1889 | Survey 2 (2022) n = 1319 | |
|---|---|---|
| Vaccine confidence | ||
| “How confident are you with the COVID-19 vaccines (including the booster ‡) | ||
| Very confident | 737 (39.0%) | 446 (33.8%) |
| Somewhat confident | 532 (28.2%) | 364 (27.6%) |
| Not very confident | 217 (11.5%) | 177 (13.4%) |
| Not at all confident | 312 (16.5%) | 237 (18.0%) |
| I don’t know | 91 (4.8%) | 95 (7.2%) |
| “Has the discussion about boosters changed your confidence in the COVID-19 vaccine”? | ||
| A lot more confident | 360 (19.1%) | 243 (18.4%) |
| Somewhat more confident | 240 (12.7%) | 240 (18.2%) |
| The booster has not changed my opinion about the vaccine | 749 (39.4%) | 503 (38.1%) |
| Somewhat less confident | 145 (7.7%) | 86 (6.5%) |
| A lot less confident | 313 (16.6%) | 169 (12.8%) |
| I have not heard about a booster or don’t understand what it is | 82 (4.3%) | 78 (5.6%) |
| Risk assessment | ||
| “From what you know, how serious is the current COVID-19 situation”? | ||
| Very serious | 881 (46.6%) | 343 (26.0%) |
| Somewhat serious | 648 (34.3%) | 396 (30.0%) |
| A minor concern | 269 (14.2%) | 365 (27.7%) |
| Not really a concern | 91 (4.8%) | 215 (16.3%) |
| Feelings toward the booster | ||
| “How well do each of these words describe how the COVID-19 booster makes you feel”? (1 = not at all, 10 = extremely) | ||
| Mean [SD] | Mean [SD] | |
| Hopeful ** | 6.22 [3.20] | 5.65 [3.33] |
| Frustrated | 4.81 [3.36] | 4.47 [3.21] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lin, C.; Bier, B.; Reed, A.M.; Paat, J.J.; Tu, P. Changes in Confidence, Feelings, and Perceived Necessity Concerning COVID-19 Booster. Vaccines 2023, 11, 1244. https://doi.org/10.3390/vaccines11071244
Lin C, Bier B, Reed AM, Paat JJ, Tu P. Changes in Confidence, Feelings, and Perceived Necessity Concerning COVID-19 Booster. Vaccines. 2023; 11(7):1244. https://doi.org/10.3390/vaccines11071244
Chicago/Turabian StyleLin, Cheryl, Brooke Bier, Ann M. Reed, John J. Paat, and Pikuei Tu. 2023. "Changes in Confidence, Feelings, and Perceived Necessity Concerning COVID-19 Booster" Vaccines 11, no. 7: 1244. https://doi.org/10.3390/vaccines11071244
APA StyleLin, C., Bier, B., Reed, A. M., Paat, J. J., & Tu, P. (2023). Changes in Confidence, Feelings, and Perceived Necessity Concerning COVID-19 Booster. Vaccines, 11(7), 1244. https://doi.org/10.3390/vaccines11071244